
Abstract
Introduction
Medical clinicians treating relatives is ethically complex; in paramedicine, the time-critical nature of pathologies often precludes alternative treatment without risking morbidity or mortality.
Aims
This project had three aims: firstly, to retrieve baseline data for thematic analysis on the experiences of paramedics who have attended their own families; secondly, to generate explanatory grounded theory; and finally, to translate these findings into recommendations for practice.
Methods
Glaserian grounded theory and thematic analysis methods were both undertaken using a realist perspective. Acquiescence, wording, and habituation heuristics were mitigated in the interview design. There were 44 responses (n = 93 instances of treating family), with 21 participants (n = 34) from three countries interviewed. Saturation was determined using both Guest et al.'s and Thorne's criterion. Semantic and latent themes were generated inductively via a five-step process, with grounded theory generated simultaneously via a three-step Glaserian process. Cohen's kappa ranged from 0.82 to 0.93.
Results
Incidents were both traumatic (hangings, stabbings, traumatic arrests) and medical (paediatric arrests, cardiac arrests, overdoses). The core concept-category was ‘conflict between the roles of clinician and relative’. Paramedics reported a sympathetic hyperarousal response that they quickly suppressed, a rapid transition into ‘work mode’, and difficulty obtaining their normal state of flow, balancing dual roles as clinician and relative, transitioning out of work mode and into becoming a carer, and simultaneously processing the event. Organisational responses were frequently described as inadequate. Paramedics reported short-term experiences consistent with an acute stress response, and a large proportion suffered long-term, life-altering consequences. It is theorised that this phenomenon disrupts professional detachment, increases outcome self-expectations, interrupts normal routines, and promotes overmedicalisation.
Conclusion
This research provides baseline data and theory on the experiences of paramedics attending their own families. Five themes and 24 subthemes were identified, an explanatory theorem proposed, and a preliminary set of eight recommendations for translation into practice provided.
Introduction
It is widely accepted as ethically advisable that healthcare practitioners do not treat their own family members, to avoid any impact on their professional objectivity, patient autonomy, and informed consent.1–6 This topic has been widely explored in research across other fields of medical practice in the past decades, largely from a theoretical perspective without field work.3,4,7–24 Existing literature includes 13 commentary or review articles focussed on physicians,4,7,9,11,12,14,15,17–21,24 two case studies of surgeons treating their own family members,3,13 three surveys of physicians about treating their own family members,10,16,22 and two sets of thematic interviews of physicians who have treated family members.8,23 No research currently exists exploring the experiences of paramedics attending their own families.
This is particularly problematic as while in other areas of healthcare it is often feasible to organise other practitioners to care for relative patients, this is regularly not practical in paramedicine – the time-critical nature of the disease or injury and limited number of available practitioners often precludes seeking alternative treatment without risking significant patient harm. This scenario may leave paramedics in the situation of balancing ethical requirements against the necessity of immediate treatment, providing objective care to a family member who is critical, and risking personal psychological harm from the experience. This project has three aims: firstly, to retrieve baseline data for thematic analysis on the experiences of paramedics who have attended their own families; secondly, to generate explanatory grounded theory; and finally, to translate these findings into recommendations for practice.
Methods
Design
A realist approach was adopted; the research assumes there is an objective reality able to be uncovered from the data.25,26 As no preexisting literature on paramedics attending their own family members exists to inform study design a grounded theory methodology was selected, and the research is therefore hypothesis-generating rather than testing.26–30 The broader literature discussed above was reviewed fully post hoc, as per Glaserian methods. 31 Two methods were selected: inductive thematic analysis for data description, and Glaserian grounded theory to generate explanatory theorem.27–30,32–36 The Standards for Reporting Qualitative Research reporting guidelines were followed. 37
Confirmability and reflexivity were also considered closely as one of the authors of this study (SW) has attended their own family three times in the course of their employment. This experience was the impetus for the initiation of this research; it has been acknowledged that novel research concepts may be generated by – or potentially even require – a researcher to have been affected by the phenomenon of research. 38 Many qualitative schools of thought consider being immersed in the topic a strength, while others do not.39,40 Reflexivity – the reflection on one's own standpoint, acknowledgement of how this may affect findings, and attempts to mitigate impact on impartiality – is the primary method in qualitative research to manage this. 39
In this instance, SW stated concern that they may ‘write their experience’ rather than ‘write the data’. Given the extraordinarily intensity of both the topic being explored and the experiences of that individual, it was considered that standard reflexivity may be insufficient to mitigate this risk. Therefore, to manage this risk – and to ensure that the trustworthiness of the research would not be undermined – the research team took the unusual step of SW voluntarily not being involved in the production of interviews, not being a participant in the research, and not being involved with data analysis, which was performed independently by two researchers from different institutions (MWS and MK). MWS and MK both live and work in large urban populations in Australia, and neither have attended their families clinically. Although highly unusual in qualitative research and likely to receive criticism, this was enacted to manage what was viewed as a major risk to rigor.39,41
Reflexivity was further engaged with by a priori reflection by all researchers, all of who have attended numerous high acuity and fatality incidents in their careers. Their experiences of these – including awareness that this may lead to changes in personality and worldview – was the starting point for designing the research. The team assumed that attending one's own family would be broadly similar to attending another high acuity incident, but with increased stress, and this formed the basis for the initial 11 interview questions (Appendix I). The research team explicitly discussed avoiding any further presumptions, and this was incorporated by structuring interview questions in a nonleading manner (discussed below under Interview procedures), incorporating theoretical sampling by asking specific questions on emerging themes to later interviewees (discussed below under Data analysis), and conducting independent initial coding before coming together.
Eligibility
Participants were eligible to participate in the study if they had worked as a paramedic and, during the course of their employment, attended or were dispatched to their own family. Friends and acquaintances were excluded due to potential difficulty in characterising the strength of the relationship, which was considered to be a potential confounding factor. Family was defined broadly, with separate analysis performed to determine if there was any difference between immediate and extended family. Separate analysis was also conducted to determine any difference across countries. Cases that the paramedic was dispatched to but did not attend were included, with interview questions 5 and 6 omitted (Appendix I). Cases attended while on call were eligible; this included cases in the paramedic's own home that they self-dispatched to, provided that the case was formally recorded.
Recruitment
Participants were recruited by three methods: firstly, by open advertisement in the Australasian College of Paramedicine website and email newsletter; secondly, by email from participating jurisdictional emergency medical services to their staff; and finally, via snowballing (where participants may suggest prospective additional participants). Prospective participants were invited to submit an expression of interest via a Qualtrics XM (Qualtrics, 2022) form. All interviews were voluntary and not remunerated.
From this, 44 responses were received. Results were screened manually for eligibility by one researcher (MWS), and participants contacted for clarification of eligibility in three instances: twice for respondents who worked as first responders rather than paramedics, and once for a respondent who attended other paramedics who were not family. All three were excluded. All of the remaining 41 responses were invited to participate, with 14 participants interviewed before saturation was reached and an additional seven conducted as they were already scheduled for a total of 21.
Estimated sample size
Due to ongoing methodological debate on the concept of saturation (the point at which further data collection is redundant), the research team adopted an explicit (although still subjective) criteria to determining when information redundancy had been reached.42–47 This criterion was based on the method of Guest, Namey, and Chen (using a base size of five and run length of three), with modifications to allow for the criteria espoused by Thorne.42,48,49 Adopting both methods allows for decisions on when to cease data collection to be well-informed by both a multicriteria subjective research opinion, and by objective measure on the number of new themes being generated. Each of these methods will be briefly described.
Guest, Namey, and Chen provide a validated method for determining saturation based on when novel data stop emerging during interviews. In this method, the number of unique themes across an initial baseline set of interviews (the ‘base size’) is determined and compared to the number of new themes across a predetermined series of subsequent interviews (the ‘run length’, denoted using superscript). Once the percentage of new data in the run compared to the base falls below a predetermined threshold (the ‘new information threshold’), saturation is determined to have been met. In this instance the standard base size of 5, run length of +3, and new information threshold of <5% were used. To increase sensitivity, a more conservative new information threshold of 0% and a run length of +5 were also calculated.
Thorne instead argues that the concept of saturation is fundamentally flawed and often claimed by researchers with insufficient basis, and that the more important criteria for readers to consider when assessing the findings presented in a study is if there is suitable depth, richness, detail, and coherence across the data. Depth was here interpreted as the data delving thoroughly into all aspects of the research topic rather than being superficial; richness as the data being sufficient granular to capture subtleties; detail as the data covering all aspects of the topic rather than just some; and coherence as the data having sufficient consistency to present a logical narrative without outstanding ‘loose ends’. Due to their subjectivity, the research team approached these criteria cautiously and as a team.
Combining these two methods, recruitment ceased when two conditions were met: (a) the research team agreed in midcoding discussions that there was suitable depth, richness, detail, and coherence in data to ensure credibility, and (b) a saturation ratio of <5% (with the 0% +3 and +5 saturation ratios also calculated).42–45,48,50 This was anticipated to require 10 to 30 interviewees. Saturation assessment is summarised in Table 1.
Saturation assessment using both Guest et al. and Thorne methods (italics indicates base size).
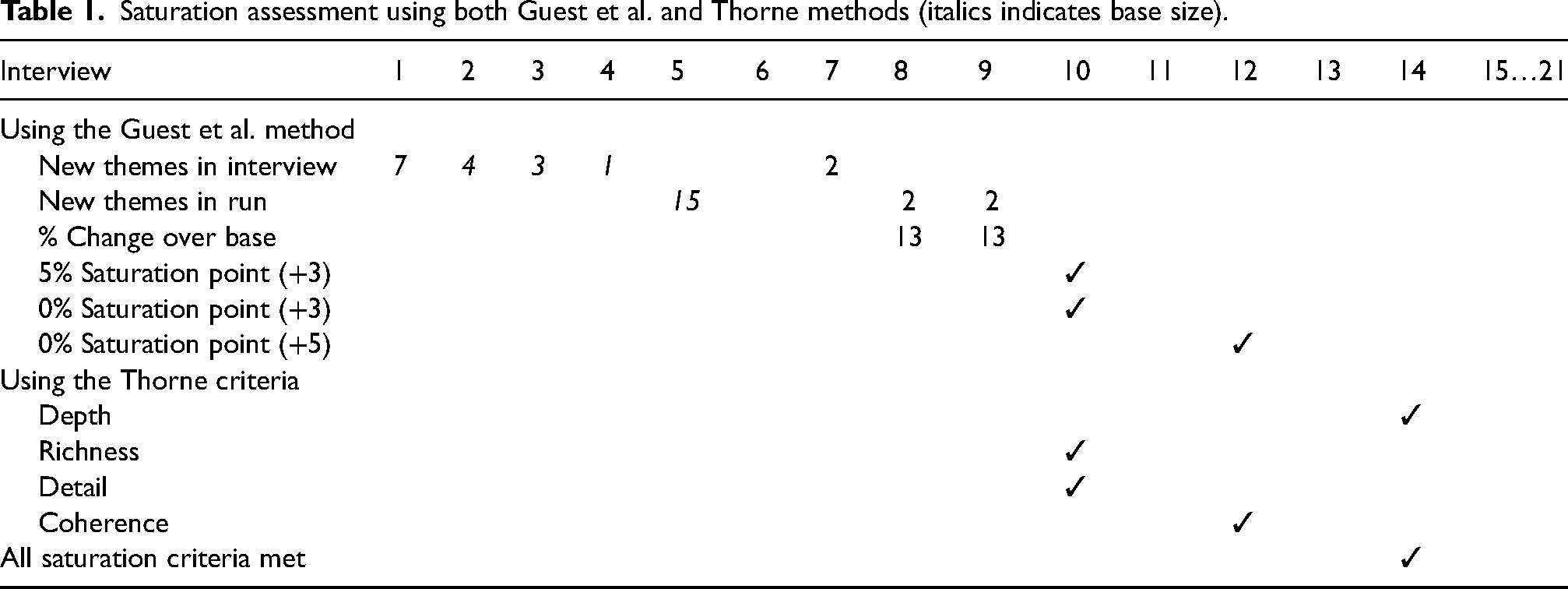
Using the Guest et al. criteria, the <5% and <0% saturation point was reached at 7 +3, with the 0% saturation points for run length of five both reached at 7 +5. Seventeen unique themes were initially identified. The base interviews provided 15 of these, with two additional themes discovered in the seventh interview and none after this point. Therefore, there was 13% new information in the runs ending with the eighth and ninth interviews, and 0% new information (meeting the predetermined threshold) in the 10th interview onwards. The more conservative 0% new information threshold using the longer run length of +5 was correspondingly reached at Interview 12.
Using Thorne's criteria, richness, and detail were both considered reached by the 10th interview, as no new themes or subthemes were emerging and the nuances of the topic fully explored. Coherence was considered met at the 12th interview, when no further ‘loose ends’ were identified in the research and a logical narrative was clear. Depth was the last criteria considered met by the research team due to cautiousness about ensuring all aspects of the topic had been fully captured and was satisfied by Interview 14.
While both sets of criteria were met by Interview 14, a further seven interviews were conducted after this as they had already been scheduled and further expressions of interest were declined. With interviews therefore continuing to 150% of those required to meet saturation criteria, the research team considered there to be a high level of reliability in the determination of saturation.
Interview procedures
Interviews were completed between July and November 2022. To ensure consistency, all interviews were conducted by a single researcher (MWS) who had completed external training in qualitative interviewing via Monash University. Interviews were conducted online via any of Zoom (Zoom Video Communications, 2022), Microsoft Teams (Microsoft, 2022), Skype (Microsoft, 2022), or telephone, and audio recorded. No time limit was provided for interviews, and the median length was 42 min with a minimum of 27 min and a maximum of 72 min.
The interview protocol was developed with a high focus on minimising any plausible wording (by being as neutral and open-ended as possible), habituation (by avoiding developing patterns of response), and acquiesce/social desirability (by masking any perceived interviewer preference) heuristics.51–54 Interview procedures are provided in full in Appendix I. Intelligent transcription was conducted by two reviewers (MWS and MK) in Microsoft Word (Microsoft, 2022).
Data analysis
Two separate forms of analysis were performed separately but concurrently: thematic analysis and Glaserian grounded theory. The two processes, although distinct, did overlap heavily as themes and theory often emerged from the data together. Firstly, the broad processes applicable to both analyses will be summarised; following that, specific processes to thematic analysis and grounded theory will be discussed separately.
Five broad stages were applicable to both thematic analysis and grounded theory development.28–30,32–36 Firstly, during the interviews, the interviewer took contemporaneous memos in a separate Microsoft Word document.33,36,55 Secondly, during the transcription phase – conducted by the researchers themselves to provide an opportunity for further familiarisation with the data – the transcribers could both memo in a separate Microsoft Word document, and also highlight key quotes within each transcript itself.33,36,55 Thirdly, completed transcripts underwent formal open coding, the segregation of data into discrete excerpts, by two researchers (MWS and MK) in NVivo (Version 1.0 [2020], QSR International, 2022).33,36,55 To prepare for coding, both coders jointly coded three training manuscripts. Once satisfied with consistency, transcripts were then alternatively allocated to one of two coders for individual coding. Five manuscripts (24%) were randomly selected for double coding using the function sample(1:21, 5) in RStudio (RStudio, 2022). The percentage of text coded to each code for these manuscripts was calculated and compared across both coders to calculate intercoder reliability in NVivo. This was ‘strong’ to ‘almost perfect’ under both Cohen and McHugh's criteria for all codes, with kappa ranging from 0.82 to 0.93.56,57
Thematic analysis followed six stages: familiarisation with data (achieved via interviewing, continual memos, and manual transcription by the researchers), initial coding, identification of initial themes, revision of themes (including considering latent themes), swapping all manuscripts for rereviewed by the alternate researcher to verify coding and themes, and interpretation.28–30,55,58 This process was inductive, where the researchers sought to draw out transferable findings from the data rather than to test hypotheses, and highly reflexive; coders met formally three times to discuss and refine codes and their emerging categories, themes, and subthemes, with further frequent informal discussions.30,55 Independence was maintained in early stages to minimise risk of confirmation heuristic.55,59 Initial interpretation was semantic; the coders took all interviewee statements at face value. 55 Following these, latent analysis was considered, as the coders attempted to interrogate meanings not explicitly stated. 55
Glaserian grounded theory was conducted separately but concurrently to thematic analysis.28–30,32–36 Theoretical sensitivity, the awareness of relationships between categories, was captured in memos throughout the entire process.32,60 Open coding, the segregation of data into grouped excerpts, was used for interviews one through fourteen, at which point saturation was reached.32,35,36 Constant comparison, where individual data excerpts are grouped via codes and continually compared against each other, was used throughout stages three to five described above.32,35,36 Theoretical sampling, the process of additional data collection during or after initial data analysis to address any discovered areas that require further investigation, was incorporated by including additional interview questions asking for participant interpretation of emerging findings from previous interviews. 61 For example, while Interviewee 2 was asked to reflect on points raised by Interviewee 1, Interviewee 21 was asked to reflect on all emerging themes. This process provided increasingly deep participant reflection as interviews continued. As the Glaserian method was used, there is no axial coding stage.32,35,36 From Interview 15 onwards, selective coding, the linking of categories, was used in both initial coding and recoding.32,35,36 After all themes were finalised, theoretical coding, the conception of a core category linking all codes, was commenced.32,35,36
Rigor and trustworthiness, the degree of certainty readers can have in results, was ensured by considering Guba and Lincoln's classic criteria of credibility, transferability, dependability, and confirmability during research design.39,61,62 Credibility, that the research accurately reflects participants’ reality, was captured by member checks where participants were presented with the list of their quotes to be used and the themes they were applied to, with participants empowered to provide or refuse consent without impacting their involvement in the study.39,61 Transferability, the applicability of findings across contexts, was provided for reader assessment by an explicit ‘thick description’ discussion of the sample characteristics, differences among participants, and clearly outlining how the data can and cannot be used in the limitations section for nonacademic readers.39,61 Dependability, analogous to reproducibility, was ensured by an exhaustive description of methods and appropriate, traceable data handling.39,61 Confirmability, the reduction of any individual's predispositions on results, was pursued by forming a multiresearcher team from three different institutions who initially reviewed data independently before coming together (described in more detail below under Data analysis).39,61
Ethics statement
Ethical approval was granted prior to commencement by the Griffith University Human Ethics Committee (GU 2022/096). Due to the risk for participant harm from discussion of psychologically stressful events, three mechanisms to protect well-being were built into the interview design. Firstly, participation was voluntary and informed, providing the opportunity to not engage if participants chose not to. Secondly, where an interviewee displayed any signs of significant emotional response, the interviewer paused the interview and explicitly offer the interviewee the opportunity to cease the interview. This occurred once, and the interviewee elected to continue. Thirdly, support services were made available to interviewees. These mechanisms are expanded on in Appendix I.
Participants were consented via one of two methods. The Consent Form was able to be digitally signed using university-approved online provider eSignature (DocuSign, 2022). If a participant was unable to complete the consent form online, participants were verbally consented at the commencement of the interview. At the conclusion of the interview, interviewees could elect to be provided with a copy of the transcript, and were additionally entitled to edit their transcript prior to coding; no interviewees elected to exercise this right. Specific consent was subsequently sought for every quote provided in the manuscript and appendices; this included providing the participant with the verbatim quote, the context it would be used in, and a statement that they were free to refuse without this otherwise impacting their participation in the study.
Initials have been replaced with randomly generated participant numbers to maintain deidentification. Incidents in Table 2 have been placed in a randomised order, and sequential incidents therefore do not necessarily relate to the same participant. An expanded deidentified selection of quotes to illustrated themes and subthemes is provided in Appendix III. Full transcripts are not intended to be stored in a public repository as, despite undergoing deidentification, the highly specific nature of these incidents (including multiple that were reported in mainstream media) means that reidentification remains a concern.
Characteristics of the study sample.
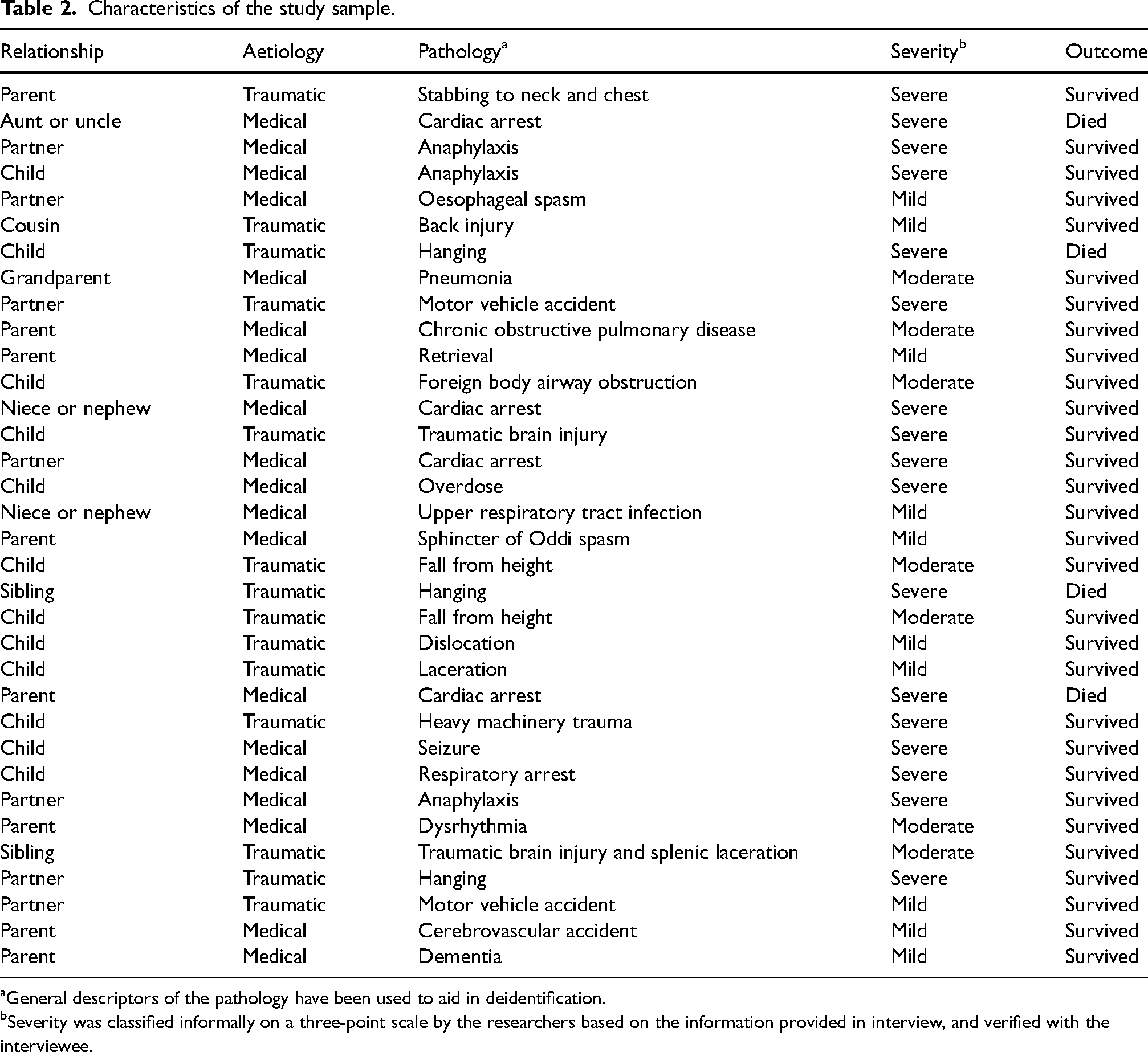
General descriptors of the pathology have been used to aid in deidentification.
Severity was classified informally on a three-point scale by the researchers based on the information provided in interview, and verified with the interviewee.
Results
There were 21 participants, collectively reporting 34 instances of attending their own families. The characteristics of these cases are summarised in Table 2. The degree of time elapsed between the incident and the interview ranged from 1 year to 25 years. All interviewees were employed by an Australian, United Kingdom, or New Zealand jurisdictional ambulance service at the time of the event. 62% (n = 21) of incidents were noted to be in a rural or remote area, a finding not anticipated by the research team who operate primarily in urban areas. No difference was found between immediate or extended family members, or between country of origin. Twelve percentage (n = 4) of incidents resulted in the death of the family member. Severe cases were overrepresented, comprising 56% (n = 19) of the incidents. In 32% (n = 11) of cases, the related paramedic drove to scene, in 88% (n = 30) they were the first response on scene, and in 50% (n = 17) of cases they continued working their shift after conclusion of the case.
For both thematic analysis and grounded theory, the core concept-category was ‘conflict between the roles of clinician and relative’. During thematic analysis, five themes and 24 subthemes were identified. The themes were: ‘the first few moments: shock, suppression, focus’, ‘the duality of clinician and family member’, ‘inconsistent organisational support’, ‘acute personal effects: the short-term consequences’, and ‘chronic personal effects: the long-term fallout’. These are illustrated in Figure 1.
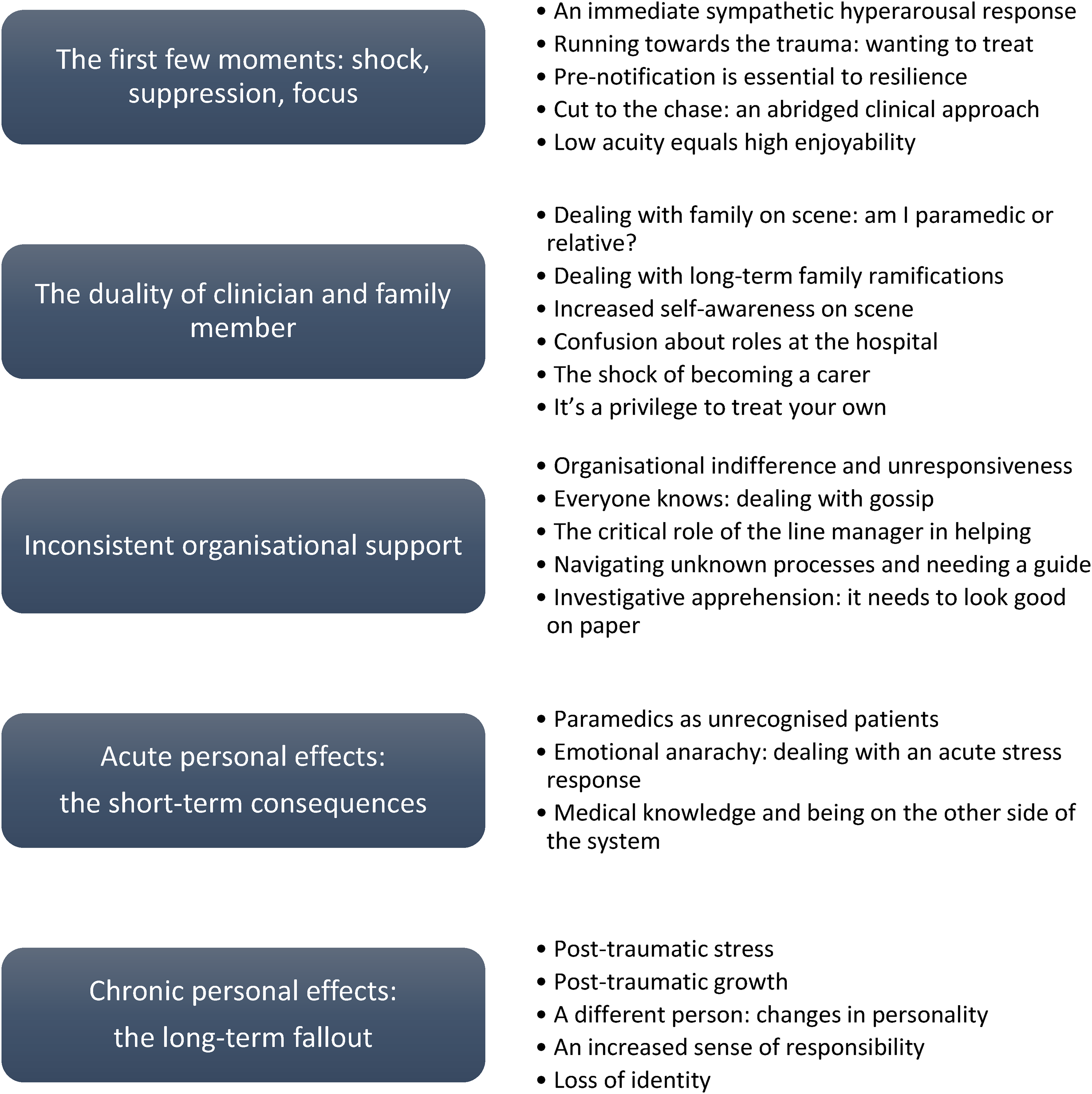
Themes and their subthemes.
A small selection of quotes to illustrate themes are presented here; these are selected for their conciseness and clarity of expression rather than comprehension or variation. An expanded list of quotes is provided in Appendix III. The five themes and 24 subthemes can be viewed either by who they relate to (family members, the employer, the paramedic alone) or temporally (those before arrival, at scene, immediately after, and long term).
The first few moments: shock, suppression, focus
There was near universal reporting of sympathetic hyperarousal to the initial dispatch. I was shaking. The adrenaline had gotten to me. The stress and panic had gotten to me. – 16 I was dumbfounded. It didn’t make sense. I thought Comms may have made a typo… you can’t comprehend what you’re reading. – 4 Fuck. That's not supposed to happen. – 8
Paramedics were quick to repress their shock, and stated they rapidly transitioned into ‘work mode’. We are action people. We arrive at something that is atrocious, but we take action. We move towards it. – 6 I think I said the F word. It's game on, isn't it? You just got to do what you got to do. – 11 I immediately dropped into full blown paramedic mode. It's so hard to explain the clarity of thought. Every synapse I had was on fire, and I was so calm and so concise and so exact in my decision making. I have never been to that place again. It was an extraordinary place. – 3
A latent theme was ongoing hyperarousal, despite being in ‘work mode’. When I went in I didn’t carry anything, I just ran in. – 20 I've just literally burst through the house. I've not looked in any of the corners for dangers. I just went in, blinkers on. – 14 Very heightened. I was in work mode, but it was very heightened. – 20 I knew I'd let the stress and adrenaline get to me, to the point I couldn't hold anything. My hands were very badly shaking… but then I went into training. It was all the training… it is almost a muscle memory. – 10 We're very good at mentally pushing family aside and putting on our paramedic hat and doing what needs to be done. – 14 I had no one else to call on. I was it. – 2 She was still my daughter, but I needed to help, I had to help, I wouldn't forgive myself if I didn't help. – 17 I'm too close to this, I can't make unbiased objective decisions. – 2 I knew I had to step back. – 14 I probably had a hundred and twenty seconds… I think it was good that I knew who I was going to, because otherwise you would have rocked up at the address and gone ‘boom’ [mimics head exploding]. – 1 The adrenaline was pumping the whole way, but there's enough time to kind of calm and rationalise before you get there. – 14 A lot of the stuff you don't need to ask… I don't want to waste any more time. – 20 After being with him and being acutely aware of changes in his status, I could tell that he was crashing. – 2 Instead of having to gather that history… we’re already doing things… It was a lot faster. – 12 As we’re there I’m kneeling on the ground, she's sitting on a chair, and we’re cuddling. – 14 And then when I saw him and I was like, you know, he's okay, it was kind of – let's go and give him a hug. – 21 It was a real easy job, I was there to help, I really enjoyed it… It was a joy, all of it. – 15
The duality of clinician and family member
Managing family on scene was noted to be difficult by many. I was just torn in every direction, and there was no way to handle it properly. – 20 It was less than a breath between being the mum and being the paramedic. Less than a heartbeat between being the mum and being the paramedic. – 14 It really tears at you professionally because I walked away from it feeling I was a terrible partner and a terrible paramedic. I felt I couldn't do both. Because I had her telling me that she just needed me and wanted me to sit and be her partner and that kind of thing. But I had to treat her because we didn't have enough resources on scene for me not to. – 13 I saw them at the funeral… I had a normal interaction with them, I think I might have said sorry a lot, but they weren't blaming me, even though I continued to blame myself. – 10 The next time I saw the family members, unfortunately was at her funeral. So that was quite challenging, because I felt that people were looking at me as if… you know she's the paramedic, and she wasn't able to save her life. So I felt like I was being scrutinized a bit at the funeral. – 6
Being self-conscious on scene was a latent theme. Because it's your family member it just it makes you so much more aware of what you're doing in each step that you're doing. – 8 All eyes were on me. – 16 [Doing a 12-lead on stepfather] He's hairy so I was like ‘Sorry dude, going to have to shave you. This is weird and creepy’. – 4 You don't think too much about the person that you're attending I suppose. – 9 You actually forget it's your mother. It's a patient. – 4
Transitioning out of the clinical role and into a relative role after handover was noted to be difficult, and this was exacerbated by a lack of clarity around rights and demarcation of roles. I remember this doctor looking at me with that ‘Who the fuck are you?’ look on his face… I was totally in paramedic mode. Like I gave handover, best handover ever, really impersonally, and then I stood back and watched them work on her. – 5 Probably the thing that infuriated me the most was that because I was in uniform the hospital staff didn't respect my relationship to the patient, and I found that extremely annoying. – 13 The doctors weren't actually believing that this child had arrested… I was like, ‘No, no, no! This kid has arrested. We have the ECG to prove it. Please. Look at her correctly, don't just dismiss her’. Because I was so junior, I’d not had a lot of experience, truly, having to fight, to advocate for your patient. – 3 I was begging them in the resus bay just to continue ventilating him. – 19 I was advocating so much that I was worried that I would be kicked out of the ED. – 3
Paramedics also reported difficulties after patient discharge, transitioning into being a carer. This was noted to impede their own psychological recovery. I went straight from being paramedic, straight into carer… I was a full-time carer, I was showering her, all of that. I've never actually had time to process anything. – 7 [Being a carer] Every day was like waking up in a nightmare…. I very rarely slept… Emotionally, it was taxing, it was like waking up in hell. Like it was a nightmare, I just couldn't believe it was happening. – 8
Many paramedics, particularly for low acuity cases, reported being grateful for the opportunity to treat their own family. I was just thankful that I was able to be there… you're grateful that you can help your family. – 20 It's a special privilege to treat your own and in many ways I would rather it be me than anybody else. – 4 It's a privilege too, to go to them. – 12
Inconsistent organisational support
A major theme across almost all interviews was inconsistencies, and occasionally a complete absence, of organisational support. They're pretty shit, I didn't get much support from my organisation. – 7 It was rubbish, it was absolute trash. – 12
This regularly included no debriefing, and also involved organisations disregarding attempts to seek support. Even though I talked to a manager a few days later, saying, ‘Hey, what happens when you attend your family?’ They weren't very helpful. And when I called up Comms and said, ‘Hey, I've attended a family member’, it didn't flag anything. – 11 There was actually no initial debrief done of the incident… my psychologist has identified as why it affected me so much was that I never got a chance to process what had happened at the scene. – 20 They never sent [anyone] to check on me. They never asked me how I was doing. They got cranky at me… The bit that stung the longest was that lack of organisational support. – 10 I didn't hear anything… Didn’t even reach out to see if I was okay. They just give you a number at the very start of your enrolment and go ‘Call this if you are not okay’. – 14 They absolutely did no sort of debriefing or anything. So it was basically as after any job, we would be expected to go back to work. There was no offer of that or anything. One of my colleagues called out the manager… he didn't really talk to me at all. I just said that ‘I'm going home’ through a haze of tears and then that was it. – 8 You would have to ask for that support. You wouldn't be necessarily offered it. – 21 It is very ‘you’ driven… You need to wave the flag basically. – 20
Others were indignant to learn that other organisations do offer proactive support. [Talking to a colleague from a different service] He goes, ‘Well that triple fatal is a sentinel event’. I go, ‘What is that?’ And he goes, ‘It is a sentinel event… we get a peer debriefing and a clinical debriefing’. I’m going, ‘What the? We don’t get anything like that. Are you joking? I have to go back to work’. – 13
Almost all paramedics reported experiencing being gossiped about after their case. This was noted to be a negative experience by several. It defines me in the area that I work. Everyone knows me as, ‘Oh, you're that paramedic that did that’. – 2 It's hard to move on when other people define you by what you were involved in. – 2 There's already a gossip chain happening by the time you get to hospital. You feel like confidentiality is gone, just wiped out. – 11 There were people knowing about things that they shouldn't of… I knew confidentiality had been broken, which made me resent those ambos more. – 14 When I did get back to work, it was just the constant bombardment of every person I saw wanted to hear what had happened. So it was that constant retailing of the story over and over and over again… I hadn't processed it myself. – 17 Most of the people that knew were my friends and I didn't mind it. I also think that talking about it was helpful for me rather than shutting it down. – 19 It became a thing at work with some people that we worked with were, ‘Oh, you guys, you just get everything because you were in this accident, and you're all treated special now, and you get whatever time off you want’. – 17
Many paramedics continued working for the rest of the shift, including after family fatalities. A latent theme was paramedics’ sense of obligation compelling them to continue working unless reassured that they did not have to. This was compounded as, in some instances, the organisations actively sought to have the staff return to work. They got in touch with me and wanted me to come back to work. – 15 I should have finished my shift after this job. But I didn't, and I kept going, and had like hectic case after hectic case, and ended with like a resus on the beach… I was so fatigued, so drained. All my shift I could see that something was definitely wrong with me. – 20 I took 24 hours off, and then we were very short staffed. We had no one, so I felt guilty, and I jumped back on. – 10
Long term negotiations with organisations were fraught with difficulty. Paramedics lost their positions, were required to reinterview for their own positions, and were interviewed as a group to determine who was at fault. There were few reports of positive long-term organisational support. I was basically interviewed for my job that I already had. Then I was put in with an instructor and given a viva that I was completely unprepared for, that I just failed miserably. And I literally walked out of headquarters… and I went and sat in my car and howled. Because I felt so insulted, and so assaulted, because I was unprepared for this interview. I thought I was going in for a chat about pathways back into work, and basically I ended up interviewing for my own job. I was heartbroken. – 6 The organization was like, ‘You guys are numbers, and we need answers to do our risk assessments, and we need to tick these boxes and these boxes. Who cares about your mental health?’ – 19 I had a bit of time off after my experience and then when I went back I had lost my part time status, my rank, and my home station. – 14
Immediate managers were often mentioned as being vital in assisting the paramedic through the acute stress phase. Many line managers were praised highly by interviewees. I came out of the doors after she had gone into theatre, and he was standing there, and he didn’t say anything, he just put his arms around me, and he just stayed with me for an hour or so… I always appreciated that, and I don’t know where he came from or how he even knew. – 9 It wasn’t the guys on the road that did me wrong, it was management that did me wrong. – 8 My workplace is fantastic, the area manager at the time, he didn't bother me, but he checked in on me every day, didn't phone me but he'd send me a message, be like, ‘Just checking in on you. Is there anything you need? Let me know if there's anything I can do for you’. – 12
Many paramedics were unsure how to navigate the situation. [My work partner] turned to me and said, ‘As I've just attended your family in front of you, you attend for the rest of the day’… I’m so junior, at this point I will do anything to please anyone. – 15 I couldn't sleep, and I just remember ringing my best mate, and just completely falling to pieces. And just being like, ‘This just happened. I don't know what to do’. – 10 I didn’t know these things. I didn’t know I could book off. – 13
Paramedics also reported feeling apprehensive at the potential that the case would be audited or investigated. If anyone has to go and review this case, you've got to be spot on… It's just got to be perfect, to make sure that I've got the right cover. – 15 It just made me a bit more meticulous about making sure that everything was done exactly the way that it should have been done so. There was no room for any sort of criticism. – 18
Acute personal effects: the short-term consequences
Among the paramedics who experienced severe and long-term psychological effects from attending their own family, several reported this being minimised, particularly in comparison to the patient they attended. A lot of them dismiss my experience, because I wasn't actually the one hurt. It's difficult to navigate that as well, and acknowledging that no, I did. This did happen, and I was diagnosed with PTSD. And it's yeah, it's… It was very much real for me. – 18 No one asked about me this whole time… It was obviously a huge thing for me. – 8 I was just considered as the person that happened to be there. – 14 [Referring to the patient] [My partner] said ‘I think she is clinically depressed’ and I said ‘If she's not I certainly am’.- 11 I was sitting there, and I'm typing away during my paperwork, and it just hit me. I completely broke down. What the fuck just happened? How is this even something that's just happened? – 5 I quit. – 7 If someone complains about a sore toe I’m going to punch them in the neck… I just couldn’t fathom and deal with the stupidness of people today. – 3 I walked out into the ambulance bay and lost my bananas. – 11 I never went back to work. – 1
Chronic personal effects: the long-term fallout
It was noted that, for some paramedics, attended their own family resulted in significant psychological harm. It was in December the following year that I started to get flashbacks of the apparatus that she hung herself on. – 19 I lost my relationship, and I have never had another relationship. – 18 I think it scared the shit out of the counsellor. – 7 I blamed myself for a long time. – 1 I had an emotional breakdown. I got angrier and angrier initially as the months went on… I started to, literally over about three weeks, I unravelled. – 20 I lost the trust that I could keep my family safe. I had never been in that position before. – 10 It changed me in ways that I never thought were possible. I had always lived my life with great joy and curiosity and complete confidence that it was going to be ok. That is what got taken away from me that day. – 16 Everyday I walk in the front door, that's like walking into the place that he essentially died. – 1 It enthused me to be a paramedic all the more, and it enthused me to be more capable, more knowledgeable. – 10 I’m not going to let this break me. – 7 Our job is not the be all end all. – 1 It made me feel toughened up a little bit maybe, a bit harder than what you maybe necessarily would have been previous to that. I think that hardness is a good thing to have to be successful in the role as a paramedic, and to be able to deal with the things that we deal with both physically and emotionally. – 17 It just adds to maybe almost a feeling of kind of armour. These are the things that I can do, and I'm not scared about going to these kind of jobs. – 8 Still the best damn job in the world. I would love to still be on road now. – 3 Am I more emotional than I was before? Shit yeah. – 4 I have become a more empathetic person to the survivors of suicide. Not that I wasn't empathetic, but you know I just have that extra understanding. – 9 It definitely gave me a different, deeper understanding. – 11 It really highlighted just how shit our services are out here, like just how horrific it is… the lack of support… terrifying to really find out how bad the system is for rural people. – 15 Well, what happened if something happens to me now? Who's going to come and look after me? – 5 That definitely contributed to my anxiety in that environment. I worked in that environment for 13 years and I did need to seek psychological support for anxiety working in that environment, and it definitely was contributed by that awareness that I would potentially be the responder to my family, and there is no one else. It does have an impact most certainly. – 20 [After resigning paramedicine and nursing for 13 years] I joined the ambulance service, that was my identity… My identity was so tied to that job so when all that happened I was so let down, I was so heartbroken…. even now, after nursing for however long I have been nursing for, I’m still a paramedic. I’m not a nurse. – 14 I lost my career. Something I loved. – 15 This job will eat you up and spit you out before you even know it. – 17
Explanatory grounded theory
Paramedics who attend their own family can be broadly segregated into two distinct cohorts based on the severity of the case and how favourable the outcome was. Those who attended low severity cases, or who rapidly achieved a positive outcome for their patient, often reported an enjoyable experience that they were grateful to have had with no meaningful negative consequences. The main theme reported by this cohort was a sense of gratefulness for the opportunity to help their family member.
However, the majority of respondents attended severe cases, occasionally resulting in the death of a family member, and their experiences were often described as traumatic and life-altering. This article has focussed on the second cohort, who both made up the majority of participants and who provide a greater opportunity to improve future outcomes by implementing amendments to practice.
It is theorised that a clinician attending their own family for emergency treatment disrupts professional detachment, increases outcome self-expectations, interrupts normal routines, and promotes overmedicalisation. Collectively, this leads to a greater likelihood of eustress progressing to distress, overwhelming of resilience, and heightened risk of psychological harm (both acute and posttraumatic stress disorders). This is exacerbated by lack of recognition of this event by organisations inhibiting comprehensive support mechanisms in both the acute and chronic phases.
Discussion
This research had three aims: firstly, to retrieve baseline data and perform thematic analysis on the experiences of paramedics who have attended their own families; secondly, to generate explanatory grounded theory; and finally, to translate these findings into recommendations for practice. There are five key findings here that match with existing literature.
Firstly, previous research has shown that training improves performance and minimises psychological harm in paramedicine, policing, and military populations.63–66 Consistent with this, the sample in this study stated that they consciously recognised an initial stress response as it occurred, and actively attempted to mitigate this by focussing on their training.
Secondly, knowing that they were about to attend family, and having time to accept this and mentally prepare for the scene, was subjectively regarded as critical to psychological resilience and clinical performance. Past research has found that mental preparation assists in minimising vicarious trauma, 67 transition shock,68,69 and emotional flooding. 70
Thirdly, despite the stress, wanting to treat family members was almost universal, and some stated they would attend even if they were not the crew dispatched. Proximity to a relative patient is already known to be sought by family members in the emergency department, 71 intensive care unit, 72 and paediatric72,73 contexts, and this appears to extend to the out-of-hospital environment as well.
Fourthly, participating in treatment was considered a ‘safe place’, with a latent theme suggesting it distracted from a relative's suffering, performance pressure, and other stressors. Similarly, some paramedics were initially disconcerted by treating their family, but once in a state of flow found that this eased. Both of these findings are potentially consistent with previous studies suggesting that distraction – here suggested to include focusing on work – reduces experiences of discomfort.74–77
Finally, many paramedics spoke at length about organisational issues, and this was viewed as a major theme. The core issues raised in the paramedics’ perception were a lack of support and guidance, including their employer not recognising the significant risk of psychological harm and providing support to mitigate this. Many paramedics did not receive any debriefing, despite evidence that a hot debrief is considered beneficial in upwards of 90% of participants. 78 Organisational stress is already known to be a preeminent stressor for paramedics.79,80 Paramedics have previously reported feeling demoralised when managerial support fails to materialise, a factor some research has suggested is exacerbated by a managerial culture that tends to respond with interrogation and analysis rather than empathy and compassion.80,81 Some individuals in this study stated that their organisation's focus on following procedure and risk management limited the ability to provide a humane response. Ongoing supports – often limited to informal check ins by an immediate manager – were stated to reduce dramatically shortly after the incident as other people ‘moved on’. Paramedics felt that, in the aftermath of an incident, organisational focus rapidly reverted from their health to finalising postincident reporting and pressuring paramedics to return to work.
This is a key finding for several reasons. Firstly, these are medical organisations, and provision of physical and mental healthcare is their fundamental function. Secondly, many of the paramedics noted that the organisations had support programs but identified that these either weren’t being initiated in their specific case or required the paramedic to proactively seek out support. Some paramedics reflected on their own heightened state impeding their ability to actively seek supports themselves, and that they needed to be referred. It is theorised by the authors that these two elements in tandem led to a disconnect between paramedics and contemporaneous support. Thirdly, some paramedics stated that attending their own family was not classified as a reportable event by their organisation. If true, given both that a diagnosis of posttraumatic or acute stress disorders do not require actually witnessing a traumatic event, the risk of psychological harm from attending these cases seems self-evident. 82 While the presence of organisational mental support services is correlated to reduced paramedic harm, it is intuitive that the access and use of these services is the mechanism enabling this.64,83
Translation of research into practice
One of the key findings of this study is that paramedics regularly reported the long-term effects being more important to their experience: the level of organisational support, the attitude and support of colleagues, and dealing with any investigation were routinely considered equally as traumatic as the incident itself. Organisational stressors are known to be a major contributing factor to paramedic stress.80,83 It is important to note that the majority of these incidents occurred many years ago and may no longer reflect current practice. Nonetheless, the responses suggest practical steps that may be taken by paramedics and organisations to mitigate harm from future incidents:
Having paramedics’ addresses preloaded into Computer Aided Dispatch's geospatial mapping functionality (as is already the case with entry codes, violence warnings, or similar) to notify dispatchers and supervisors. This would only capture incidents when the paramedic's relative patient is at home. Low paramedic threshold for seeking clinical advice on scene, due to the high risk of impaired decision-making. Maintaining confidentiality by all staff who are aware of the case. The decision to share their experience with coworkers should be at the discretion of the paramedic. Organisational recognition that attending a critical family member has a high risk for psychological harm to the employee. A mandatory hot debrief, followed by automatic stand-down for the remainder of the shift. Automatic referral to appropriate internal mental health services. This should not be a ‘one-off’ but include long-term follow-up over a period of several months and should be integrated into investigations and return to work plans. Organisational presumption that leave is to be granted after this event, with the paramedic able to waive this if they choose. The paramedic should not be pressured into making that decision at the time, as they may remain heightened. If the patient survived, information on support for carers should be provided.
The authors have not considered the feasibility or efficacy of these suggestions, and they are purely reported based on the comments of the sample group. Other critical perspectives – such as legal duty of care or impact on resourcing – are outside the scope of this article.
Limitations
There are five key limitations to this research; many of these are inherent to qualitative research, but are explicitly discussed here to ensure usability of this research for a general audience.38,84 Firstly, as with all participant recruitment via public advertisement, there is high risk of sampling impacting results.84,86 Due to this, the transferability of sample's findings to the larger population is unknowable. For those adopting a positivist view, it cannot be assumed that the experiences of this sample are universal, nor that they are representative of the population.
Secondly, this study does not contain any epidemiological investigations, and a rate of occurrence for paramedics attending their own families cannot be determined. Sample characteristics, such as the overrepresentation of rural and severe events, cannot be assumed to hold for the larger population.
Thirdly, while both semantic and latent themes were considered, this study was designed to investigate paramedics’ own conscious beliefs (i.e. ‘what people say they think’); any unconscious beliefs (i.e. ‘what people actually think’) may be different to this. Although all attempts were taken to minimise the risk of interviewers improperly impacting participant responses, including acquiescence and social acceptability heuristics (that interviewees are consciously or subconsciously reporting, or being influenced by, what they think interviewers want to hear), this nonetheless remains plausible.
Fourthly, the methods did not provide subgroup analysis to quantitatively capture severity or duration of the impact of attending their own family; while formal medical diagnoses (such as acute or posttraumatic stress disorders) were routinely discussed by participants, these have not been independently assessed by the investigators. While qualitative research does not capture rates of correlation, it can capture the strength of an experience by participants; as discussed in the Results and Grounded Theory, the entirely unique responses of paramedics attending low acuity and high acuity pathologies is suggestive of a connection between severity of the case and significance of the impact on that individual paramedic.
Fifthly, the study does not identify objective sources of harm or benefit, but only those subjectively considered as such by the participants. Guidance on the recommended mechanisms to manage this scenario are inferred from statements solely by participants themselves, and their efficacy is not considered.
Conclusion
This is the first research to investigate the experiences of paramedics attending their own family. For the small proportion attending a low acuity pathology, the experience was characterised as an enjoyable novelty. For those attending critical incidents, paramedics reported having a sympathetic hyperarousal response that they quickly suppressed, followed by a rapid transition into ‘work mode’. Some paramedics stated difficulty obtaining their normal state of flow during treatment and were faced with balancing dual roles as clinician and relative on scene – occasionally leading to a conflict in priorities. This conflict continued into the hospital, where paramedics struggled to transition out of ‘medical mode’ and, in some instances, into becoming a carer. Organisational responses were widely discussed as minimal, and in some instances became a major ongoing stressor. Paramedics reported short-term experiences consistent with an acute stress response, and a large proportion suffered negative long-term, life-altering consequences.
Supplemental Material
sj-docx-1-pam-10.1177_27536386231178961 - Supplemental material for ‘Send everyone, it’s my son’ – Combined Glaserian grounded theory and thematic analysis of paramedics attending their own families
Supplemental material, sj-docx-1-pam-10.1177_27536386231178961 for ‘Send everyone, it’s my son’ – Combined Glaserian grounded theory and thematic analysis of paramedics attending their own families by Matt Wilkinson-Stokes, Merianne Kellermeier and Steve Whitfield in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386231178961 - Supplemental material for ‘Send everyone, it’s my son’ – Combined Glaserian grounded theory and thematic analysis of paramedics attending their own families
Supplemental material, sj-docx-2-pam-10.1177_27536386231178961 for ‘Send everyone, it’s my son’ – Combined Glaserian grounded theory and thematic analysis of paramedics attending their own families by Matt Wilkinson-Stokes, Merianne Kellermeier and Steve Whitfield in Paramedicine
Supplemental Material
sj-docx-3-pam-10.1177_27536386231178961 - Supplemental material for ‘Send everyone, it’s my son’ – Combined Glaserian grounded theory and thematic analysis of paramedics attending their own families
Supplemental material, sj-docx-3-pam-10.1177_27536386231178961 for ‘Send everyone, it’s my son’ – Combined Glaserian grounded theory and thematic analysis of paramedics attending their own families by Matt Wilkinson-Stokes, Merianne Kellermeier and Steve Whitfield in Paramedicine
Footnotes
Acknowledgements
Thanks to Sonja Maria for consulting on methods and for proofreading a copy of the manuscript.
Authorship
The study was conceived by SW, designed by MWS and SW, recruitment by SW and MWS, interviews conducted by MWS, transcription by MWS and MK, coding by MWS and MK, analysis by MWS and MK, and drafted by MWS, MK, and SW. All authors have reviewed and approve of the submitted version of this manuscript.
Data availability
A deidentified selection of quotes to illustrated themes and subthemes is provided in ![]() . Full transcripts are not intended to be stored in a public repository as, despite undergoing deidentification, the highly specific nature of these incidents (including multiple that were reported in mainstream media) means that reidentification remains a concern.
. Full transcripts are not intended to be stored in a public repository as, despite undergoing deidentification, the highly specific nature of these incidents (including multiple that were reported in mainstream media) means that reidentification remains a concern.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. MWS’s research is generally supported by the Westpac Scholars’ fund, University of Melbourne's PhD Award, and the Australian Government's Research Training Program.
Research ethics and patient consent
Ethical approval was granted by Griffith University's Ethics Committee, reference GU2022/096.
Participants were consented via one of two methods. The Consent Form was able to be digitally signed using university-approved online provider eSignature (DocuSign, 2022). If a participant was unable to complete the consent form online, participants were verbally consented at the commencement of the interview. At the conclusion of the interview, interviewees could elect to be provided with a copy of the transcript, and were additionally entitled to edit their transcript prior to coding; no interviewees elected to exercise this right. Specific consent was subsequently sought for every quote provided in the manuscript and appendices; this included providing the participant with the verbatim quote, the context it would be used in, and a statement that they were free to refuse without this otherwise impacting their participation in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.