
Abstract
Introduction
As the paramedic profession continues to grow and evolve, a shift from purely reactive to holistic patient care models is required. As the first and often the only point of medical contact for many patients from marginalised and under-served populations, the paramedic role and its potential future implications in caring for these patients need to be explored.
Aim
The objective of this scoping review was to explore the paramedic's role in caring for people who use illicit and controlled drugs.
Methods
A scoping review of English language literature published since 2002 was conducted using CINAHL, Medline, Embase and Google Scholar. We used a previously published paramedic search term filter for sensitivity combined with search terms related to illicit and controlled drug use and addiction. Studies were selected based on relevance to the research question.
Results
A total of 104 peer-reviewed and 14 grey literature articles were selected for inclusion. The main finding of this scoping review is the notable lack of evidence base surrounding the contemporary paramedic role in the care provision of people who use drugs. The results highlight high rates of mortality following a paramedic-attended drug poisoning event, presenting a unique opportunity for paramedics to approach care in meaningful ways that extend past traditional drug poisoning response.
Conclusions
The interface between the community of people who use drugs and the paramedic may be a highly influential encounter during a patient's journey through the healthcare system. The evolving role of the paramedic in this encounter requires focused study and should be viewed as a research priority in response to the ongoing drug poisoning crisis.
Keywords
Introduction
The international incidence of drug poisoning-related morbidity and mortality is well-documented.1–3 Opioids have been a particular area of focus in the discussion of drug poisoning-related morbidity and mortality due to their significant impact on public health. 4 Opioids are a class of drugs that include prescription painkillers, such as oxycodone, hydrocodone and fentanyl, as well as illicit drugs like heroin. Over the last decade, the use of prescription opioids and the proliferation of illicitly produced fentanyl have led to a staggering increase in opioid-related drug poisoning deaths worldwide.4,5 This crisis has prompted urgent action from healthcare providers, policymakers and researchers to address the issue. Regions identified as suffering from significant impacts, such as North America, have produced a growing body of literature that calls attention to the high incidence of drug poisoning–related deaths secondary to the increasingly toxic supply of unregulated drugs.6–11 In recent years, there has been growing concern over the high incidence of opioid-related drug poisoning deaths in North America. The United States, in particular, has been hit hard by the opioid epidemic, with an estimated 187 people dying daily from opioid-related drug poisoning events. 12 Similarly, in British Columbia, Canada, drug toxicity from illicit substances is now the leading cause of premature death in the province, responsible for more deaths than suicides, homicides, motor vehicle incidents, drownings and fire-related deaths combined. 13 Paramedics play a crucial role in responding to drug poisoning events and providing care to people who use drugs. 14 Given their unique position to provide care in a variety of contexts, including patients’ homes and communities, they may be well-placed to reduce drug-related harm. 15 However, previous research has largely focused on the emergency response to drug poisoning events, with less emphasis on the holistic and preventative role of paramedics in reducing drug-related harms. 16 To address this gap in knowledge, it is essential to explore opportunities as well as the patient experience of paramedic care and how it can influence each encounter.
By better understanding the role of paramedics in caring for people who use drugs, we can develop more effective therapeutics that support patient autonomy and promote positive health outcomes. 17 Paramedics are uniquely positioned to make a significant difference in the lives of people who use drugs. However, this potential impact can only be fully realised if we start to truly understand and appreciate their crucial role. There is a paucity of literature exploring the patient experience of paramedic care for people who use drugs, and how this impacts each interaction.
Objective
The aim of this scoping review was to explore how paramedics provide care to people who use drugs, identify gaps in the literature and recommend areas for further research. 18 A scoping review was chosen as the most suitable methodology to address these research questions, as it enables the mapping of literature in the field of paramedic care for people who use drugs, identification of key concepts, research gaps and sources of evidence that can inform policy making, practice and research. 19 This review sought to answer the following research questions: (1) What is currently known about the paramedic role in caring for people who use drugs? (2) What are the current gaps in the literature related to this topic? and (3) How can the findings of this review inform contemporary and future paramedic practice? The study population consisted of people who use both illicit and controlled drugs, including the non-medical use of prescription medication. To ensure that the literature search was comprehensive, the search terms were selected to include stigmatising language that is no longer accepted as person-centred (see Appendix 1) and was informed by a list of suggested search terms related to addiction. The review included paramedic-delivered care in both acute and non-acute settings, such as the home, mobile integrated health response and safe consumption sites. The review encompasses the entire scope of the paramedic profession, including all levels of practice, settings and contexts.
Language
The authors recognise the importance of language in describing substance use and the population of people who use drugs in the literature.20,21 To ensure the language within this manuscript is consistently person-centred and trauma-informed, some terminology may have been changed to reflect the most currently accepted language within the community of people who use drugs. Examples include changing ‘addicts’ to ‘people who use drugs’ and ‘substance abuse’ to ‘substance use’.
The authors further recognise that although not all geographic areas throughout the world are experiencing ‘toxic drug’ crises, the predominant literature that met inclusion criteria was produced from the United States which has been experiencing an increasingly pronounced surge in drug poisoning deaths as a result of a drug supply that is contaminated by synthetic opioids and non-opioids alike including adulteration or complete substitution. 20 For consistency, and to incorporate variances in terminology, ‘drug poisoning’ and ‘drug poisoning crisis’ will be used to represent what was traditionally known as ‘overdose’ and ‘overdose crisis’. 22 The purpose of doing so is to reduce the stigma associated with the term ‘overdose’ which may suggest that a person knowingly took too much of a drug, which may conceal factors that could have perpetuated the event such as social isolation, lack of access to harm reduction supplies and the contaminated drug supply as examples.
The authors acknowledge that paramedics care for people who use non-illicit and controlled drugs that were not included in the review (e.g., caffeine and cannabis). For the purposes of the review, and to accurately reflect the inclusion criteria, ‘illicit and controlled drugs’ is used throughout which includes the use of opioid and non-opioid drugs that may be prescribed or non-prescribed. 23
Methods
The scoping review was conducted in accordance with JBI Scoping Review Guidance. 24 The protocol was created in March 2022 and later registered with the Open Science Framework (https://bit.ly/3V32ehD). We reported our process and findings according to the PRISMA Extension for Scoping Reviews. 25 No ethics approval was required for this scoping review as no human participants were involved.
A preliminary search of Medline, PROSPERO, the Cochrane Database of Systematic Reviews and JBI Evidence Synthesis was conducted to prevent duplication of effort, and no current or in-progress systematic or scoping reviews on the topic were identified.
Identification of relevant studies
The search strategy aimed to locate both peer-reviewed and non-peer-reviewed studies. Only articles published at the time that this review was completed were included in this study. An initial limited search of Medline and CINAHL was undertaken to identify articles on the topic. The text words contained in the titles and abstracts of relevant articles, and the index terms used to describe the articles were used to further inform the search strategy keywords. The search strategy, including all identified keywords and index terms, was further adapted for each database and/or information source (see Appendix 1).
We searched Embase via Ovid, CINAHL via EBSCO and Medline via Ovid in April 2022 with supplemental searches in June 2022. We searched for grey literature by screening the first 1000 results returned by the search engine Google, as well as the first 1000 results from Google Scholar. 26
Study selection
Peer-reviewed empirical studies of any design as well as grey literature were selected if the study objective or articles’ body discussed the care of people who use drugs from an out-of-hospital and paramedic-focused perspective. Articles were eligible for inclusion if they pertained specifically to the paramedic's role in caring for people who use drugs and were published in English since 2002. This limit was set with the aim of appreciating the evolution of the paramedic role by capturing the past two decades and was informed by the literature related to the drug poisoning crisis. Articles were excluded if their primary focus was isolated alcohol use, suicidality related to drug toxicity, excited delirium, clinical drug efficiency, occupational risks to providers, substance use by paramedics, non-illicit drug poisonings, ethnography of people who use drugs or geospatial analyses. Although these areas intersect with the drug poisoning crisis in salient ways, they do not inform the research questions posed.
The review process consisted of two levels of screening: first, a title and abstract review, and second, a full-text review. For the first level of screening, a title/abstract screening form was developed by the primary author (JB) informed by the JBI Scoping Review guidance, 24 using Covidence (Veritas Health, Melbourne, Australia) and reviewed by two co-authors (RA and AB). The screening criteria were tested on a sample of abstracts prior to beginning the abstract review to ensure that they were sensitive enough to capture any articles that may relate to the review question. Conflicts were resolved by discussion with co-authors and criteria were refined until agreement was reached.
In the second step, four of the authors (JB, MOT, ML and RA) independently assessed the full texts of screened articles in duplicate to determine whether they met the inclusion/exclusion criteria.
Data charting
Data were extracted by at least one reviewer (JB, MOT, ML or RA), using a data extraction form created by the primary researcher (JB), informed by the JBI Scoping review guidance 24 (see Appendix 2). Informed by restricted review methodology, 27 a 20% quality check was then completed by the most experienced reviewer (AB) who did not partake in the data extraction stage. Data extracted included article title, author name and year of publication, country of study, study aim/objective, study design, key findings in the study results, discussion, conclusions about the paramedic role and iterative categorisation. The extracted data were exported from Covidence into Excel 365 (Microsoft, Redmond, WA) for collation, analysis and synthesis.
Collating, summarising and reporting results
Extracted data were organised and used to report on the included articles’ findings. Descriptive statistics were used to report the occurrence of concepts, characteristics and populations. We further conducted a descriptive qualitative content analysis of study characteristics to explore, summarise and report qualitative data. 28 We performed this via basic-level inductive coding, whereby papers were categorised based on their principal issue. 29 This was performed independently by two authors (JB and AB) in Covidence, and any discrepancies were then resolved via discussion. Codes were combined into organising categories as appropriate to facilitate summary and discussion. We report both measures and descriptions to quantify and explore the characteristics of the literature.
Trustworthiness and rigour
In addition to the steps outlined to ensure rigour in the scoping review screening and extraction process, we aimed to ensure trustworthiness in our analysis of the included studies. 30 Data were extracted directly from Covidence, reducing the chance of transcription errors. We aimed to ensure credibility and confirmability by performing multiple in-depth searches of the literature and using an inductive approach to our descriptive qualitative content analysis. This allowed the literature to guide the categories rather than applying a-priori categories. 29 We aimed to ensure transferability by exploring literature on a global scale, thereby accounting for a wide variety of contexts. Dependability was ensured through protocol publication, a clear audit trail and multiple author reviews of data throughout the study.
Results
Identification of potential studies
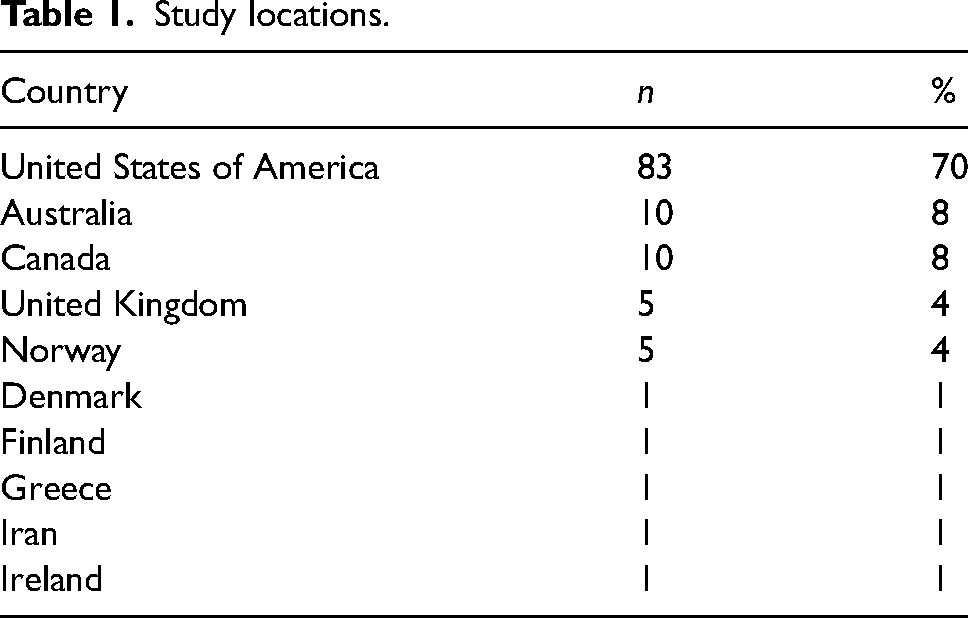
Searches from three databases yielded a total of 5332 records (Embase: 1,943, CINAHL: 1,765, Medline: 1530) which led to the removal of 1569 duplicates. The remaining 3967 abstracts were screened (see Figure 1). A manual search of Google Scholar and Google yielded 204 grey literature articles for abstract screening. The full-text screening phase led to the inclusion of 104 peer-reviewed and 14 grey literature articles. Most studies included in this review were from the USA (n = 83), followed by Australia (n = 10), Canada (n = 10) and the United Kingdom (n = 5) (see Table 1).
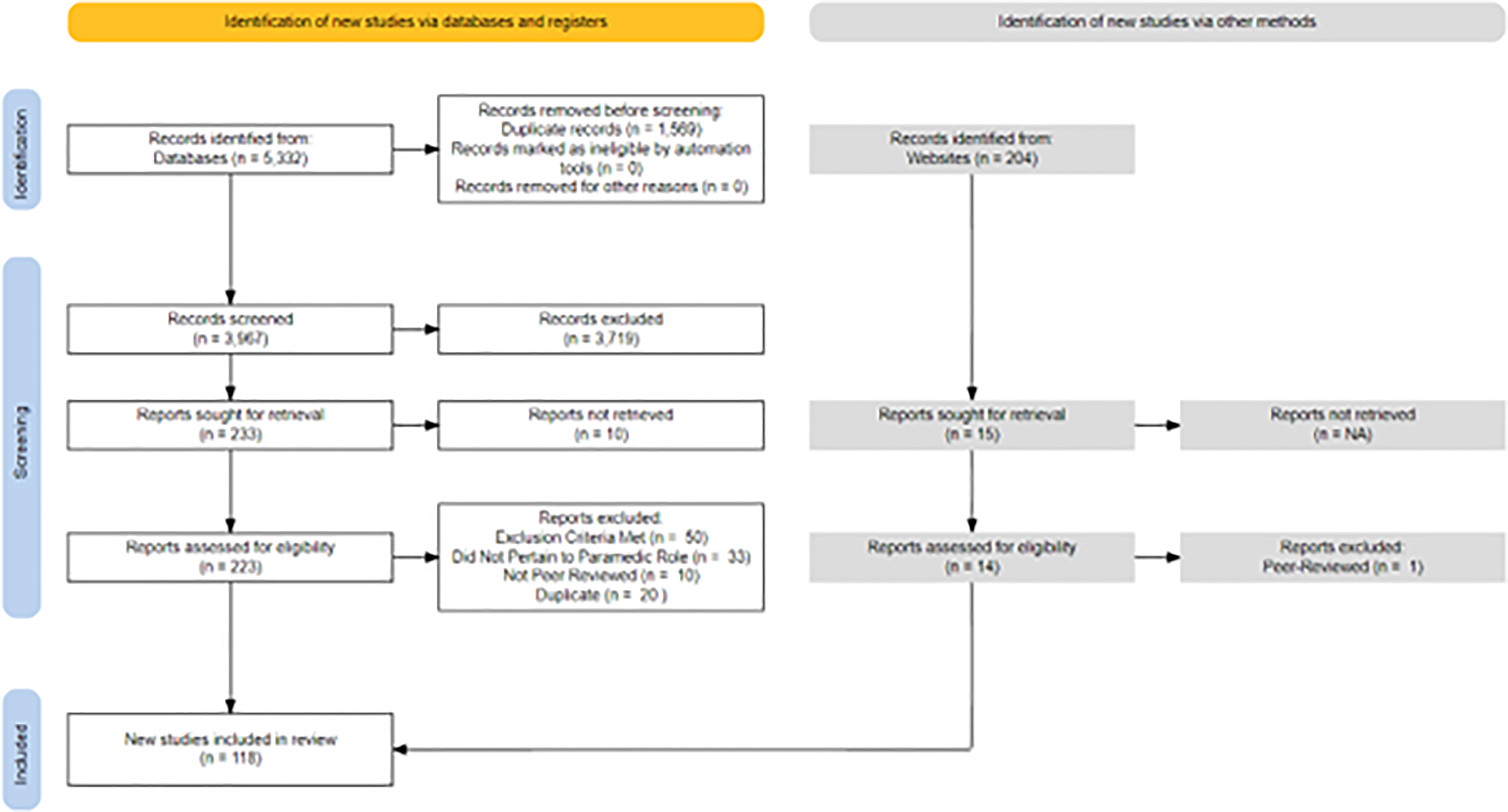
PRISMA diagram.
Study locations.
The prevalent methodology utilised in the included peer-reviewed articles was retrospective chart analysis (n = 46), followed by qualitative analysis (n = 21), literature review (n = 10), prospective cohort studies (n = 9), non-randomised control trials (n = 5), randomised control trials (n = 4), mixed methods (n = 3), editorial (n = 2), consensus guideline (n = 1) and case series (n = 1). Of the included studies, a small number incorporated the perspectives of people who use drugs (n = 3). Full study characteristics can be found in Appendix 3. The majority of included studies were published in the last decade. In 2021, most studies were conducted (n = 21), and prior to 2017, less than 10 studies per year were produced (see Figure 2 and Appendix 4). The practice settings discovered were predominantly acute ambulance care (n = 97); however, other settings included community paramedicine (n = 4) and mobile integrated health models (n = 3).
The majority of the included literature focused on people who use opioids (n = 100). Four areas of research attention were iteratively identified in this review via content analysis: (1) naloxone access and utilisation in the prehospital setting; (2) mortality trends and safety of discharge on scene; (3) the expanding opportunities for paramedic-led harm reduction, and (4) the empathy and attitudes of paramedics and paramedic students.
Naloxone access and utilisation in the prehospital setting
Naloxone access and utilisation were the predominant category of research attention in this review, with 38 articles included, 29 of which were from the USA. Several studies focused on paramedic utilisation of naloxone, all of which concluded that naloxone is a safe and effective treatment that should be accessible to all levels of care.31–35 Twenty-six articles pertaining to the dose and route of paramedic naloxone administration were included.15,36,37 Dose-related themes included the sharp increase in which paramedics are administering multiple doses of naloxone.38,39 Findings suggest that one large intramuscular (IM) (1.6 mg) or intranasal (IN) (2 mg) dose may be sufficient in reversing an opioid-related drug poisoning event, where less than 10% required subsequent dosing upon arrival at the emergency department. 40 With respect to adverse effects, lower dosages of 0.4 mg IM/IN appear to cause less unpleasant symptoms associated with acute withdrawal and have similar effectiveness to higher IN/IM doses. 41 Relating to sex, paramedics were 18% less likely to administer naloxone to women experiencing a drug poisoning event than their male counterparts. 42
Naloxone route of administration studies focused on the IN route as an efficient, safe and needleless alternative to parenteral administration, highlighting the nasal cavity as being readily available, pain-free and faster.43–46 Several included studies demonstrated IN was effective in reversing 74–93.65% of cases, despite the likelihood of requiring re-dosing which was higher than in IV administration.47,48 Despite the incidence of re-dosing, cases of complete reversal after one IN dose remained as high as 91% in some studies. Further, the decision to re-dose based on qualitative analysis appears to be subjective and may reflect the practitioner's reluctance to wait for the desired effects of the drug to take effect. 37
Mortality trends and safety of discharge on scene
Safety of discharge on scene and mortality trends following an out-of-hospital drug poisoning event was the second most researched category discovered in this review. Twenty-seven articles were included for data extraction, predominantly from the USA (n = 18). Twelve studies involved the evaluation of mortality trends following an out-of-hospital drug poisoning at as short as 12 h and as long as 5 years following the initial encounter. Included articles outlined that mortality following a treated out-of-hospital drug poisoning is more likely due to subsequent use rather than rebound toxicity. Historical consensus exists that discharge on the scene following a drug poisoning event is safe. 49 However, contemporary studies have shown that the same-day mortality rate after paramedic naloxone administration is as high as 6.5% (n = 787), 46 while the three-day mortality rate is as high as 8.3% (n = 807). 50 Additionally, mortality risk increases ten-fold at 30 days after drug poisoning and continues to rise thereafter. 51 Multiple studies have examined one-year mortality rates following naloxone administration by paramedics and have found them to be substantially higher. 52 The incidence of death one year after naloxone administration ranged from 9.9% 52 to 15.5%. 53
Expanding opportunities for paramedic-led harm reduction
Three major paramedic-led harm-reducing initiatives included in this review were (a) alternative care pathways, (b) paramedic delivered take-home naloxone, and (c) paramedic-initiated opioid agonist therapy (OAT). Nineteen articles discussed novel and holistic approaches to care, sixteen of which were from the USA. Emerging evidence indicates that paramedics can help address the crisis by potentially preventing drug poisoning events before they occur.54,55 Several included studies in this review conclude that paramedics are uniquely positioned to offer alternative care pathways that reduce and prevent drug-related harm.56,57
In addition to alternative care pathways, Naloxone Leave Behind (NLB) programs were reported as promising. Despite some barriers, notable findings included that patients who were offered and accepted a kit were 2.47 times more likely to seek out support services than those that did not accept a kit, and 5.6 times more likely to seek out services when their family was given the NLB kit. 58 In areas where naloxone is left behind, there was as high as a six-fold likelihood of naloxone being administered prior to paramedic arrival. 59
Opioid agonist therapy is described in this review as an emerging novel treatment option for paramedic care of people who use drugs. Although results are limited, early findings from prehospital OAT trials have been promising, illustrating that 100% of patients who were administered prehospital buprenorphine had an improvement in their opioid withdrawal symptoms, and many remained engaged in OAT at 30 days.60,61 Although buprenorphine is reported as a good ‘first step’, the emphasis reported in these studies remains on the days following the initial administration of OAT, ensuring patients are connected to continuing treatment and or support services. 62
Further harm reduction opportunities for paramedics identified in this review include specialised community paramedicine.63,64 Community paramedicine has become a highly effective vehicle for harm reduction offering many opportunities for harm reduction including education on needle use, follow-up care following a drug poisoning and widespread naloxone education and distribution. 17
Empathy and attitudes of paramedics and paramedic students
A total of seven studies investigated paramedic and paramedic students’ attitudes and empathy towards their role in caring for people who use drugs. Regarding out-of-hospital harm reduction initiatives, paramedic attitudes towards them were polarised, with some refusing to participate in programs altogether. 65 Of all patient demographics, substance use was associated with the lowest mean empathy scores by a large margin for paramedic students.66–70 Some students went as far as relaying a perception that people who use drugs are unworthy of medical treatment, and a burden on the medical system. Further reported is the degree to which student empathy levels appear to decline (in general) over the course of their education, whereas students with previous addiction and substance use education were significantly less likely to stigmatise this population. 68
Five major themes identified by a study of paramedic attitudes in Vancouver, BC, included: connecting with patients’ lived experiences; occupying roles as clinicians and patient advocates; navigating on-scene hazards; difficulties with transitions of care; and emotional burden of the drug poisoning crisis. 71 The core category discovered from this study was one's capacity to help, identified by a limited capacity to follow up on patients, to emotionally process stressful encounters and to address the needs of a patient who experiences a drug poisoning event. Despite paramedics feeling highly confident in their role as clinical care providers, their capacity to treat the underlying drug use is described as much more limited.
Discussion
This scoping review sought to explore what is known about the paramedic role in caring for people who use illicit and controlled drugs and the corresponding research focus areas that exist within the literature. We identified 118 articles from 10 countries between 2002 and 2022.
Our findings illustrate that people who experience an out-of-hospital drug poisoning have extremely high mortality rates, and the literature is largely focused on responsive models of patient care. Categories of research attention discovered in this review focused on acute management and the unmet health needs of this population. Despite calls for a move towards more holistic care, 72 little guidance on how paramedicine may transition to such models of care was discovered. We identified patterns of student and provider-based stigma associated with drug use, and diverging perspectives of harm mitigation among paramedics, which present a barrier to implementing harm reduction programs. Finally, and perhaps of greatest concern, our study revealed a significant lack of engagement with the perspectives of people who use drugs in the existing literature.
The traditional role of the paramedic at a drug poisoning event is a responsive and reactive one, focused on emergency response, resuscitation and reversal of the opioid toxidrome specifically. Although opioids remain at the epicenter of drug poisoning crises in most areas, literature surrounding the paramedic role in caring for people who use non-opioid illicit and controlled substances was scarce. This traditional role has positioned paramedics as the first point of medical contact with the health care system for people who use drugs for decades. 73 Prior to the beginning of the drug poisoning crisis, paramedics were able to reverse opioid toxicity with relative ease, and the subsequent care after reversal did not involve paramedics. However, in recent years, the steady increase in drug toxicity and incidence of drug poisoning has complicated the traditional response.74–78 Paramedics spend significantly more time on the scene with patients in the resuscitation phase, at times struggling to reverse a drug poisoning potentially complicated by potent and co-intoxicating substances that may not respond to naloxone administration. In addition, the significant decrease in emergency department conveyance following a drug poisoning puts a person at much higher risk of short- and long-term mortality. Given the correlation between ED non-conveyance and increased mortality, coupled with a marked decrease in emergency service/paramedic service activation at the event there may be a narrowing window of opportunity for paramedics to positively influence a patient's journey through the health care system by offering alternative harm-reducing pathways and care. 79 Despite a decrease in paramedic service activation, the rate at which paramedics encounter people who use drugs continues to surge, further positioning them to offer alternative models of care that do not necessitate ED conveyance.
Throughout all contexts of practice within paramedicine, the focus of the paramedic role is shifting from one that is somewhat responsive and linear, to a holistic ‘system navigator’.80,81 Today, paramedics advocate for a patient's wants, needs and rights which can involve alternative destination pathways, outreach and referral, community care and more. Despite an awareness that this shift will benefit patients, and may benefit paramedics, this shift in the paramedic role in caring for people who use drugs remains unexplored.
The greater role of the paramedic in the drug poisoning crisis may be complicated by increasing burnout, helplessness and moral distress among paramedics. Some evidence suggests that a once rewarding patient encounter for paramedics has evolved into one which may leave both parties (the patient and the paramedic) feeling dissatisfied. The consequences of being left on the scene while experiencing acute withdrawal may lead to subsequent substance use to stave off undesirable symptoms, potentially leading to further drug poisoning events. The downstream effects of subsequent drug poisonings on paramedics can manifest as multiple resuscitations, sometimes of the same patient, lending to a sense of harboured helplessness. 82 This has contributed to a notion described by paramedics as being confident in treating a drug-poisoned patient but lacking in the ability to treat the underlying cause. Introducing paramedic-led harm reduction programs such as referral pathways, take-home naloxone programs and treatment of acute withdrawal 83 has the potential to not only break the drug poisoning cycle for patients but also break the responsive cycle for paramedics and expand their capacity to help. Implementing such programs require the involvement of key stakeholders and harm reduction subject matter experts, as well as people who use drugs to ensure person-centred, non-paternalistic approaches to develop trust. Program success, however, will depend on paramedic engagement, an apparent barrier to success discovered within this review.
Such divergent views related to harm reduction among paramedics could potentially be the greatest barrier to program success. Some paramedics describe harm reduction programs as enabling riskier drug use and being ineffective in reducing drug-related deaths. These misconceptions have influenced some paramedics to reject drug-related harm reduction as a context of practice. Compassion fatigue and cumulative stress are potential contributory factors. However, these constructs may begin to form as early as initial paramedic education. Multiple studies identified in this review revealed that paramedic students have the lowest levels of empathy for people who use drugs than any other patient population66,84,85 and in some cases, their empathy decreases throughout their education. To what extent paramedic education contributes to or neglects to address provider-based stigma is not well understood and requires urgent research attention. In the absence of clinician buy-in towards harm-reducing programs, the evaluation of program success will be limited and misrepresented. Whether formal harm reduction programs are implemented or not, non-judgemental and empathetic approach that includes the use of non-stigmatising language are informal harm reduction approaches that can be integrated into an individual paramedic's practice instantly. 86
The relationship between paramedics and people who use drugs has historical underpinnings that have caused confusion and at times hostile perceptions. By choosing to use language that embodies an empathetic approach towards people who use drugs, feelings of guilt and shame which can cause a person to isolate and use drugs alone, can be suppressed. The relationship between provider-based stigma or attitudes and decreased activation of the EHS system is not well understood. However, many people who use drugs perceive calling for paramedics as akin to calling for police. Decreasing police presence at a drug poisoning may have the potential to reduce on-scene tension bred from long-standing negative associations which may have stemmed from intergenerational trauma, criminalisation and stigma. Improving the relationship between people who use drugs and the EHS system must begin with and be sustained by ethical engagement with people who use drugs in service design and delivery. It should be acknowledged that in some areas, due to delayed wait times and other complicating contributors, the relationship between people who use drugs and the EHS system is strained. 87 The importance of the paramedic role in caring for people who use drugs, however, will simply not be fully realised without this collaborative approach. Despite three studies included in this review seeking perspectives of people who use drugs, only one focused on them. 88 People who use drugs offered key insights towards the barriers of harm reduction, such as the willingness to activate EHS, as well as the opportunities, such as the sentiment that paramedic-initiated post-drug poisoning therapeutics can be viewed as life-saving. 88 Success to a health care organisation may not be defined as success to people who use drugs, and vice versa; therefore, organisations that do not consult with people who use drugs will likely struggle with the success of person-oriented outcomes within their programs.
Limitations
Despite our efforts to be comprehensive, we may have missed relevant studies. Although we used previously established terms to describe drug use in our search strategy, there may be other terms that were not included. Additionally, the lack of consistency in indexing keywords and descriptive terms in abstracts may have affected our search results. Our search was limited to English-language articles and our Google Scholar search only included the first 1000 results. Despite these limitations, we offer that our review offers a comprehensive overview of the current understanding of the role of paramedics in caring for people who use illicit and controlled drugs and provides suggestions for future research.
Conclusion
This scoping review underscores the urgent need to address the overlooked and under-researched role of paramedics in caring for people who use illicit and controlled drugs. The review revealed significant gaps in knowledge regarding alternative and holistic models of care, as well as the importance of incorporating patient perspectives in research on system-level changes. 89 Innovative harm reduction and holistic care strategies have the potential to create a ripple effect in reducing harm on both sides of the paramedic encounter. 14 By empowering paramedics with the tools to provide holistic care, we can foster their resilience, purpose and empathy towards people who use drugs, leading to improved wellness, job satisfaction and patient outcomes. 71 The paramedic role exerts a significant influence on a patient's healthcare journey, and it is crucial that we direct research attention to this highly understudied area. 90 Ultimately, holistic models of care can enhance the relationship between paramedics and people who use drugs, driving meaningful progress towards reducing harm and improving health outcomes.
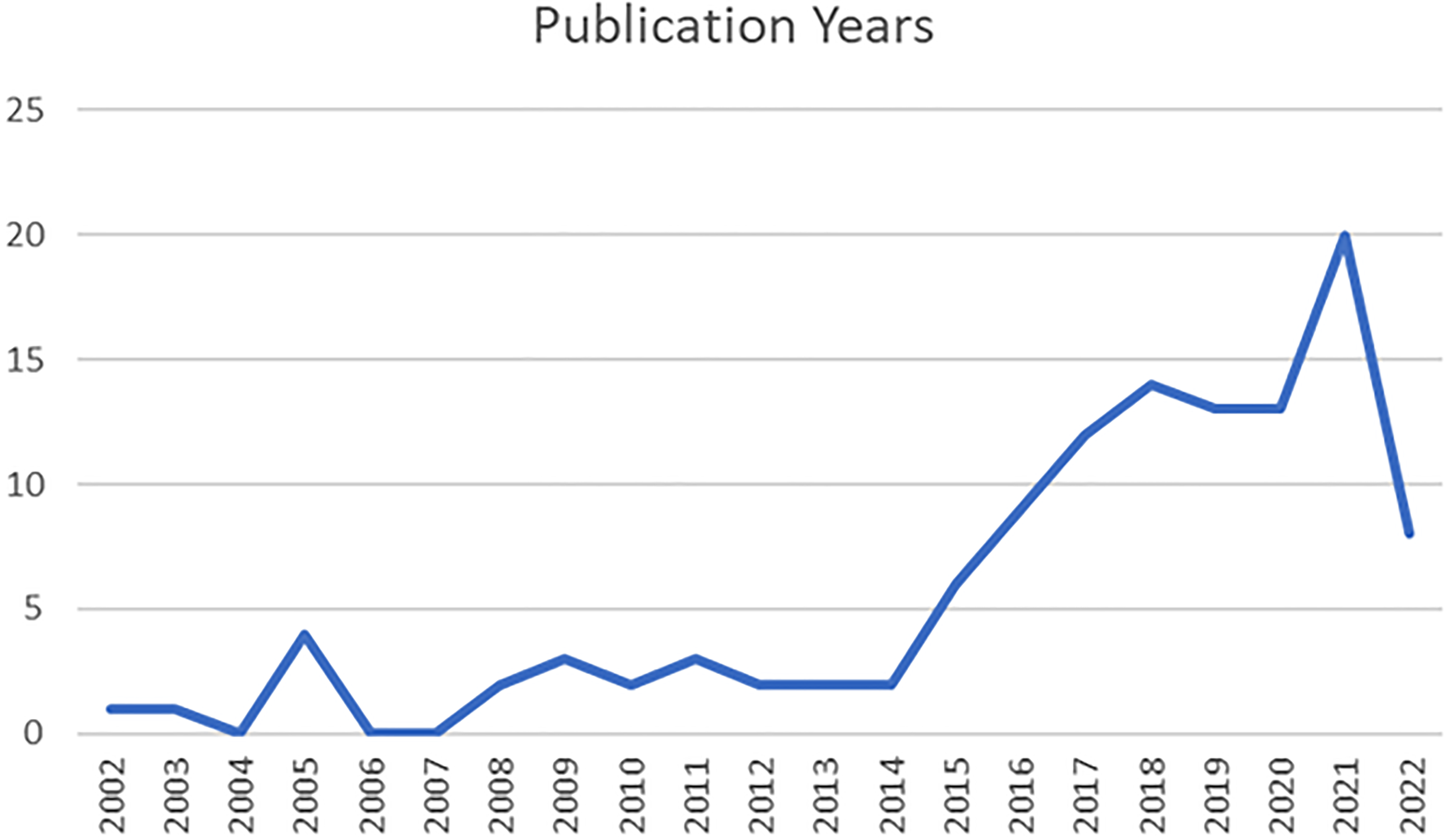
Studies by publication year.
Supplemental Material
sj-docx-2-pam-10.1177_27536386231171813 - Supplemental material for The paramedic role in caring for people who use illicit and controlled drugs: A scoping review
Supplemental material, sj-docx-2-pam-10.1177_27536386231171813 for The paramedic role in caring for people who use illicit and controlled drugs: A scoping review by Jennifer Bolster, Richard Armour, Michelle O’Toole, Meghan Lysko and Alan M. Batt in Paramedicine
Supplemental Material
sj-docx-3-pam-10.1177_27536386231171813 - Supplemental material for The paramedic role in caring for people who use illicit and controlled drugs: A scoping review
Supplemental material, sj-docx-3-pam-10.1177_27536386231171813 for The paramedic role in caring for people who use illicit and controlled drugs: A scoping review by Jennifer Bolster, Richard Armour, Michelle O’Toole, Meghan Lysko and Alan M. Batt in Paramedicine
Supplemental Material
sj-docx-4-pam-10.1177_27536386231171813 - Supplemental material for The paramedic role in caring for people who use illicit and controlled drugs: A scoping review
Supplemental material, sj-docx-4-pam-10.1177_27536386231171813 for The paramedic role in caring for people who use illicit and controlled drugs: A scoping review by Jennifer Bolster, Richard Armour, Michelle O’Toole, Meghan Lysko and Alan M. Batt in Paramedicine
Footnotes
Availability of data and materials
Search results and screening information can be obtained from the corresponding author.
Author contributions
JB and AB conceptualised the study. JB and AB conducted the initial and subsequent searches. RA, MO, ML and JB screened abstract and full texts for inclusion, as well as extracting data from the studies included full texts. AB resolved conflicts in the screening phase and performed quality assessment of the extracted texts. JB performed analysis, synthesised the results and authored the first draft. All authors edited the manuscript for intellectual content. All authors have approved the final version for publication and accept responsibility for its content.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AB is Deputy Editor of Paramedicine.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.