
Abstract
Determination of death requires specific knowledge, training, and experience in most cases. It can be particularly difficult when external conditions, such as objective hazards in mountains, prevent close physical examination of an apparently lifeless person, or when examination cannot be accomplished by an authorized person. Guidelines exist, but proper use can be difficult. In addition to the absence of vital signs, definitive signs of death must be present. Recognition of definitive signs of death can be problematic due to the variability in time course and the possibility of mimics. Only clear criteria such as decapitation or detruncation should be used to determine death from a distance or by laypersons who are not medically trained. To present criteria that allow for accurate determination of death in mountain rescue situations, the International Commission for Mountain Emergency Medicine convened a panel of mountain rescue doctors and a forensic pathologist. These recommendations are based on a nonsystematic review of the literature including articles on determination of death and related topics.
Keywords
Introduction
Activities in the mountains are associated with risks of accidents that can cause death. Knowledge regarding determination of death at the scene of an incident is important for medical and other mountain rescue personnel. In a mountain environment, there may be objective hazards such as rockfall, avalanches, inclement weather, bad visibility, and low partial pressure of oxygen at high altitudes, limiting the work capacity of rescuers. These affect the safety of the rescue team, which must always take priority when deciding whether a rescue should be undertaken. 1 If the victim is declared dead, a rescue mission could be aborted for safety reasons, and evacuation of the body could take place later when conditions are safer. Furthermore, unnecessary medical interventions, such as futile attempts at cardiopulmonary resuscitation (CPR), could be avoided. 2 Determination of death can be particularly helpful in incidents with several victims or when multiple incidents occur simultaneously by allowing resources to be reallocated and rescue personnel to be assigned to other duties. 3 Finally, the workload of the hospital team can be reduced by preventing unnecessary admissions.
Death must be determined with absolute certainty. Incorrect determination of death, 4 with failure to perform CPR, may lead to an avoidable death with emotional and legal consequences for the rescuers 5 and more distress for the next of kin.
We do not discuss termination of prehospital CPR that is already in progress6,7 or autorescuscitation (the “Lazarus phenomenon”), 4 in which there is return of spontaneous circulation after termination of CPR in a patient who was considered to be dead.8,9 Our goals are to summarize the methods used to make a determination of death, define objective criteria that can help in this difficult task, discuss pitfalls, and provide recommendations on how to proceed in special situations that may be encountered in mountain rescue.
Methods
The International Commission for Mountain Emergency Medicine convened a panel of mountain rescue doctors and a forensic pathologist. In addition to searching the internet for guidelines regarding determination of death, a nonsystematic literature search was performed in PubMed for articles related to determination of death and related topics. Abstracts of pertinent articles and reference lists of interesting articles were skimmed for further articles. Seventy-nine articles were included. There were no exclusion criteria based on article type. Only articles without relevant content were excluded.
Discussion
Definition of Death
In the past, death was based on a simple determination of the cessation of heart and lung function. It was then assumed that an individual was no longer alive. The development of ventilators and other life-support methods that replace the functions of the heart and lungs has made the definition and diagnosis of death much more complicated. 10
Internationally, death is defined as a permanent loss of capacity for consciousness and all brainstem functions, which cannot resume spontaneously and will not be restored through intervention or because of situational or environmental conditions. This can happen as a result of permanent cessation of circulation or after catastrophic brain injury.2,11-13 In addition, a primary or secondary respiratory event can cause hypoxemia resulting in cardiac arrest and cessation of circulation to all organs including the brain.
14
The phenomenon of death can be divided into 2 categories
15
: The absence of vital signs. This is unreliable for confirming that life has ceased. The presence of definitive signs of death that are sufficient to determine death.
Timeline of Events Immediately before and after Death
Dying can be a process that takes place over time in which biological and physiological functions gradually cease, but it also can be sudden, as in trauma.13,16 Death itself is an event during this process. It is the step beyond which a cell or an organism is irreversibly committed to die 17 and is the time when a person can be said to have died.13,18 Death can sometimes be delayed or averted by life-sustaining treatment. Doctors should decide at what point in this process there is permanence and death can be appropriately declared. 16
As soon as a person has died, postmortem changes begin. The rate at which these occur can be modified by various factors. Examples of internal factors include bleeding, fever, or infections. An example of an external factor is ambient temperature. A general timeline can only roughly depict the events immediately before and after death (Figure 1).
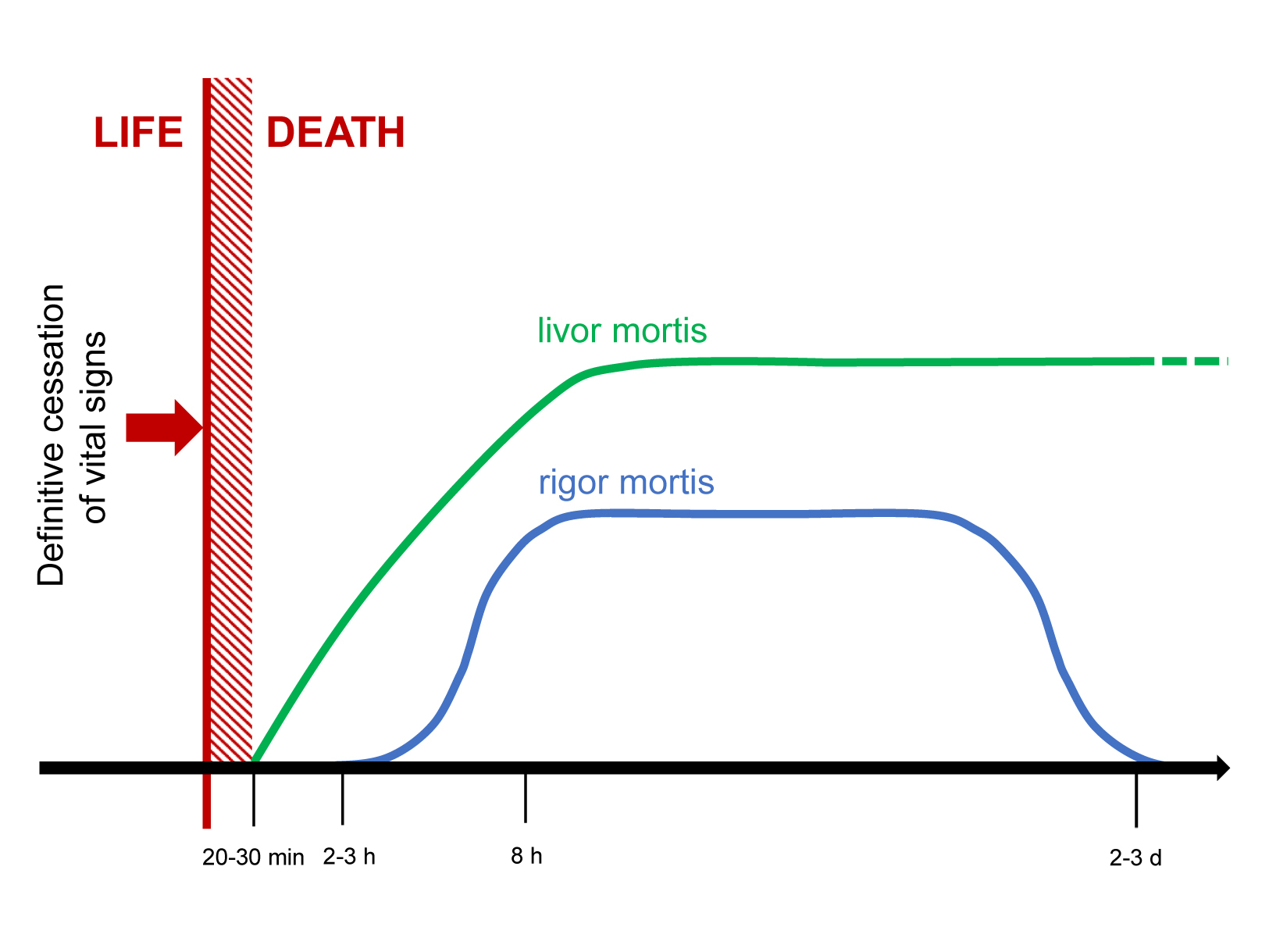
Events before and after death. Although vital signs are completely absent at the time of death, definitive signs of death appear only after an additional 20 to 30 min. During this time (hatched column) death cannot be determined by physical findings in most cases. The heights of the lines are not proportional to intensity.
Methods of Determination of Death
The determination or diagnosis of death describes the examination of a person to establish whether clinical features are present indicating that death has occurred. This can be one of the most difficult decisions in medical practice. It must be accomplished while avoiding diagnostic errors. 16 In a prehospital setting in a mountain environment, determination of death may be even more difficult because a physician, who is responsible for this task in most organizations, may not see the person at the scene 19 and because technical support, such as cardiac monitoring, may not be available.
Differentiating between a newly deceased person and an apparently lifeless person who might benefit from immediate CPR can present a special challenge.5,20,21 Death should only be determined and resuscitation efforts withheld when it is clear that the victim has sustained irreversible cessation of circulatory and respiratory functions. In many cases, this is only possible with certainty if definitive signs of death are observed during an external inspection of the body. 16 It may take at least 20 to 30 min after death before definitive signs of death appear. Therefore, it may be almost impossible to pronounce a victim dead immediately after death. Exceptions are the presence of criteria for the termination of CPR or a catastrophic injury, such as decapitation.7,22 Protocols for withholding resuscitation should be based on the determination that there are no signs of life, that injuries are obviously incompatible with life, or that there is evidence of prolonged arrest (Figure 2). 23
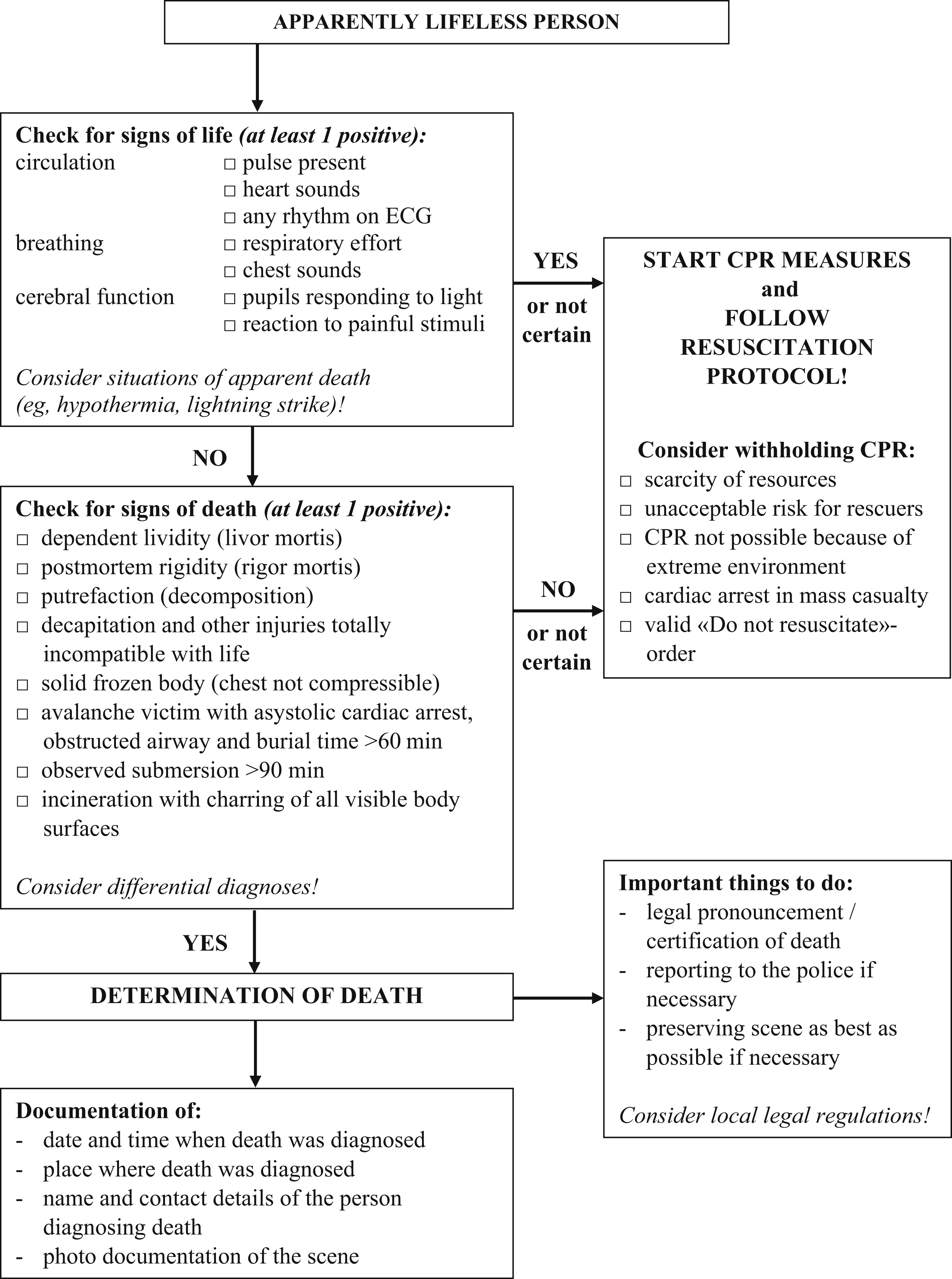
Algorithm for the determination of death in mountain rescue.
Unless there is a valid do-not-resuscitate order, if there is any uncertainty about the determination of death, all feasible life-saving measures should be attempted and the patient should be transported emergently to a hospital.20,24 The same applies to patients with traumatic cardiac arrest without definitive signs of death, although factors that predict failure of CPR, such as long duration of transport to a hospital and high injury severity score, are common in mountain incidents. The outcomes of CPR in trauma patients are dismal. 25 In a mountain or remote environment, a patient in cardiac arrest has an extremely poor prognosis, often because the rescue network is too thinly stretched. 26 For example, in a retrospective study from Austria, only 3% of patients with primary cardiac arrest in the mountains survived to hospital discharge. 27 Similarly, a study from Korea assessing patients who had sustained nontraumatic out-of-hospital cardiac arrest while exercising in a national or provincial mountain park found that outcomes were worse compared to patients in cardiac arrest in other locations. 28
Vital Signs and other Clinical Findings
If an apparently lifeless person is found and it is not obvious that the person is dead, rescuers should check for signs of life. Breathing and pulse may be faint and very hard to detect, especially in a hypothermic patient. 29 Rescuers should suspect special circumstances, such as severe hypothermia, when a cardiac arrest occurs in the mountains and should check for signs of life for up to 1 min. 30 If electrocardiography or point of care ultrasound are available, rescuers should look for signs of cardiac activity. A hypothermic patient in cardiac arrest is not dead unless warm and dead, unless there are definitive signs of death.
Consciousness
A conscious person responds purposefully to voice, touch, or painful or other noxious stimuli, such as a sternal rub. An unconscious person may not respond but nevertheless can still be hemodynamically stable.
Breathing
The rescuer should open the airway by extending the neck and lifting the chin, or by using a jaw thrust if there is a concern about a possible high spinal injury. The rescuer should look for chest movement or place a hand flat on the chest to feel for small chest rises. If the rescuer places an ear close to the patient’s mouth, breath sounds may be audible or air movements may be sensed. If a stethoscope is available, the rescuer should listen for breath sounds over the trachea. Another technique is to hold goggles over the nose and mouth to look for misting. Absence of misting does not indicate absence of respiration. The rescuer should allow 1 min to check in case the person is breathing very slowly, possibly as slowly as once every 10 to 15 s. 29 Breathing is often easier to detect than a pulse, although slight respiratory movements can be overlooked with thick clothing. Circulation is present if regular breathing is present, rather than gasping or agonal (occasional) breaths. Point of care ultrasound or measurement of end-tidal CO2 may also be useful, if available.
Pulse
A pulse may be felt where large arteries lie close to the skin. In adults and children, the best locations are the carotid arteries at either side of the neck or the femoral arteries in the groin. In infants, the brachial and femoral arteries are easiest. 31 If a stethoscope is available, the rescuer should attempt to check for heart sounds, although these may be faint. If available, cardiac monitoring can be very valuable for assessing the presence of cardiac electrical activity and for checking the rhythm. As with breathing, the pulse can be weak and very slow (bradycardic), with a heartbeat only every few seconds, and very difficult to detect. A low-output circulatory state can be present, even when a pulse is not palpable. 16 In severe hypothermia, there may be a very slow, small-volume, irregular pulse that is not palpable, and blood pressure may be undetectable. 30
Movement
Any active movement of joints must be considered a sign of life. Active movements must be distinguished from passive movements caused by touching the body or changing the position of the body because of gravity in rough terrain. Gasping is considered to be a sign of recent cardiac arrest and should trigger CPR. 32
Pupils
Pupillary response is tested by shining a light in the eyes. Pupils normally constrict with direct illumination (direct response) and with illumination of the opposite eye (consensual response). In patients with intracranial pathology, bilateral fixed and dilated pupils (large pupils that do not respond to light) can indicate brainstem damage with a poor prognosis or can be caused by drug use. Especially in severe hypothermia, drowning, or lightning injury, fixed and dilated pupils are not reliable signs of death.
Core temperature
Temperature measured with a probe in the lower third of the esophagus correlates well with the core temperature of the body. 33 Epitympanic temperature may be falsely low if the environment is very cold, the probe is not well insulated, or the external auditory canal is filled with wax, snow, or water.33,34 Vital signs may be present below a core temperature of 24°C. 29 The lowest core temperatures from which patients have been successfully resuscitated are 4.2°C for induced hypothermia 35 and 11.8°C for accidental hypothermia.35,36 Core temperature should not, by itself, be used to determine death or withhold resuscitation. 37
Absence of vital signs is not pathognomonic of death because signs may be absent although a person is still alive. In some situations, a person can have no vital signs but can be resuscitated. Reversible causes of cardiac arrest include the “Hs” (hypovolemia, hypoxia, hydrogen ion [acidosis], hypo- or hyperkalemia, hypothermia, and hypoglycemia) and “Ts” (tension pneumothorax, tamponade [pericardiac], toxins, thrombosis [coronary or pulmonary], and trauma) of advanced cardiac life support.38,39
Technological Adjuncts for the Determination of Death
In the prehospital setting, there are limited opportunities to obtain information about a patient’s status using technological methods. In addition to cardiac monitoring, point of care echocardiography may be useful to diagnose cardiac arrest. 38 Other technical methods, or measurements of physiologic parameters such as end tidal (exhaled) carbon dioxide (ETCO2) and serum potassium, have no role in determining death in a prehospital setting. High and increasing ETCO2 values are associated with increased rates of return of spontaneous circulation and survival after CPR. Low ETCO2 alone should not be used to decide whether CPR can be stopped. Similarly, absence of ETCO2 alone should not be used to determine death. 40 Low serum potassium can only be used as a factor in rewarming decisions in hypothermia.30,41-45 In cold conditions, which are common in the mountains, electronic devices often fail. A meticulous clinical examination is therefore mandatory.
Definitive Signs of Death and other Conditions that are Diagnostic of Death
Many conditions are diagnostic of death (Table 1). When at least 1 of these conditions is present, initiation of CPR is contraindicated.5,16,23,24,46-48
Conditions allowing determination of death in the mountains
Early Postmortem Changes
Early postmortem changes of the body may appear as early as 20 to 30 min to several hours after the person has died.
Dependent lividity (livor mortis, postmortem hypostasis)
After permanent cessation of circulation, blood pools in congested vessels. Dependent lividity is caused by gravity and refers to skin discoloration of the dependent (lower) parts of the body in the position in which the body rests after death occurs. This discoloration does not form in areas of the body with pressure on the tissue from contact with a hard surface or from tight clothing. Dependent lividity first appears approximately 20 to 30 min after death. It is most often the first postmortem transformation that can be detected. It is initially blotchy but later becomes confluent. During the first few hours, dependent lividity may blanch easily with pressure. Later, it becomes fixed. Dependent lividity usually has a bluish color due to oxygen depletion. In cold temperatures, it may completely or partially assume a reddish color (Figure 3A and B). It can be decreased or absent after blood loss (Figure 4), in people with anemia, or when the body is in constant motion after death, as in water. When dependent lividity is decreased or absent, determination of death in the early postmortem period can be very difficult. Areas of dependent lividity that are spaced widely apart indicate that the body has been moved after death. This situation should be investigated, although there might be a simple explanation in the mountains (eg, a change in the position of the body caused by natural forces such as rockfall). Depending on the time the body position changed, dependent lividity may be found on both sides of the body. To see lividity, the body must often be at least partially undressed.
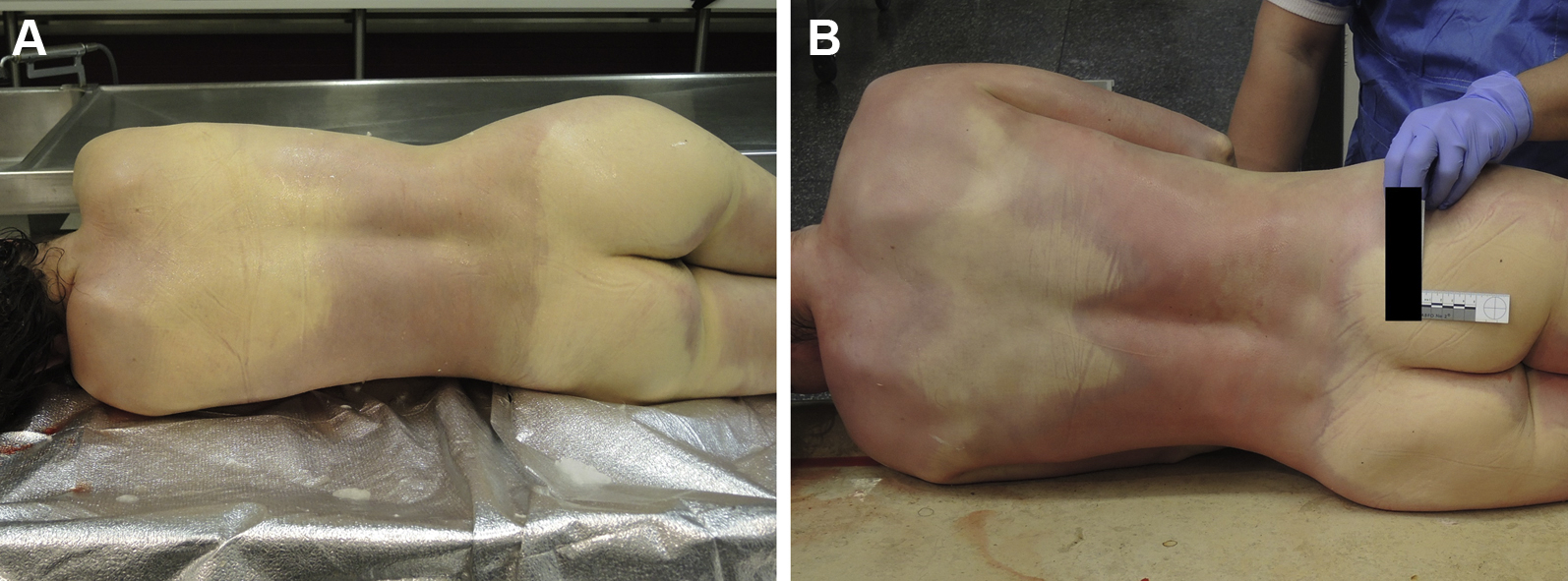
A, Dependent lividity in a woman about 3 h postmortem. B, Dependent lividity of the same woman 1 d later after being placed in a cold storage. Dependent lividity is more intense and has developed red and blue areas. (photos: Corinna A. Schön)

Victim with nearly any dependent lividitiy 1 d after death, likely due to internal hemorrhage after a fall from a height. (photo: Corinna A. Schön)
Postmortem rigidity (rigor mortis)
Stiffening of a corpse is normally the second definitive sign of death. After initial complete relaxation, the muscles become increasingly rigid due to postmortem breakdown of enzymes in the muscle fibers. This phenomenon can usually be recognized by stiffening of joints, such as fingers, elbows, or knees, approximately 2 to 3 h after death. The stiff body remains in the configuration in which it became rigid, even if it is moved (Figure 5). Normally, postmortem rigidity disappears about 2 to 3 d after death (secondary relaxation) due to disintegration of the muscle fibers because of tissue breakdown and putrefaction.
49
The factors that influence postmortem rigidity include49,50

Body with postmortem rigidity. After the body was turned from the prone position to the supine position, the joints of the upper extremities maintained their positions. (photo: Corinna A. Schön)
Late Postmortem Changes
Late postmortem changes of the body indicate in most cases that the person has been dead for a longer time.
Putrefaction (decomposition)
Decomposition of the human body is caused by bacteria in hypoxic conditions. 52 Changes include discoloration of the skin ranging from green-gray to brown-red (Figure 6A and B), marbling, formation of fluid-filled skin blisters, flatulence of body cavities, and air in soft tissues. The nature and timing of the changes depend on temperature and on the presence of pre-existing infections.
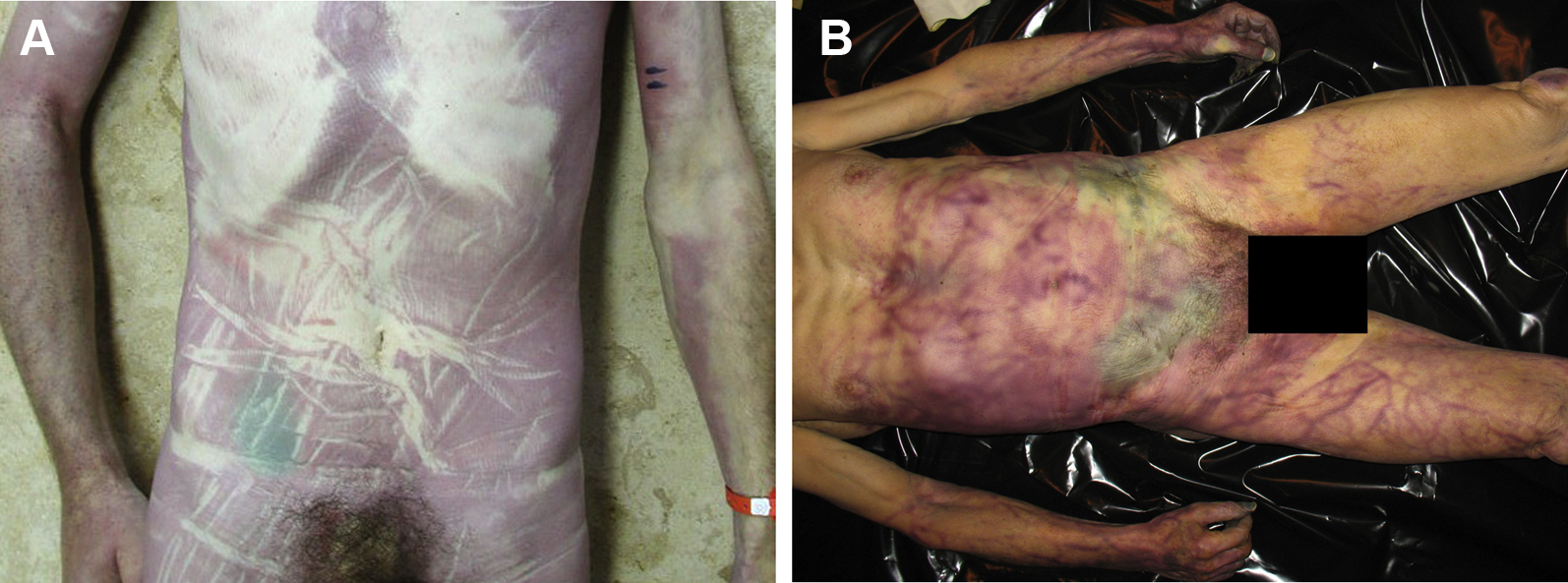
A, Early putrefaction of the right side of the abdomen. The green discoloration of the skin is typical but can be misdiagnosed as a hematoma. The purple discoloration of the skin is due to dependent lividity. This victim was found in a prone position. B, Green discoloration of the skin of both sides of the abdomen. Visible superficial veins are also due to putrefaction. (photos: Corinna A. Schön)
Mummification
Mummification is a process in which the skin of a corpse is preserved. It occurs when conditions are cold or dry. 52 Strong direct sunlight can also cause rapid dehydration. Tissue becomes very dry, hard, and brown or black (Figure 7).

Early mummification of the nose, lips, and skin on the left side of the face. The tissue is dry, hard, and brown-black. (photo: Corinna A. Schön)
Adipocere
Adipocere refers to tissue that has become soap-like, whitish, hard, crumbly, and greasy. The formation of adipocere is the result of decreased microbial degradation due to a lack of oxygen in an environment with a high amount of water. Incompletely putrefied corpses develop adipocere when there is no exchange of air or water between the corpse and the environment.52,53 The soft tissue, mainly body fat, is converted by saponification to free fatty acids, alkali salts of fatty acids, and glycerol. Adipocere has no odor. The timing of the formation of adipocere depends on environmental conditions, but it occurs a few weeks after death at the earliest. Once formed, adipocere can persist for hundreds of years, acting as a preservative. 54 In addition to mummification, adipocere is a typical finding in “glacier mummies.” 55 -57
Skeletonization
Skeletonization (Figure 8) refers to the final stage of decomposition, during which the last remains of the soft tissues of a corpse have decayed or dried to the point that the skeleton is exposed. The rate of skeletonization depends on factors such as temperature and humidity and the presence of insects or other animals. Especially in bodies found outdoors, skeletonization can be at least partially a result of predation by animals. Depending on altitude, there may be insects, such as flies or beetles that feed on soft tissue. Larger animals also can eat soft tissue, especially in areas in which skin is not covered by clothing (Figure 9A and B).

Partly skeletonized body found several weeks after the person went missing. Parts of the spinal column in the neck and the coccyx can be seen without overlying tissue. (photo: Mario Milani)
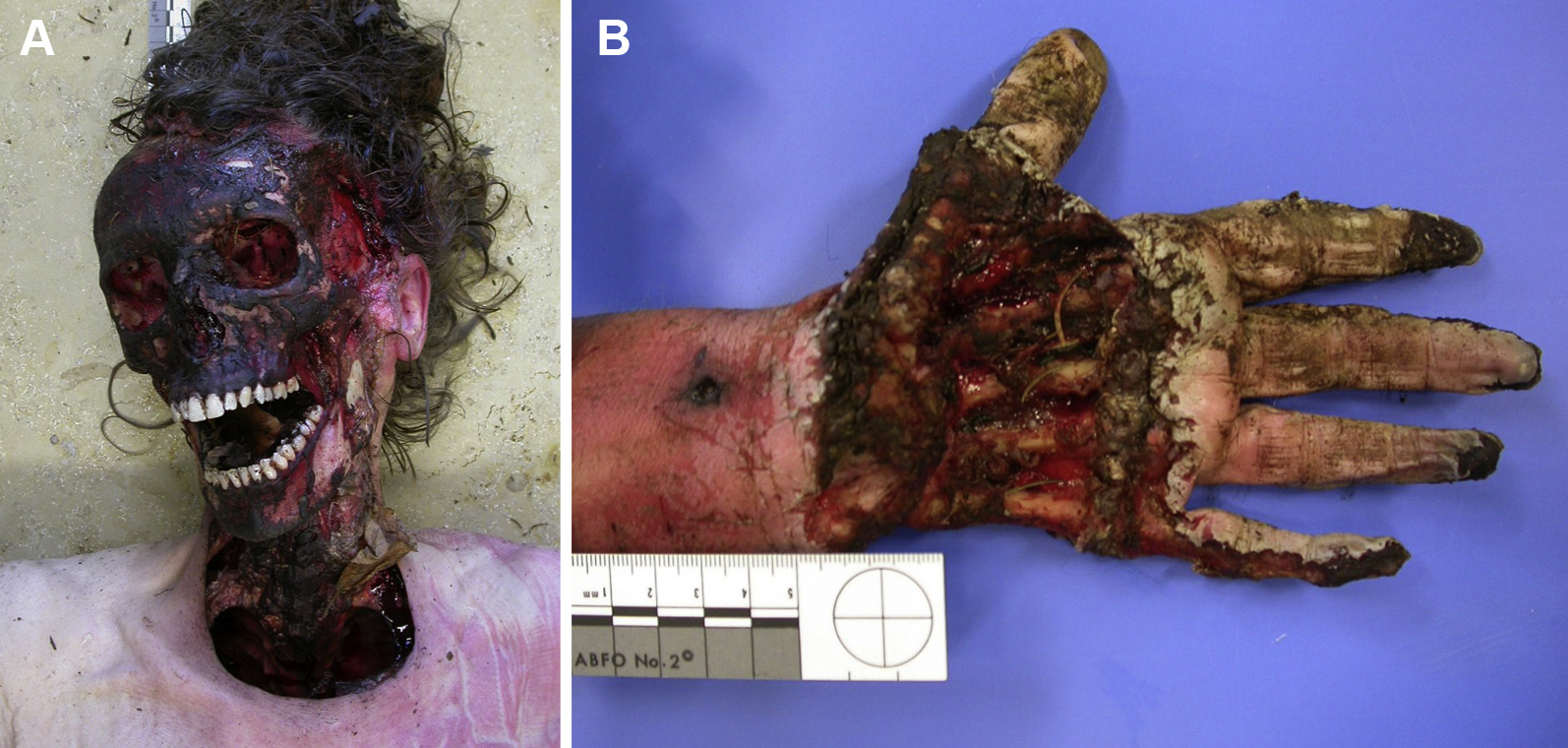
A, B, Skeletonization of the head, neck, and the left hand due to animal predation in a body that was found in a forest. (photos: Corinna A. Schön)
Body States that are Incompatible With Life
It can be quite difficult to determine whether an injury is fatal or to predict the outcome in a prehospital setting. 24 In addition to the aforementioned definitive signs of death, there are several body states that are incompatible with life. Catastrophic injuries include decapitation (beheading), which is separation of the head from the trunk; massive destruction of the skull and brain, with loss of brain matter (Figure 10); detruncation (hemicorporectomy or truncal transection), which is complete separation of the trunk below the shoulders and above the hips, through major organs and vessels (Figure 11); and incineration (charring of all observable body surface). These are conditions in which resuscitative efforts should be withheld. A frozen body with an incompressible chest is also not compatible with life. When only extremities are frozen, successful resuscitation may be possible. 58

Massive destruction of the head with loss of a large part of the brain after a fall from a height. (photo: Corinna A. Schön)

Detruncation after a fall from a height in rough terrain. (photo: Corinna A. Schön)
Special Situations
Water
In addition to other factors, water temperature and the duration of submersion (complete immersion in a liquid with head under water) play important roles in the outcome of drowning. 59 -62 Streams and pools can be very cold, especially in the mountains. If a victim of submersion without signs of life is found in icy cold water, there may be a neuroprotective effect with extended hypoxic survival of the brain. This may be caused by selective brain cooling because of hypothermia in general and as a consequence of inhalation of very cold water. The heart and the blood in the carotid artery, and therefore the brain, are cooled rapidly. 63 A submersion shorter than 10 min in water colder than 5°C has a potentially good prognosis. 61 A submersion longer than 25 min in water that is warmer than 5°C is associated with very low chances of favorable outcomes.64,65 However, resuscitation measures should not be withheld unless there has been a witnessed submersion in cold water for longer than 90 min. After 90 min, successful resuscitation is extremely unlikely.60,61 The time frame may be longer when the person has been submerged in an air pocket, such as in a vehicle. In such cases it may be difficult to estimate the duration of actual submersion with asphyxia. 66 Survival may be possible even after prolonged apparent submersion. 67
Avalanche
Resuscitation should not be initiated in an asystolic avalanche victim who has a completely obstructed airway and who was buried longer than 60 min. 30 A cardiac monitor should be used to confirm asystolic cardiac arrest. Resuscitation should also not be attempted for an avalanche victim in cardiac arrest when there are unacceptable risks to the rescuers, when the rescuers are exhausted, or in extreme environmental conditions in which effective CPR is not possible.7,68
Pitfalls
Misdiagnosis of vital signs
There are situations in which a deceased person can appear to be alive:
Misdiagnosis of definitive signs of death
Depending on the level of knowledge, training, and experience, even medical providers may have difficulty evaluating definitive signs of death. Several findings can be confused with definitive signs of death, so that a living person could be declared dead or attempts could be made to resuscitate a deceased person. Mimics of dependent lividity include hematomas (a solid swelling of clotted blood within the tissues), reddish skin discoloration of parts of the body that are not generally the lowest parts in hypothermia and frostbite, and some skin conditions. Dependent lividity can be overlooked in poor lighting conditions, in people with dark skin, when there are superficial injuries, and when skin is covered with blood, dirt, or other substances (Figure 12). Mimics of postmortem rigidity include stiff joints in cold conditions,5,69 severe hypothermia, sequelae of surgical procedures, or consequences of injuries. Conditions that can be confused with different stages of putrefaction include dark skin, hematomas, blistering, sepsis, and bleeding from the mouth and nose. Full thickness frostbite with black, mummified skin, especially affecting cold-exposed areas such as ears, nose, fingers, or toes can cause local mummification (dry gangrene), similar to beginning mummification after death (Figures 13A and B, Figures 14A and B).

It is difficult to appreciate dependent lividity due to multiple superficial skin injuries of the back. (photo: Corinna A. Schön)
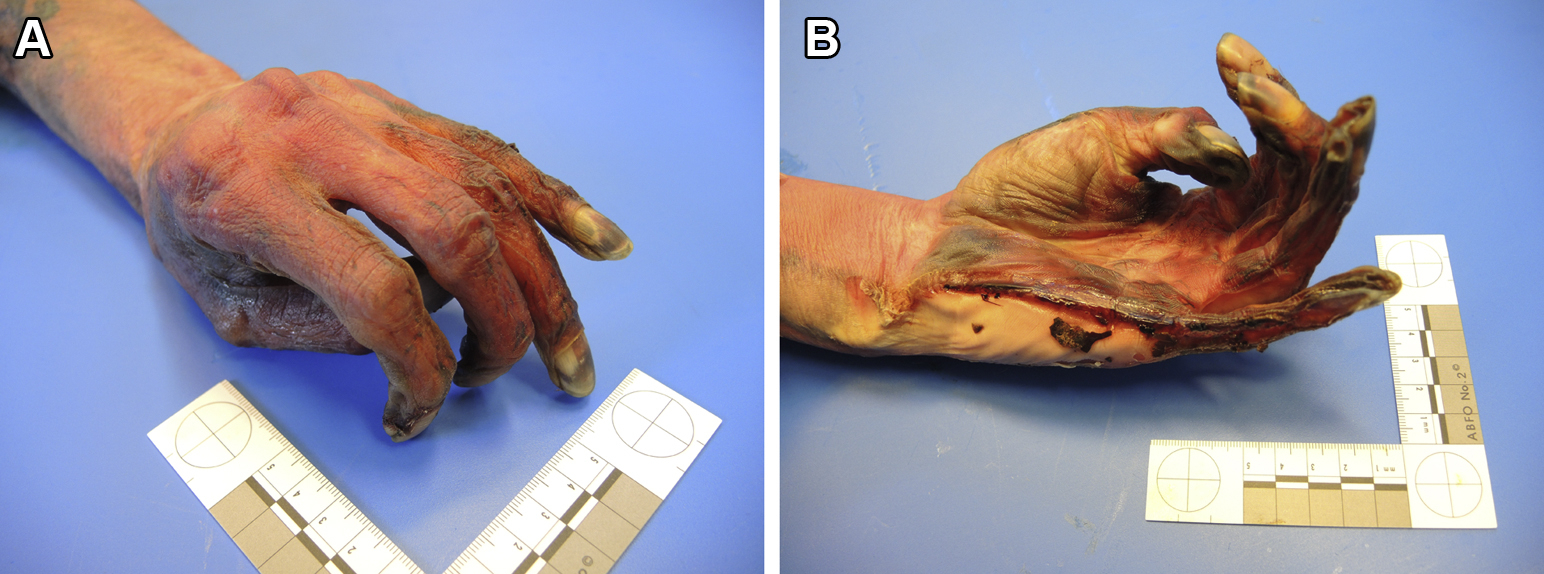
A, B, Left hand of a deceased person with early mummification. The skin is mostly brown and hard without sharp demarcation between mummified and nonmummified skin. (photos: Corinna A. Schön)
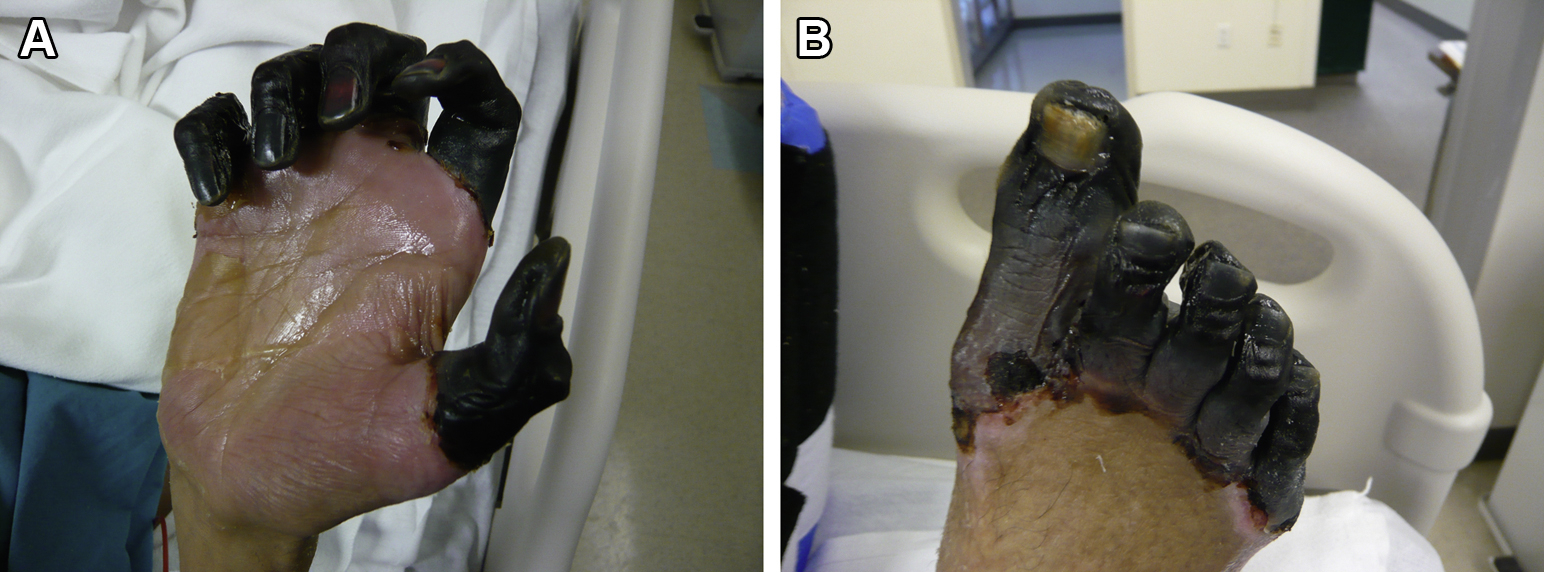
A, B, Severe frostbite of fingers and toes of a living person. The skin is black and shows sharp demarcation between necrotic (gangrenous) and intact skin. (photos: Ken Zafren)
Apparent death
There are many conditions that can simulate death. The term apparent death describes the situation in which a live person appears to be dead and no vital signs can be found, yet there are no definitive signs of death that could allow determination of death. Possible causes of apparent death are shown in Table 2.5,21
Possible causes of apparent death
Misdiagnosis of death by history of an event
One should be extremely careful if using the nature of an event to pronounce death. For example, the fact that a person fell from a certain height does not justify a declaration of death, even if there is no question that the chance of survival is low. If the rescue team is not in danger, they should attempt to reach the patient for inspection and direct examination if necessary, as rapidly as possible.
Determination of Death in Special Situations
Determination of death from a distance
Usually, the distinction between death and a condition requiring resuscitation should be made immediately. During a mountain rescue mission in hazardous conditions, it may be possible to conduct an initial visual inspection only from a distance. To declare a person dead without examining the body closely, it must be absolutely clear from the visual evidence that the victim is dead. This is only possible with conditions such as decapitation, detruncation, massive destruction of the body, or incineration.
Determination of death by nonauthorized persons
There is great international variability regarding the qualifications and specific conditions necessary to pronounce a person dead legally. In many countries, only a physician is officially allowed to do this. However, there are other jurisdictions in which medical professionals other than physicians, such as paramedics or nurses, can also pronounce death. This may apply in all cases or may be limited to certain situations.
If no officially authorized person can reach the site to determine death (eg, because of hazardous terrain with difficult access requiring specially trained personnel), special arrangements may be necessary. 76 It should be clear whether an unauthorized person may determine death on site and how to proceed after the body has been evacuated.
For an unauthorized person with no medical training, clear criteria must be defined so that a determination of death can be made with absolute certainty. A rescuer without medical training should determine death only by observing conditions that are incompatible with life, including late postmortem transformation, because the assessment of early definitive signs of death or early postmortem transformations is subject to error. In these situations, it is advisable that at least 2 rescuers assess the criteria to determine death.
On the scene, laypersons should attempt to discuss the decision with a physician or with another qualified medical professional by radio or telephone. 76 However, mobile and landline telephone networks and radio communications may be limited or unavailable in the mountains. 1 If death was determined on site by someone who was not authorized to declare a person dead, an official determination of death should be made by an authorized person at the earliest opportunity.
Risk Assessment
Due to hazards in the mountains, rescuer safety always takes precedence. The safety of the rescue team comes before the safety of the victim. Whether the victim is alive or dead, salvageable or not, the team should never put themselves at undue risk. In every rescue operation, a risk assessment should be made and a safe rescue plan should be adopted. The chance of a good outcome after cardiac arrest may be decreased due to limitations of human and material resources, delayed access, and prolonged transport in a mountain environment. 30 To minimize the risks, rescuers should be competent in moving in difficult terrain and in handling equipment and should mitigate the objective hazards.
Withholding resuscitation efforts at the scene may be acceptable if resuscitation attempts could increase the risk to the rescuers. If it is too hazardous to examine an apparently lifeless person on site, the victim should be evacuated to a safe location for further examination. 7 It may be necessary to delay a rescue operation until the risk to the rescuers has decreased to an acceptable level. 77 -79 This is especially important if the operation is a body recovery.
Training
Mountain rescue organizations should carry out regular training on determination of death and the actions that should be taken after a death. This training should be appropriate for medical professionals and medically and (especially) nonmedically trained mountain rescuers. Depending on the situation, there is no guarantee that a medical professional will be at the scene. Education and training must include identification of the definitive signs of death. In addition, rescuers must be aware of local requirements, including regulations, the roles of other agencies, methods of interagency communication, and ethical considerations. Fortunately, determination of death is not part of the daily routine in mountain rescue, but mountain rescuers should be aware that it needs to be handled with the utmost professionalism in the interest of all parties. 76
With appropriate training, support, and a detailed flowchart or protocol, the task of determining death can be undertaken successfully and reproducibly. It is the responsibility of a mountain rescue organization to establish a standard operating procedure with clear criteria defining the situations in which rescuers without medical training are allowed to determine death, including a step-by-step outline of the actions that are triggered by the determination of death.
Actions to be Taken after Determination of Death
When a person has died, a number of steps must be completed in addition to the determination of death. Some actions must be taken within a certain time. The case must be reported to the authorities depending on the manner of death or if the body is not identified. In these cases, the authorities must be notified and permission granted to remove the body. When there are suspicious circumstances, every effort should be made to preserve the scene and the body as much as possible. Any manipulation of the scene should be reported to the authorities. Especially if the body will be removed, photographic documentation should be taken showing the scene, any equipment that was used, and the position and state of the body before any manipulation. If the authorities are involved, communication with the family, friends, and other parties is usually done by law enforcement agencies. Only a designated suitably trained member of a mountain rescue organization should give information to the media, in consultation with the authorities.
Rescuers who have contact with the family of the victim should show empathy. Information about the circumstances of death may be an important stage in the grieving process. Because death in mountain rescue is usually a sudden and unexpected event, it may be helpful to involve a crisis intervention team or other psychological support service for the next of kin and for the members of the mountain rescue team. The privacy and dignity of the deceased should always be protected as much as possible.
Limitations
Because there is international and regional variability in legal regulations, mountain rescuers should be familiar with the applicable regulations in their own areas and should implement specific procedures for determination of death and for the management of the event.
Conclusions
Determination of death requires specific knowledge, training, and experience. Recognition of definitive signs of death can be problematic due to the variability in time course and the possibility of mimics. Determination of death is particularly difficult when external conditions, such as objective hazards in the mountains, prevent close physical examination of an apparently lifeless person, or when examination cannot be accomplished by an authorized person. We present criteria to allow the accurate determination of death, even in extreme situations, to avoid unnecessary rescues.
Footnotes
Acknowledgements
Author Contributions: CS wrote the initial draft consisting of a nonsystematic review and recommendations. All coauthors expanded, and revised the draft. Following discussion among the authors, further critical revision, and approval of the final version, ICAR MedCom approved the manuscript to be submitted for publication in Zakopane, Poland, in October 2019. Photos were contributed by CS, MM, and KZ with permission to publish.
Financial/Material Support: None.
Disclosures: None.
Presented in part at ICAR Congress, October 2019, Zakopane, Poland.