
Abstract
Objective:
To describe trends in the pediatric mental health care continuum and identify potential gaps in care coordination.
Methods:
We used electronic medical record data from October 2016 to September 2019 to characterize the prevalence of mental health issues in the pediatric population at a large American health system. This was a single institution case study. From the electronic medical record data, primary mental health discharge and readmission diagnoses were identified using International Classification of Diseases (ICD-9-CM, ICD-10-CM) codes. The electronic medical record was queried for mental health-specific diagnoses as defined by International Classification of Diseases classification, analysis of which was facilitated by the fact that only 176 mental health codes were billed for. Additionally, prevalence of care navigation encounters was assessed through electronic medical record query, as care navigation encounters are specifically coded. These encounter data was then segmented by care delivery setting.
Results:
Major depressive disorder and other mood disorders comprised 49.6% and 89.4% of diagnoses in the emergency department and inpatient settings respectively compared to 9.0% of ambulatory care diagnoses and were among top reasons for readmission. Additionally, only 1% of all ambulatory care encounters had a care navigation component, whereas 86% of care navigation encounters were for mental health-associated reasons.
Conclusions:
Major depressive disorder and other mood disorders were more common diagnoses in the emergency department and inpatient settings, which could signal gaps in care coordination. Bridging potential gaps in care coordination could reduce emergency department and inpatient utilization through increasing ambulatory care navigation resources, improving training, and restructuring financial incentives to facilitate ambulatory care diagnosis and management of major depressive disorder and mood disorders. Furthermore, health systems can use our descriptive analytic approach to serve as a reasonable measure of the current state of pediatric mental health care in their own patient population.
Introduction
Over the last 20 years, there has been a 60% rise in mental health (MH)-related emergency department (ED) visits 1 and a 68% increase in MH-related inpatient (IP) hospitalizations among children in the United States. 2 It is estimated that 13–20% of children aged 3–17 years will experience a MH condition in a given year with the majority receiving either suboptimal or no treatment; with increasing costs to payors.1–4
Care coordination is a best practice that improves outcomes and reduces hospitalizations but is not universally used.5,6 It is broadly defined as a process that links those with care needs with resources and services across the care continuum, from prevention to early diagnosis and coordinated individualized support and treatment services (i.e. wraparound services), 7 with the aim to achieve desired health outcomes. 6 However, such a model is not in widespread use, despite its previously demonstrated efficacy to improve outcomes. 8
For example, when comparing a standard-care cohort with a cohort receiving coordinated, patient-centered care through the federal Substance Abuse and Mental Health Administration’s Children’s Mental Health Initiative, which included an expanded set of home and community-based individualized services and enhanced communication across the care continuum, Stroul et al. 9 showed fewer hospitalizations and ED visits for MH problems. The authors also reported a 42% cost reduction in the IP setting and 57% cost reduction in the ED for MH-related visits. Additionally, children receiving coordinated care were found to be less likely to get arrested and drop out of school, and had lower suicide rates. 9
Care coordination is an essential part of other best practice care delivery models such as patient-centered medical homes (PCMHs), which consolidate care provision and facilitate interprofessional collaboration. 6 However, over 43% of children with MH conditions are reported to have unmet care coordination needs. 6
The goal of this study is to track pediatric MH utilization within a health system’s care continuum in order to identify access and capacity issues and gaps in care coordination and communication across care delivery settings. 5 Current literature evaluates pediatric MH care utilization separately for the ambulatory care (AC)—restricted to primary care for the purposes of this study—ED, and IP settings and indicates a potential lack of insight into care coordination across these care delivery silos.5,10,11 To address this critical knowledge gap, we evaluated patient encounter data across care settings in one large health system as part of a 1-year, mixed methods quality improvement (QI) project, which also had a broader goal of characterizing opportunities for improvements to care coordination and patient-centered care. 12 For the purposes of this study, the authors focus on care coordination as the concept of interprofessional care delivery between ED, IP, and AC settings. The broader QI project involved community health statistics obtained from the state Department for Health and Human Services, patient utilization data, patient and provider focus groups and surveys, interviews with key health system stakeholders, an environmental scan of peer-reviewed and grey literature, and quantitative electronic medical record (EMR) data analyses. Here, we present our findings related to pediatric MH care coordination, which are based wholly on EMR data.
We then identified potential care coordination gaps for children with MH conditions from a care continuum perspective, leading to insights that studying encounters within siloed care settings would not provide. Though there are care coordination strategies already employed in the health system under study, such as use of care navigators and tools such as dedicated discharge summaries between IP and AC providers, we discovered additional opportunities for optimizing pediatric MH care coordination and, more importantly, established a conceptual framework for understanding the magnitude of the need for MH care coordination.
Methods
We analyzed EMR data from October 2016 to September 2019 for an academic health center in the Midwestern US which serves as a tertiary/quaternary referral center for suburban/rural populations across the state.
Statistical analysis
Dataset elements and variables related to ED, IP, and AC were identified and analyzed from EMR data from the 36-month date range, which were extracted and compiled by the health system’s Quality Analytics department. MH discharge diagnoses for all children ages 0–18 with documented encounters in the study date range were identified using International Classification of Diseases (ICD-9-CM, ICD-10-CM) codes (WHO, Geneva, Switzerland) through assessment of primary diagnosis (i.e. based on claims-based diagnosis codes). To ensure specificity for MH visits, the analysis was restricted to those with a primary MH discharge diagnosis code. “Mental health diagnosis” codes used can be seen in Supplemental Information and were comprised of the generally agreed upon codes F01–F99, as well as several R codes for suicidal ideation/other emotional states. Encounters with MH related primary discharge diagnoses were then characterized by care setting (i.e. AC, ED, IP). Readmissions for MH diagnoses were evaluated as a stratification variable to gain insight into effectiveness of care transitions between settings of care. Care navigation utilization was tracked for all pediatric AC encounters, which was possible in instances where care navigation encounters were specifically coded as such and was primarily associated with MH conditions. All statistical analyses were conducted using SAS Version 9.4 (SAS Institute, Cary, NC, USA).
This project was deemed exempt from human subjects’ oversight by the institution’s Institutional Review Board.
Results
The health system under study is comprised of three hospitals, inclusive of 1,000 beds, as well as 40 outpatient facilities and 125 clinics. There were 106,451 ED visits and 2.5 million outpatient visits in 2018. Twenty-four percent of patient encounters were for pediatric patients. Seventy-three percent of pediatric patients were White, 10% Black, 5% Hispanic, 5% Asian, and 7% other. Forty-eight percent of pediatric patients were female. Our analysis of the past 3 years of discharge diagnosis data were stratified by number of encounters by care setting. Twenty-four percent of patients seen in the health system during the 3-year span were pediatric patients (⩽18 y.o.). Seventy-three percent of those pediatric patients were White and 52% were male. Our analysis yielded 1,131,054 total pediatric patient encounters during the study period, of which 1,003,697 were AC encounters, 98,981 were ED encounters, and 28,455 were IP encounters. Of the total all-cause ED encounters, 3540 encounters (4.11%) were for major depressive disorder (MDD) and other mood disorders. Of the total all-cause IP admissions, 643 (2.39%) were for MDD.
Of the totals, 40,673 AC encounters, 6,456 ED encounters and 938 IP encounters were associated with MH-specific discharge diagnoses. Pediatric MH care utilization by setting is shown in Figure 1. MDD and other mood disorders were more common in the ED (49.64% of ED MH diagnoses) and IP settings (89.34% of IP MH diagnoses) compared to the AC setting (8.96% of AC MH diagnoses). Of note, 4.0% of all ED MH encounters over the study period were coded as being for “suicidal ideation.” Anxiety disorders were also relatively common in the ED, comprising 4.68% of ED MH diagnoses.
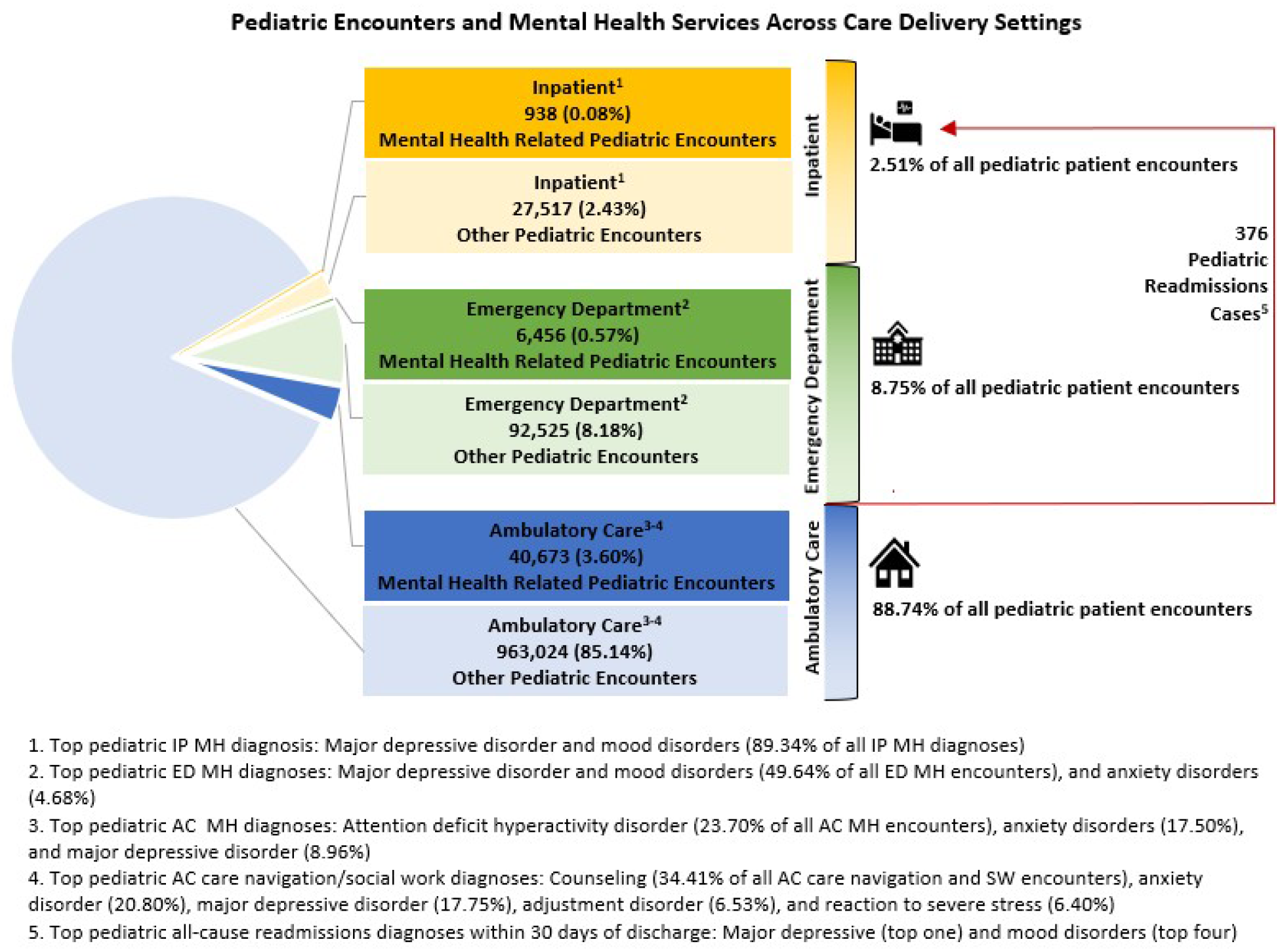
Pediatric mental health-related care utilization and top diagnoses across ambulatory care, emergency department, and inpatient settings.
In the AC setting, the top five diagnoses were anxiety disorders (23.70% of all AC MH encounters), attention-deficit/hyperactivity disorder (ADHD) (17.50%), eating disorders (11.95%), MDD (8.96%), and autism spectrum disorders (8.55%). In the ED setting, the top five diagnoses were MDD (33.61% of ED MH diagnoses), mood disorders (16.03%), anxiety disorders (4.68%), suicidal ideation (4.00%), and conduct disorder (2.94%).
Additionally, there were also 9674 all-cause readmissions to IP care within 30 days of discharge for pediatric patients over the project period, of which MDD and mood disorders composed the top one and fourth most common readmission diagnoses. Only about 1% of all pediatric AC encounters had a care coordination/navigation component, but MH-associated diagnoses comprised a cumulative 85.89% of all care coordination/navigation-associated encounters.
Discussion
Our analysis highlights potential gaps in pediatric MH care coordination across the care continuum in one large health system.
The large number of MH-related ED visits and hospitalizations may indicate a lack of capacity to manage MDD patients in the AC setting. Mood disorders comprised nearly 50% of MH diagnoses in the ED and nearly 90% of IP MH-related diagnoses and were overall top reasons for ED visits and admissions among all-cause ED and IP encounters. A greater percentage of MDD and mood disorder-related visits occurred in the ED and IP settings compared to the AC setting.
Though existing pediatric MH (e.g. depression, anxiety) screening tools have excellent psychometric properties,13,14 one study showed that some practices have reduced the sensitivity of MH screening tools due to insufficient capacity to handle the volume of MDD patients identified. 11 This may explain later escalation to more acute care as many patients go undertreated or even unrecognized in the AC setting. Studies have shown that if screening is conducted for MDD, its purpose and confidentiality is often inadequately explained to patients, which might reduce patient willingness to answer truthfully. 15 Furthermore, screening for MDD faces cultural apathy and resistance due to stigma15,16 and parents may not fully understand or communicate the scope of their child’s MH problem 4 or fail to complete referrals to specialists. 6 This coupled with the incremental cost of time and lack of provider training on MH issues together present a challenging obstacle for many primary care practices to detect and follow up on MH concerns.11,17 Supporting this is literature showing that primary care providers (PCPs) only identify 25% of children with MH conditions. 11 Additionally, it is widely known that there are too few outpatient child psychiatrists who can then provide specialized management for MH conditions. 17
In light of these challenges, one potential opportunity for health systems to improve MDD care across the continuum may be incentivization of training in addressing MH diagnoses for AC providers through education credits and protected time as well as restructuring compensation and utilization targets 18 so that MH care needs of children can be effectively addressed in the AC setting as much as possible. Of course, MDD and mood disorders may present more acutely (e.g. with suicidality), and thus some number of ED and IP encounters will always be for MDD despite best efforts. 19 Increasing AC capacity via phone triage lines, outpatient crisis programs with dedicated care management and counseling, and connection to third-party community programs has seen some success. 20 Additionally, making care more accessible by offering weeknight/weekend hours, same day visits, and telehealth visits, as well as making care more family-centered and compassionate through increased primary care provider MH training would help increase access to PCMH-level care. 3
Despite 86% of care navigation encounters being for MH in the health system under study, with only 1% of all pediatric encounters having a care navigation component, there are still high IP readmission rates for MDD and mood disorders, indicating a potential gap in care coordination and AC capacity. The striking preponderance of MDD and other mood disorders as causes for IP readmission among all causes for readmission suggest deficiencies in transitions of care for MH concerns, such as connecting discharged patients to intensive or dedicated MH care options in the AC setting. The fact that the top five AC care navigation diagnoses are for MH conditions (with MDD being the third top diagnosis) may indicate a lack of resources for addressing complex MH needs for children in the AC setting. Of course, some MH diagnoses may simply just be missed at the AC level. Institutions should increase investments in dedicated care coordination personnel, programs that bridge care settings, and intensive outpatient MH treatment options. 18
Limitations
Our analysis was limited to one health system; however, the analytic framework we utilized can be used in other health systems to identify gaps in care coordination. While using primary discharge diagnoses offered greater MH-related encounter-level specificity, visits with non-primary MH diagnoses were excluded, due to the fact that we did not have secondary discharge diagnoses in our dataset. Therefore, we are likely underestimating the true count of pediatric encounters with a MH component. Future work should attempt to integrate all visits with any component of MH care need. Finally, as a purely retrospective, observational study with access only to discharge diagnosis data, our study cannot comment on the effectiveness (or cost-effectiveness) of proposed training and compensation interventions.
Implications and conclusions
Through analysis of MH diagnosis-related encounters across the care continuum, we identified potential gaps in pediatric MH care coordination and laid the groundwork for how to explore EMR data in pediatric MH care coordination and utilization studies in other health systems. Comparing utilization for conditions such as MDD between the ED/IP settings and AC settings can serve as a useful high-level assessment of an institution’s pediatric MH care capabilities for health system leadership.
Our approach in using typically accessible EMR data across the care continuum should be applicable to other institutions, though different EMRs and data structures at other institutions may warrant tailoring of this approach.
Future work should attempt to justify the investment in such care coordination strategies through evaluating the impact of such interventions on MH outcomes for children (and their cost-effectiveness) to make optimizing care coordination across the care continuum more attractive to health system administrators and policymakers.
Supplemental Material
sj-xlsx-1-smo-10.1177_20503121231181939 – Supplemental material for Evaluating the pediatric mental health care continuum at an American health system
Supplemental material, sj-xlsx-1-smo-10.1177_20503121231181939 for Evaluating the pediatric mental health care continuum at an American health system by Joshua Thariath, Rama A. Salhi, Neil Kamdar, Kristian Seiler, Margaret Greenwood-Ericksen, Wilson Nham, Kaitlyn Simpson, Timothy Peterson and Mahshid Abir in SAGE Open Medicine
Footnotes
Author contributions
JT conducted literature review, developed figures, and drafted, reviewed, and revised the initial manuscript. MA, MGE, and TP conceptualized, designed, and led the study, and critically revised the manuscript for content. RS and K. Simpson assisted with study design and critically revised the manuscript for content. NK and K. Seiler conducted the requisite statistical analyses and critically revised the manuscript for content. WN served as project manager for the study, developed figures and charts, including Figure 1, and critically revised the initial manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NK has a potential conflict of interest of serving as 1) Consulting Methodologist at the University of North Carolina, Sheps Center for Health Policy, Chapel Hill, NC and 2) Consulting Research Statistician at Stanford University, Center for Population Health Sciences, Stanford, CA. The remaining authors have declared that they have no competing or potential conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the institution under study.
This study was funded by Michigan Medicine, the health system of study, as part of a quality improvement project.
The funder/sponsor did not participate in the work other than receiving a final report.
Ethics approval
This requirement was waived by the institutional review board for this study being a quality improvement initiative commissioned by the health system of study.
Informed consent
This requirement was waived by the institutional review board for this study, being a quality improvement initiative commissioned by the health system of study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.