
Abstract
Introduction
The rise of formal degree programs has significantly expanded professional and independent paramedicine systems globally. Paramedicine now includes a wide range of responsibilities, from managing life-threatening conditions to addressing diverse patient needs. However, current education frameworks often lack specificity, being largely adapted from other clinical disciplines. This study aims to provide a comprehensive description of the current state of undergraduate paramedic education concerning paediatric content in Australia.
Methods
A content analysis was conducted on publicly available curriculums from accredited Australian universities offering Bachelor of Paramedicine programs. Initial data analysis involved searching for paediatric terminology in learning outcomes and/or synopses. Subsequent analysis of curricula from institutions that completed member checking comprised two components: a descriptive arm to quantitatively assess paediatric education and an inductive arm to qualitatively explore categories of paediatric curriculum.
Results
Curriculum of 15/16 programs were searched, revealing a median of three units which included paediatric terminology in learning outcomes or unit synopses. Four institutions across five Australian states completed member checking, revealing a national median paediatric content inclusion of 0%. Only 32% of units included any paediatric content, with a median inclusion of 10%. Examination of the hidden aspects of curriculum highlighted discrepancies between learning outcomes and paediatric content percentages. No overarching degree learning outcomes mentioned paediatrics. Unit learning outcomes that had paediatric mention were categorised into three groups: content, conceptual understanding and skills development. Additionally, distribution analysis revealed a notable emphasis on non-technical skills, potentially overshadowing core knowledge essential for paediatric care.
Discussion
The findings underscore the need for curriculum reform, to enhance paramedic student preparedness to manage paediatrics. Scaffolding paediatric content into the curriculum could foster a comprehensive understanding of patient care and mitigate disparities in paediatric management. Collaboration with stakeholders and innovative teaching methodologies hold promise for advancing paediatric education in paramedicine.
Introduction
Paramedicine, as a vital component of emergency medical services (EMS), encompasses a broad spectrum of responsibilities, from addressing social needs to managing life-threatening conditions and attending to patients from all walks of life. 1 However, current education frameworks often lack specificity to the unique dynamics of the field, being largely adapted from more established clinical disciplines like nursing and medicine.2,3 In 2021, Bell et al. highlighted the need for robust research on paramedic education, including the identification of a signature pedagogy. 2
In contemporary Australia, the paramedic profession has transitioned from on-the-job first aid training to university degree programs over the past 50 years, with formal education beginning in the early 1960s through specialised training centres within ambulance services. 4 This evolution is also seen all over the world with similar professionally autonomous systems in New Zealand and the United Kingdom. 5 Paramedics are now recognised as essential healthcare professionals, conducting thorough patient examinations, utilising evidence-based treatment guidelines and formulating individualised care plans.6,7
With the introduction of entry-to-practice degree programs accredited by bodies such as the Australian Health Practitioner Regulation Agency (AHPRA) or the Pre-Hospital Emergency Care Council (PHECC) in Ireland, there has been a notable emphasis on higher education.8,9 The transition from Council of Ambulance Authorities (CAA) accreditation to AHPRA accreditation in 2018 marks a significant advancement, elevating paramedicine to a regulated medical profession and emphasising patient safety and higher standards of practice.7,10
Accreditation is invaluable in setting minimum standards and, when implemented effectively, should encourage individuality and foster the evolution of educational practices, allowing education providers to design their own curriculum, leading to diversity in philosophy and teaching.11–13 However, some critics argue that accreditation can hinder progress and individuality enforcing standards too rigidly.13,14 When accreditation competencies, such as those set by AHPRA, do not explicitly address areas like paediatrics, 15 there is a risk that essential aspects of paediatric care may be overlooked, potentially limiting education in this crucial area.
Paediatrics constitute a minority (4.5–13%) of paramedic cases.16,17 These patients pose unique challenges due to their physiological differences and specialised care needs. 18 These are high-stress, low-occurrence events that require strong foundational knowledge. Drayna et al. (2017) found that limited exposure to these cases results in a low frequency of interventions, even when patients show clear physiological signs of acute illness, often resulting in untreated conditions. 19 Documentation of complete vital signs and condition-specific assessments is also less frequent in children, particularly in younger age groups. 17 This trend is attributed to lower rates of paediatric encounters, inadequate paediatric training for personnel and discomfort among clinicians when dealing with paediatric patients.17,19–21 Paramedics often feel less confident in obtaining vital signs from younger patients, which is compounded by equipment limitations such as improperly sized blood pressure cuffs, although targeted educational interventions have shown promise in addressing these challenges. 22 These disparities in paediatric care may suggest a need for targeted paediatric educational interventions to ensure competence in managing paediatric emergencies.
Health equity is also a critical consideration in paediatric care within paramedicine. Health equity refers to attaining the highest level of health for all people and addressing disparities that affect marginalised and vulnerable populations.23,24 This means ensuring that the paramedic curriculum equitably includes paediatric care. This involves not only covering the general paediatric population but also addressing the needs of various subgroups within paediatrics. Such an approach helps prepare paramedics to meet the diverse needs of paediatric patients comprehensively.
Research conducted in 2009 highlighted a persistent theory-practice gap within Australian paramedic education, revealing disparities in clinical placements and opportunities for practical skill application. 25 These findings underline the need to bridge the gap between theoretical knowledge and real-world practice. Against the backdrop of evolving educational standards and the critical importance of paediatric care, the primary aim of this study is to provide a comprehensive description of the current state of undergraduate paramedic education concerning paediatric content in Australia. The secondary research objectives include (1) assessing the extent of paediatric content integration within paramedicine entry-level degrees, and (2) uncovering the presentation and integration of paediatric content and terminology.
Methods
Research approach
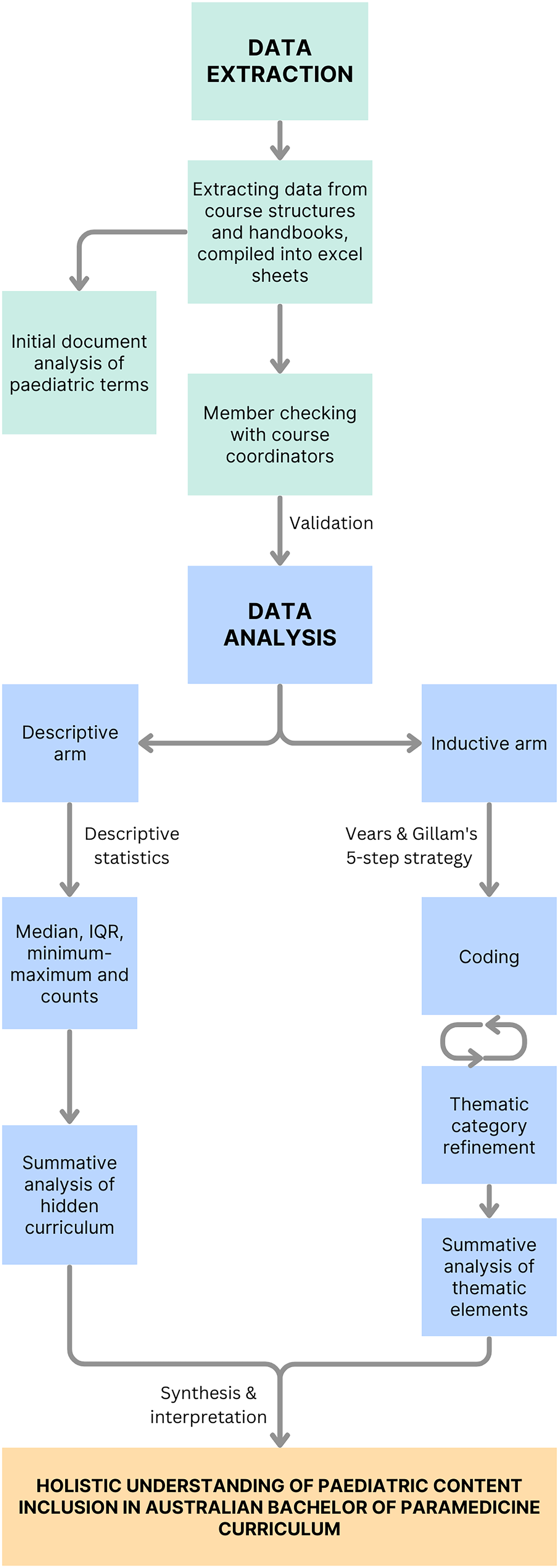
This study employs a content analysis approach, 26 to comprehensively explore paediatric content in paramedic curriculum across Australian universities. The research design incorporates two distinct arms: a descriptive arm and an inductive arm. Each arm includes a summative analysis to quantify the respective elements under investigation. The descriptive arm calculates descriptive statistics to quantify the presence and extent of paediatric content across the curriculum. The inductive arm involves a manual content analysis of learning objectives (LOs) to identify and categorise related paediatric education. The content analysis approach has been increasingly recognised in medical education research as an appropriate method to assess the inclusion of specific content areas such as women's health or ethics in curriculum.26–28 This study will utilise this approach in a similar manner to shed light on areas of paediatric education that may require enhancement.
Research paradigm
This study is guided by a pragmatist framework, acknowledging a naturalistic approach to answering the research questions by embracing both epistemological and ontological flexibility. 29 Pragmatism views knowledge as dynamic and context-dependent, focusing on practical outcomes rather than philosophical inquiries.29,30 This framework allowed for an emergent study design and guided our methodological decisions to adapt data collection and analysis methods as the data emerged, following the information to uncover actionable insights. It aligns with the goal of this research to understand and improve the extent to which paediatric content is included in paramedic curriculum across Australian universities.
The research also incorporates social justice theory, as outlined by Rawls and further adapted to the healthcare context by Daniels.31,32 Social justice theory advocates for the equitable distribution of resources, with health being recognised as one of these vital resources. 32 Social justice theory influenced the research design and methods by guiding the focus on the inclusion of paediatric content, as children are a vulnerable and often underserved population in emergency care. This perspective shaped the examination of the curriculum to ensure fairness in representing paediatric patients. The theory also influenced the interpretation of the findings, highlighting disparities in paediatric education and advocating for equitable curriculum reform.
While these frameworks support a dynamic and context-dependent approach, their practical implications may introduce flexibility that could affect the consistency and comparability of the findings. Despite the theoretical ideals inherent in these frameworks, significant limitations or challenges in balancing them with practical constraints were not encountered, nor did the framework restrict the scope of analysis or introduce biases.
Research team social position and reflection
The research team comprises one novice and three experienced academics, working in varying fields and capacities in a university setting. The first author is an Indigenous early career researcher with a paramedic background. With lived experience with paediatric chronic illness, a range of interactions with paramedics as a child and trouble identifying extensive paediatric content in their undergraduate paramedic degree, this author has both personal and professional motivations to explore this topic. Any personal biases were mitigated through regular reflexivity exercises, where the researcher critically examined their own influence on the research process. Additionally, the involvement of co-authors with diverse backgrounds helped to provide a balanced perspective.
The second author is a lecturer in dietetics, nutrition and food and is more qualitatively aligned. The third and senior authors are both paramedic educators who hold leadership roles within the institution and a wealth of experience in health research, specifically quantitative methods. Their experience and differing methodological perspectives were crucial in ensuring that the research was conducted with rigour and balance. Regular team meetings facilitated ongoing discussions about potential biases, with a focus on maintaining objectivity throughout the research process. These positionalities determined the theoretical approach as all authors are motivated to find a pragmatic answer to improve education practice.
Setting and eligibility
In Australia there are 25 accredited paramedicine courses across 18 institutions. The setting for this curriculum-focused study was all accredited Australian universities where a Bachelor of Paramedicine program is currently offered (16/25 accredited programs). 33 This review excluded programs that were accredited but no longer actively accepting admissions, post-graduate or diploma programs, as well as dual degrees involving nursing (9/25). These programs were not included because they could skew the results by introducing variables that are not present in standalone paramedicine degrees, such as different curricula, admission criteria and professional outcomes. For example, nursing accreditation in Australia mandates 800 h of clinical practicum, which provides more extensive opportunities – often in hospital settings with additional chances for interprofessional collaboration – to develop paediatric management skills compared to what is available in a standard paramedicine degree. 34
Accredited by the Paramedicine Board of Australia (under the umbrella of AHPRA), the programs included offer two to four-year degree programs in paramedicine. Education is based on accrediting board competencies, in areas such as anatomy, physiology and pharmacotherapy. The curriculum extends beyond biomedical sciences to include significant interprofessional contexts such as Indigenous health, communication in healthcare, social determinants of health, mental healthcare, clinical reasoning, decision making and risk management. 15 Students are trained to practice ethically and professionally and collaborate effectively with other health practitioners. These educational experiences are complemented by practical placements in diverse clinical and community settings, in collaboration with ambulance services. 15 Graduates become eligible for national registration upon successful completion of an accredited degree program.
Data extraction
Data were extracted from all eligible degrees, using a pre-developed template. Information was extracted across July 2023 from current publicly available course structures and course/unit handbooks into a Microsoft Excel (Version 2019) 35 spreadsheet including: basic degree information; all listed academic units; year and semester of each unit offering; each unit description, aim and learning outcomes (LOs).
Once all data was extracted for each course, the course coordinator/director/lead of each university was contacted on their publicly available email address and asked to review the document for their institution and correct any mistakes. Coordinators were then asked to provide estimates regarding:
the percentage of time dedicated specifically to paediatrics in each unit (herein referred to as unit coverage), time spent on paediatrics practicals, scenarios or tutorials (tutorials & practicals) the proportion of paediatrics-related assessments, encompassing practical assessments, exams and in-semester evaluations (assessment).
Paediatric content was defined to the course coordinators as any curriculum content that included patients aged <18 years old. This member checking was conducted in August 2023 to validate and enhance the accuracy of the collected curriculum information.
Data analysis
The initial data analysis involved a document analysis of paramedic curricula from all accredited universities in Australia. This analysis aimed to assess the similarity of curricula and validate the generalisability of the member-checked curricula subjected to further analysis. Using Excel, an overall count was conducted to determine the number of units within each curriculum that included at least one paediatric learning outcome (LO) and/or paediatric terminology in their synopses. Paediatric terminology encompassed terms such as ‘paediatric’ or ‘child’, as well as more generic terms related to paediatrics, such as ‘lifespan’ and ‘diverse age group’. Maternity terms were excluded from this count. The inclusion of member checking was deemed crucial as it provided an additional layer of validation to the extracted results, ensuring greater confidence in the subsequent analyses.
Subsequent analysis conducted on the curricula from institutions that completed member checking comprised two main components, as illustrated in Figure 1.
Research method
Descriptive arm of analysis
Descriptive statistics were calculated on numerical data utilising Jamovi (Version 2.3). 36 As all variables were nominal data presented as count data or percentages, medians and interquartile ranges (IQR) were utilised. Minimum-maximum counts and distribution density plots were also utilised to provide comprehensive results. This was first conducted across the degree, quantifying the percentage of paediatric content in total and subsequent analysis of units with paediatric content assessed: unit coverage; tutorials & practicals; and assessment.
The first summative analysis encompassed two components. First, a more detailed count of LOs were conducted to quantify the number of all LOs (some units had multiple) that included paediatric-specific or affiliated language. Second, the hidden aspects of the curriculum were examined to assess the alignment between stated LOs and the content dedicated to paediatrics within paramedic curriculum units. Here, the hidden aspects of curriculum refer to any misalignment of inclusions in formal curriculum that are not explicitly stated in LOs or indicated by course coordinators. This involved identifying units where paediatric content was indicated by course coordinators without specific paediatric LOs outlined, as well as units with paediatric LOs but without a designated percentage of content dedicated to paediatrics. Additionally, units were identified where both paediatric LOs and a percentage of content dedicated to paediatrics were indicated. Finally, units lacking both paediatric LOs and a designated percentage of content dedicated to paediatrics were noted.
Inductive arm of analysis
An inductive content analysis approach was conducted on LOs related to paediatric patients. LOs were selected for the content analysis as opposed to the unit descriptions or aims as they provided specific and measurable goals for the unit and are often used by universities to guide all content and assessment. 37 This analysis was conducted manually by two investigators, drawing insights from unit LOs to identify what is covered in paediatric learning and teaching. 27
The inductive content analysis was completed in line with Vears and Gillam's (2022) 5-step strategy. 38 The process began with a thorough reading and familiarisation with the LOs to gain an overall understanding of the content. In the first round of coding, overarching subjects were identified to capture the main concepts present, such as populations served relevant to paediatrics, including ‘Complex patients’, ‘Paediatric’ and ‘Lifespan’. Subsequently, in the second round of coding, additional codes were connected to capture latent (less obvious) meanings, such as ‘Cardiology,’ ‘Clinical skills,’ and ‘Critical reasoning’. Redundant codes were refined and consolidated in the following step to streamline the coding scheme into main categories and subcategories.
A summative content analysis was then conducted. For each subcategory element, the presence and coverage percentages of paediatric-related content were assessed across the units. To prevent data skewing, each unit contributed only once to each element, resulting in a binary output. This was essential as each unit could include multiple LOs, and recording each of these would misrepresent the distribution. Linking the frequency of category occurrences to the percentage coverage for each instance provides insight into the proportion of content dedicated to each category. Additionally, the descriptions of units lacking paediatric LOs but assigned percentages by course coordinators were analysed to identify the breadth of content covered within the curriculum beyond paediatric-focused LOs.
Furthermore, a radar chart visualisation was employed to illustrate the distribution of paediatric LOs across subcategory elements. Each LO contributed only one count to each element it fell into, adhering to the binary output described earlier. This approach allowed for a clear representation of the proportional representation of elements within the paediatric curriculum.
Trustworthiness
Two investigators conducted manual coding together, ensuring a rigorous process of intercoder reliability. All codes were agreed upon jointly, demonstrating 100% agreement between the coders. To achieve this, the team engaged in calibration exercises, which included coding a subset of data together and discussing any discrepancies in interpretations. When disagreements arose, they were resolved through consensus meetings, where each coder's perspective was considered, and the final decision was made collectively. Frequent peer coding debriefing sessions were conducted to review and refine coding decisions, further enhancing the reliability and consistency of the coding process. These sessions allowed for critical reflection on assumptions, biases and methodological decisions, ensuring transparency and rigour in the research process. Furthermore, constant reflexivity was maintained throughout the research process. Triangulation was achieved using multiple analytical approaches, including summative and inductive content analysis.
Ethical statement
The Monash University Human Research Ethics Committee was consulted regarding this project and the researchers were advised that the project was exempt from requiring ethical approval, as the information collected is not considered ‘human data’ and does not include any data related to the opinions or lived experiences from the people participating in member checking. Data consisted of publicly available information, with course structures and learning objectives sourced from university recruitment websites. To safeguard institutional intellectual property, no data was republished. Member checking was conducted with implied consent following the distribution of detailed project information. Analysis was de-identified to maintain participant confidentiality.
Results
Overall document analysis
Out of 16 accredited Bachelor of Paramedicine programs in Australia, data from 15 were analysed due to one institution lacking publicly available curriculum documents. As indicated in Table 1, the analysis identified a range of one to seven units that included at least one paediatric LO, with a median of three units (IQR: 3–5). Approximately one-third of universities had three units with paediatric LOs. Similarly, the number of synapses containing paediatric terminology ranged from one to six, with a median of three (IQR: 2.5–4). It is worth noting that many of these terms were generally related to paediatrics rather than specifically mentioning ‘paediatric’ or ‘child’. Approximately one-third of universities had three units with paediatric terminology mentioned in their synopses.
Quantifying paediatric terminology inclusion in Australian degrees.
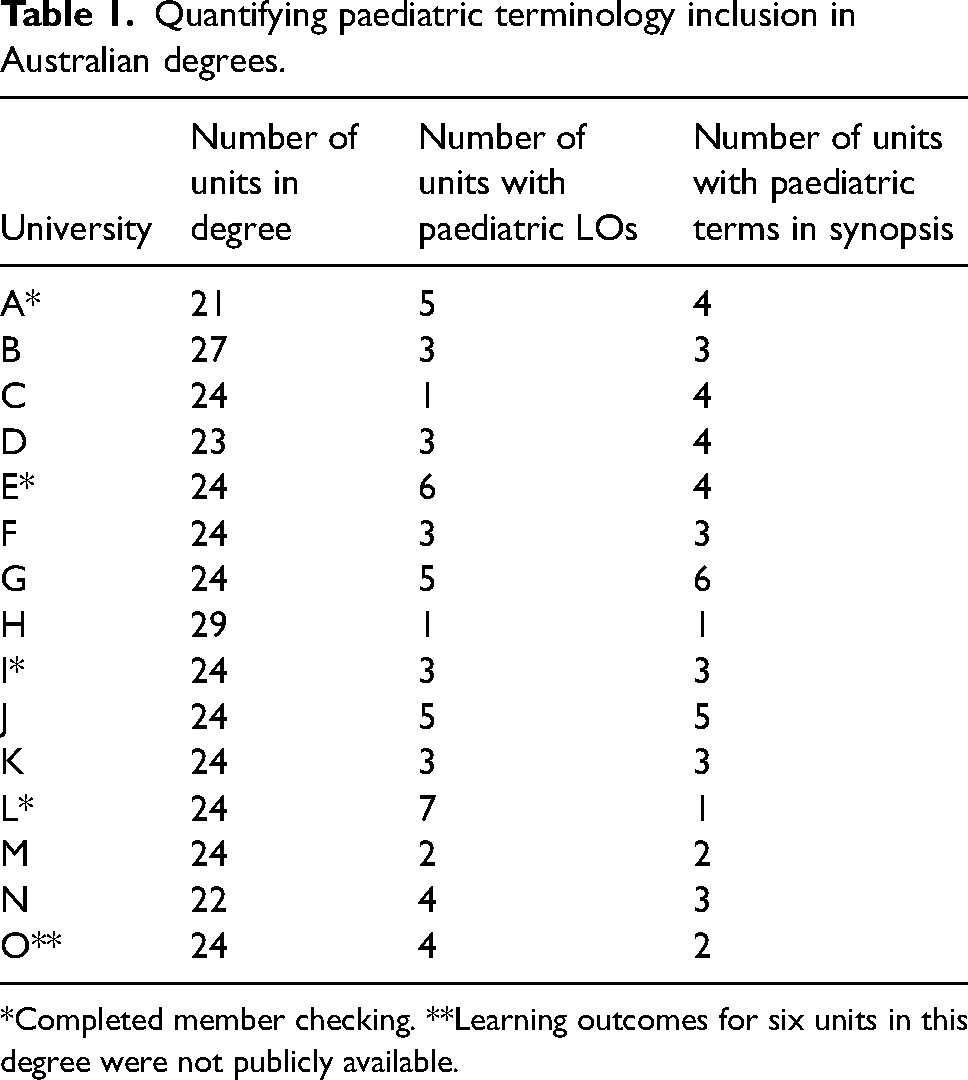
*Completed member checking. **Learning outcomes for six units in this degree were not publicly available.
Descriptive arm: Quantifying paediatric inclusion in degrees
Four institutions spanning most Australian states (Victoria, Northern Territory, South Australia, Western Australia and Queensland) completed member checking and were thus included in further analysis. All were a Bachelor in Paramedicine (or equivalent) and were three-year full-time degrees, with part-time offerings. All universities require students to hold a working with children's card or equivalent credential, a mandatory background check in Australia ensuring that individuals are safe to work with children. This requirement is relevant as it reflects the administrative consideration for child safety and indicates an inherent acknowledgement of the importance of paediatric care within the paramedic curriculum. Only one university had a specific paediatric content-only unit and paediatric-specific placement (though limited spaces were available).
All units within the four degrees (93 units combined, across four universities) were analysed, and paediatric content in all three elements (unit coverage, tutorial & practicals and assessment) equated to a 0% median. Figure 2 visually represents the national distribution (all four institutions combined). However, individual university median scores of unit coverage ranged from 0% to 2.5% most ranging from zero to approximately 50% with one university ranging 0–100% as one unit was paediatric content only. Individual university tutorial and practicals inclusion ranged from 0% to 4% medians while all institution assessments had a median of 0% (Supplementary Material 1). A map of paediatric content inclusion is included in Figure 3.
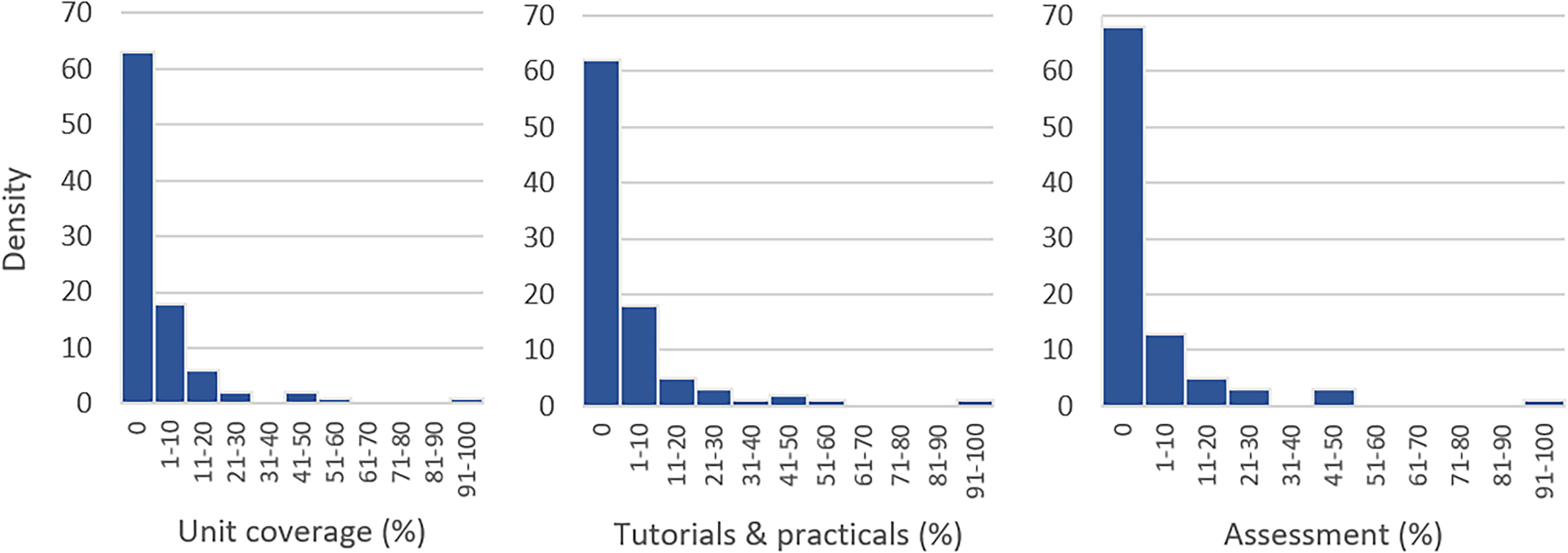
Density of overall degree distribution (combined institutions).
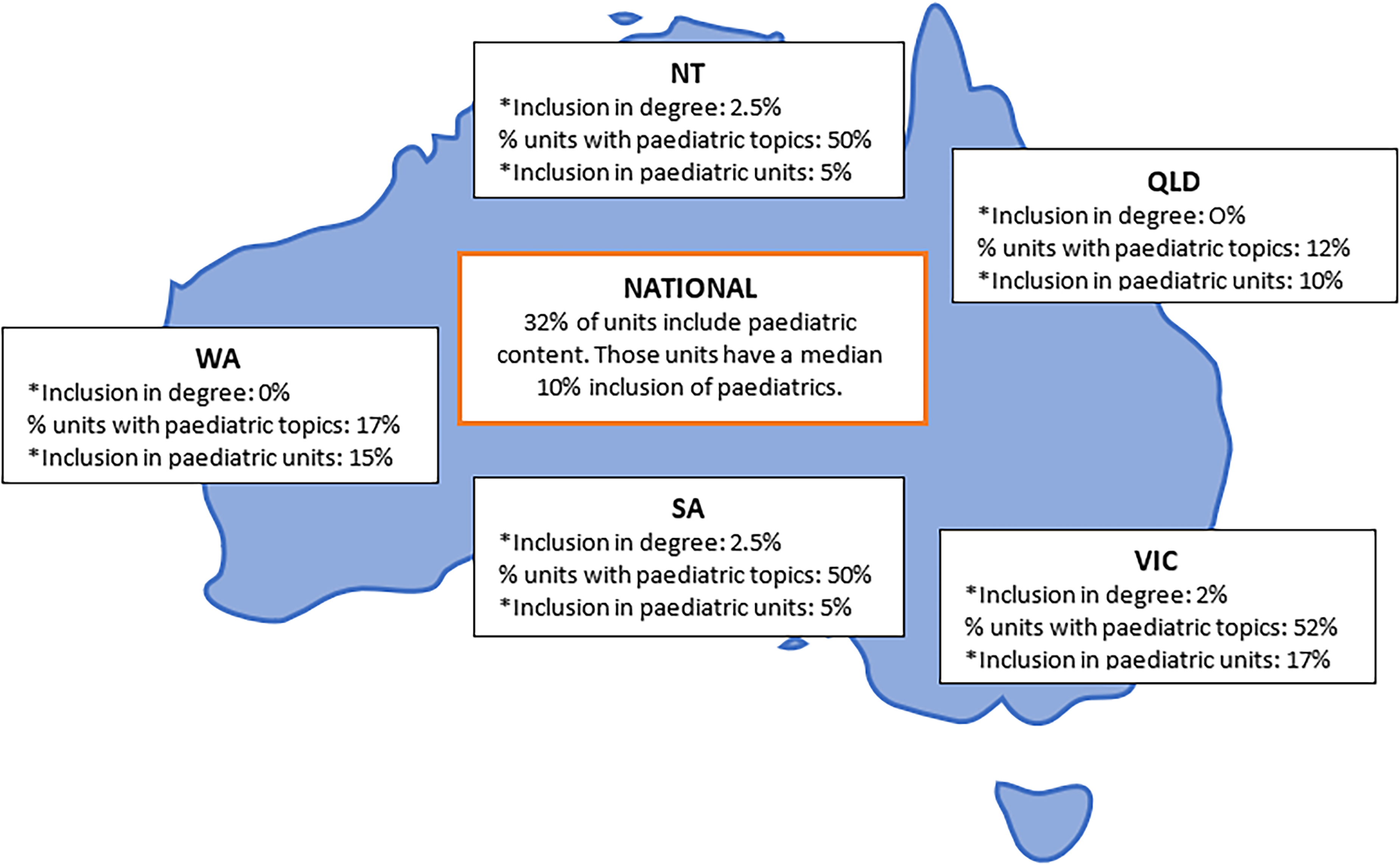
National mapping of combined curriculum paediatric inclusion. *median statistic. NT, Northern Territory; QLD, Queensland; VIC, Victoria; SA, South Australia; WA, Western Australia.
Thirty of the 93 units (32%) analysed had the inclusion of paediatrics as identified by course coordinators. The median paediatric unit content coverage of these 30 units was 10%. The combined total increased over time after each year of study as seen in Supplementary Material 1.
Learning outcomes
Each institution has five-to-eleven-degree learning outcomes, none of which mentioned paediatrics or any affiliation (i.e., special populations, diverse age groups). Across all four institutions, 481 unit LOs were assessed (129, 135, 94 and 123, respectively), and 39 were found to relate to paediatrics (10, 9, 9 and 11, respectively). This means 8% of national LOs relate to paediatrics in some way, by name or affiliation (special populations, diverse age range). Eighteen LOs (3.7%) used paediatric-specific terminology i.e., ‘paediatric, child, newborn’.
Hidden aspects of the curriculum
Analysis of the hidden aspects of the curriculum revealed several findings regarding the alignment between LOs and the percentage of content identified by member checking to be dedicated to paediatrics. The search identified 17 units where member checking indicated that paediatric content was present (ranging from 2% to 30%), yet no specific paediatric LOs were outlined. Among these units, one notably allocated 30% of its content to injury prevention across the lifespan in its description but lacked corresponding LOs. Similarly, other units mentioned topics like childbirth and paediatric neuro-emergencies in their descriptions but did not include them in the LOs. Conversely, eight units were found to have paediatric LOs without a dedicated percentage of content identified as paediatrics by the member checking process. These units typically covered diverse age groups without specifying paediatric LOs explicitly.
The analysis identified 13 units where both paediatric LOs and a percentage of content dedicated to paediatrics were present, with percentages ranging from 5% to 100%. Finally, a substantial number of units (55) had neither paediatric LOs, nor a designated percentage of content dedicated to paediatrics. These findings underscore the importance of ensuring strategic alignment between stated LOs and the content covered, particularly in the context of paediatric education, to optimise LOs and curriculum effectiveness.
Inductive arm: Exploring meaning in learning outcomes
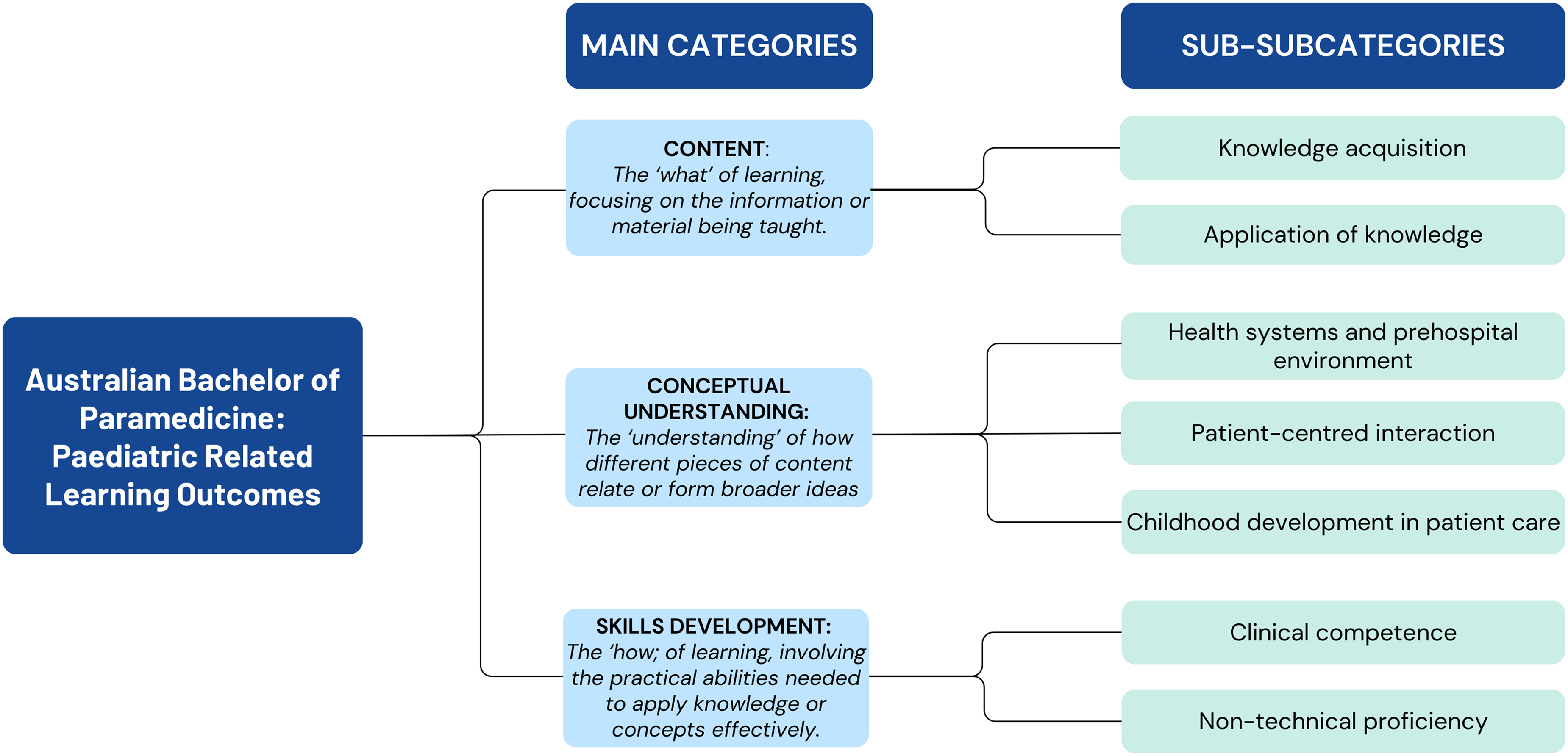
The analysis of the 39 paediatric-related LOs identified three main categories: Content, Conceptual Understanding and Skills Development as displayed in Figure 4. The content category encompasses LOs that serve as the “what” of learning, providing the foundation of knowledge, while concepts facilitate the understanding of relationships and connections between different pieces of content. Skills, on the other hand, represent the “how” of learning, involving practical abilities needed to apply knowledge and concepts effectively in clinical practice.
Category flow chart.
Content
Content encompasses the subject matter and information presented in the curriculum. Within this category, analysis revealed two key subcategories: Knowledge Acquisition and Application of Knowledge. These subcategories delve into specific topics such as childhood development, disease progression, acute and chronic conditions, trauma and pharmacological interventions, underscoring the breadth of content covered in the curriculum.
Conceptual understanding
Furthermore, analysis identified conceptual understanding as a fundamental component of the curriculum, focusing on the broader understanding of healthcare systems, patient-centred interactions and developmental concepts in patient care. These LOs involved understanding care modalities, considering social and cultural factors, developing effective communication strategies and applying developmental concepts to enhance paediatric patient care.
Skills development
Moving beyond content, skills development was also identified as a key aspect of the paediatric curriculum. This category encompasses the practical abilities and competencies necessary for effective paediatric care. Subcategories within skills development include clinical competence and non-technical proficiency, which encompass topics ranging from advanced life support techniques to effective communication and evidence-based practice (See supplementary material 2 for mapped out code scheme).
Summative analysis of subcategory elements
Within the elements of the category ‘Content’, knowledge acquisition was identified in seven of the 21 units with paediatric LOs, with coverage percentages ranging from 0% to 50% across these units. Similarly, the application of knowledge subcategory was noted in four units, with coverage ranging from 0% to 17%. Moving to the elements of the ‘Conceptual understanding’ category, health systems-related content was identified in three units, with coverage percentages varying between 17% and 54%. Patient-centred interaction was present in five units, with coverage percentages ranging from 5% to 54%. Childhood development concepts appear in a smaller proportion of units, with only one unit having a 5% coverage and two units that were not identified to have a percentage. Within the elements of ‘Skills development’, clinical competence is prominent, being identified in 10 of 21 units with paediatric LOs. Likewise, the non-technical proficiency subcategory was identified in 13 units, both with varying coverage percentages from 0–100%.
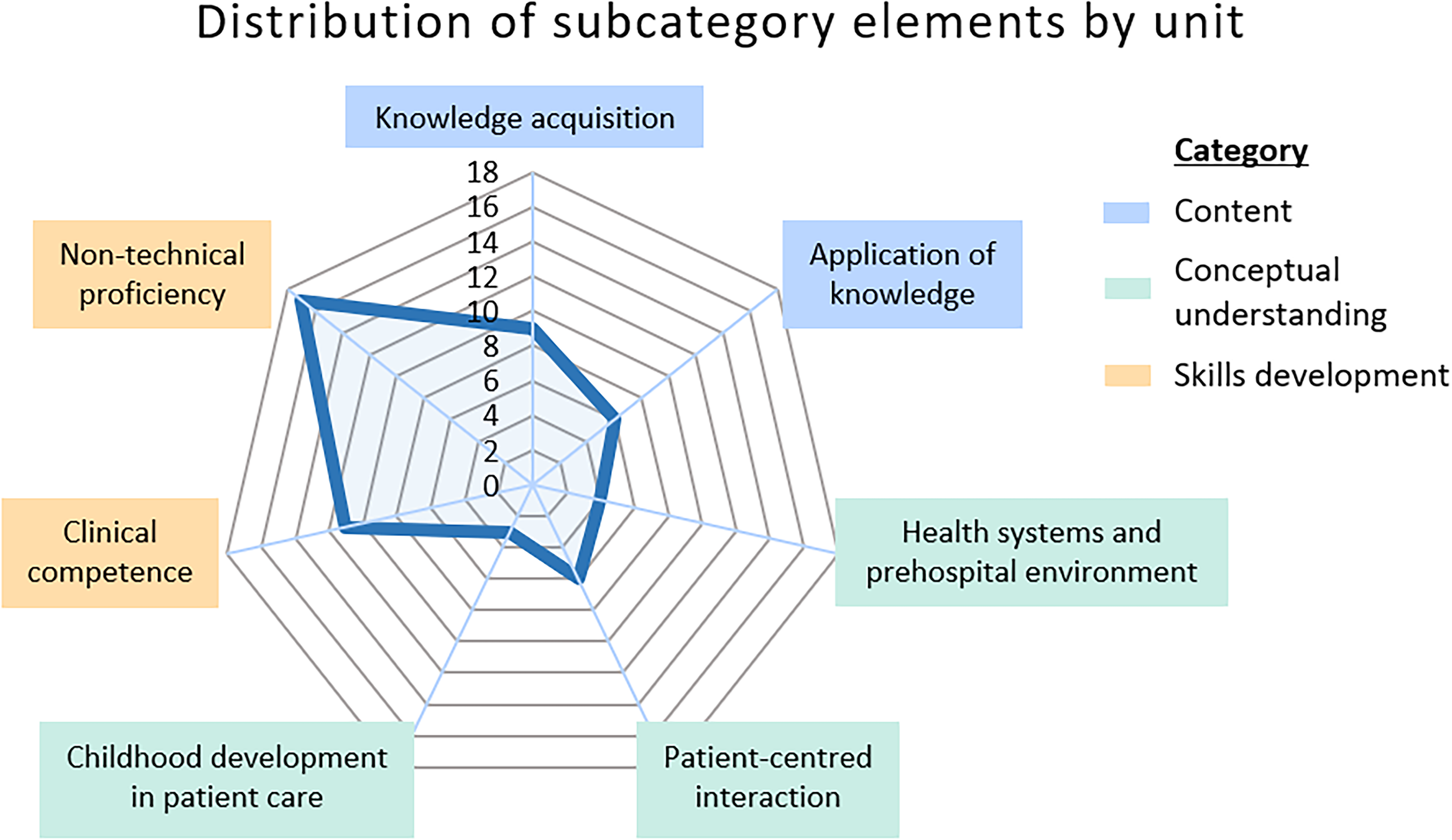
The radar chart (Figure 5) illustrates the distribution of paediatric LOs across elements, with each unit contributing only one count to each element it fell into. Non-technical proficiency was prominent with the highest count of 17, while childhood development in patient care represents the lowest with three counts.
Quantifying LO exposure density to subcategory elements.
Units lacking paediatric LOs but assigned percentages by course coordinators cover a wide array of topics, including anatomical structures/physiology of the human body, pharmacology, neurological emergencies and mental health.
Discussion
The purpose of this study was to examine the current inclusion of paediatric content in undergraduate paramedic education across Australia, a topic that has not been extensively explored in existing literature. To the best of available knowledge, this is the first study of its kind, employing a novel approach to assess paediatric inclusion across multiple Australian states with similar program designs, aiming to achieve information power and generalise findings to the broader Australian curriculum landscape.
Coverage of paediatric content
To address the first research objective measuring the extent of paediatric content integration within paramedicine entry-level degrees the curriculum of fifteen institutions was assessed, revealing a median of three units which included paediatric LOs or terminology in unit synopses. Four institutions were analysed further after member checking. The analysis revealed a concerning lack of paediatric content integration within paramedic education curricula. Out of 93 units analysed nationally, only 30 were identified by course coordinators to include paediatric content, with just 21 units having specific paediatric LOs. Across the units, 481 LOs were evaluated with 39 related to paediatrics, and only 18 using specific paediatric terminology. The median national inclusion of paediatrics in paramedicine units was 0%, highlighting the need for urgent curriculum reform.
The limited inclusion of paediatric content and its infrequent explicit mention in LOs could be attributed to several causes. These include, among others, the history of the profession being predominantly male and ALS-focused during wartime, 39 a general medical apprehension toward treating children,17,19–21 and the recent evolution of paramedicine in Australia. 7 With not yet six years since the transition from CAA to AHPRA registration in the country, institutions are still adapting. Current registration requirements do not explicitly mandate the inclusion of specific populations, such as paediatrics, in LOs. 15 The current lack of specific LOs for paediatrics may persist until registration requirements explicitly include specific populations.
Accompanying the limited exposure to paediatric education, paramedics are also not often exposed to paediatric practicum in clinical environments. 16 These factors impounded by the general health disparities of this population present a complex issue. Children present unique challenges in emergency medical care due to several factors, including faster deterioration, smaller bodies with higher physiological instability, and communication challenges, all of which can complicate treatment. 40 Provider stress and anxiety levels tend to rise during interactions with paediatric patients, increasing the risk of safety incidents, often stemming from insufficient exposure to paediatric cases. 41 Moreover, issues such as undertreatment of pain in paediatric pre-hospital care, 42 and lower survival rates in paediatric out-of-hospital cardiac arrests emphasise existing disparities in paediatric management. 43
Considering these discrepancies in paediatric care is crucial within the context of a curriculum that prioritises health equity. Paediatric patients represent a minority group; nevertheless, comparing the curriculum's content percentage to the actual prevalence of cases or population assumes uniform needs from the outset, which does not reflect reality. This awareness underscores the necessity to shift to an equitable approach. Current literature in medical training suggests reframing education from a systematic to a health equity approach, guiding curriculum with social determinants of health.23,44 A health equity approach would prioritise content for populations with health disparities including paediatrics.
Despite observing a subtle increase in paediatric inclusion over the three years of the degree, this study highlights a potential flaw in the timing of paediatric education within paramedic curricula. If paediatrics are relegated to the latter stages of the degree, students may not possess adequate paediatric knowledge until their final year, potentially compromising their ability to practice providing optimal care during clinical placements. Scaffolding of curricula is a concept mentioned in paramedic literature, it involves structuring learning experiences in a way that supports students’ progression from simpler concepts to more complex ones, providing the necessary support and guidance along the way. 2 In the context of paramedic education, scaffolding paediatric content into the curriculum means integrating paediatric topics and skills throughout the educational program in a systematic manner. Rather than presenting paediatric material as isolated modules or units, it would be woven into the broader curriculum, aligning with the overarching themes or systems-based approach used in paramedic training. By integrating paediatric topics throughout the curriculum, students can better grasp the interconnectedness of different aspects of paramedic practice and develop a more holistic understanding of patient care. It is not intended to displace but complement current non-paediatric content.
To that end, Bell et al. (2021) contend that Australian paramedic programs have traditionally segregated the supporting sciences like biology, anatomy, pharmacology and physiology into distinct areas of study. 2 This approach may create a gap between theoretical knowledge and its practical application in paramedic practice, especially within the industry, referring to it as ‘the theory-practice gap’. 2 As a result, there is growing consideration that transitioning from a partitioned, systems-based approach to a more integrated, scaffolding-based curriculum design might better bridge this gap and enhance the relevance of education to real-world paramedic practice.
Hidden aspects of the curriculum
The concept of hidden curriculum, which encompasses the implicit messages and lessons conveyed beyond the explicit curriculum, has long been discussed in health education. It includes unwritten norms, values and behaviours that students absorb during their training, often shaping their professional identities and practices. 45 This paper has shown in addition to what may be defined as the hidden curriculum, there are also hidden aspects to the curriculum where misalignment between course coordinators’ perception of content and explicit LOs exists.
Literature suggests potential benefits of hidden curriculum, such as experiential learning through observation and emulation. 45 Studies demonstrate it can also foster positive outcomes, such as the internalisation of robust medical ethics as a professional value and the fostering of professional identity formation if the complexities of clinical practice are made explicit.46,47
However, there are concerns about relying on the hidden curriculum. Brown et al. (2020) highlighted those disparities in experiences within the hidden curriculum create assessment complexities. Students reported feeling that covert institutional agendas undermined their professional identity, pushing them away from the intended professional standards. 48 The predominant reliance on this implicit form of instruction for paediatric education raises concerns regarding standardisation and consistency across educational settings.45–47
The reliance on the hidden curriculum for paediatric teaching – where 20 out of 33 identified paediatric-inclusive units potentially embed such content – raises concerns about consistency and standardisation. The hidden curriculum may inadvertently perpetuate negative attitudes or hesitancy towards paediatric cases among students, particularly if educators and role models express apprehension or discomfort in dealing with such cases.45,48 As practising paramedics often share apprehensions about paediatric cases, the hidden curriculum may reinforce these sentiments, further hindering students’ confidence and competence in paediatric care. Without clear guidance and standardised exposure to paediatric content, students may lack the necessary preparation and confidence to navigate paediatric cases competently.
To address these challenges, a scaffolded approach to paediatric education, as recommended earlier in this discussion, could provide a structured framework for gradually introducing and reinforcing paediatric concepts and skills throughout the curriculum. By incorporating paediatric-specific LOs and experiences at various stages of the program, educators can ensure that students receive comprehensive and standardised exposure to paediatric content, thereby mitigating the influence of the hidden curriculum and fostering confidence and competence in paediatric care among paramedic students.
Content areas and concepts addressed in paediatric learning outcomes
Regarding the secondary research objective to uncover the presentation and integration of paediatric content and terminology, the predominant content areas and concepts addressed in paediatric learning outcomes within paramedic education programs were explored. Learning outcomes serve as foundational pillars within a curriculum, guiding both assessment and content delivery. 37 While a unit may contain content that is not explicitly outlined in the LOs, the specificity of paediatric-focused LOs is crucial for accountability in teaching resources, assessment practices and content coverage. Analysis of LOs revealed three overarching categories: content, conceptual understanding and skills development. This division aligns with expectations for a health degree program, which historically prioritises the attainment of competencies. 49 The identification of these overarching categories signifies alignment with key aspects typically found in health curriculum, suggesting that a complete restructuring may not be necessary. While these findings indicate that the essential components are present, there may be room for refinement in the distribution of these elements to ensure a more balanced curriculum. It is also prudent to note when analysing these elements of curriculum that not all LOs will be weighted the same in curriculum.
Distribution of subcategory elements
This analysis aimed to assess the alignment between paediatric content coverage and the categorisation of paediatric learning outcomes. A notable portion (17 out of 56) of the content aligned with the non-technical skills subcategory, including communication, application of knowledge and evidence, reflective practice skills, and critical thinking or reasoning. The evolution of paramedic education towards emphasising non-technical skills has been crucial in transitioning from a purely technical-based approach to an independent healthcare profession. However, it prompts the question: has this evolution adequately addressed the non-technical skills essential for paediatric care? A recent study identified decision-making, communication, empathy, leadership and ethics as key non-technical skills in the literature required of paramedics. 50 Additionally, a recent Delphi study gained consensus that ‘communication, problem-solving, situational awareness, professionalism, and interpersonal skills’ are vital to the role of paramedic. 51 Adapting some of these skills specifically for paediatric contexts may be necessary.
Clinical competencies, comprising 11 out of 56 counts in the radar chart, may have been overshadowed by the historical emphasis on technical skills in paramedic education, potentially neglecting paediatric training. While competency-based models excel in producing ‘road-ready’ paramedics, 2 they may inadvertently overlook the comprehensive preparation needed for handling paediatric cases. Importantly, while clinical skills codes acknowledge learning in overall assessment, there's no specific mention of pain assessment, a priority in literature.42,52 However, it is unclear how the skill of adapting pain assessment for paediatrics is included in the curriculum content, as it is not mentioned in any LOs.
Furthermore, the distribution of elements revealed lower counts for applying childhood development concepts to patient care, knowledge acquisition and application of knowledge (3, 9 and 6 out of 56, respectively). This discrepancy underscores the need for further attention to be directed towards these areas within paediatric education. For instance, mental health issues are a leading cause of mortality among teenagers, 43 yet only four LOs of 481 discussed psychosocial development, psychological factors or mental health impacts of paediatrics. This observation underscores the importance of enhancing the curriculum to better address the multifaceted needs of paediatric patients, particularly in areas such as mental health awareness and support.
While this paper provides valuable insights into the distribution of content within publicly available LOs, it is essential to acknowledge that curriculum content may extend beyond what is explicitly described in these documents. Nonetheless, the inclusion of critical concepts and skills within LOs remains imperative as they serve as a framework for educators to deliver comprehensive instruction and assessment. Moving forward, future research endeavours could explore the optimal distribution of elements within the curriculum through collaborative efforts involving educators, stakeholders and interprofessional healthcare advisors. Engaging in dialogue and consultation with these key stakeholders ensures that paediatric education is effectively structured to meet the diverse needs of learners and ultimately improve patient outcomes. Additionally, considering the influence of the hidden aspects of curriculum, which encompasses the implicit messages conveyed through educational experiences, warrants further exploration to ensure alignment between intended and actual LOs.
Recommendations
This study suggests adopting a health equity approach to curriculum design and recommends scaffolding paediatric content throughout the entirety of the paramedic degree program. Future research collaborations with educators and stakeholders should aim to assess how elements of the paediatric curriculum should be distributed across the degree. Integrating enhanced paediatric content aligns with the broader educational goals of producing safe, competent paramedics who meet high professional standards.7,10 By strengthening paediatric education, we support the development of essential competencies required by accreditation bodies, ensuring practitioners are well-prepared to deliver quality care across all patient populations.
Future research should consider mapping LOs against predetermined paramedic capabilities as set by the professional body or piloting specific paediatric capabilities to ensure alignment with graduate competencies. Collaboration between stakeholders, including course coordinators, paediatric specialists, health curriculum innovators and psychiatrists, could enrich curriculum development and ensure comprehensive coverage of paediatric content. This has successfully been implemented by other healthcare professions. 53 Implementing interprofessional learning approaches, which have been shown to enhance paediatric interprofessional competencies, could be beneficial for paramedic education. 54 Exploring novel approaches to include paediatric content in the curriculum, such as medical play in mock paediatric wards or placements in special needs schools, may offer opportunities to develop non-technical skills essential for paediatric care.55,56 In light of these findings, several recommendations are proposed for future research and curriculum development. The next step is to assess the feasibility and potential impact of these recommendations, aiding stakeholders in strategic planning and intervention prioritisation to enhance paediatric education.
Limitations
While this study utilised a combination of quantitative and qualitative data analysis methods to comprehensively explore the inclusion of paediatric content in paramedic curricula, it is not without limitations. The study acknowledges that the examination of publicly available LOs may not fully capture all aspects of course content, particularly those conveyed through the hidden curriculum. Additionally, there is a degree of assumption that LOs represent the entirety of course content, which may not always be the case.
Member checking was conducted to validate and enhance the accuracy of the collected curriculum information, it introduced a level of subjectivity. The responses from course coordinators may have been influenced by individual perceptions or interpretations of the curriculum, potentially introducing response bias into the data. Despite efforts to ensure accuracy through member checking, there is a possibility of data inaccuracies or omissions in the extracted curriculum information, which could impact the validity and reliability of the findings.
A limitation of this study is that the further analysis was based on responses from only four of the sixteen institutions due to the response rate from member checking. This could introduce bias as the curricula of non-responding institutions were not included, potentially affecting generalisability. The exclusion of certain states, such as New South Wales or Tasmania, may limit the national representation. While more responses would have strengthened the findings, this participant group is inherently constrained by time limitations which was anticipated to affect their ability to fully engage in the study. The initial analysis showed a high degree of similarity among all sixteen curricula regarding paediatric terminology inclusion. Therefore, the findings from the four universities across five Australian states are still considered quite generalisable.
The analysis focused primarily on the prevalence of paediatric-focused units, learning modalities and assessment strategies. Other important aspects of paediatric education, such as teaching methodologies, faculty qualifications and clinical placement experiences, were not comprehensively explored. Future research could address these limitations by employing a more comprehensive data collection approach, involving multiple sources of information and a larger sample size of participating universities.
Conclusion
This study found a substantial lack of integration of paediatric content within paramedicine curricula, evidenced by a combined median inclusion of 0% in degrees and the identification of only a third of units containing any paediatric content. Concerns regarding the hidden aspects of curriculum's influence on standardisation and consistency of paediatric exposure among students have been raised, alongside discernible categorisation of content presentation and integration. Particularly notable is the emphasis on non-technical skills, potentially overshadowing core paediatric knowledge essential for effective care. The limited structured education measures related to paediatric content may have implications for assessment and subsequent competency. This study's limitations include potential biases from reliance on publicly available learning outcomes and member checking. Additionally, the limited response rate from institutions and the exclusion of certain states may affect the generalisability and national representation of the findings. Other aspects of paediatric education like teaching methodologies and clinical placements were not comprehensively explored.
Addressing these deficiencies is imperative for ensuring the delivery of high-quality care to paediatric patients. By implementing the recommendations outlined in this study, paramedic education programs can better equip students to meet the diverse healthcare needs of the communities they serve. Further investigation is needed to develop innovative strategies for integrating paediatric content and to evaluate their effectiveness in improving paediatric care competencies among paramedic students.
Supplemental Material
sj-png-1-pam-10.1177_27536386241286346 - Supplemental material for Mapping the future: A scoping analysis of paediatric content in Australian paramedic curriculum
Supplemental material, sj-png-1-pam-10.1177_27536386241286346 for Mapping the future: A scoping analysis of paediatric content in Australian paramedic curriculum by Rachel Peasey, Linda Ross, Julia McCartan and Kelly-Ann Bowles in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386241286346 - Supplemental material for Mapping the future: A scoping analysis of paediatric content in Australian paramedic curriculum
Supplemental material, sj-docx-2-pam-10.1177_27536386241286346 for Mapping the future: A scoping analysis of paediatric content in Australian paramedic curriculum by Rachel Peasey, Linda Ross, Julia McCartan and Kelly-Ann Bowles in Paramedicine
Footnotes
Acknowledgements
During the preparation of this work, the authors used ChatGPT to refine the language and structure of the manuscript, ensuring grammatical correctness and clarity of expression. ChatGPT was employed solely for linguistic revision and did not contribute to data extraction, analysis, or referencing. All content generated by ChatGPT was reviewed for accuracy and validity by the authors, who take full responsibility for the publication's content.
Author contribution
All authors contributed to the study and manuscript in a manner that meets the requirements of authorship.
Declaration of conflicting interests
Authors KB and LR are associate editors of Paramedicine. The authors declared no other potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.