
Abstract
Introduction
We have all likely heard the expression that ‘time heals all wounds’. Since the 1300s, time has been identified as an important factor in healing, even being described as the ‘great physician’. 1 While writers and poets have focused largely on the healing of emotional wounds over time, paramedics and physicians have observed that time is an important factor in the care of acutely injured and ill patients. 2 In fact, the need to reduce time from physiologic insult to intervention was how paramedicine began – medicine needed someone who could respond quickly in the community to provide immediate care and transport, especially in conditions such as out-of-hospital cardiac arrest. 3
One may argue that this need to reduce time to treatment forms an important part of our professional identity, 4 and indeed most of us can think of an instance when time did matter – when the time it took us to gain access to a patient and apply some sort of airway, breathing or circulatory intervention literally made the difference between continued life and immediate death. On the other hand, we can also think of many more instances where it mattered less. Yet many systems use time, specifically response time in all its various definitions, as a prominent measure representing quality of service.5,6 However, anyone who has ever ordered food knows fast service doesn’t matter if the food's awful. To translate this concept to paramedicine, responding quickly may be important in some events, but the quality of the care that we provide is important in all events.
As emergency telecommunicators and paramedics we know intuitively that other factors are central to providing quality care in addition to time, such as how competent we are at performing a particular assessment or intervention, whether we have the right equipment, if our equipment is in good working order, whether we have a trustworthy partner, or enough resources on-scene, and if we are in the right physical or emotional state.
Recently, the Paramedic Chiefs of Canada, in collaboration with other largely North American paramedicine related organisations including the American Ambulance and Paramedic Associations, released a joint statement encouraging ‘emergency medical services (EMS) systems and community leaders’ to utilise patient-centred measures describing clinical, operational, financial, experiential and equality and safety aspects of service provision. 7 In other words, to move away from the utilisation of time to service as the most prominent measure of service quality.
In this editorial, we aim to explore what quality means in paramedicine, what currently exists for measures of quality, and the critical need for further knowledge creation and translation in this area.
The language of quality
Before we can discuss measures of quality, we can’t emphasise enough the importance of having a common language. Creating mutual nomenclature and shared understanding amongst healthcare professionals, regulators and stakeholders can contribute towards ensuring consistency in defining, measuring and interpreting healthcare quality and performance. Ultimately this common language will allow for effective comparisons and benchmarking across different services and systems. 8
A quality indicator is ‘a measurable element of practice performance for which there is evidence or consensus that it can be used to assess the quality, and hence change in the quality, of care provided’. 9 (p. 104) As such, quality indicators specify quantifiable aspects of healthcare provision that can serve as a tool to monitor, evaluate, and ultimately assist with improvements in the quality of patient care, clinical support services or organisational functions that influence patient outcomes.
Different organisations and individuals may use terms differently and thus the terms quality indicator and performance indicator are often used interchangeably. However, quality refers to the concept that describes the degree of excellence in patient care and aims to achieve best possible patient outcomes. The concept of quality includes dimensions such as safety, effectiveness and patient-centredness. Performance, meanwhile, focuses more on how well healthcare services are executed, often relating to productivity, processes, adherence to standards and efficiency.
Inherently, quality indicators infer a judgment about the quality of care provided (such as 12-lead ECG in patients with suspected ST-elevation myocardial infarction (STEMI)), while performance indicators are statistical tools used to monitor performance (such as unit hour availability (UHA))) without necessarily inferring anything about the quality of that care. 10 Confusion also exists around the terms ‘indicator’, ‘measure’ and ‘standard’. It is important to understand that an indicator suggests the relevant attribute without being a direct measure, whereas a measure facilitates quantifying what is being assessed. 11 In healthcare, indicators are often transformed into measures which, especially when paired with standards, can be used to evaluate the quality of care and service delivery (Table 1).
Example of a quality indicator, quality measure, and quality standard.
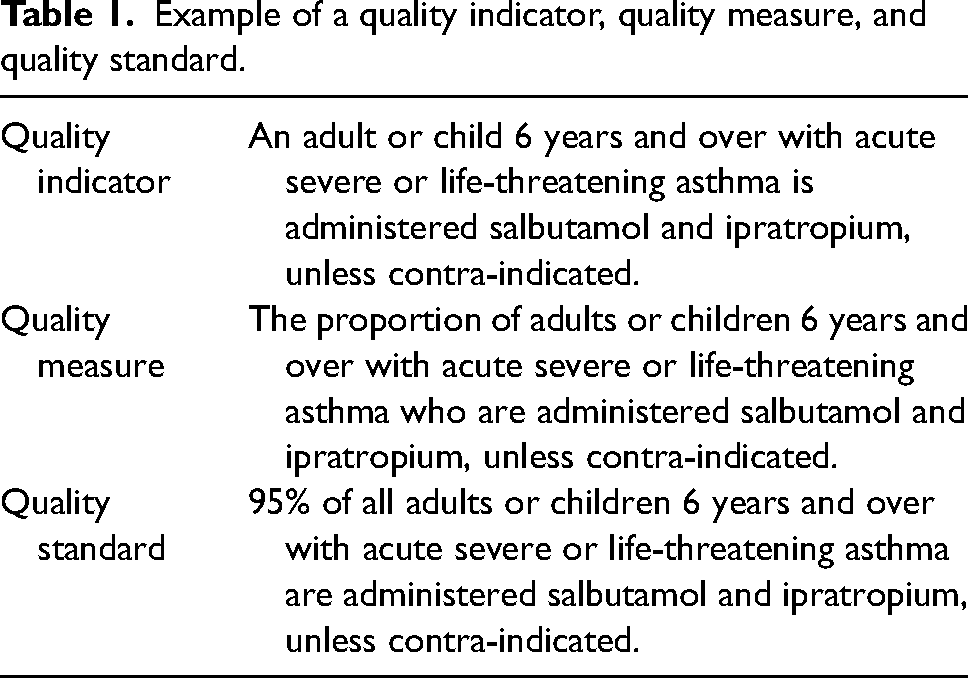
A useful quality indicator possesses several desirable characteristics such as being important to users, valid and evidence-based, utilising reliable data, statistically robust, simple to understand and remediable. 12 While individual quality indicators assess a specific element of quality (e.g., the administration of bronchodilators in acute asthma), those using these quality indicators, such as healthcare providers, patients and policymakers, are often interested in evaluating a broader area (e.g., overall quality of acute asthma care), which necessitates utilising a set of several quality indicators. Similar, to good individual quality indicators, good quality indicator sets also have desirable characteristics, such as being balanced, cost-efficient and non-redundant, to name a few. 13
Quality indicators and sets typically focus on a particular attribute of care that may align with a framework. Quality frameworks rely on measurements to assure desired standards of quality or identify areas for improvement, and then track progress over time. Since frameworks typically consider different perspectives on quality, quality indicators and sets need to recognise the unique priorities and needs of various stakeholders, such as providers, patients and policymakers. A common quality framework has been proposed by the Institute of Medicine in the United States, which includes six dimensions: safety, care effectiveness, patient-centredness, timeliness, care efficiency and equity. We could also use the framework proposed in the joint statement described above – clinical, operational, financial, experiential and equality and safety.
The importance of determining what is important
The phenomenon of promoting the measurable as important, rather than making the important measurable is critical for us to appreciate in paramedicine. In other words, just because we can measure something with reasonable validity and reliability, does not mean we should promote it as being universally important. For example, response time, or the time from the emergency call to the arrival of the first response unit on-scene, is widely used as a key indicator of quality and a good example of the challenges that can occur in making the measurable important. 14 The original research that supported the development of an eight minute response time standard measured response time from emergency call to critical intervention in out-of-hospital cardiac arrest (OHCA), 2 yet the definition was changed to first unit arrival on-scene as this was easier to collect in a valid and reliable manner. Moreover, this definition was generalised to all ‘high priority’ events not just OHCA. Subsequent research has called into question this practice from a clinical perspective,15–20 yet many systems are often singularly judged on this quality indicator.
While response times, or similarly on-scene times and transport times, are generally accepted as important clinical indicators in specific time-sensitive conditions, such as STEMI, stroke, major trauma or OHCA,21–24 they are not important in commonly encountered non-time-sensitive patients and do not reflect other dimensions of out-of-hospital patient care, such as clinical appropriateness, safety and patient-centredness. Furthermore, most quality indicators in paramedicine describe a process rather than an outcome. This is partly due to the inherent difficulties in linking out-of-hospital care to long-term patient outcomes due to cost, complexity and access to data. 25
Using outcomes is also challenging due to the influence of confounding and modifying factors outside of the control of the paramedicine system (e.g., differing quality of hospital-based care, severity of injury, etc.), or the potential for bias through incomplete outcome linkage.26,27 Therefore, while it is crucial to ensure that important processes of care are measured, it is equally important to use systematic and evidenced-informed development processes for these process-type indicators so that they have a clear link to meaningful patient outcomes, and of course to continue to build the methodological rigour for outcome measurement in paramedicine.11,28 This includes improved tracking of patients from emergency call to outcome, better risk adjusted models of care and the ability for systems to determine care over time to measure quality interventions. 29
Perspectives on quality
The challenge of defining and measuring quality in paramedicine, and indeed healthcare, is exacerbated by the different perspectives on what constitutes ‘quality’. From a clinician's perspective, the concept of quality is frequently characterised by effectiveness, safety and adherence to evidence-based practices. On the other hand, patients and stakeholders may prioritise social or experiential aspects, and have described the importance of reassurance, which is enhanced through communication and professionalism. 30 When viewing response time from this ‘social perspective’, how long it takes for paramedics to arrive at the patient's side is potentially an important measure – perhaps especially when there is a perceived time sensitive emergency by the emergency caller.15,30
A holistic quality framework and associated suite of quality indicators considers various lenses through which quality may be viewed. Balancing these viewpoints is essential but theoretically challenging – an overly strong clinical focus risks overlooking the importance of patient experience, while a disproportionate focus on patient experience might neglect critical clinical outcomes. In reality, evidence from hospital-based research suggests that clinical safety and effectiveness may enhance patient experience and that patients may have a role to play in improving safety and effectiveness of care. 31
Another challenge is the collection of data to inform these measures, especially for aspects reported by patients or other external stakeholders. Capturing patient-reported outcome measures (PROMs) that measure a patient's self-reported health and well-being, and patient-reported experience measures (PREMs) that measure a patient's self-reported experience of receiving healthcare may be challenged by system, service and provider level barriers. 32 Not only does this increase the financial burden on the service, but it also requires well-developed infrastructures to ensure the data are accurately and consistently captured, analysed and interpreted.32,33 However, in spite of the challenges in capturing patient experience, there is an example of a paramedicine specific PREM developed in the UK.34,35 Both PROMs and PREMs are a critical part of the assessment of quality in health care and a good example of making the important measurable.
Where are we now?
The development of quality indicators and frameworks for paramedicine has been the focus of much research and non-academic efforts, reflecting the growing need to assess and improve how quality can be measured and used for assurance and improvement. Below we briefly describe the efforts of three countries in measuring quality in paramedicine.
Australia
The national evaluation of ambulance service quality is coordinated by the Council of Ambulance Authorities (CAA), which collects and reports data for the Australian Government Productivity Commission's Report on Government Services (RoGS). 36 These data, gathered from the nine statutory Australian ambulance services, covers areas such as revenue, demand and patient care, and are used to create benchmarking reports that assess service performance. 36
A performance indicator framework is employed that distinguishes between the outputs (services delivered) and outcomes (the impact of these services) to evaluate equity, effectiveness and efficiency. Notwithstanding continuous efforts to improve performance reporting, including addressing data gaps and enhancing comparability, the number of indicators remains limited. Most recent data are complete and facilitate comparison of response times, pain management, cardiac arrest survival (defined as return of spontaneous circulation on arrival at hospital), patient satisfaction, and workforce sustainability. In addition, state-based corporations, such as the Bureau of Health Information in New South Wales (NSW), provide independent information about the performance of the public healthcare services including ambulance services, 37 and individual jurisdictional ambulance services develop and utilise their own indicators to facilitate quality assurance and improvement efforts.
There have also been recent research efforts to develop new quality indicators. The AuStralian Prehospital care quality IndicatoR projEct (ASPIRE) was a three-phased research project utilising mixed methods to develop and test prehospital care quality indicators for the Australian setting. 38 Phase 2 of the project used an evidence-informed expert consensus process to assess the validity of a large set of quality indicators previously charted in a scoping review,14,39 and none of the response time indicators were deemed valid by the expert panel. Further recent developments in the Australian context include the publication of a National Safety and Quality Health Service (NSQHS) Standards Guide for Ambulance Health Services by the Australian Commission on Safety and Quality in Health Care. 40 Whilst these do not include specific quality indicators or measures, the NSQHS standards provide robust direction on how to improve the quality of health service provision in Australia by providing clear actions, including the implementation of meaningful measures to monitor performance against the standards.
United Kingdom
In England, recognising the limitations of time measures as a proxy for quality, the National Institute for Health Research commissioned research dedicated to developing new ways of measuring the impact of ambulance service care. The researchers undertook consensus and development work identifying what is important to measure 11 and developed linked datasets to create and test 41 potential measures. From this, the Prehospital Outcome for Evidenced Based Evaluation (PhOEBE) 12 research programme developed a potential set of case-mix adjusted ambulance service quality indicators that were reflective of the current scope of ambulance service care and were important to ambulance services, wider stakeholders and service users.
One of the indicators presented a different way of reporting response time (average response time), that was felt to be more representative of whole service performance and less susceptible to target chasing. Feeding into the Ambulance Response Programme (ARP – a programme of work by the National Health Service [NHS] in England to improve emergency ambulance response performance), 42 led to changes in the way that response time is reported nationally, which are now reported by the mean and 90th percentile response time for each of the ARP call categories. However, without better data sources that are more easily linked, further advances have been limited.
Whilst the PhOEBE programme was ambitious in its outlook, at the same time a focus on what can be currently measured has progressed 43 and for over a decade, data for 11 Ambulance Quality Indicators (AQIs) 44 are routinely provided by all English ambulance trusts to NHS England. These monthly data are published on a national dashboard, providing a constant and consistent source of information. The AQIs cover a range of measures, including time, processes, responses to specific clinical conditions and ambulance responses and outcomes. Although time is considered as part of a suite of indicators, the move away from solely focusing on time has been welcomed. Better access to data that can be used to measure quality and performance in the context of the emergency and urgent care system remains a priority. This is not insurmountable, as Scotland has developed a national linked pathway of patient level data to understand the patient journey from first urgent or emergency care telephone contact to ED admission. 29
United States
In the United States, moving away from the use of response times as the most prominent measure of quality in paramedicine is not a new concept. 6 Similar to Australia and the UK, an organised initiative is making a significant contribution to defining and implementing quality measures. Originating from the EMS Compass Project funded by the National Highway Traffic Safety Administration (NHTSA), the National EMS Quality Alliance's (NEMSQA's) mission is to develop and endorse evidence-based quality indicators for EMS. 45 Currently there are 11 approved indicators that describe care for advanced airway, asthma, hypoglycemia, general respiratory, seizure, stroke, syncope, trauma, pediatrics, non-transport and safety. Future development of indicators will follow a standardised development process that includes research, testing and a public comment period. 45
Conclusions
The recent position statement issued by a consortium of largely North American paramedicine agencies calling for expanded and more holistic measures for paramedicine systems provides an opportunity for pause and reflection on the current state of understanding of quality in our profession and the systems in which we work. In this editorial we have highlighted some of the academic and non-academic work that is being done to this end. While this excellent work has created new knowledge, the currently available measures merely scratch the surface of quality in paramedicine.
The post-COVID reality of many systems necessitates that we expand quality indicators of service beyond that of merely recording time, especially considering global paramedic challenges such as staffing shortages and hospital offload delays to name a few. Moreover, the translation of current knowledge to action, where existing quality indicators, measures, and sets are used and publicly reported is the exception rather than the norm. 46 Initiatives such as the newly formed Prehospital Qualitology Network (https://www.prehospitalqualitology.com), provide hope that the disparate efforts to date, can be joined to offer international collaboration and action to use scientific methods to challenge and improve the systems we work in.
We therefore advocate for paramedicine system leaders, frontline colleagues, patients, and academics to work together and focus on meaningful measurement of quality in our burgeoning profession, so that we can make the important measurable, improve what is important, and demonstrate that paramedicine is more than a means by which to stop a clock.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Pap is an Associate Editor for Paramedicine, but played no role in editorial decision making, which was conducted in adherence to the journal's blind review policy. Dr. Coster and Dr. Blanchard have no conflicts to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.