
Abstract
In this perspective, the authors argue that paramedicine's core structure and mandate (i.e., the 9-1-1 system) can innovate to better align with the needs of the public and address the evolving healthcare landscape. Examining Canada as a case, paramedic services are increasingly utilized by the public as a first point of contact for health and social care and often for nonemergent events. Existing emergency-focused paradigms leave the health profession poorly aligned or underprepared to meet the needs of the public and isolated from other healthcare providers and systems. While advances in healthcare policy, infrastructure, and best practices have been proposed to address Canada's healthcare challenges, these advances have yet to sufficiently translate into core paramedicine systems. To illustrate these points, the authors critically examine the alignment of paramedicine models of care with public need, paramedicine's response to government and scholarly advances in healthcare policy and practice, and contemporary public healthcare issues in Canada. Paramedicine's changing landscape is also examined as context for innovation and change. The authors argue that core paramedicine systems be augmented with (not replaced by) an integrated interprofessional primary care paradigm and introduce a novel conceptual strategy, approach, and model of care referred to as IMPACC—Improving Patient Access to Care in the Community, including its guiding principles, conceptual framing, intended outcomes and domains for education. The authors conclude that paramedicine in Canada stands at a pivotal juncture and that the traditional emergency-focused model is increasingly misaligned with contemporary health and social care needs, necessitating a shift toward a more integrated, interprofessional primary care approach. The IMPACC concept offers a viable conceptual blueprint for this transformation, proposing a redesigned 9-1-1 system that incorporates timely primary care services and fosters interprofessional collaboration and integration for differentiated and undifferentiated patients in the community within core paramedicine systems.
Introduction
In a rapidly changing healthcare landscape, paramedicine, in terms of its core structure and mandate, can do more to innovate and support a health and social care system that is under strain. Long wait times, difficulty accessing primary care, overcrowded emergency departments (EDs), and a crisis in health human resources are examples of this strain.1–6 Navigating these challenges calls for innovation that is responsive to current needs and forward-looking to ensure health and social care systems can adapt. This means leaders must explore where and how to shape policy and practice and participate in identified strategies. For instance, recent government policies have advocated for more community-based health and social care, optimizing or broadening the scope of practice of health professions and introducing new models of care, all intended to alleviate system strain and optimize system performance and patient outcomes.7–9 While these kinds of policy advances span several health professions and contexts, core paramedicine systems are favorably positioned to leverage their large and mobile healthcare structure to play a vital role in a health and social care system redesign if guiding paradigms can advance to support such roles.
Paradigms, systems, and shifts
Paramedicine's infrastructure, funding, scope of practice, and models of care have historically been informed by and aligned with public safety, emergency care, resuscitation, and transport ideas, consistent with Makrides et al.'s description of a “directive paramedic system.” 10 These ways of seeing and shaping paramedicine represent contemporary paradigms. Paradigms can be thought of as views that represent distinct concepts, practices, and standards at a particular time and space. It guides understanding and how researchers, leaders, and practitioners approach problems, and how to perceive and interpret ways forward. Possibly due to healthcare system gaps and shifts toward continuous care needs, the public has broadened its use of paramedic services to include events beyond emergencies, often for combined health and social needs that do not require resuscitation or transportation to an ED but remain complex11,12 This raises questions about how aligned paramedicine systems are with the needs of the public or how well this health resource is attending to shifting needs. This broadening and increasing use by the public, 13 poor alignment, 14 as well as calls for paramedicine locally, nationally, and internationally to rethink its guiding paradigms and axiology,15–19 means paramedicine must change if it is to keep pace with the shifting healthcare landscape and public expectations and be considered or leveraged as a suitable and sustainable healthcare resource.
In this perspective, we contribute to the rethinking process by critically examining core paramedicine systems in Canada. While we recognize that internationally, similar efforts may be considered or underway20,21 and that several approaches continue to be explored, we focus on the Canadian context as a case to stimulate the Canadian paramedicine community to rethink its guiding paradigms and other jurisdictions with the same opportunity as appropriate. Our arguments are that (1) core paramedicine systems must anticipate and be responsive to a changing healthcare landscape, (2) alignment be a priority guiding principle and conceptual framework for model design and outcomes, and (3) it is the augmentation of guiding paradigms that shape the profession's direction in meaningful ways. New paradigms emerge and become helpful during periods of dissatisfaction. They allow us to examine not just what systems do or how they are structured, as Makrides et al. have described, 15 but also why and what new structures become possible when viewed with an additional lens.
We begin by looking at contemporary healthcare strategies—calls for more integrated healthcare and the primary care crisis—to demonstrate that the emergency-informed paradigm that underpins paramedicine is misaligned with the evolving healthcare landscape and the needs of the public it interacts with and serves. We argue, as others have,15,18 that adhering to a narrow emergency-only paradigm when shaping paramedicine infrastructure and function places limits on this health profession's contributions despite its significant potential. We note that these shifts are informed by an awareness that stronger relational collaboration between non-colocated providers results in a deeper understanding of the complex needs of each patient. We end by presenting an innovative clinical program for Canada titled “Improving Patient Access to Care in the Community” (IMPACC) that represents a concept, strategy, and model of care as a targeted redesign of core paramedicine systems (i.e., the 9-1-1 system). IMPACC shifts the guiding paradigm for paramedicine to one that is additionally guided by an interprofessional and integrated primary care paradigm and axiology and appreciates health and social complexities of every contact paramedics make with the public.
We aim to contribute to the ongoing discourse, including paradigmatic and axiological shifts, to the redesign of paramedicine systems as proposed by Tavares et al.16,17 and Makrides et al., 15 such that paramedicine (a) be better at keeping up with a changing healthcare landscape, (b) provide health and social care that are more aligned with community and public needs, and (c) promote and contribute to more accessible and timely interprofessional primary care services in the community.
Defining core paramedicine systems
Before exploring these issues, we offer two clarifications. First, we are placing an intentional boundary on “core” paramedicine to mean the 9-1-1 system in Canada. Core paramedicine is generally a public-activated healthcare resource for undifferentiated patients (i.e., those whose medical history and health and social needs and circumstances are unknown to paramedics at initial patient contact). No specific patient type or acuity level is targeted, even if identified by dispatch or secondary triage algorithms. Dispositions and continuity of care plans for these patients are often very limited. We differentiate core paramedicine from “community paramedicine” (also referred to as mobile integrated healthcare), a moniker often used to describe various clinical programs that use paramedics in the community but outside of core paramedicine systems in Canada. 22 Often, these include targeted patient populations such as those with complex health and social care needs, older adults, frequent users, patients with specific disease processes, patients discharged from the hospital, and patients with mental health and addiction issues.23,24 For example, in Ontario, Canada, community paramedicine programs are typically distinct from core paramedicine systems, operating under different regulatory frameworks, funding, education, medical oversight, and infrastructure. 25 Second, we note that paramedics engaged in interprofessional primary care work is not a new concept, especially in international contexts, 26 (e.g., paramedics working in clinics), but different from our focus when that work exists outside of the “core” paramedicine system described above. Also, some models target lower acuity patient types with different health care providers, specialized and interprofessional response teams,27–29 which are again different than paramedics working in core 9-1-1 systems with undifferentiated patients without implementation of alternative response models.
Aligning paramedicine with a changing healthcare landscape
We use alignment within a changing healthcare landscape as a guiding conceptual framing and issue. By alignment, we mean the degree to which services provided by paramedicine systems are meeting the needs of the public it serves or representative of contemporary healthcare policy. Alignment can also be viewed as an outcome differentiated from efforts to, for example, reduce 9-1-1 calls or reductions in transports to an ED. 30 We note that alignment (what others before us may have meant when asking for reconfigurations) 31 is not necessarily a new concept, but contemporary needs, based on contemporary challenges, are ever-changing and obligate attention to guiding paradigms. We examine alignment as the potential impetus for system redesigns.
Alignment with public use
In recent studies, examining the structure of paramedicine systems in Canada, researchers observed that a significant proportion of patients who access care via 9-1-1 and are subsequently transported to a local ED are discharged directly from the ED. 11 Many of these patients did not require emergency interventions, and only 5–10% received any interventions by paramedics. Further, the ongoing analysis of data spanning several years across multiple paramedic services suggests that the traditional model of care accounts for only about 20% of all patient interactions, with considerable misalignment with lower acuity patient presentations, 14 a finding consistent with studies elsewhere. 32 In other words, it is not just that the public is accessing paramedic services for lower acuity events more often, it is that when they do, paramedicine has very little to offer. This is in a context where the use of paramedic services by the public has increased 38% over the last decade. 13 Collectively, this suggests a misalignment between the manner in which the public uses paramedicine, and the emergency-focused services that paramedics are well positioned to attend to. This misalignment calls for action in both system effectiveness and a person-centered care perspective. 33 Consequently, researchers have advocated for system redesigns that contribute capabilities (i.e., the inclusion of novel diagnostics and interventions not commonly included in paramedicine systems) to better align with the needs of the public, introducing more community-based capacity into the healthcare system. 11
Integrated health care
In response to the fragmented nature of healthcare delivery systems that may not meet the needs of patients comprehensively and efficiently, integrated healthcare has been a subject of growing interest.34–36 The concept aims to create a seamless, efficient, and patient-centered healthcare experience and has become a key healthcare system strategy.37,38 The impetus for implementing integrated care is not just theoretical but substantiated by several advantages such as collaborations in patient care, promoting accessibility, optimization of resources, minimization of duplication of services, improved cost-effectiveness through coordination among providers, better patient satisfaction, and overall health care experiences and outcomes. 39 While challenges persist (e.g., information sharing, professional silos, fragmented funding, inadequate interest-holder engagement),40,41 an integrated healthcare system continues as a strategy for more patient-centric, equitable, and cost-effective healthcare. 42
It is difficult to find evidence of core paramedicine systems evolving in this way. The “Rainbow Model of Integrated Care” provides a common, comprehensive conceptual model that offers insights into the multidimensional and multilevel nature of integrated care.43–45 It includes several integration layers, including clinical, professional, organizational, system, functional, and normative types, at multiple levels (micro, meso, macro) and degrees (linkage, coordination, full integration). Viewed through this lens, Canadian core paramedicine systems have not evolved in ways that would suggest much health systems integration. Coordination of care, shared responsibilities for care, joint initiatives between separate health care entities, the alignment of rules and policies, health care record sharing, shared values and missions, and shared decision-making (to name a few) are hard to find and if present in any degree, would be the exception rather than the rule for paramedicine in Canada.
Access to primary care
Access to primary care in Canada continues to be limited. Primary care is defined as the first point of contact for health care that is continuous, comprehensive, and person-focused. 46 It involves the integration and coordination of health and social care provided elsewhere or by others. Effective primary care helps alleviate several downstream issues (e.g., chronic disease, reduced use of emergency services, 47 and ED visits and hospitalizations) and continues to be supported with innovation.47,48 However, timely access, or even access at all, continues to be difficult for many Canadians.49–51 The problem is worsening with increasing administrative burdens on health care providers, family physicians reducing their practice or retiring without sufficient replacements, physician burnout, and fewer trainees selecting primary care.52–58 These issues collectively limit or threaten the supply of primary care services overall, 59 a problem made worse when we consider disparities in access across regions, age groups, income levels, racialized groups, and certain health needs (e.g., mental health). 60
Researchers have argued for setting new expectations related to access, advocating for timeliness by ensuring services are closer to home, promoting patient access to information, expanding scopes of practice of allied health professions, and more team-based models of care.61,62 Governments have supported primary care expansions, including the formation and funding of Family Health Teams (FHT), more Nurse Practitioner-led clinics, and the restructuring and provision of a broad range of community-based services.63,64 These are organizational and conceptual shifts intended to include a diverse group of health and social care providers working together to provide accessible and timely primary care in the community. At present, paramedics are not conceptualized as part of these initiatives.
A critical examination of paramedicine's core systems, particularly its role in mitigating the primary care crisis through integration into interprofessional teams or models of care, reveals significant gaps. Examples of shifts in supportive policy, education standards and opportunities, scope of practice, and professional cultural norms, when including more interprofessional primary care roles, functions, or identities, are lagging. For example, existing patient care standards 65 and competency frameworks 66 do not prioritize (or sometimes do not even account for) nonemergency patient events or needs that are commonly encountered in the 9-1-1 system. They also do not integrate social needs and services, do not obligate or facilitate collaboration with other care providers, and ignore continuity of care or the coordination of care needs. A recent (2023) review of the literature on research supporting the advancement of paramedicine in Canada (i.e., what researchers prioritize) also highlighted gaps in evidence related to these issues. 67 Instead, knowledge production has focused mainly on unrelated operational issues, resuscitation, airway management, emergency pharmacological interventions, and trauma care. 67
Evidence suggests that paramedicine may be poorly aligned with public needs.11–14 There is also difficulty finding evidence of core paramedicine systems in Canada adapting to contemporary healthcare issues or policy, specifically the inclusion of integrated care models or strategies to alleviate access to primary care issues.65,66 While the evidence base has not aligned with these issues, 67 it is evolving and providing new insights.15–21 When viewed through these lenses, this leaves paramedicine as a potentially misaligned healthcare system and service. A counterargument may be that existing systems were not designed for these issues; therefore, it is unfitting to expect that they would. We add that existing paradigms did not permit attention to these issues and suggest that it is the guiding paradigm, not these issues themselves that matter most. Our intention is to highlight how existing paradigms shape how and why the profession acts as it does. Only with new or augmented guiding paradigms will we educate, practice, and conduct science in new ways. Next, we summarize three initiatives that begin to suggest this transition is underway, offering opportunities for change.
Paramedicine's changing landscape in Canada
At least three broad initiatives are signaling a changing paramedicine landscape in Canada. First, Canadian paramedicine system leaders have identified new principles to guide system design. 17 Some principles signal a paradigm shift from traditional values toward a more holistic, patient, and community-focused approach. For example, principles include the integration of paramedicine within broader healthcare services, collaboration across sectors using integrated healthcare frameworks, and providing care along a health and social continuum. The principles overall deemphasize a public safety, transportation, or resuscitation paradigm for something more holistically health and health-system-oriented. 17 Emphasizing professional autonomy, the framework suggests paramedics could navigate advances more independently, informed by an evidence-based and quality-driven ethos. The health and well-being of paramedics are also prioritized and reminding us that any changes in a healthcare model of care must also take into consideration its providers. Advocating for “Intelligent Access to and Distribution of Services” challenges the long-standing singular access point and structure for core paramedicine systems.
Second is the redefining of national educational and entry-to-practice frameworks for core paramedicine systems. Recently, Batt et al. led the redevelopment of the National Competency Framework for Paramedics in Canada, signaling a new comprehensive set of requisite activities, capabilities, and roles for all paramedics regardless of practice setting, including core paramedicine systems.68,69 The framework augments emergency care with newer ways of thinking about practice. For example, “collaborative care” is emphasized, encouraging education systems to prepare paramedics to work as part of dispersed interprofessional and integrated healthcare teams involved in care delivery, planning, and continuity. Another is the Pan-Canadian Essential Regulator framework. 70 This entry-to-practice framework also emphasizes similar broadening of capabilities representing newer paradigms, including collaborative patient care, patient preferences, and care planning. Both signal a broadening of thinking regarding what matters when preparing for paramedicine practice and setting entry-to-practice expectations.
Third, “community paramedicine” programs have become widespread and successful.22,71 Generally, these clinical programs focus on providing care in the community using paramedics in innovative and unconventional ways, with specialized skill sets and mainly outside of core systems. For example, this has included scheduling paramedics to support seniors in their homes72,73 providing ongoing and intensive support for patients at risk of readmission, 74 more aligned services for patients experiencing social isolation and mental health issues, 75 or to support marginalized patient populations that encounter challenges in accessing healthcare. 76 A recent review of local community paramedicine programs suggested that, contrary to core paramedicine, different types of integration are underway, from prevention to population-based public health initiatives and from providing responses to exacerbations of chronic conditions to being part of broader care pathways. 24 Examples of clinical programs where paramedicine “partnered with otherwise siloed service providers in the geographic area, including hospitals, primary care, social services, community-based allied health such as nursing and physiotherapy, mental health facilities and homeless shelters” were identified. 24 Others reported community paramedicine programs as examples of local leadership, and availability of a workforce that is flexible, mobile, and willing to change roles that could enable integrated care and increase a systems' ability to adapt.24,77,78
New principles guiding system design, broadening competency frameworks, and community paramedicine programs provide insights into the services that might suit the broader core paramedicine infrastructure. However, these advances have yet to translate into significant or scaled changes for core paramedicine systems, and enablers (e.g., collaborative governance, data sharing, policy alignment or integration, shifts in cultural identity, practice, or education) still need to be explored. One notable exception has been the widespread inclusion of palliative care principles in Canada into core paramedicine systems.79–81 This was, at the time, a conceptual shift that challenged existing practices and improved the alignment of services with the public's needs. Internationally, shifts in paramedicine to include primary care services have demonstrated promising results, 82 including reduced system pressure, increased in health human resources, and better access to care. 26 Still, much of the research exploring paramedicine as primary care, while generally favorable, is structured as community paramedicine programs or as paramedics working in primary care contexts (i.e., outside of core paramedicine systems).26,82,83 Next, we describe a project titled “IMPACC,” designed specifically as an integrated, interprofessional primary care strategy for core paramedicine systems.
Redesigning core paramedicine systems with IMPACC
Overview
IMPACC is a conceptual and practical broadening of the 9-1-1 system, intended to better align services with the needs of undifferentiated patients when they access health care using 9-1-1, and for differentiated patients who require timely—but not emergent, nor delayed—care in collaboration with a health care team. We differentiate it from several existing and ongoing community paramedicine program innovations that target specific patient demographics, disease types or patient needs (e.g., frail seniors, people living with diabetes, or mental health challenges), or clinical programs that exist outside of the core 9-1-1 system (e.g., hospital-to-home programs, senior's home support programs). 22 IMPACC is a redesigned and reconceptualized 9-1-1 system intended to better support health and social complexities for patients encountered as part of common 9-1-1 responses and as an integrated resource with interprofessional but non-colocated primary healthcare teams. With IMPACC, undifferentiated patients can expect more aligned services when their needs are less emergent. Primary health care providers and systems can broaden reach and services by collaborating with core paramedicine systems to support existing differentiated patients who have access challenges, require timely nonemergent care, and may not be suitable for scheduling or referral. This approach augments core paramedicine with an interprofessional primary care paradigm to promote better alignment of services and infuses a large and geographically dispersed existing resource into a strained healthcare system. See Box 1A and Box 1B for clinical vignettes illustrating the IMPACC concept for both undifferentiated and differentiated patients.
Clinical vignette illustrating IMPACC with undifferentiated patients.
Zahra is a 72-year-old Middle Eastern female living alone in a small community with no primary care provider. She develops a mild fever, experiences mild shortness of breath, and feels generally unwell. She contacts 911. Paramedics respond but they are part of a program called “Improving Patient Access to Care in the Community” (IMPACC). With broadened competencies and while part of an interprofessional primary care team, paramedics establish a working diagnosis of early onset pneumonia and start Zahra on antibiotics without needing to be transported to an emergency department. Recognizing the social determinants impacting Zahra's health, such as social isolation and limited access to regular medical care, the paramedics take additional steps to address her broader needs. They assess her home for safety, ensuring it is free of hazards that might exacerbate her condition. Plans are made to connect Zahra to primary care services, and referrals are arranged for social support services to help address her isolation. Before leaving, the paramedics organize a follow-up visit by community paramedics or other appropriate services, and, with Zahra's consent, share health information with her new interprofessional primary care team to promote continuity of care and address her holistic well-being.
Clinical vignette illustrating IMPACC with differentiated patients.
Stefano, a 65-year-old Italian male who also lives alone in the same small community, experiences similar symptoms and condition to Zahra (early onset pneumonia). However, Stefano has a family doctor who is part of a family team that includes the IMPACC program. Instead of calling 911, Stefano calls the family health team and is connected with a primary care physician, nurse practitioner, or other appropriate primary health care provider who is concerned about his health. The health care provider, believing he does not require emergency department care, and knowing he cannot be seen at the clinic that day, contacts the IMPACC paramedics. Paramedics arrive that same day, assess Stefano, and in consultation with the team, initiate a care plan. Stefano receives the same services Zahra did (see Box 1A), including care coordination and continuity plans. During their visit, the paramedics notice that Stefano's home is poorly insulated and the heating system is inadequate, which could exacerbate his respiratory condition, especially during colder months. Recognizing the impact of substandard housing on his health, the paramedics coordinate with local social services to arrange for home heating assistance and improvements. Before leaving, the paramedics assess the home for other health risks, organize a follow-up visit by community paramedics or other appropriate services, and, with Stefano's consent, share health information with the IMPACC team to promote continuity of care and address the environmental factors contributing to his health.
Guiding principles and targeted outcomes
IMPACC is based on a broadening evidence base supporting paramedicine's role in healthcare, provincial government directions that call for more integrated community-based healthcare, and national visioning reports that call for a restructuring of paramedicine systems.15–17 Specifically, IMPACC is informed by the following national paramedicine principles: (1) Patients and Their Communities First, (2) Health Care Along a Health and Social Continuum, (3) Integrated Health Care Framework, and (4) Intelligent Access to and Distribution of Services.
17
Translating these contributions as a collective led to four targeted outcomes shaped by an interprofessional,84,85 integrated43,44 and primary care2,86 paradigm and axiology. For core paramedicine systems, these include:
Alignment: to improve the alignment of health and social care interventions provided by paramedics with community needs and to do that collaboratively with other health care providers. Integration: to integrate core paramedicine systems with interprofessional and community-based primary care teams, creating new capacities and opportunities for community-based health and social care services for patients. Access: to support timely access to interprofessional primary care for undifferentiated (i.e., those who access healthcare via the 9-1-1 system) and differentiated patients (i.e., existing patients of primary care providers who require timely—but not emergent, nor delayed—care in collaboration with a health care team while still in the community). Care Continuity and Coordination: to ensure patients are supported with continuity and coordination of care plans and the appropriate disposition, education, resources, pathways, and communication to support these goals.
Conceptual framing
IMPACC broadens core paramedicine systems by opening two broad access pathways (see Figure 1). The first focuses on undifferentiated patients and is represented by Box A in Figure 1. Patients activate this pathway by using the 9-1-1 system, as they already do. Their needs may or may not be emergent or life-threatening. Given the undifferentiated nature of this interaction, paramedics continue to respond using existing notification and distribution algorithms and are equipped with emergency and resuscitative approaches. However, in those instances when needs do not require such interventions, additional health and social services informed by an interprofessional and integrated primary care lens and infrastructure are applied. Health and social services more consistent with primary care, including care continuity and coordination, become a focus. This can include leaving the patient in place with support, organizing ongoing care plans, or transportation to a destination other than an ED (e.g., a community health clinic, FHT, or mental health hub). For patients attached to a primary care provider, health information is shared to support continuity. For those who are not, an attachment process is initiated to address the gap. Where appropriate, patients may also be referred to community paramedicine, or other services (e.g., provincial health services, local FHTs) for ongoing support or follow-up. See Box 1A above for a clinical vignette related to this pathway.
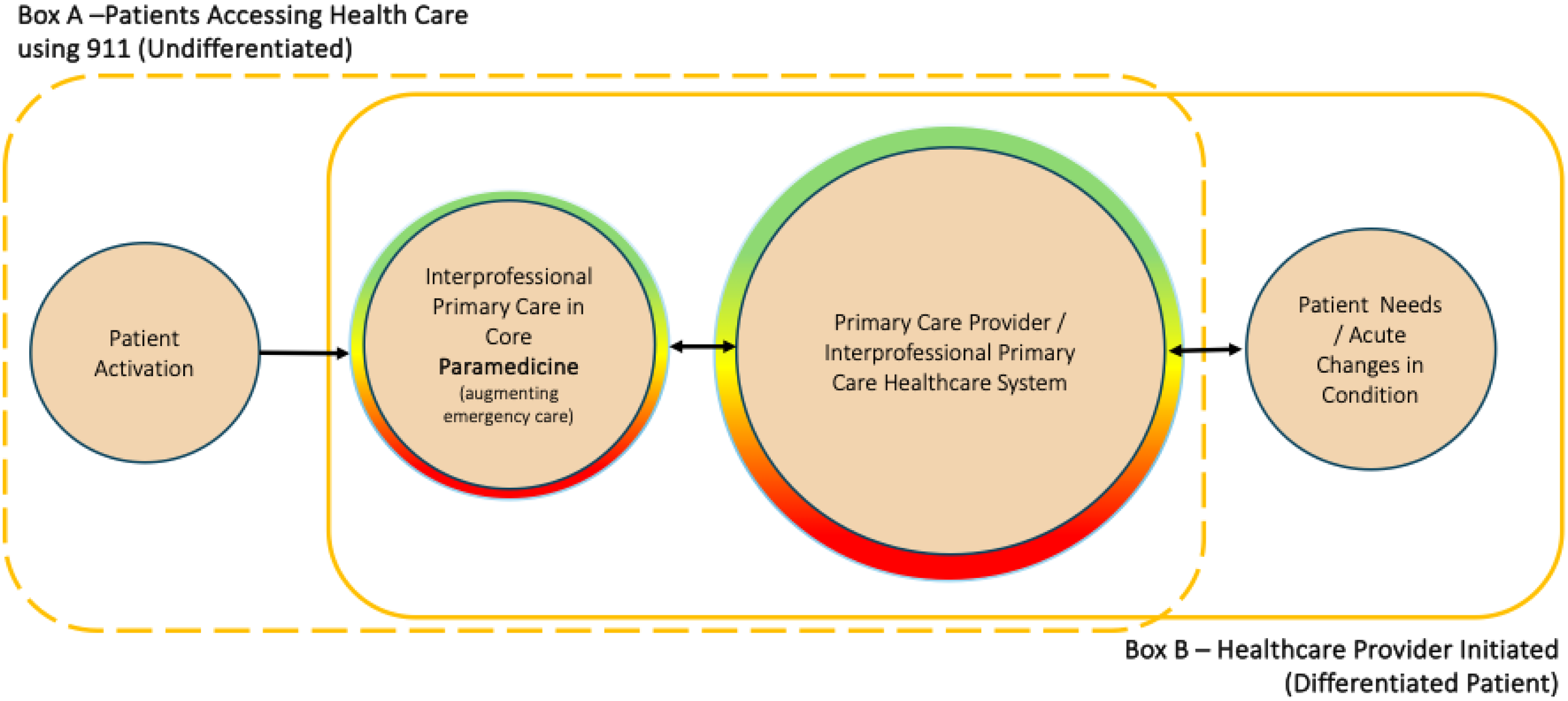
Improving Patient Access to Care in the Community (IMPACC) conceptual model. *The color scheme represents a continuum of emergent (red) and nonemergent (green) health, and social care needs for every patient interaction.
Second is the differentiated access pathway, represented by Box B in Figure 1. Here, patients have experienced a change (perhaps acute) in their condition and access health care through their primary healthcare provider or other primary care services. However, the patient cannot physically access care, and/or the virtual or clinic-based primary health care provider has identified that timelier same-day in-person assessment or attention is needed. In collaboration with the health care team, paramedics within the existing core paramedicine system respond using modified notification and distribution algorithms and approaches. Again, services that are interprofessional, team-based, and more consistent with primary care are provided, and care continuity and coordination become a focus. Health information is shared to promote continuity. Patients may also be referred to community paramedicine, or other services for ongoing support or follow-up. Similarly, those accessing community paramedicine who require more urgent services can be serviced by this pathway and infrastructure. See Box 1B above for a clinical vignette related to this pathway.
Developing the educational framework
Achieving these outcomes and pathways involves broadening the core function of paramedic clinical work to include a broader conceptualization and operationalization of the role and new services, relationships, and structures with interprofessional primary care team members. To prepare paramedics and support implementation, an interprofessional group of clinicians and leaders considered the model of care, and existing provincial educational and practice standards, and identified the following domains for inclusion in educational frameworks: new professional roles, a broader understanding of health assessment and diagnostics, new treatments and interventions (not currently included in the core paramedicine context), a focus on preventative care and health promotion, chronic disease management, mental health crisis intervention, broadened geriatric care, health education and counseling, patient communication and patient advocacy, cultural competence and equity, care coordination, integrated care, and continuity of care, community participation, broadened documentation and reporting, public health, relational-centered collaborative practice, and provider reflexivity and wellness. These domains are poorly attended to in existing educational models in Canada, if at all, and represent a broadening of scope and competence.
Ninety competencies were distributed across these 16 domains intended to support commonly encountered conditions or events encountered in primary care and those identified as potential priorities based on previous research. 11 See Supplementary File 1 for a copy of the proposed initial competencies by domain. Several new procedural skills (e.g., point-of-care diagnostics), pharmacological interventions (e.g., antibiotics, steroids, respiratory agents, antiemetics), and new medical directives were also added. These competencies and materials have been shared with the development group for the new National Competency Framework for Paramedics in Canada, 67 and to inform a distinct and targeted educational model.
A critically oriented and relationally centered interprofessional approach underpins the IMPACC competency framework and curriculum. We call this approach interprofessional practice education-plus (IPE+). The approach leverages established competency-based interprofessional education domains identified by the Canadian Interprofessional Health Collaborative84,85 and broadens it by emphasizing relationality and criticality in collaborative work. The IPE+ employs relational expertise, introduced by Edwards as a capacity that health and social care providers can draw on to navigate the dynamics of knowledge, power, and identity in interprofessional interactions. 87 It has been suggested that relationality can be particularly productive in a dynamic health and social care landscape, where provider-to-provider interactions are as likely to be brief and occur between providers unfamiliar with each other, as they are to be in colocated teams. 88 Criticality is centered on supporting paramedics as they navigate hierarchical and inequitable distributions of power as part of their everyday interprofessional interactions. The IMPACC program uses the IPE+ model to equip paramedics to navigate a diversity of practice interactions with a variety of colleagues who are situated across the health and social care system.
Our intention is not to suggest that these competencies are inconsistent with those of other jurisdictions or some community paramedicine programs. Rather, we suggest that they be part of core Canadian paramedicine systems, most of which are absent in existing entry-to-practice education, hiring processes, continuing or advanced paramedicine education, and practice.
Discussion
We have argued that, in a rapidly changing healthcare landscape, paramedicine in Canada, in terms of its core structure and mandate, must do more to innovate and contribute toward an integrated health and social care system that better aligns its services with the needs of the public. Paramedicine systems are a long-standing and stable health human resource whose large geographically dispersed infrastructure has become increasingly utilized by the public and ought to be more aligned with growing needs and integrated with other health and social services. Core paramedicine has been relatively stagnant in a changing healthcare landscape, despite advances toward supporting better community-based health and social care. Healthcare strategies to promote non-colocated team-based interprofessional collaboration and primary care have yet to translate into new models of care within core paramedicine.
Core paramedicine appears to have been locked by an emergency, resuscitation, and transport paradigm, limiting the opportunity or responsibility for change. However, a changing landscape in paramedicine represented by contemporary analyses of the system, 10 national visioning reports,15,17 new national educational frameworks, 69 and several new innovations and long-standing practices in community paramedicine, are making clear the need and opportunity to think differently about paramedicine systems.
With this in place, we introduced the concept, strategy, and model of care referred to as IMPACC. Informed by new principles guiding the future of paramedicine in Canada, we encourage others to rethink core paramedicine systems on an ongoing basis. Given the current healthcare landscape, we suggest augmenting emergency care with an integrated interprofessional primary care paradigm and axiology. This approach emphasizes relationality and criticality, is responsive to contemporary health care challenges, integrates advances in health care practices, and is intended to promote better alignment with existing use of the service by the public. Implementation of this model is underway and is, in some ways, redefining what we mean when we say paramedicine or paramedic systems as more than the availability of emergency medical services.
Implementation of such a model is expected to be challenging. For instance, existing primary health care services in Canada are isolated from paramedicine services. Healthcare integration, in general, continues to be challenging even when working under similar governance structures and mandates and a willingness of health professionals to work collaboratively. Some have leveraged community paramedicine models to support the primary care crisis in Canada. However, integrating interprofessional primary care teams that are not colocated is challenging even in these isolated programs,23,42,89 and even when leaders of organizations and health professions are supported by government mandates and share a collective will. These challenges have not been sufficiently overcome, explaining in part why core paramedicine systems with more restrictive guiding paradigms and infrastructure have not observed needed changes, despite evidence that shows receptiveness for change by the public. 90
This leaves team-based models without the inclusion of core paramedicine systems (a large geographically dispersed healthcare resource) and core paramedicine systems without the inclusion of other primary healthcare providers. However, enabling factors have been identified, including the need to shift professional culture and identity, enhance knowledge, promote a shared understanding of paramedicine, integrate data environments, leverage advanced technologies, and advance policy, regulation, and legislation. 17 At the Ministry of Health in Ontario, some of this policy change is underway with the availability to propose new Patient Care Models. 91
Elsewhere calls have been made for the inclusion of paramedicine as a primary healthcare resource. For example, the Australasian College of Paramedics recently advocated for the employment of paramedics in primary care clinics as part of interprofessional teams. 92 Researchers in the United Kingdom have made similar arguments, demonstrating paramedics' capabilities and the opportunities associated with engaging paramedics in these settings.26,82 While this research has for some time suggested that the competencies and services paramedics are providing in primary and urgent care settings can or should be brought into core paramedicine systems, this has not translated into significant change. As a result, in many jurisdictions across Canada and internationally, paramedicine systems remain underprepared—structurally, conceptually, or technically—to navigate what tends to be the more common needs of the public they engage with. IMPACC proposes to stimulate that change.
Our argument is not that paramedicine alone is the solution to healthcare strain. Several juxtapositioned approaches may be necessary to make headway in ensuring access to integrated health and social care. 58 Rather, our argument is that healthcare is an ever-changing challenge, and the guiding paradigm that has shaped paramedicine has led to a growing disconnect between the existing infrastructure and those changes. The existing guiding paradigm has left blind spots in paramedicine systems and has led to a state where most patient needs could be better served than they currently are. It is this—the alignment issue—that has prompted us to argue for an additional lens on which to augment and guide core paramedicine system design without replacing its necessary emergency function in our healthcare system.
Going forward, at least five initiatives will require attention and may serve as a roadmap in addition to the enablers identified above. These follow, first and foremost, a willingness to augment the emergency focus of core paramedicine systems. These next steps support that call to action. First, ongoing interest-holder engagement, including healthcare providers, policymakers, data teams, administrators, government, and the public, will be needed to better understand and build support for the proposed changes and ensure their successful implementation. Further, this shift may represent identity shifts not welcome by all and in particular the health care providers whose work this may affect most. Second, there will be a need to refine the competency framework and educational strategies to support training in interprofessional collaboration and community-based primary care concepts. Our contribution has included a preliminary competency framework and the inclusion of those competencies into national frameworks intended to support that effort. Should IMPACC be pursued, new educational models, frameworks, accreditation standards, and more will need to evolve with it. Third, advocacy for ongoing policy changes locally, provincially, and across partnering organizations that support the integration of paramedics into interprofessional primary care teams will be needed. Fourth, shared implementation projects of the IMPACC model (even if flexibly enacted) with linked rigorous and new quality-based evaluation efforts will be needed to test and refine the concept. To enhance scalability and sustainability, it is essential to systematically gather and share data, insights, and challenges encountered during these initiatives. Achieving this requires a shared conceptual framework supported by a robust infrastructure and well-connected, communicative groups. Additionally, leveraging tools from implementation science will be crucial in facilitating these processes and ensuring that efforts are coherent and aligned across different teams and initiatives. Fifth, partnerships with academic centers and scientists supported with funding, access to data, and autonomy to examine the impact of these changes on healthcare outcomes, patient and provider satisfaction, system efficiency, and health economics (to name a few), will be needed to inform further refinements and scale-up efforts.
Our analysis, synthesis, and proposed directions are intended as stimuli for further debate and discussion. While these ideas have been derived based on an analysis of the Canadian context and, therefore, are contextually bound, they provide a way forward that can and should be discussed and shared internationally.
Conclusion
Paramedicine in Canada stands at a pivotal juncture. The traditional emergency-focused paradigm is increasingly misaligned with contemporary healthcare challenges and needs of the public. This necessitates a shift toward paradigms that also include an integrated, interprofessional, community-based primary health, and social care ethos and axiology. The IMPACC strategy, concept, and model of care offers a viable blueprint for this transformation, proposing a redesigned core paramedicine system that incorporates primary care services and fosters interprofessional collaboration and integration of care for both differentiated and undifferentiated patients in the community. This model may not only enhance the alignment of paramedic services with public needs but also supports broader healthcare system goals of improving timely access, integration, and care coordination and continuity.
Supplemental Material
sj-docx-1-pam-10.1177_27536386241300216 - Supplemental material for Redesigning paramedicine systems in Canada with “IMPACC”
Supplemental material, sj-docx-1-pam-10.1177_27536386241300216 for Redesigning paramedicine systems in Canada with “IMPACC” by Walter Tavares, Sanne Kaas-Mason, Chris Spearen, Natalie Kedzierski, Jeremy Watts, Phil Moran and Matthew S Leyenaar in Paramedicine
Footnotes
Acknowledgements
The authors extend their gratitude to professional, leadership, and academic colleagues whose insights have significantly contributed to the development of the ideas discussed in this paper. Special thanks are owed to the clinicians who continually refine and implement these concepts in real-world settings. The authors also appreciate the valuable feedback from both formal and informal reviewers, whose efforts have greatly enhanced the clarity of this manuscript.
Declaration of Conflicting Interests
Author Walter Tavares is a member of the Editorial Board of Paramedicine. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Correction (October 2025):
In this article, “Declaration of conflicting interests” section has been updated.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.