
Abstract
Background:
Bystander cardiopulmonary resuscitation is a key component of life-saving after an out-of-hospital cardiac arrest. In the pre-arrival instructions for out-of-hospital cardiac arrest, it is recommended that the patient be laid on a flat floor. However, the most common reason for not performing cardiopulmonary resuscitation is that the bystander could not move the patient.
Objectives:
This study aim to investigate the effects of using a home-bed mattress on the quality of chest compression.
Methods:
In this prospective, randomized study, chest compression without ventilation was performed for 4 min on a Resusci Anne manikin placed on a flat floor or on three types of home-bed mattresses (hard, medium and soft). Chest compression depth, chest compression rate and chest recoil were measured from the manikin with the Laerdal PC Skill Reporting System, and changes in chest compression quality using the four different surfaces were compared.
Results:
Thirty participants were enrolled to perform chest compression. There was no significant difference in chest compression depth and depth accuracy between the four surfaces. The median chest compression rates were 108.1 ± 8.5, 107.0 ± 8.3, 103.3 ± 8.9 and 98.3 ± 7.9 compressions/min (p < 0.001) for the flat floor, hard-, medium-, and soft-firmness mattresses, respectively. Moreover, there was no a significant difference in chest recoil accuracy.
Conclusion:
Using a home-bed mattress did not decrease the chest compression quality, except chest compression rate of soft-firmness mattress. Thus, it may be effective to initiate chest compression on a home-bed mattress if the bystander cannot move the patient to the floor.
Introduction
Bystander cardiopulmonary resuscitation (CPR) is a key component of life-saving after an out-of-hospital cardiac arrest (OHCA). 1 After recognizing an OHCA, a bystander can activate the emergency medical service (EMS) and perform dispatcher-assisted CPR (DA-CPR). 2
In the pre-arrival instructions for OHCA, it is recommended that the patient be laid on a flat floor. 3 However, moving the patient from the bed to the floor can be time-consuming, and secondary injuries may occur. A study on DA-CPR reported that the time to start DA-CPR averages 220 s, and the most common reason for not performing DA-CPR is that the bystander could not move the patient. 4
Previous studies have demonstrated the effect of using a hospital-bed mattress on chest compression (CC),5,6 but no studies have shown the effect of using a home-bed mattress on CC. In this study, we hypothesized that CC performed on a home-bed mattress by a bystander is not significantly different from CC performed on a flat floor and that knowledge on this might increase the bystander’s willingness to initiate CC. This study thus aimed to investigate the effect of utilizing a home-bed mattress on the quality of CC, using a resuscitation manikin.
Methods
Sample size
The sample size was calculated based on compression rate in interim analysis. The two-sided significance level was set at 0.05, and the power of the test was set at 80%. Standard deviation of compression rate was 7.9 compressions/min, based on the results of interim analysis. Assumed effect size was 0.686. The minimum number of participants in each group was calculated using a sample size calculator 7 and was determined to be 28.
Study design, setting and population
This prospective, randomized study was performed using a manikin. The study was conducted at a tertiary academic hospital between 1 November 2018 and 31 December 2018. Thirty healthy participants were enrolled to perform CC; 20 of them were certified advanced cardiac life support providers, and 10 were certified basic life support providers. The study was approved by the institutional review board of the hospital, and all participants provided written informed consent.
With the assumption of encountering an OHCA, the participants performed CC on a resuscitation manikin (Resusci Anne Simulator®; Laerdal Medical, Stavanger, Norway) using four different surfaces: a flat floor and three types of home-bed mattresses (Figure 1). The firmness of the mattresses (Beautyrest; Simmons Bedding Company, Quebec, Canada) ranged from 1 (firmest) to 10 (super soft). The three types of home-bed mattresses used were hard (firmness scale 2), medium (firmness scale 5), and soft (firmness scale 9). CC without ventilation was performed for 4 min. 8 The order of the interventions was randomly assigned, and follow-up tests were performed at least 3 days after the first test.
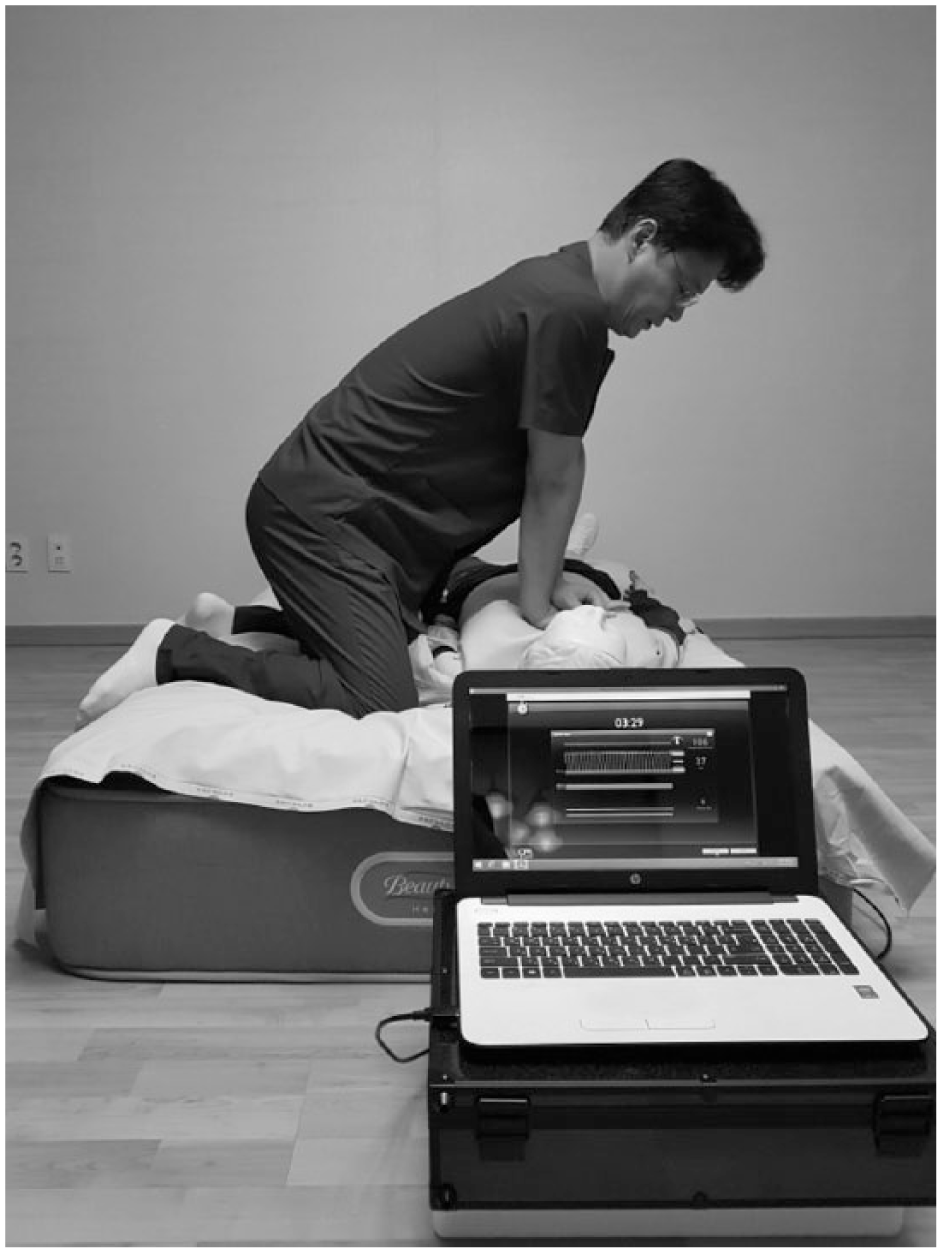
Experimental setup for chest compression on a home-bed mattress.
Outcome measures
Data on CC depth, rate and chest recoil were obtained from the Resusci Anne Simulator® using the Laerdal® PC Skill Reporting System (Laerdal Medical, Stavanger, Norway). CC was considered accurate when the compression depth was 5–6 cm, the compression rate was 100–120 compressions/min, and there was complete chest recoil. After 4 min of CC, bystander fatigue was measured using the rating of perceived exertion (Borg 9 scale). Physiological variables (blood pressure, heart rate and oxygen saturation) were measured before and after the bystander performed CC.
Data analysis
CC depth and rate, chest recoil, and bystander fatigue values for the four surfaces were compared, and variations in CC depth and rate over time were analysed. The Shapiro-Wilk test was conducted as a normality test for all continuous variables. For the multiple comparisons of the four surfaces, the normally distributed continuous variables were analysed using one-way analysis of variance and the non-normally distributed continuous variables were analysed using the Kruskal-Wallis test with a post hoc test (Mann-Whitney test after Bonferroni correction). SPSS 19.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis of all data.
Results
Thirty participants (15 males and 15 females) were enrolled. The characteristics of the participants are shown in Table 1.
Demographic characteristics of participants.
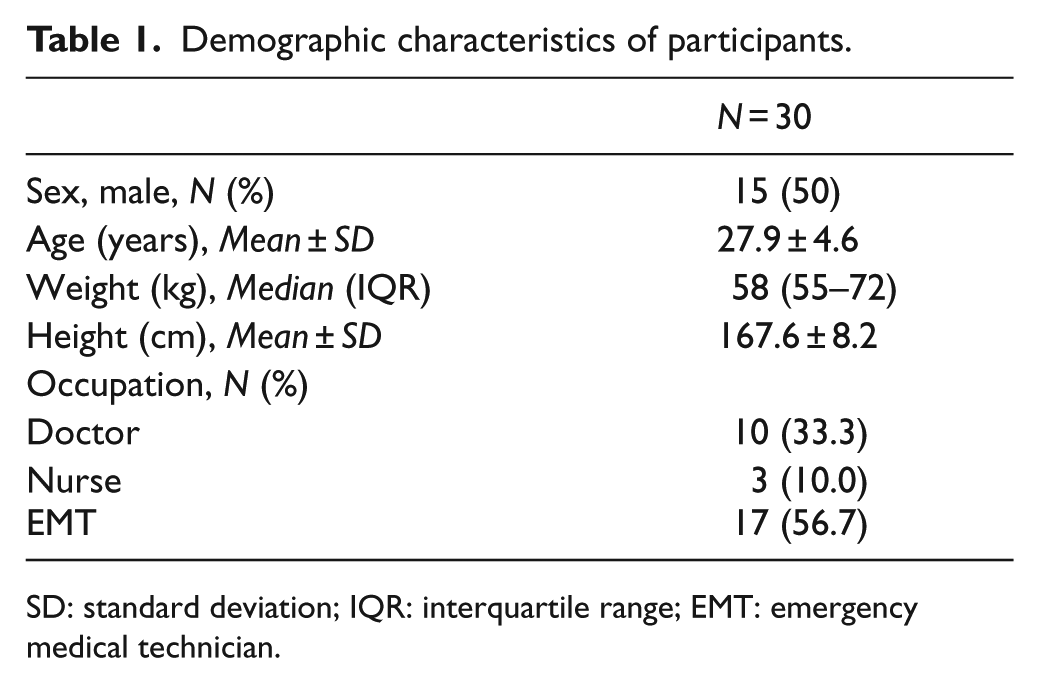
SD: standard deviation; IQR: interquartile range; EMT: emergency medical technician.
The physiological variables before and after CC did not show any significant differences (Table 2).
The physiological variables before and after chest compression for participants.
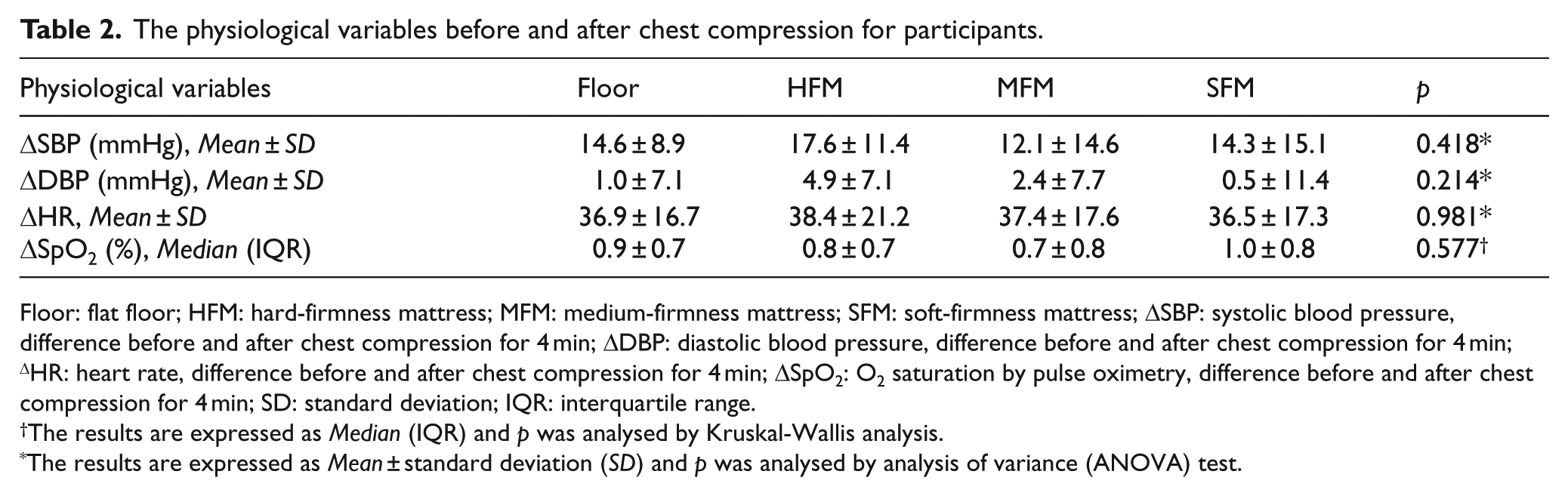
Floor: flat floor; HFM: hard-firmness mattress; MFM: medium-firmness mattress; SFM: soft-firmness mattress; ΔSBP: systolic blood pressure, difference before and after chest compression for 4 min; ΔDBP: diastolic blood pressure, difference before and after chest compression for 4 min; ΔHR: heart rate, difference before and after chest compression for 4 min; ΔSpO2: O2 saturation by pulse oximetry, difference before and after chest compression for 4 min; SD: standard deviation; IQR: interquartile range.
The results are expressed as Median (IQR) and p was analysed by Kruskal-Wallis analysis.
The results are expressed as Mean ± standard deviation (SD) and p was analysed by analysis of variance (ANOVA) test.
There were also no significant differences in the median CC depth and depth accuracy between the four surfaces (Table 3). The median CC rates were 108.1 ± 8.5, 107.0 ± 8.3, 103.3 ± 8.9 and 98.3 ± 7.9 compressions/min (p < 0.001) for the floor, hard-firmness mattress (HFM), medium-firmness mattress (MFM) and soft-firmness mattress (SFM) (Table 3), respectively.
Quality of chest compression on four different surfaces.
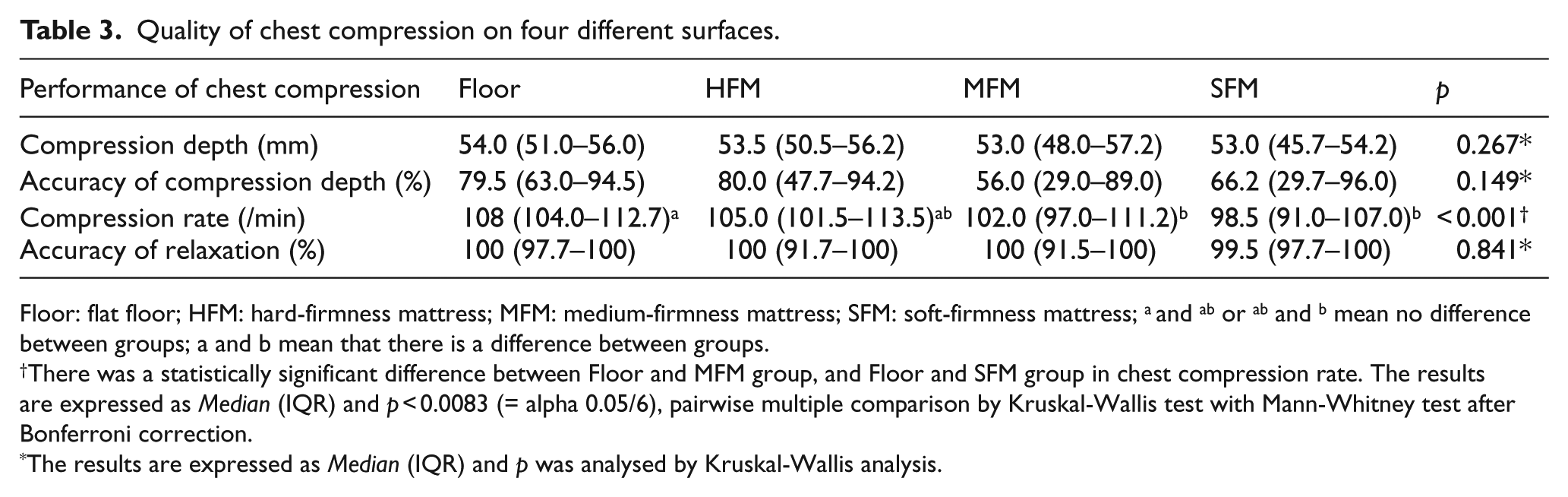
Floor: flat floor; HFM: hard-firmness mattress; MFM: medium-firmness mattress; SFM: soft-firmness mattress; a and ab or ab and b mean no difference between groups; a and b mean that there is a difference between groups.
There was a statistically significant difference between Floor and MFM group, and Floor and SFM group in chest compression rate. The results are expressed as Median (IQR) and p < 0.0083 (= alpha 0.05/6), pairwise multiple comparison by Kruskal-Wallis test with Mann-Whitney test after Bonferroni correction.
The results are expressed as Median (IQR) and p was analysed by Kruskal-Wallis analysis.
There were no significant differences in chest recoil accuracy (Table 3).
For the four different surfaces, there were no significant differences in CC depth over time, but CC depth decreased significantly after 3 min (Table 4).
The change in chest compression depth and rate during 4 min period on four different surfaces.
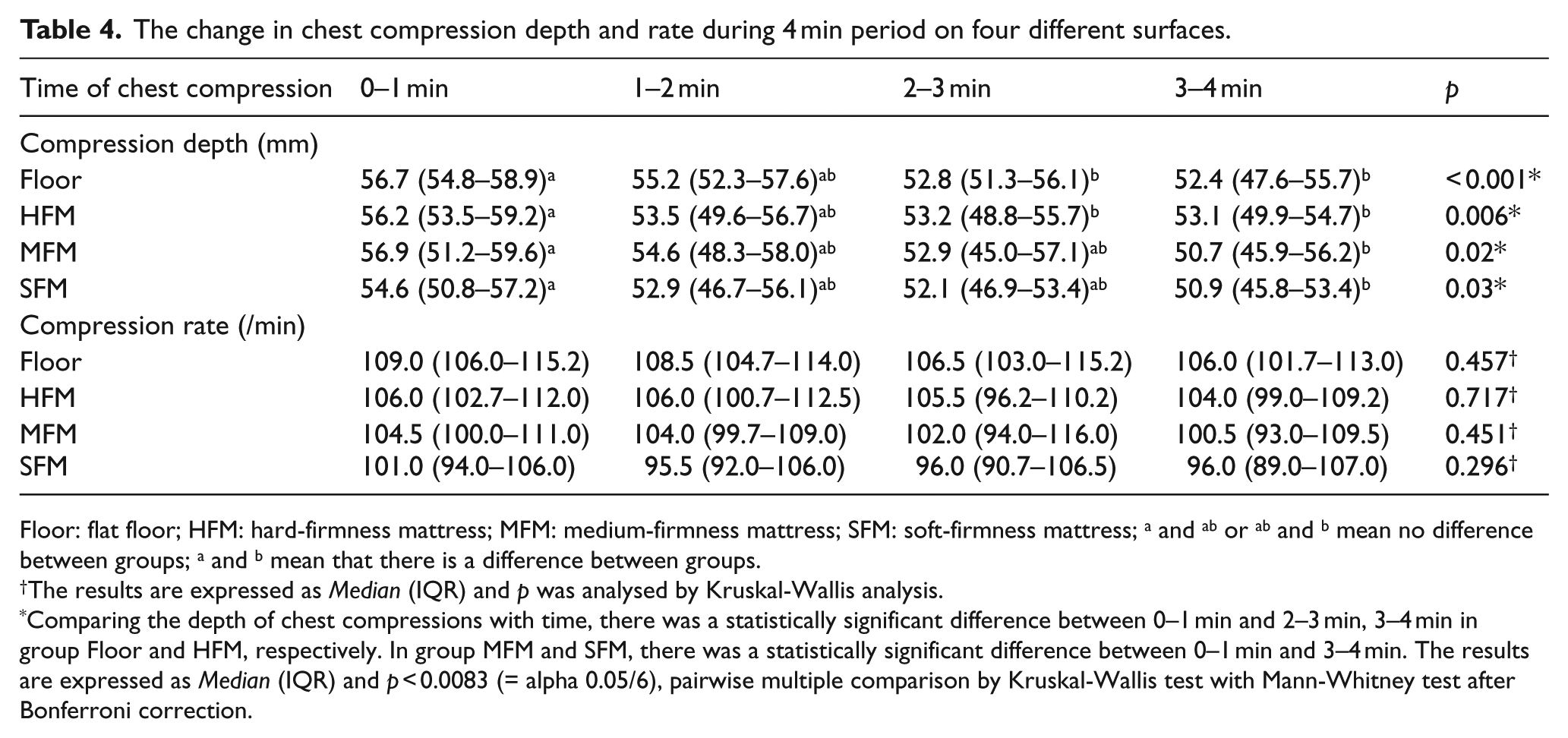
Floor: flat floor; HFM: hard-firmness mattress; MFM: medium-firmness mattress; SFM: soft-firmness mattress; a and ab or ab and b mean no difference between groups; a and b mean that there is a difference between groups.
The results are expressed as Median (IQR) and p was analysed by Kruskal-Wallis analysis.
Comparing the depth of chest compressions with time, there was a statistically significant difference between 0–1 min and 2–3 min, 3–4 min in group Floor and HFM, respectively. In group MFM and SFM, there was a statistically significant difference between 0–1 min and 3–4 min. The results are expressed as Median (IQR) and p < 0.0083 (= alpha 0.05/6), pairwise multiple comparison by Kruskal-Wallis test with Mann-Whitney test after Bonferroni correction.
The participants showed less fatigue when CC was performed on the floor than on the mattresses (p = 0.003, Table 5).
Comfortability and Borg scales of performing chest compression on four different surfaces.
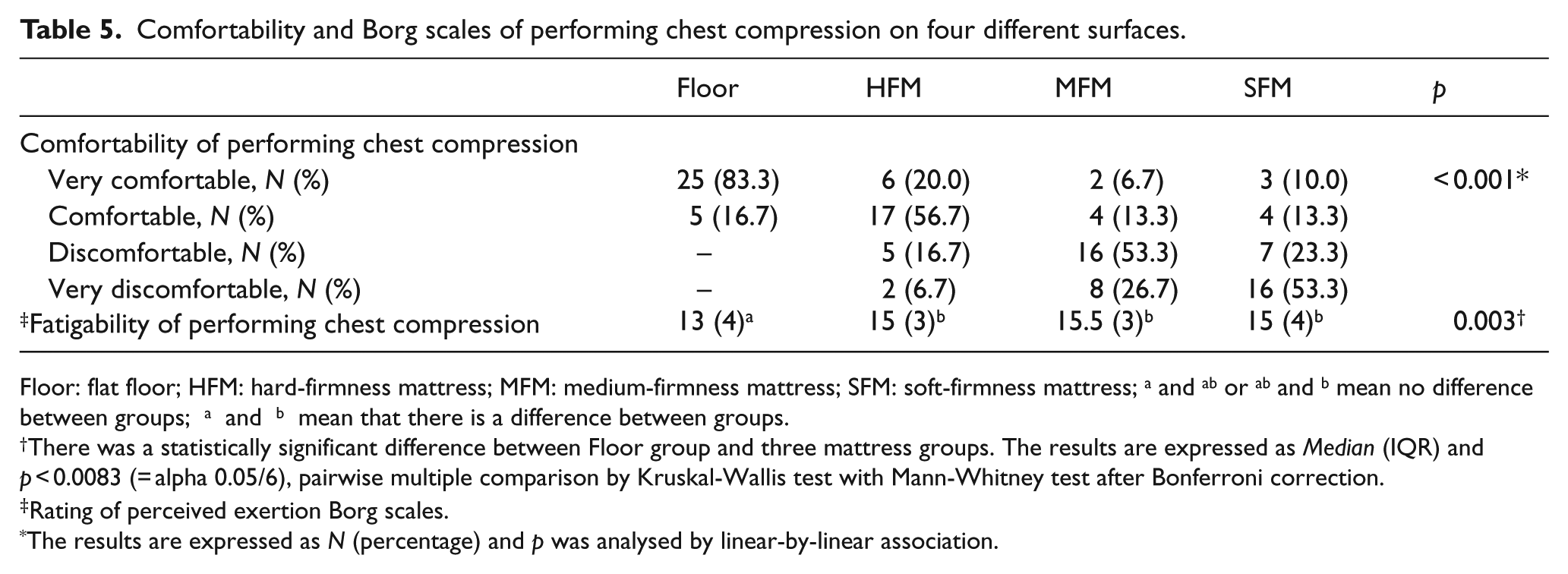
Floor: flat floor; HFM: hard-firmness mattress; MFM: medium-firmness mattress; SFM: soft-firmness mattress; a and ab or ab and b mean no difference between groups; a and b mean that there is a difference between groups.
There was a statistically significant difference between Floor group and three mattress groups. The results are expressed as Median (IQR) and p < 0.0083 (= alpha 0.05/6), pairwise multiple comparison by Kruskal-Wallis test with Mann-Whitney test after Bonferroni correction.
Rating of perceived exertion Borg scales.
The results are expressed as N (percentage) and p was analysed by linear-by-linear association.
Discussion
In the event of an OHCA, the 2015 American Heart Association Guidelines recommend that the victim be laid on a flat floor before the bystander can perform CPR. However, there are barriers that prevent bystanders from initiating CPR, such as stress/emotion, fear of harming the patient, inability to do the procedure and difficulty in moving the patient, the last being the most common barrier. 4 Bystander CPR is a key factor for the survival of a victim before the EMS arrives.1,2 The survival rate for OHCA has increased with increased incidence of bystander CPR through CPR training.10,11 A nationwide study in Denmark reported that after an implementation of mandatory resuscitation training, bystander CPR incidence increased from 21.1% in 2001 to 44.9% in 2010, and the 30-day survival rate also increased from 7.9% to 23.8%. 12
There are cases when the bystander cannot move the victim to a flat floor, so the bystander must perform CC on a home-bed mattress while waiting for the EMS to arrive. This might be beneficial for reducing no-flow times.
Previous studies have reported that CC on a hospital-bed mattress reduced the CC depth and increased the fatigue of the provider.13–15 To prevent the adverse effects of a hospital-bed mattress on CC, the use of a backboard, mattress compression cover and vacuum pump has been studied.16,17 However, Nishisaki et al. 18 suggested that a backboard should be used for CPR only in paediatric beds and soft beds of the intensive care unit, whereas other studies reported that the firmness of the surface had no significant effect on CPR.5,6 In our study, there were no significant differences in CC depth between the flat floor and the three types of home-bed mattresses.
A study by Gyllenborg et al. 19 on bystander CPR using public automated external defibrillators found that the median CC depth within the guidelines was 26% and the CC rate was 42%. In our study, as the firmness scale of the mattress increased, the CC depth decreased more than that when the manikin was on the floor; however, we did not observe any significant difference. The median accuracy rates of CC depth within the guidelines were 79.5%, 80%, 56% and 66.2% for the floor, HFM, MFM and SFM, respectively, whereas the CC rates were 76.7%, 83.3%, 60% and 43.3%, respectively. These results indicate that the differences in home-bed mattress firmness did not significantly influence the CC quality. In a previous study, a slow rebound of the home-bed mattress increased its neutral position and the time cycle during CC. 15 This slow rebound caused the CC rate to slightly decrease. Moreover, bystander fatigue was higher when performing CC on the SFM than on the flat floor.
CPR quality may decline over time due to the rescuer’s fatigue and unawareness of poor CC performance.20,21 Meanwhile, DA-CPR improved the quality of bystander CPR, including the recognition of cardiac arrest, time to initiating CC, time to defibrillation and survival rate for OHCA.4,22,23 During DA-CPR, the recognition of cardiac arrest and CC were reported to improve to 95% and 83%, respectively, and the time to initiating CC was reduced to 2.8 min. 24 Moreover, continuous coaching for DA-CPR has helped bystanders perform CC properly. 25 As mentioned above, our study revealed that bystander fatigue was higher with using the SFM than with using the flat floor. Thus, bystanders need encouragement in increasing CC depth and rate through DA-CPR to help prevent the adverse effects of using home-bed mattresses.
This study has some limitations. First, it was conducted on a manikin; hence, our data cannot be well extrapolated to all patients. Second, we used only three types of mattresses according to firmness to evaluate CC quality. Finally, CC was performed by healthy young adults, without considering age, sex, race, education or body mass index, so the results may not be generalizable to all bystanders. We therefore recommend clinical studies or further study on variations in CC quality by considering more types of home-bed mattresses and the physical conditions of the bystander.
Conclusion
Our study revealed that CC performed on HFM and MFM did not decrease the CC quality, compared to CC performed on a flat floor. However, in SFM, participants were delivered poorer CPR quality regarding compression rate by slow rebound of mattress. Thus, bystanders need encouragement in increasing CC depth and rate through DA-CPR to help prevent the adverse effects of using home-bed mattresses.
We recommend that CC can be effectively initiated on a home-bed mattress with DA-CPR if the bystander cannot move the patient to the flat floor for reducing no-flow times.
Footnotes
Acknowledgements
The authors thank all the participants who participated in this study.
Author contributions
Research conception and design were done by Y.C., H.J.A. and Y.H.Y. The experiments were performed by Y.C., H.J.A., J.H.M. and W.J.J. Data acquisition was done by Y.C., H.J.A. and S.R. Data analysis and interpretation were done by Y.C., H.J.A. and J.W.L. Statistical analysis was done by Y.C., H.J.A. and S.U.C. Drafting of the article was done by Y.C., H.J.A. and S.K.O. Critical revision of the article was done by Y.C., Y.H.Y. and J.S.P. All authors reviewed and edited the article and approved the final version of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and material
The data set used and analysed during this study is available from the corresponding author on reasonable request.
Informed consent
Written informed consent was obtained from the participants for their anonymized information to be published in this article.
Ethical approval
The study was approved by the institutional review board of the hospital (IRB no. CNUH 2018-11-065).