
Abstract
There has been exponential growth in paramedicine research activity and capacity over the last decade. With a strong academic culture emerging from its tertiary-based paramedicine education pathways, Australasia sits comfortably amongst the leading regions for paramedicine research. In the absence of clear paramedicine research priorities, there is concern that inadequate support infrastructure is in place to guide researchers, academics, paramedics, and policymakers within the profession to produce meaningful research capable of triggering change and advancement. The identification of paramedicine research priorities in Australasia, along with the barriers and enablers to research in this field, will prove invaluable to support the paramedicine profession, and improve healthcare systems, and patient outcomes in Australia and New Zealand. The study used a cross-sectional survey design which aimed to identify perceived barriers and enablers to the conduct of paramedicine research in Australasia and describe the demographic profiles and characteristics of respondents across professional, academic and research themes. Of the 341 respondents, 223 (65.4%) were male, 114 (33.4%) were female, and all geographical areas were represented. Approximately 60% of participants worked for a jurisdictional ambulance service in a clinical role. The median number of years of experience in paramedicine was 13 (IQR: 6, 24), with 52.8% having less than 15 years of experience. The analysis resulted in the identification of three themes for research barriers (system, process and human) and enablers, (work conditions, worker profile, and workplace). This study identifies the disconnect between stakeholders and the provision of resources such as funding, time, training, roles and data as major barriers to conducting paramedicine research. The ability or capacity of paramedics, as health professionals, to lead and undertake their own research was not questioned. The value of evidence-based research and autonomous paramedic-led research was identified as likely to empower future capacity within the profession.
Keywords
Introduction
Paramedics are integral to the Australasian health care system as they play a crucial role in delivering unscheduled community-based health care for injury and illness across the spectrum of acuity. In Australia and New Zealand, there were over 4.5 million patients attended to by paramedics during 2020–2021, consuming an annual budget of over four billion Australian dollars.1,2
In recent decades, paramedicine as a discipline has evolved considerably and continues to morph away from historical ambulance jurisdiction roots. Models of care continue to emerge, scope of practice continues to expand, and the role of the paramedic continues to diversify.3,4 Concurrent to this evolution in practice has been an exponential growth in paramedicine research activity and capacity. With a strong academic culture emerging from its tertiary-based paramedicine education pathways, Australasia sits comfortably amongst the leading regions for paramedicine research. 5 The rapid growth in research can, however, lead to a myriad of research activities that as a result may become diluted, fractured, and lacking in collaboration and sharing of common resources. This in turn may lead to a proliferation of smaller localised collaborations rather than larger cooperative research groups with greater research power arising from pooling of resources and expertise. Smaller localised research teams with less frequent collaboration are less likely to attract research grant funding required to upscale projects into larger suites of research capable of achieving greater impact, and at more risk of duplication in projects. This is not to suggest a lack of merit in smaller-scale studies which form the building blocks to further research and allow novice researchers to develop their skills, confidence and connections. Establishing a research agenda, however, that provides clear priorities may draw researchers together, promote greater collaboration and resource sharing, and garner the most efficiency and impact from the research resources available. 6
The need for national research agendas has been recognised internationally, where there has been considerable effort to identify research priorities throughout North America and Europe.7–13 Despite Australasia's leading role in paramedicine research, no such work has recently been undertaken in this region, hence there exists what appears to be a lack of research focus, direction and prioritisation. 6
Australasia was an early proponent of national research agendas in paramedicine. In 2003 the first step in identifying Australian pre-hospital research priorities using expert opinion from delegates at a national symposium was undertaken and emphasised the importance of an ‘ongoing, targeted and coordinated research effort’. 14 In 2015 further research reignited the issue, arguing the importance of an Australasian research agenda being developed, and recommending a framework for how this research could be conducted. 6 Despite this, in the 20 years since this preliminary work, there has been no coordinated effort to identify the key research priorities for paramedicine in Australasia.
In the absence of clear paramedicine research priorities, there is concern that an inadequate support infrastructure is in place to guide researchers, academics, paramedics, and policymakers within the profession to produce meaningful research capable of triggering change and advancement. 6 The identification of paramedicine research priorities in Australasia, along with the barriers and enablers to research in this field, will prove invaluable to support the paramedicine profession, improve healthcare systems, and ultimately patient outcomes in Australia and New Zealand.
In establishing a national agenda of research priorities, it is also necessary to identify enablers and barriers to research into those priorities being conducted and implemented. Previous paramedicine research agenda projects have sought to identify barriers and enablers. In Canada, for example, barriers to paramedicine research include limited suitable funding opportunities, a lack of post-graduate research training infrastructure within the discipline, a lack of research mentors in the discipline, and a lack of connectedness between paramedic services and the tertiary academic sector. 7 These findings highlighted that an agenda requires a multifaceted implementation strategy if it is to achieve the required adoption and desirable impact. Amongst the enablers of paramedicine research, it has been suggested that the academic sector is central to research endeavours as the driving force within which the required research infrastructure and resourcing exist. In Canada a lack of connectedness between industry and academia was discussed, 7 a phenomenon previously highlighted in Australia. 15
The Australasian paramedicine academic research workforce is pivotal in this context however little is known about the demographic constitution of this group. The first description of Australasian paramedic academics and their experiences was from a small sample project in 2013.16,17 A decade on, during which the tertiary sector has evolved considerably, the demographics of academic researchers in Australasian paramedicine have not been revisited; this represents a gap in understanding the scale of the research capacity available to implement a research agenda, given the tertiary sector is most likely to initiate and lead research projects.
In an Australian or New Zealand context, no previous research has explored the barriers and enablers to paramedicine research. Against this background, the primary aim of this study was to identify barriers and enablers to conducting paramedicine research in Australia and New Zealand as perceived by key stakeholders including registered paramedics, university academics and researchers, and paramedicine industry managers and educators. In order to fully understand the barriers and enablers to research in paramedicine it is also important to understand the profile of those responding as it relates to their responses. The secondary aim was therefore to describe the demographic professional, academic and research profiles of respondents.
Methods
Design and paradigm
The study used a cross-sectional survey design, grounded in a relativist paradigm (valuations are subjective and relative to the perspective of an observer or the context) 18 and through a pragmatic theoretical lens (focuses on what works, considering multiple viewpoints, perspectives, positions and standpoints.) 18 The study was conducted as the first phase in a broader two-phase research project, ‘Research Agenda for Australasian Paramedicine’, aimed at creating a consensus-derived research priorities agenda for Australasian paramedicine. This first phase involved a national survey of paramedicine discipline stakeholders with three aims: (1) to identify perceived barriers and enablers to the conduct of paramedicine research in Australasia; (2) to determine the demographic profiles and characteristics of respondents across professional, academic and research themes; (3) to gather data on research priorities in paramedicine as perceived by a diverse group of discipline stakeholders. Aims 1 and 2 are addressed in this article. Aim 3 will be addressed in a separate paper describing the creation of the research priorities agenda using Delphi consensus methodology.
Participants
The project sought participants from all paramedicine profession stakeholders in any role that engage closely with the paramedicine profession. Participants were eligible if they were from Australia or New Zealand and engaged in the profession as a clinician, educator, manager, researcher or student.
Sampling and recruitment
A convenience sampling approach was adopted. The primary means for recruitment was through the Australasian College of Paramedicine (ACP), the peak professional body representing paramedicine in Australasia (https://paramedics.org/). ACP has membership numbers of approximately 9,000 and has an expansive reach throughout the region. ACP promoted the study through regular member email announcements, a monthly emailed newsletter, and social media posts. Recruitment then snowballed as the aforementioned communications were forwarded independently by recipients throughout the discipline. Survey responses were monitored in real-time throughout the response period to allow tracking of geographic location and participant-described areas of primary paramedicine engagement (education, clinical, management, or academia). In order to ensure balance in representation across areas of practice and geography, targeted promotion was strategically made to key members of the profession in some areas to ensure diversity and balance in sampling.
Instrumentation
A rapid literature review was undertaken to identify existing survey instruments, validated or otherwise, that could be used in original form or with some modification to meet the requirements of the study. None were identified, resulting in the creation of a new survey instrument tailored specifically to the aims and objectives of the study. The resulting 18-question survey instrument is provided in Supplementary Appendix 1. Fifteen questions related to participant demographics and characteristics, using drop-down menu options to gather nominal, ordinal or categorical data. Three questions were ‘open-ended’ free text responses, in which participants were asked to list and describe their perceived priorities for paramedicine research, and their perceived barriers and enablers to the conduct of paramedicine research in Australasia.
To test content and face validity, the survey was piloted by 15 people with research and survey design experience from outside the paramedicine discipline, as well as 10 paramedics representative of the participants the study sought to engage. They were asked to comment on clarity, appropriateness of item choices, time to complete and any other interpretive, structural or survey-logic issues. Minor amendments to the survey functionality and response options were made based on this feedback to produce the final instrument.
Data collection
Data were collected online using the Qualtrics (Qualtrics, Provo UT, USA) survey platform. The data collection period spanned 11 weeks, from 15 November 2021 through 31 January 2022. Weekly reminders were released by the ACP to promote awareness of the participation opportunity. Data collection was anonymous.
Data Analysis
Quantitative survey data were compiled and analysed using Excel (Microsoft Corporation), to produce descriptive statistics; these were reported as number and percentages, and as mean (standard deviation) or median (interquartile range) as appropriate following the assessment of distribution.
The qualitative open response free text data were analysed using NVIVO (QRS International, Doncaster, Australia). A thematic analysis was conducted utilising Braun and Clarke's 6-phase approach: data familiarisation, generating initial codes, searching for themes, reviewing themes, defining and naming themes, and producing a report.19–21
The open response data provided by participants was qualitatively analysed by two team members (HR and LR) to generate coded, thematic categories. HR provided the initial coding, generating over 500 separate entries. LR then grouped these initial codes into major thematic categories.
The amalgamation of these identified themes allowed for meaningful relationships of the phenomena under investigation to be developed. The process of identification and organisation was an iterative process, as the researchers worked concurrently on the data set. Both HR and LR consulted at various times throughout the coding and organising stages. Using NVIVO, the initial coding and development of the hierarchical coding schema or taxonomies was examined, compared and contrasted iteratively, emergent and not forced. HR and LR reviewed the schema to establish links between the ideas and concepts represented in the codes, which were further refined with each iteration as a constant comparative process.
Ethics
This study was approved by the Human Research Ethics Committee at Western Sydney University (H14650).
Results
Demographic and Professional Profile
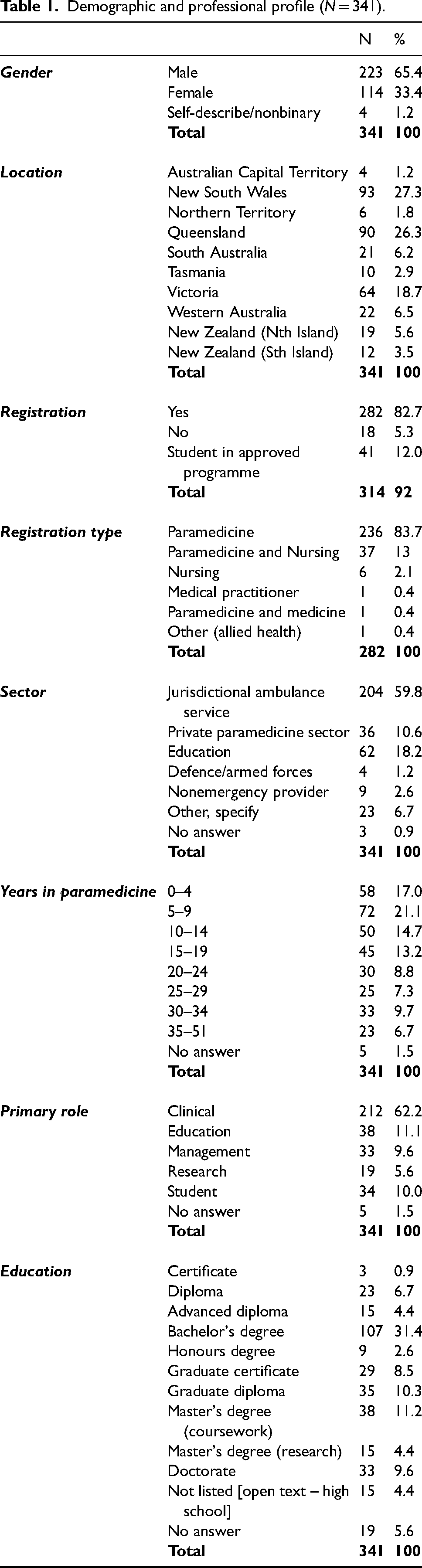
Of the 341 respondents, 223 (65.4%) were male, 114 (33.4%) were female, and all geographical areas were represented. A total of 282 (82.7%) participants were registered health professionals and of those 274 (97.1%) held Paramedic registration, inclusive of those with dual registration. Approximately 60% of participants worked for a jurisdictional ambulance service (JAS) in a clinical role. The median number of years of experience in paramedicine was 13 (IQR: 6–24), with 52.8% having less than 15 years of experience. Regarding education, 107 (31.4%) participants had a Bachelor's degree and 33 (9.6%) had a Doctorate. See Table 1 for a complete summary of participant demographics and paramedicine profession profiles.
Demographic and professional profile (N = 341).
Academic Profile
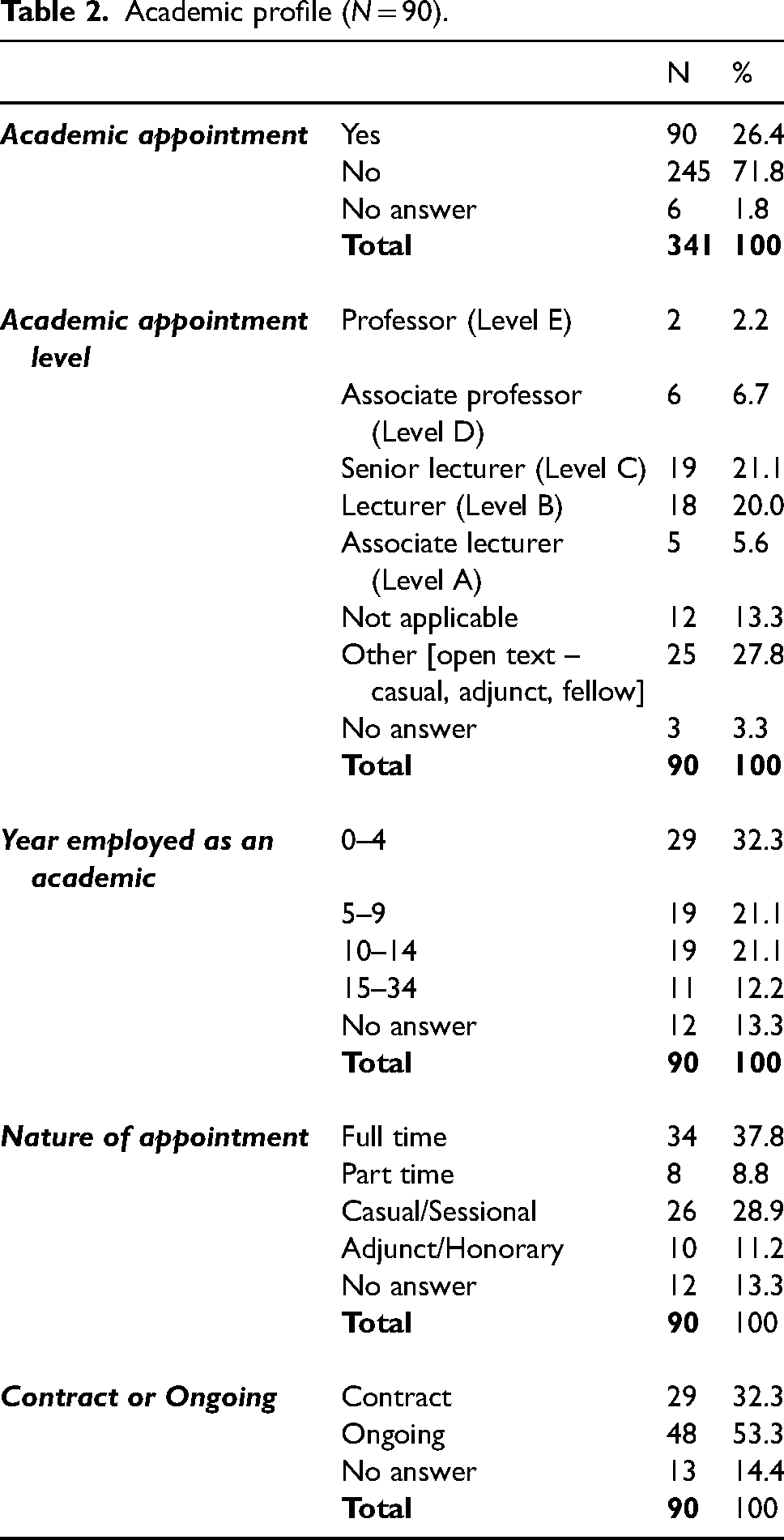
Of the participants, 90 (26.4%) held an academic appointment within the university sector. Of those the majority were Level C, Level B or casual appointments. The median number of years of experience in academia was 8 (IQR: 4–10.5), with 74.4% having less than 15 years of experience. The complete summary of participant academic profiles is described in Table 2.
Academic profile (N = 90).
Research Profile
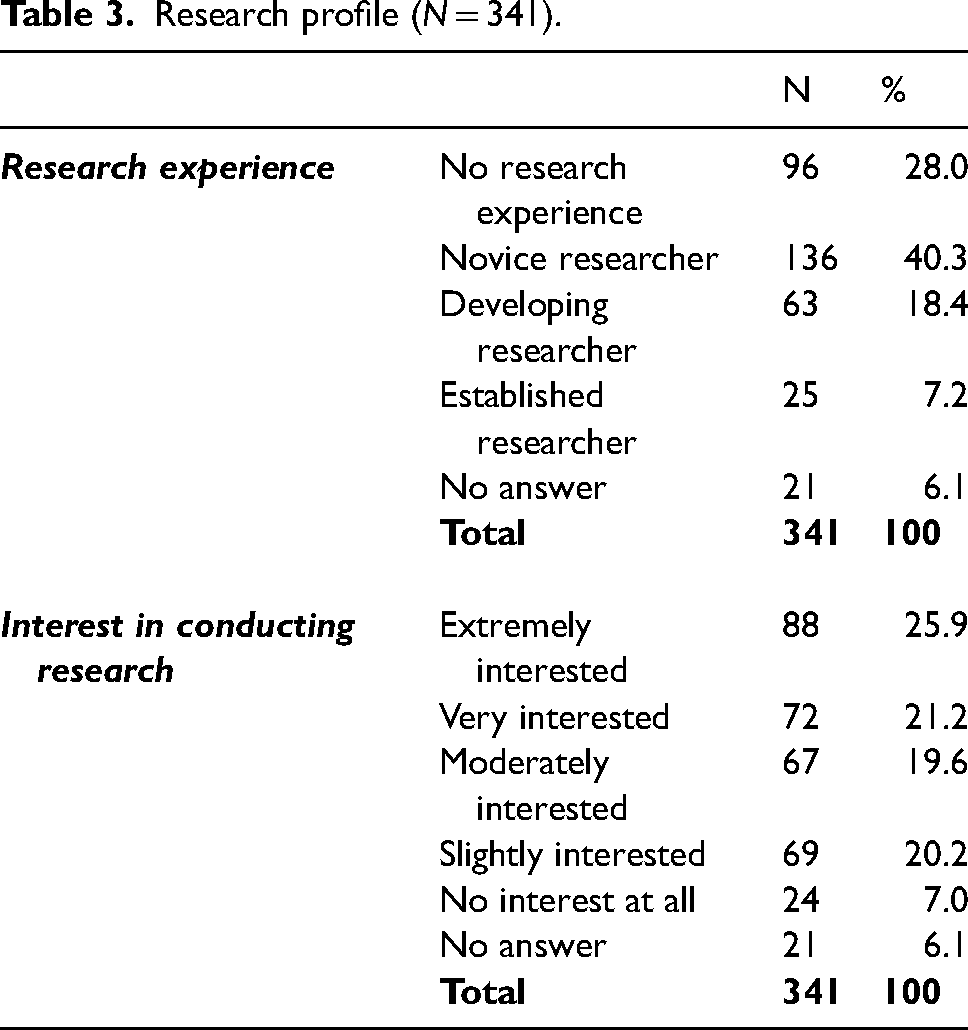
Of the participants, 232 (68.3%) described themselves as a novice researcher or having no research experience at all. Regarding interest in research, 227 (66.7%) described themselves as between moderately to extremely interested. See Table 3 for a complete summary of participant research profiles.
Research profile (N = 341).
Barriers and Enablers
Free text responses to the questions on perceived barriers and enablers to conducting research in the paramedicine discipline elicited responses which were coded from over 500 separate entries. The barrier responses generated 322 codes, while the enabler responses generated 183 codes. Analysis resulted in identification of 3 themes each. For ‘research barriers’, these were ‘system’, ‘process’ and ‘human’. For ‘enablers, these were ‘work (type) conditions’, ‘worker profile’, and ‘workplace (systems)’. Tables 4 and 5 provide examples of the most frequently reported codes and examples of individual comments.
Barriers to conduct of paramedicine research in Australasia.
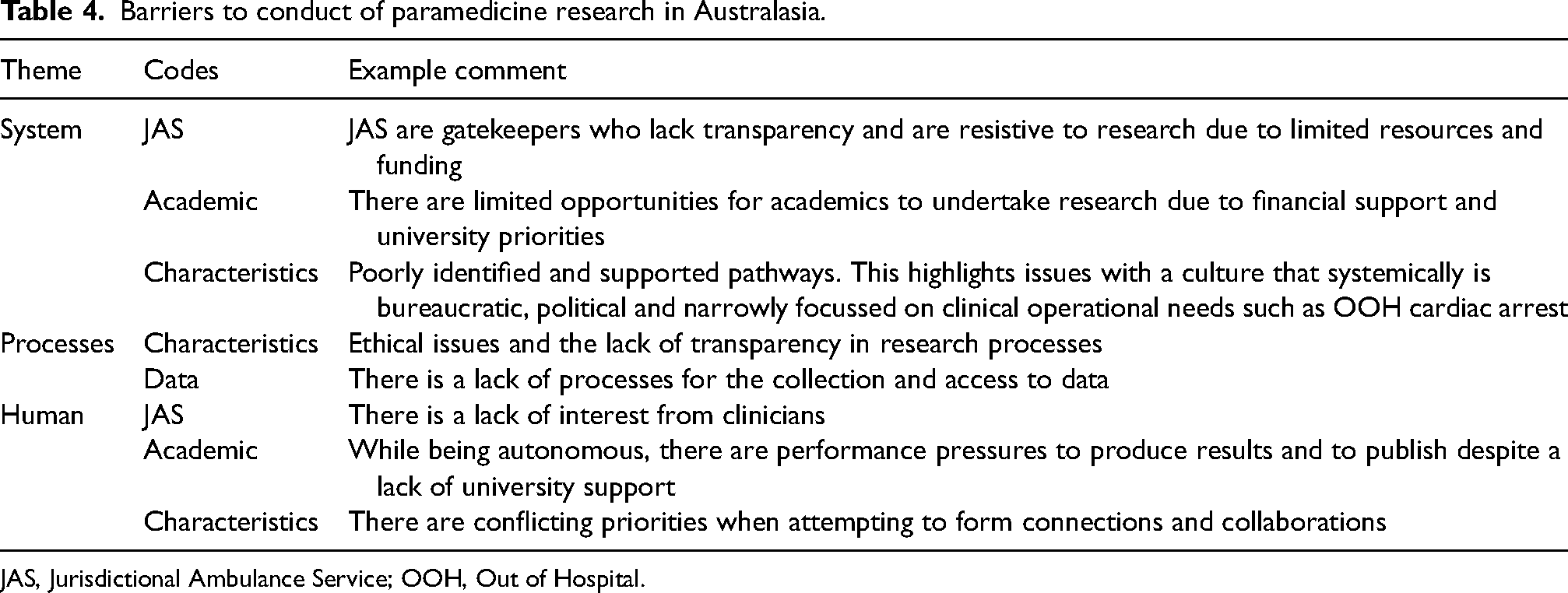
JAS, Jurisdictional Ambulance Service; OOH, Out of Hospital.
Enablers to conduct paramedicine research in Australasia.
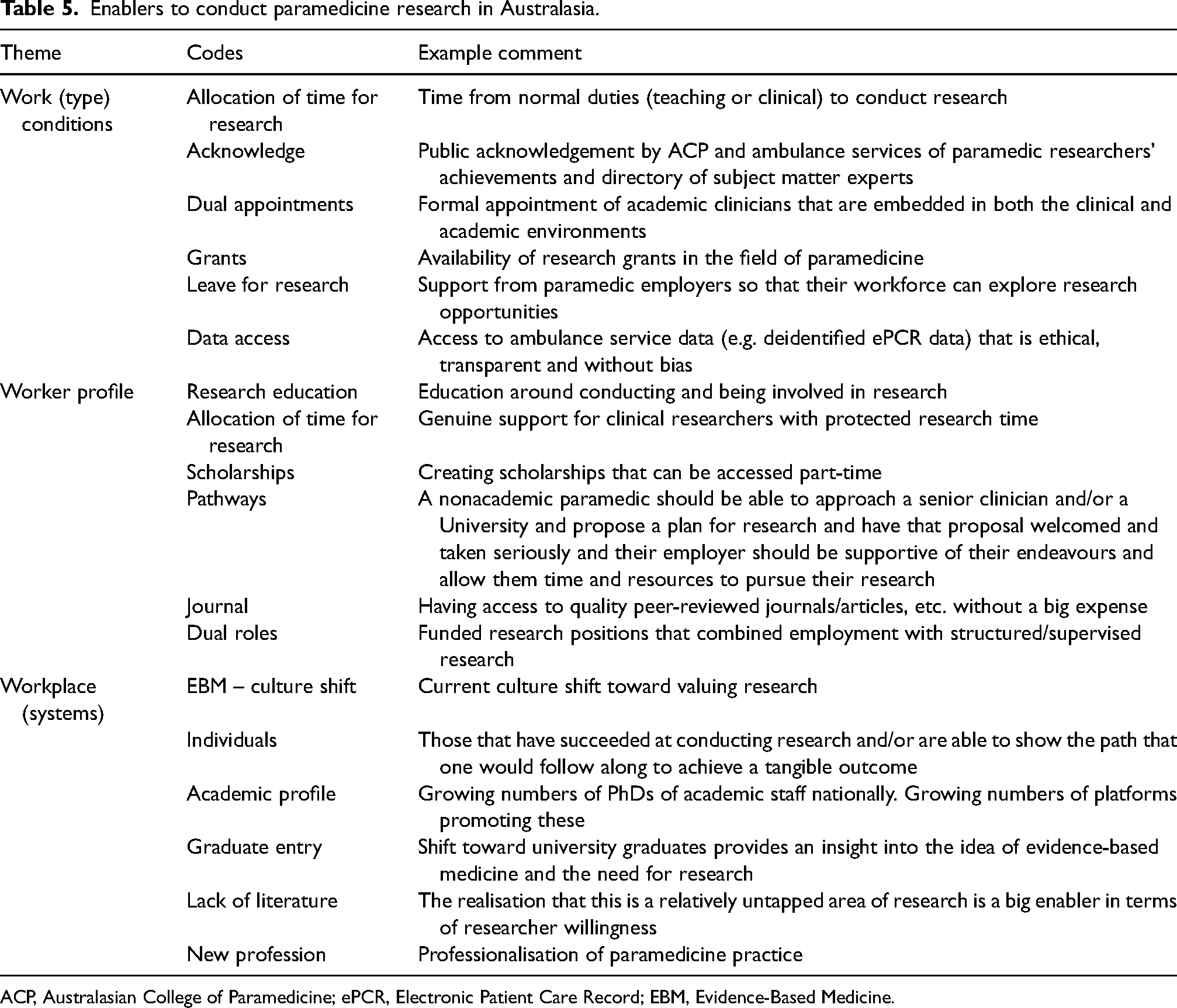
ACP, Australasian College of Paramedicine; ePCR, Electronic Patient Care Record; EBM, Evidence-Based Medicine.
Discussion
The development of a unique body of research is a key element of the professionalisation of paramedicine along with the development of a strong professional college, entry of the occupation into higher education (HE), and professional regulation. 22 Indeed, many international studies have examined the challenges faced and the opportunities that might encourage and sustain paramedicine research through the perspectives of ambulance services, medical directors, and other stakeholders.7–9,11,13,14 This effort to determine research barriers and enablers is another step in the journey toward professionalisation in Australasia.
The primary aim of this study was to determine barriers and enablers to conducting research in paramedicine. As the two concepts (barriers and enablers) are linked, with themes often overlapping and intertwined, we integrated them both into the following discussion.
Resources were a major theme throughout. The need for resources including human and financial were identified. This requires the active involvement of industry partners such as ambulance services and HE. Respondents identified that both JAS and HE can be associated with barriers and enablers when resourcing is needed to support paramedicine research. For example, the provision of pathways into research roles within JAS and/or HE requires support with time, mentorship, training, funding for projects and positive recognition. Studies over the last two decades in the United States, 8 Canada, 7 and Australia, 14 identified similar key weaknesses and opportunities that needed to be addressed if progress was to be made.
The provision or absence of sufficient time and support can act as both a barrier and an enabler for those wishing to engage in research roles. It was evident from the responses that time facilitated the ability to engage in the scholarship of attaining research skills through education pathways, study leave, and time to engage in research activity, particularly when managing the competing demands of academic, clinical or management roles. Participants identified having to use leave entitlements to facilitate relevant qualifications to attain research skills through education pathways. Research skill training was independent of being in a clinical or non-clinical role, when coupled with an academic role that was both challenging, problematic and perceived to be unsupported.
Participants felt stigmatised by being a paramedic engaged in research, and perceived that being identified as active in research, and associated roles, could lead to potential reputational risk and lack of peer support. This broad ‘blue-collar’ set of values has been previously reported in Australia, 23 and the UK, 24 and is still evident in the United States where the academicization of paramedicine is sometimes used as a derogatory term, 25 with a continued reliance on trade publications to disseminate research findings to paramedics. While these negative attitudes toward research might be residual markers that hark back to an earlier era when all scholarly endeavours were viewed with some level of suspicion or distain,4,26,27 action does need to be taken to improve research literacy and better support paramedicine research. A deeper exploration of this finding using qualitative methodology would be enlightening, as understanding the phenomenon may lead to strategies for the mitigation of such concerns.23–25
Our respondents expressed concern about the capacity and willingness of the JAS and HE to work together to effectively sustain paramedicine research activities. Research roles, whether in JAS or HE, need to be recognised as having intrinsic value to the wider profession. Supporting dedicated roles was both an enabler and a barrier to the scholarship of research. The challenges that paramedics face when transitioning into academic roles from clinical practice when supported and recognised academic pathways are weak or absent have previously been highlighted.16,17,28 This is perhaps particularly important for JASs that are almost completely dependent on the flow of well-educated graduate paramedics from HE to sustain their clinical workforces. They have a stake in sustaining a vibrant paramedic academic workforce that is held in the same professional esteem as those from other registered health professions. Continuing development of the paramedicine ‘research culture’ enables the increasing professionalisation of paramedicine. The evolving research culture requires an ongoing commitment from both JAS and HE with the physical and financial resourcing of research training programmes and dedicated JAS research units. In contrast, some participants identified the lack of research culture, particularly within JAS, with barriers to engaging in professional development, the lack of physical and financial resourcing of activities and consistent support for research projects.
Participants identified a wide range of practical support enablers and barriers for research activities, in particular the need for collaborative partnerships that facilitate ethically approved access to data, and improved systems to both record and manage this data. Similar issues have been identified in other countries that have developed research agendas for ambulance services or prehospital systems.7,11,29,30 At a national level, there is some anecdotal evidence that the quality of clinical data has improved and that collaboration across jurisdictions is possible. However, one issue may be that JASs are perceived to serve as gatekeepers to their own data and the collection of independent data within their organisations. As a result, paramedic academics from many paramedicine programmes have been unable to build the strong research profiles required for academic advancement in HE, with a number returning to clinical practice or leaving the profession as a result of their frustration. There is a perception that research access to JAS is not equitable across HE institutions or for researchers using qualitative or novel research methodologies.31,32 This concern was reinforced in a recent international study that found that while Australia is strongly represented in the paramedicine research literature, many of the authors were non-paramedics. 5 It is possible that the establishment of a more open access system or readily accessible data warehouse might better support the profession and arguably enhance the value of independent paramedicine research.10,33
Ethics approvals to gain access to data were perceived to be a barrier. While some concern was expressed about the perceived difficulties associated with receiving human research ethics board approvals, there appears to be a strong research workforce capacity to address these and other potential barriers to research that were identified in previous studies.14,34
In a positive development in 2020, the Australian Research Council (ARC) allocated paramedicine its own ‘Field of Research’ code for the first time, and it is anticipated that this will have a positive impact on funding opportunities. 35 At the same time, paramedicine research dissemination options have improved with Australasian paramedicine researchers now widely published in high-impact journals throughout the world. Several academic paramedicine journals are emerging around the world that aim to provide opportunities for emerging researchers to publish and to improve research literacy amongst paramedics. It is prudent to acknowledge however that there are many measurements for impact and that industry journals, as an example, also serve the purpose of disseminating the latest research to the discipline more broadly. The secondary aim of this study was to describe the demographic professional, academic and research profiles of respondents. Overall, the respondents were experienced, well-educated paramedics working in a variety of roles across a variety of settings and locations (Table 1). There was a disparity in gender with approximately two-thirds of the sample being male. Current research suggests the number of females entering the workforce is higher than their male counterparts.36,37 Perhaps the disparity in this sample is more related to who completed the survey and their roles and/or seniority, as historically males far outweighed females.36,37 Over one quarter (26.3%) worked in management, education and research roles. These roles tend to be filled by more senior paramedics rather than new graduates. This is also supported by the age break down with 62% of respondents having 10 or more years of experience in the profession.
While impacted by selection bias the generalisability of the barriers and enablers results were strengthened by the diversity of respondents beyond gender. Every state, territory and island in Australia and New Zealand were represented. Participants also worked in a variety of sectors. While dominated by JAS, the private sector, education sector and armed forces were also represented. Role variety was also evident with participants from clinical, education, management, and research roles as well as students. Finally, a broad range of years of experience was represented with percentages diminishing as years increased over 20.
The education profile of the study respondents (Table 1) shows minimal numbers below degree qualified (12%) and larger numbers completing postgraduate qualifications (47%). The growing number of paramedics completing postgraduate education enhances not only their clinical capabilities but in other areas including leadership and research. Postgraduate programmes generally contain at least some research components, therefore the knowledge, understanding, and capacity to conduct research across the profession can only be strengthened by this.
Also influencing the capacity of the profession to engage in research is the number of paramedics in academic appointments (26%). In general, there is an expectation that academics who participate in research and universities are best placed to provide the education and resources required to enhance engagement. Furthermore, regardless of their roles or appointments 47% of respondents were extremely or very interested in conducting research with another 40% moderately or slightly interested. The professional profile results from this sample suggested there is a very high level of interest in conducting research which can be attributed to the professionalisation of paramedicine and all that that entails, including education and value placed on the importance of evidence-based practice.
Limitations
Self-selection bias of only motivated people could have occurred due to the recruitment methods through social media and professional networks. However, the range of responses across most questions indicates good diversity. A notable outlier to this is the research experience with 68.3% placing themselves in the novice or no experience categories. This percentage could have influenced the barriers and enablers responses as those with little or no experience of the research process would have less expertise to comment on it. Conversely, their responses could highlight or amplify the barriers to beginner researchers getting involved. The number of respondents could be considered small and non-representative of the discipline being surveyed. A response rate cannot be generated though as there is no accepted population denominator that could be used for this. Together with the exploratory nature of the study, no a priori sample size could be calculated.
Conclusion
This research delivers insight into the paramedicine workforce, its relationship to research, and the perceived barriers and enablers to conducting research in paramedicine. It provides a snapshot of a diverse sample of the Australian and New Zealand paramedic workforce, spanning the spectrum of roles and experience. The demographic results in comparison to previous research describes a growing profession with increased capacity and interest in paramedicine lead research. This study identifies the disconnect between stakeholders and the provision of resources such as funding, time, training, roles and data as major barriers to conducting paramedicine research. The strategies required to confront these and other professionalisation barriers must include the development, adoption, and implementation of a paramedicine research agenda for Australia and New Zealand. The ability or capacity of paramedics, as health professionals, to lead and undertake their own research was not questioned. The value of evidence-based research and autonomous paramedic led research was identified as likely to empower future capacity within the profession.
Supplemental Material
sj-docx-1-pam-10.1177_27536386231167590 - Supplemental material for Barriers and enablers to paramedicine research in Australasia – A cross-sectional survey
Supplemental material, sj-docx-1-pam-10.1177_27536386231167590 for Barriers and enablers to paramedicine research in Australasia – A cross-sectional survey by Linda Ross, Louise Reynolds, Harry Reeves, Amy Hutchison, Peter O’Meara, Robin Pap, Nigel Barr, Michelle Thomson, Matthew Reardon and Paul Simpson in Paramedicine
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Linda Ross, Louise Reynolds and Robin Pap are Associate Editors of Paramedicine. Paul Simpson is the Editor-in-Chief of Paramedicine.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Correction (September 2023):
This article has been updated to disclose the Declaration of conflicting interests statement.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.