
Abstract
Introduction
Previous evaluations of paramedic-to-general practitioner (GP) referrals have focused on subsequent emergency department presentations or ambulance representations; however, we aimed to appreciate patient adherence where paramedics have recommended follow-up with a GP.
Methods
This was a prospective cohort study of adult patients in Victoria, Australia, who were referred to a GP by a paramedic over a 28-day period in June 2021. Patients were then contacted within five days to determine subsequent GP attendance.
Results
Of the 752 patients who met the inclusion criteria, 47% (n = 353) consented to participate. At the time of the survey, 65% of patients had followed up with their GP, with a further 15% booked in for a future appointment. Factors associated with the increased adjusted likelihood of the participant following up with a GP after paramedic referral included female gender (adjusted odds ratio [AOR] 2.21, 95% confidence interval [CI] 1.22–3.99, P = 0.009) and those given a specific time frame for the follow-up appointment by the paramedics (AOR 3.98, 95% CI 2.26–7.02, P < 0.001). Participants who presented to ambulance services overnight were less likely to follow up with a GP (AOR 0.34, 95% CI 0.17–0.68, P = 0.002). The three most commonly stated reasons for not following up with a GP were that the patient felt it was unnecessary (n = 48), their regular GP was unavailable (n = 33) or they had followed up with an alternative service (n = 31).
Conclusion
Most patients who are referred to a GP by attending paramedics will follow up with a GP within 72 h. The most common barrier to GP follow-up is the patients’ perception that follow-up is unnecessary.
Introduction
Traditionally, ambulance services have been staffed by non-medical officers and performed a simple first aid and transport role. This is reflected in the World Health Organisation ‘Emergency care system framework’ that maintains a focus on the role of the ambulance as a mechanism of transport to a traditional hospital setting for patients who require emergency management. 1 However, in many countries including Australia, ambulances are now staffed by paramedics who are university-educated and registered and are increasingly exposed to low-acuity patients with chronic and complex healthcare needs.2,3 Internationally, ambulance service usage continues to grow disproportionate to that of population growth and overall emergency department (ED) demand with a large proportion of this service usage for patients calling with low-acuity conditions.4,5
Australian paramedics have a responsibility to ensure they promote the wise use of healthcare resources that are ‘appropriate, necessary and likely to benefit the patient’. 6 Similarly, paramedics in the United Kingdom maintain a responsibility to ‘be able to make a decision about the most appropriate care pathway for a patient and refer patients appropriately’ and the Clinical Procedures and Guidelines for personnel within the New Zealand Emergency ambulance sector explicitly state that ‘not all patients assessed by ambulance personnel require referral to a medical facility’.7,8 In jurisdictions such as these where paramedics are expected to perform a role as systems gatekeepers, low-acuity patients can be provided with advice by paramedics on scene and referred to their general practitioners (GPs). In the Australian context, the GP is the primary care physician who provides a ‘holistic, patient-centred and relationship-based approach’ whilst acting as care coordinators and systems stewards. 9 As such, GPs are often better placed to provide complex and ongoing care for low-acuity patients than ED physicians. Subsequently, this referral mechanism also reduces potentially avoidable ambulance conveyance and ED presentations. Avoidable presentations to an ED are burdensome for both the individual patient and the wider community.10–12
Whilst increasing linked data literature offers the opportunity to explore adverse events from these referrals such as subsequent ED presentation, hospital admission or death,13,14 it is currently unclear what proportion of patients will proceed to attend their GP if advised to by a paramedic. Due to the nature of their practice, paramedics are unable to individually follow up with these patients to determine if they have attended their GP or required further management. To ensure the safety of the paramedic-to-GP referral process, it is important to establish whether there is continuity of care for these patients.
As the promotion of referral pathways is relevant in the current paramedic setting, this study aims to quantify patient behaviour when paramedics have recommended follow-up with a GP. This will be achieved by:
Quantifying the percentage of patients who attend their GP following a paramedic referral. Identifying the patient and referral factors that increase or decrease the likelihood of GP attendance following a paramedic referral.
Methods
Setting
Ambulance Victoria (AV) is the sole provider of emergency medical services for Victoria, Australia, covering a total land area of approximately 227,500 km2 and a population of 6.7 million residents. AV employs approximately 4,500 full-time equivalent operational clinical staff and operates on a ‘user-pays’ system with free access for those of lower socio-economic status or persons who have inclusive private health cover or ambulance insurance. 15 Telephone calls to the emergency services telephone number (000) are initially triaged by non-medical call-taking staff and may receive an immediate ambulance response or be transferred to secondary phone triage with a registered health professional to discuss alternative care options. 16 Approximately 18% of 000 callers do not receive an ambulance response following this secondary triage process. 15 Paramedics employed by AV have tertiary qualifications and maintain registration through the Paramedicine Board of Australia, administered by the Australian Health Practitioner Regulation Agency. Ambulance Victoria maintains ‘red flag’ criteria for patients at risk of serious deterioration who must be recommended ambulance conveyance to an ED 17 however outside of this criteria, paramedics are considered independent healthcare practitioners and are not required to undertake medical consultation regarding patient management or referral.
This study was conducted over a 28-day period from June to July 2021. This time frame was in between COVID-19 pandemic peak periods. Stringent stay-at-home orders were enacted in Victoria, Australia, during pandemic peak periods; however, at the time of this study, there were no stay-at-home orders except for those isolating due to COVID-19 infection or close contact. Schools, medical centres and public transport were open, although health care settings did not allow visitors unless they were a carer for the patient or for end-of-life reasons. 18 During the study period, residents were able to bulk-bill telehealth consults through federal funding regardless of the patients COVID-19 infectious status.
For the purposes of this study, patients are considered to be ‘referred to GP’ if the treating paramedic lists the case outcome as GP referral on the paramedic-written electronic Patient Care Record (ePCR). The ‘case outcome’ is taken from a pre-defined drop-down menu of incident outcomes, which is a mandatory data item for all ePCRs. At the time of the study, this list had some options which are not mutually exclusive to the outcome of ‘referred to GP’ such as ‘ambulance transport not required’ and ‘patient refused transport’, that is, a patient may refuse ambulance conveyance and subsequently be referred to a GP in the course of safety-netting. This case could be documented as referred to GP or patient refused transport. This introduces some heterogeneity into the cohort in regard to the nature and strength of the recommendation to follow-up.
Paramedics referral practices are guided by the ‘Non-transport checklist’ in the AV Clinical Practice Guidelines 17 ; however, this is the first study to provide insight into the actual referral practices of AV paramedics.
Participants
This study is a prospective cohort study of all adult patients seen by an AV paramedic with a contact phone number. To be eligible for inclusion, the ePCR was required to list the case outcome as referred to GP. Patients were excluded if they resided in a supported accommodation facility or if the ePCR indicated the patient had a cognitive impairment.
To combat the Hawthorne effect, operational paramedics were not aware of the study, and patients were not advised of the study until three to five days after their ambulance attendance when researchers contacted patients by phone. If the patient did not answer the initial call, a voicemail message was left informing the patient of a follow-up phone call in 24 h. If the patient did not answer on the second call, a contact phone number for the research team was provided to which they could reply if they wished to participate. Once telephone contact was made the researcher read an explanatory statement to the patient including acknowledgement that the interview would be audio recorded. Explicit consent to proceed was then sought.
Data collection
Once explicit verbal consent was sought, the participant's age, gender, and postcode (as per the paramedic ePCR) were confirmed. Postcode was then used to determine rurality as per the Australian Statistical Geography Standard: Volume 5 – Remoteness Structure. 19 There were no financial incentives provided to participants, and interpreters were offered and used where required.
The interview consisted of a verbal survey containing three domains. The first domain is related to demographics and regular GP relationship. The second domain related to the paramedic referral and participants were asked to recall and recount the components of the paramedic referral, such as whether they were given an explicit timeline to follow up with their GP or given any paperwork to give the GP. The third domain related to the outcomes of ambulance attendance and participants were asked if they had followed up with their GP or planned to do so, and if there were any barriers preventing them from doing so. Questions were multiple choice with ‘other’ options if the multiple-choice selections were not applicable. For the primary complaint from the AV attendance, paramedics are only able to record a single primary complaint. These complaints were extracted from the ePCR and categorised by the researchers into (1) no problem identified, (2) pain (without further elaboration in PCR), (3) injury, (4) mental health and/or substance use, (5) cardiorespiratory, (6) gastrointestinal and (7) neurological. Additional complaints where n < 5 were combined into (8) other medical.
The data collected during the study, including the audio recordings, remain the property of AV and are stored securely within the AV data warehouse.
Statistical analysis
As the primary aim of the study was to determine the prevalence of patient who attends their GP following a paramedic referral, sample size was estimated utilising the formula n = (Z2 P(1-P))/d2 where n = sample size, Z is the Z statistic for a level of confidence of 95%, P is the estimated proportion of 0.7 and precision of 0.05. Due to the novelty of this study in the realm of GP follow-up after paramedic referral, the estimated proportion was guided by previous studies into GP follow-up after ED presentation.20–23 The estimated required sample size was 323. Utilising previous rates of GP referral per year supplied by AV and an estimated response rate of 50%, it was calculated that a 28-day study period would allow recruitment of the estimated required sample size.
Variables are presented with descriptive statistics and initial bivariate analyses using the two-sample Wilcoxon rank-sum (Mann–Whitney) test or Pearson's chi-square as appropriate. The outcome of interest (following up with the GP) was treated as a binary variable with participants coded as either: (1) those who had already followed up with their GP or booked an appointment to do so or (2) those who had not followed up with their GP and had no plan to do so for this episode. To determine the 95% confidence intervals for the proportions of participants in each category, we used the normal approximation to the binomial calculation.
A multivariable model was then created to determine the patient and referral factors that were associated with the likelihood of GP attendance. Variables whose bivariate P-value was 0.20 or less were incorporated into a preliminary multivariable model. A backward stepwise approach was then used to remove variables of the least significance as per their adjusted P-value until all variables remaining in the model had an adjusted P-value of less than 0.05 or their removal led to large changes in the model. The model AUROC is reported and represents the probability that the model will rank a randomly chosen positive instance higher than a randomly chosen negative instance. AUC values range from 0 to 1, with a higher value indicating a stronger model.
Ethics
Ethical approval was gained through Monash University Human Research and Ethics Committee (Project ID 24739) and AV Research Governance Committee.
Results
A total of 752 cases met the inclusion criteria. Of these cases, researchers were able to contact 504 cases (67%), with 353 patients (47%) consenting to participate, as shown in Figure 1.
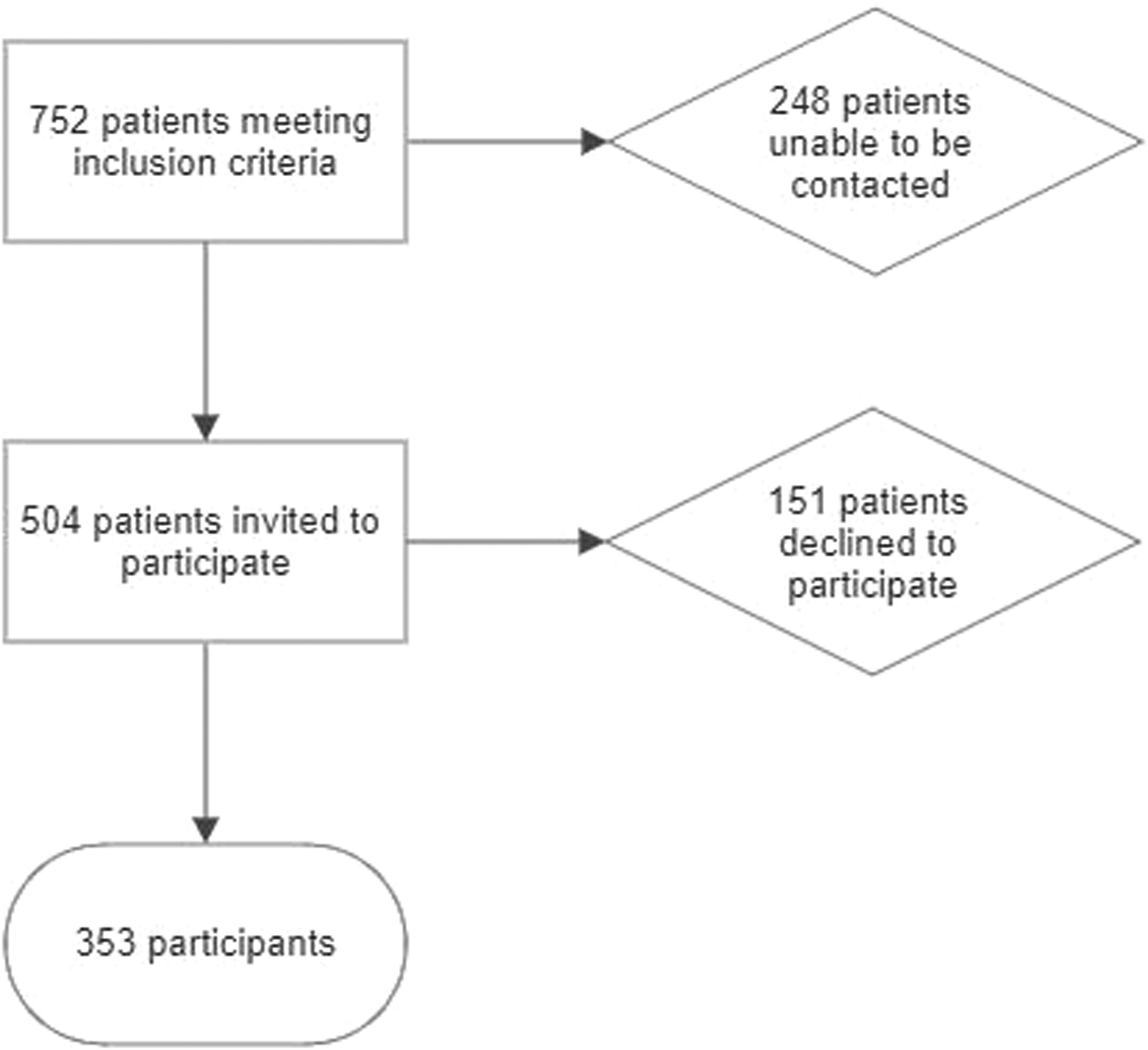
Flowchart showing the number of patients who were contacted and consented to participate in the study.
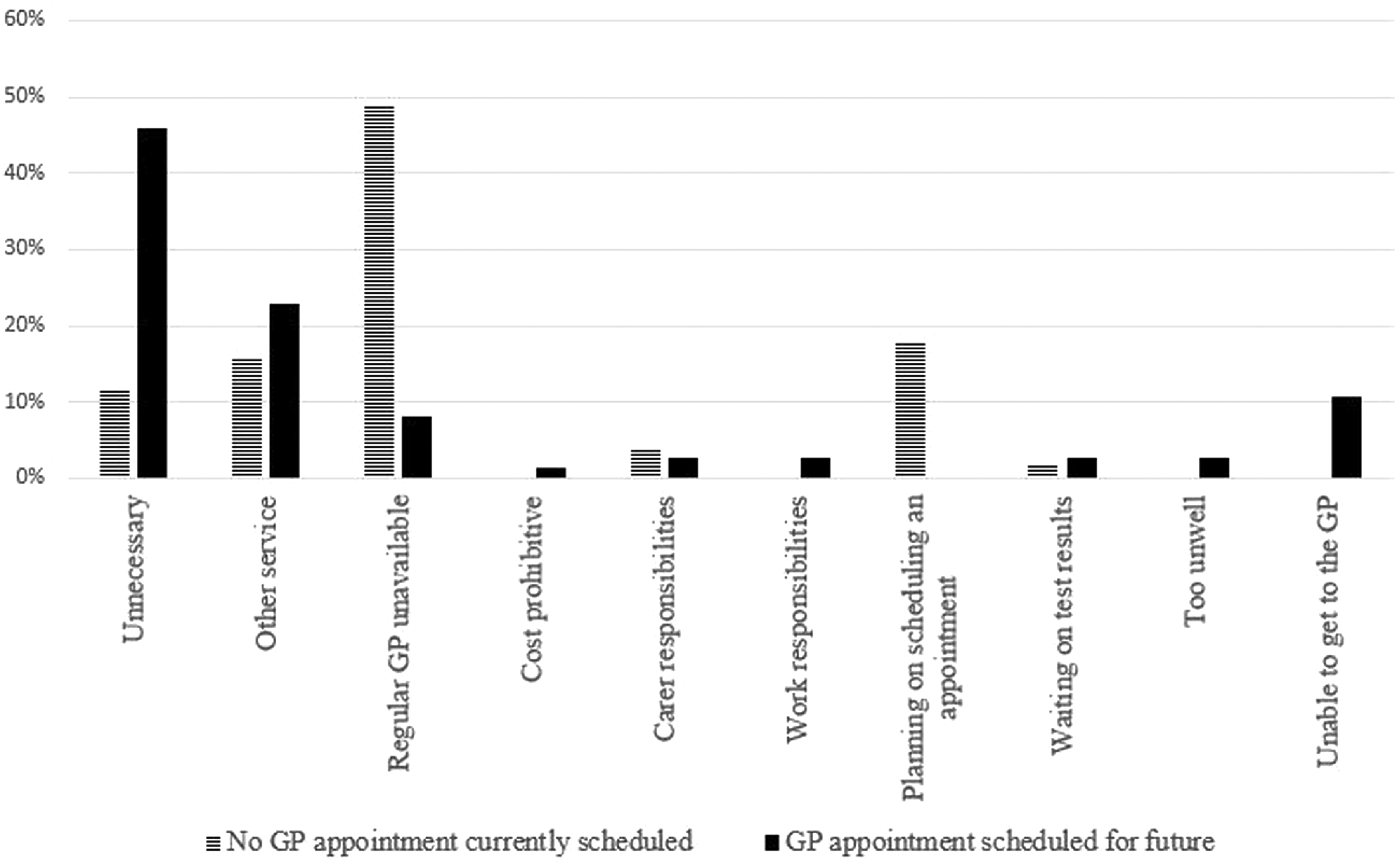
Patient reported reasons for nil GP follow-up after paramedic referral at time of interview.
The proportion of participants who attended or booked an appointment to see their GP was 79% (95% confidence interval [CI] 74–84%). Sixty-five percent (n = 228) of participants had followed up with their GP at the time of the telephone survey, with a further 15% (n = 51) of participants scheduled to see or awaiting a call-back from their GP. The remaining 20% (n = 74) of participants had not seen their GP and did not plan to do so in the following 14 days.
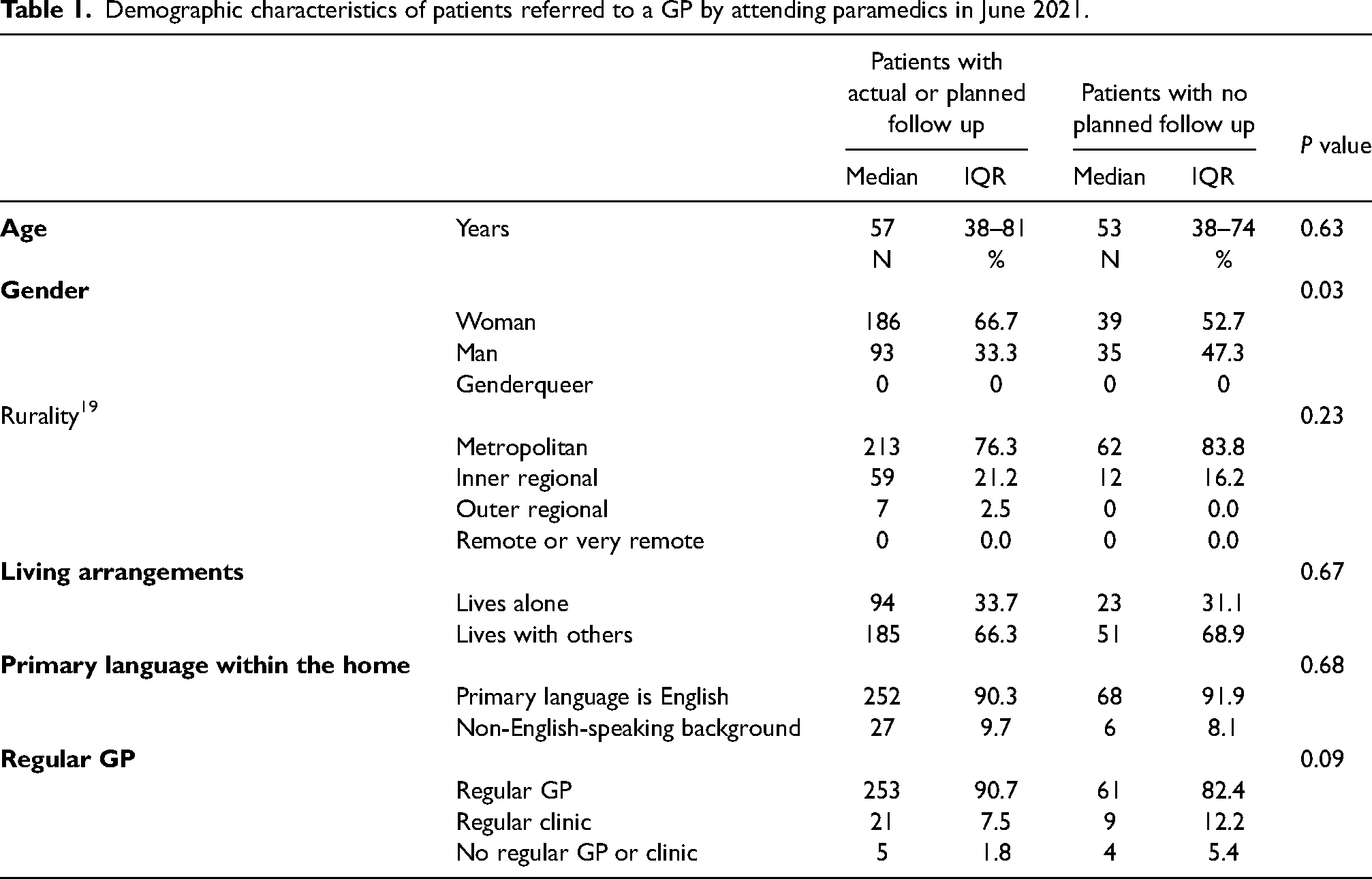
At the time of the survey, 36% (n = 128) of participants described their symptoms as resolved, 45% (n = 160) as improving, 13% (n = 46) as the same as the day they called the ambulance, and 5% (n = 18) as worsening. Demographic details of the included participants are shown in Table 1.
Demographic characteristics of patients referred to a GP by attending paramedics in June 2021.
Factors related to the ambulance attendance and the participant's recollection of the paramedic referral process are shown in Table 2. Eleven percent (n = 37) of participants were unable to recall being referred to their GP by the attending paramedic even when the paramedic had indicated that a referral had been made. Overall, only 15% (n = 53) of participants reported that the paramedic had booked an appointment for them, written a referral, or spoken directly with their GP.
Paramedic-led factors for patients referred to a GP by attending paramedics in June 2021.
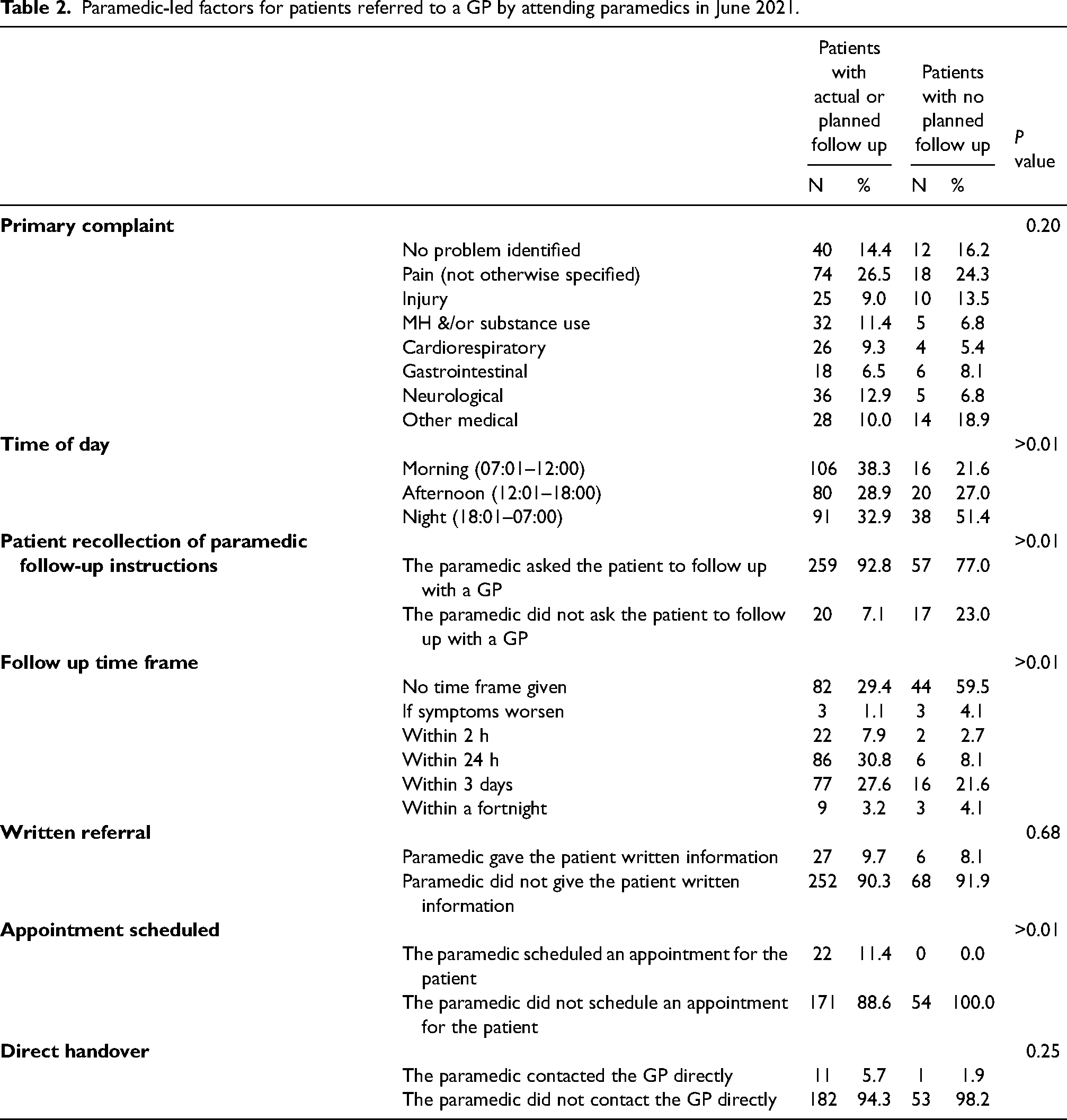
Of the 228 participants who had followed up with their GP, 83% (n = 189) had their appointment face to face, compared to 17% (n = 39) who had a telehealth appointment. There were 221 participants who recalled being given a specific time frame by the paramedic to follow up with their GP and 64% (n = 142) were able to do so within that time frame. Following the paramedic attendance, 9% (n = 21) of participants had seen their GP within 2 h, 33% (n = 74) between 2 and 24 h, 54% (n = 122) between one and three days, and 5% (n = 11) between three days and two weeks. Of the 22 participants who had a GP follow-up scheduled by the paramedic on-scene, 91% (n = 20) had followed up with their GP at the time of the survey. Paramedics were more likely to assist with booking an appointment during the day compared to overnight (9% vs 2%, P = 0.006).
The majority (94%) of participants informed their GP that an ambulance had attended to them and requested the follow-up appointment. Participants who had not yet followed up with their GP were asked to identify why they had not yet done so and could select multiple reasons, as shown in Figure 2. Of those who did not currently have a GP appointment scheduled, the most frequent response was that their regular GP was unavailable. Of those who had a GP appointment scheduled for the future, the most frequent response was that they felt a sooner GP appointment was unnecessary. For participants who chose to follow up with an alternative service: 52% (n = 16) self-presented to ED, 33% (n = 10) indicated they were following up with their specialist, 6% (n = 2) followed up with an allied health practitioner, 6% (n = 2) with a mental health service and 3% (n = 1) recalled an ambulance.
After adjusting for gender, whether the paramedics indicated a specific time frame for follow-up appointment to the patient, time of call and nature of complaint (shown in Figure 3), several factors were associated with the likelihood of the participant following up with a GP after paramedic referral. Female gender was associated with an increased likelihood (adjusted odds ratio [AOR] 2.21, 95% CI 1.22–3.99, P = 0.009). A specific time frame for follow-up appointment indicated by paramedics was also associated with an increased likelihood (AOR 3.98, 95% CI 2.26–7.02, P < 0.001). In contrast, overnight presentation to ambulance services was associated with a decreased likelihood of GP follow-up (AOR 0.34, 95% CI 0.17–0.68, P = 0.002). The model had an AUROC = 0.75 indicating the model performs well and can accurately identify if a patient will or will not follow up with a GP after paramedic referral from the factors included.
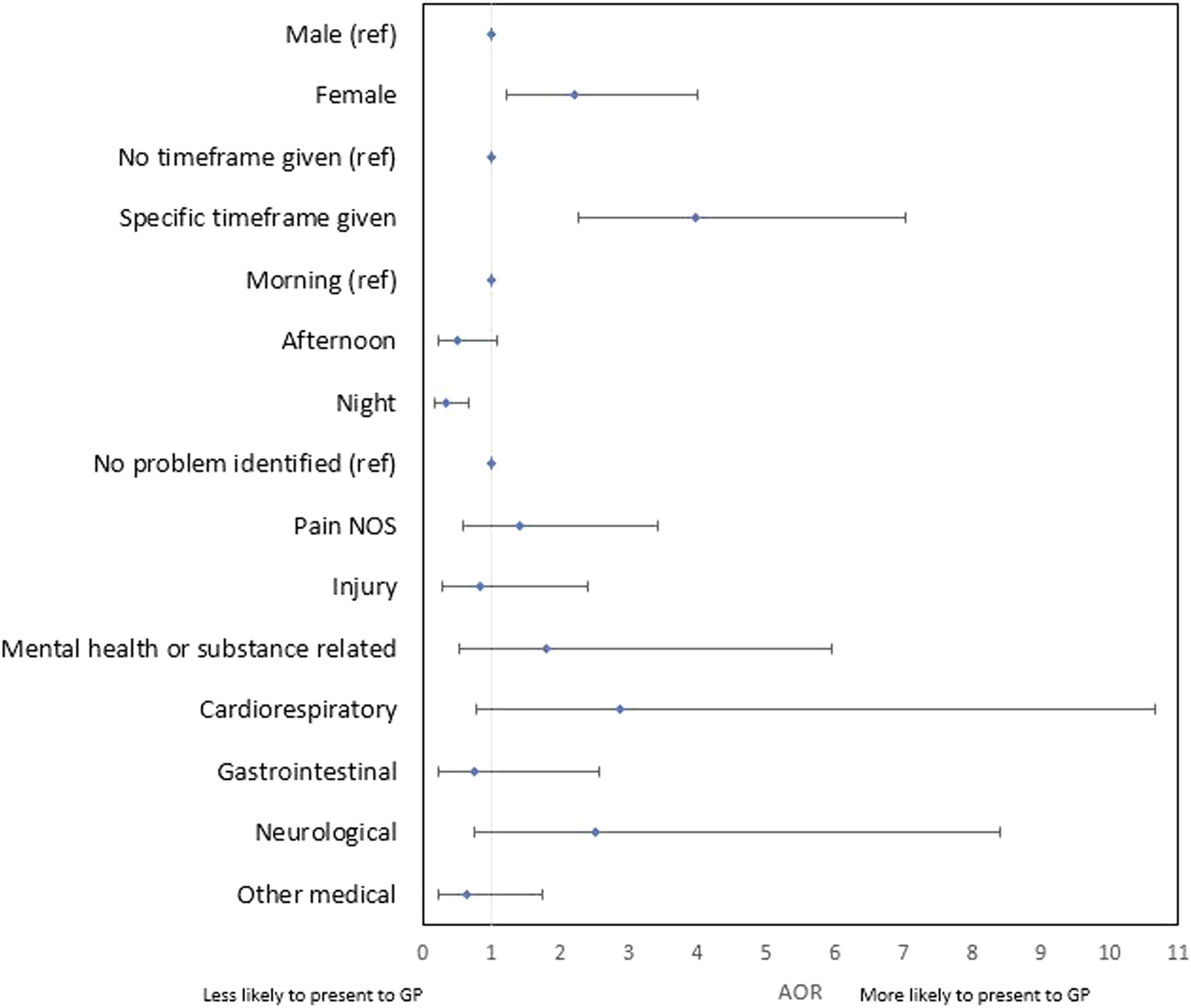
Multiple logistic regression investigating factors associated with GP attendance following paramedic referral to GP.
Participants who presented at night were twice as likely to report that further follow-up was unnecessary compared to participants who presented during the morning or afternoon (odds ratio [OR] 2.32, 95% CI 1.25–4.29, P = 0.007). There were no other statistically significant reasons noted regarding the time of ambulance presentation and subsequent GP follow-up. Participants who were not given a specific time frame were associated with multiple reasons for lack of follow-up including reporting that they had followed up with an alternative service (OR 3.41, 95% CI 1.58–7.37, P = 0.002), their regular GP was unavailable (OR 2.49, 95% CI 1.20–5.15, P = 0.014) or that further GP follow up was unnecessary (OR 3.68, 95% CI 1.95–6.97, P > 0.001).
Discussion
Previous research has examined the outcome of paramedic non-conveyance in terms of adverse events such as ED attendance, ambulance reattendance or mortality24–26 or patient satisfaction.27–29 This novel study provides new insight into patient behaviours after paramedics do not convey patients and make a referral to a GP. The majority of patients in this study who were referred to GPs by paramedics subsequently followed up with their GP or planned to do so, with almost half (27%) able to follow up with their GP on the same day.
The most influential predictor of subsequent GP follow-up was the paramedic booking an appointment for the patient with their GP whilst still on-scene, although this was not included in the multivariable logistic regression model as it was a perfect predictor. Following this, specifying a time frame to the patient in which they should follow up with their GP tripled the likelihood of the patient doing so, regardless of the actual time frame suggested. This may be indicative of a more structured referral by the paramedic inducing a sense of urgency around the follow-up, or increased compliance in the setting of clear instructions. The results of this study also showed that patients who were seen by paramedics overnight were 65% less likely to follow up with a GP and twice as likely to report that follow-up was unnecessary. Upon further analysis, no correlation was found between the time of presentation and follow-up with alternative services such as the ED, indicating that this patient cohort may be less likely to perceive a need for any additional care. It is unclear if this difference is driven by the quality of reassurance and health education offered by paramedics overnight, the role of watchful waiting or symptom severity, although there were no differences found regarding the time of presentation and the nature of the patient complaint. Further research exploring this phenomenon is warranted.
The most common reason for a lack of GP follow-up was the unavailability of the patients’ regular GP. Whilst 97.5% of Australians over the age of 45 have a usual GP or usual place of care, a quarter of Australian Survey of Healthcare respondents report not seeing a GP when they felt they needed to and GP availability was a primary barrier. 30 A significant proportion of the participants in the current study had not booked any follow-up care with a GP, which raises the potential opportunity for increased GP follow-up adherence if paramedics routinely assist patients to book follow-up appointments as part of the referral process. This may also include speaking directly to the practice to find the next available appointment or assisting the patient to find GPs in their area with increased availability. Previous studies have shown that patients demonstrate a lack of confidence in GPs compared to ED physicians for acute non-emergencies despite GP capabilities.14,31–33 This barrier may be amenable to paramedic reassurance and assistance with appointment scheduling.
Previously, men have been shown to be more likely to request an ambulance for non-emergent conditions compared to women.34–36 Men in Australia were also less likely to see a GP for any reason and have less Medicare-subsidised GP services per person per year than women. 37 Within our study, men were significantly less likely to follow up with GPs after paramedic referral. This indicates that men may be at higher risk of interrupted care which is important for future policy planning and education regarding paramedic-to-GP referrals. In contrast to gender, patient factors are generally seen to increase isolation and vulnerabilities such as increasing age, non-English speaking background, regional location and living alone were not associated with reduced follow-up.
It is important to note that 10% of patients who were listed on their ePCR as ‘referred to GP’ did not recall the paramedic referral. It is unclear whether this misunderstanding occurred during the patient care episode as a communication error between the treating paramedic and the patient, during the documentation phase as a recall error on the paramedics’ behalf, or during the survey as a recall error on the participants’ behalf. There is also a possibility that the question was misunderstood or misinterpreted between the researcher and the participant. Plain, consistent language (i.e., ‘did the paramedic ask you to follow up with your GP?’) was used to minimise jargon on the researchers’ behalf. Paramedics are generally risk-averse regarding non-conveyance, and handover or referral to another practitioner is seen to reduce the personal and professional liability of the paramedic. 38 The ‘referral’ may have been tokenistic (i.e. ‘I don’t think you need to go to hospital, but you could see your GP’) and documented as ‘referred to GP’ without a structured referral plan communicated to the patient. A tokenistic ‘referral to GP’ where neither the paramedic nor patient felt follow-up was important may offer an explanation as to why the second most common diagnosis for patients referred to a GP is ‘no problem identified’, and the frequency of patients omitting, or postponing GP follow up as they found it unnecessary. Previous literature has focused on whether patients are appropriate to be referred to a GP in lieu of ambulance conveyance, or GP referral compared to other alternative pathways 39 ; however, there is a need for future research to identify if all non-conveyed patients require or benefit from further follow-up care.
Limitations
This study relied on patient recall that has been shown to be impaired following acute healthcare events and as such the authors chose the three-to-five-day follow-up period which has been demonstrated as the optimal recall period for healthcare-related research.40–43 The research team attempted to utilise neutral language during the study explanation and consenting process – or the voicemail messages left for the proportion of uncontactable patients – to encourage open dialogue between the researcher and patients. Nevertheless, there is an appreciable risk of participation bias within this study, in particular, the possibility that the GP follow-up rates of eligible patients who did not participate in the study could differ from those who did participate. This may be a significant factor if the patients who were unable to be contacted by telephone or those who refused to participate once contacted did so because they had not followed the paramedics’ recommendation to consult a GP and did not want to be confronted with questions about it in the survey. This could potentially affect the overall findings of the study and should be considered when interpreting the results. Future objective data collection, such as the linkage of ambulance records with GP Medicare rebate data, may assist in validating the results of this study in the Australian context.
Furthermore, whilst the authors conducted the research outside of a COVID-19 lockdown period, and GPs were able to provide Medicare-rebated telehealth consults, it is known that many patients delayed both urgent and routine care during the COVID-19 pandemic.44–46 Despite this, there were no participants who specifically mentioned COVID-19-related reasons for lack of follow-up with a GP, although some patients did utilise a telehealth consult in lieu of face-to-face consultation.
Whilst the diversity of the geographical area in which the data was collected does give some confidence in the generalisability of the results between both metropolitan and regional areas, it should be acknowledged that the sample was taken from a single month period, which may reduce the generalisability of the results. An extended period of data collection may have provided greater insight into this topic, however, to protect the privacy of the participants, all phone calls were required to be made on-site at an AV location using AV-recorded phone lines. This created logistical issues for the research team due to frequent COVID-19 workplace attendance restrictions and made it infeasible to utilise a larger data collection period, which may have hindered the generalisability of the results. Further research validating the results of this study outside of the COVID-19 pandemic environment would be beneficial.
Conclusion
This study offers novel insights into patient behaviour with paramedic-initiated GP referrals. Although one in ten patients was unaware they had been referred to their GP, most patients who are referred to a GP by attending paramedics do follow up with a GP within 72 h. Paramedic referral practices that increased the likelihood of the patient following up included giving a specific time frame in which to follow-up, and assisting in booking the follow-up appointment. Men, and patients attended by the ambulance at night, are less likely to follow up with their GP, which may have implications for the continuity of care for these at-risk groups. Reasons for lack of GP follow-up include patient perception that follow-up is unnecessary, patients’ regular GP is unavailable and/or the patient has followed up with an alternative service such as the ED.
Footnotes
Author Contributions
The authors confirm their contribution to the paper as follows: Study conception and design: Delardes B, Smith K, Chakraborty S and Bowles KA. Data collection: Delardes B and Prakash S. Analysis and interpretation of results: Delardes B, Prakash S, Chakraborty S, Smith K and Bowles KA. Draft manuscript preparation: Delardes B, Prakash S, Chakraborty S, Smith K and Bowles KA. All authors reviewed the results and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Kelly-Ann Bowles is an Associate Editor of Paramedicine.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Correction (September 2023):
This article has been updated to disclose the Declaration of conflicting interests statement.