
Abstract
Occupational violence (OV) is an insidious problem for emergency medical services with continued high levels of paramedic exposure despite significant education and resources devoted to mitigation. Though there is considerable data on the epidemiology of the phenomenon, the available evidence on the experiences of paramedics exposed to acts of violence during healthcare is limited. Utilising a generic qualitative approach and a semi-structured interview framework, we examined the perceptions and experiences of 25 Australian paramedics who had been exposed to incidents of patient-initiated violence during out-of-hospital care. A general inductive methodology and a first- and second-cycle coding process assisted in the development of the principal concepts of the patient and the paramedic from the raw data. Subsequently, a further four main themes and 15 secondary themes were developed which characterise the influence of social interaction on the evolution of paramedic OV. The results of this study provide a unique insight into the phenomenon of paramedic OV. As opposed to the rudimentary manifestation of aggression typically endorsed by emergency medical services, aggressive behaviour during healthcare presents as a judicious interaction of dynamic scene management and situational context. The social interactions that occur during healthcare, and the premises which both promote and suppress this connection, were identified to exert significant influence on the evolution of aggressive behaviour. The consequences of these findings challenge traditional violence mitigation strategies which seek to position the patient as both the focal point of initiation and the key to its extenuation.
Introduction
Occupational violence (OV) is a complex social phenomenon of interpersonal aggression and violence directed towards an individual within the context of their work. 1 Though there exists contrasting definitions of OV, this study defines the act as; the extraneous abuse, threat or assault of an employee in the context of their work and involves a clear or implied challenge to the individual's personal health, safety, or well-being.2,3 OV is a concern for all occupations, however, paramedics a are subject to some of the highest incidences of patient workplace hostility with up to 90% of paramedics reporting some form of abuse, intimidation, physical and even sexual assault during their work.4–7 While paramedics are expanding into ever-increasing primary and allied health roles, the majority of paramedics still operate in an out-of-hospital setting 8 which presents a dynamic, inconsistent, and often volatile work environment. Close personal contact with patients, often during times of high stress, and isolation from the security and support systems that exist in other workplaces inevitability expose paramedics to risks rarely seen in other professions.9,10 Despite the scope and impact of OV on paramedics and emergency medical services (EMS), there remains limited data on the experiences and perceptions of those exposed to acts of patient-initiated violence. 11 It is this gap within the evidence base of paramedic OV that this study seeks to address. It is anticipated that if paramedics can better understand the rudiments of OV in their individual interactions, they may be better placed to both identify and control the threat of violence before a critical incident occurs.
Background
Paramedic OV complexity
Paramedic OV largely represents an intricate and dynamic demonstration of aggressive behaviour. Acts of violence are initiated by patients, family, friends, and even bystanders of the out-of-hospital care scene. 12 These individuals or groups present with their own characteristics of socialisation, culture, religion, and education, and each presents with their own motivation for initiating aggression, which may include frustration, injury, illness, and/or pain.9,13 The myriad of paramedic OV complexity and variability also extends to their work environment, with paramedics exposed wherever patient care manifests, including houses, streets, workplaces, the ambulance, and care facilities. Furthermore, paramedic OV can occur at any stage of the paramedic–patient interaction from the immediate patient care process, to transportation, and discharge of care responsibilities. 14 Despite the variances that exist globally between EMS systems, including educational requirements, skill credentialing, and operational practices, levels of paramedic OV remain largely consistent across geographical, cultural, and social boundaries.15,16
Paramedic OV mitigation
Despite the prevalence of OV among many professions including similar environments such as policing, the complex social, medical, and psychological influences that exist within paramedicine predicate EMS-specific understanding and interventions. 11 The inherent strategic approach of EMS towards OV mitigation is overwhelmingly focused on the identification, prevention and management of hostile individuals.11,17,18 This is evident through not only the perception of paramedics to the cause of OV but also through EMS and statutory bodies which promote the ideology of blame towards patients through OV education and campaigns such as ‘No Excuse For Abuse’.19–21 The current paramedic OV approach can be broadly classified into two distinct categories, that of proactive and reactive engagement. Proactive approaches include dispatch practices, situational and threat awareness, legal and penal strategies, body language assessment, and communication approaches. Reactive approaches dominate the OV mitigation training space and include de-escalation skills, body-worn cameras, chemical sedation, physical restraint, and self-defence practices. 11 However, despite the application of these OV mitigation practices their effectiveness remains questionable and the incidence of aggression and violence towards paramedics remains unacceptably high. 14 The focus of OV mitigation strategies on proactive and reactive strategies appears based on the limited evidence base and the disproportionate emphasis on alcohol, drug, or psychiatric-induced violence within this space.22–24 Though the influence of substance abuse and mental health on paramedic OV is acknowledged, there is a developing recognition of the role of the paramedic–patient relationship within this context.25,26
The paramedic workspace
Paramedicine is generally provided in environments that can be dynamic, hazardous and often outside the paramedic's control. The connection between the complexity of patient care and the environment or paramedic workspace is important. The paramedic workspace, which includes the relationship between the patient, their illness or injury, and the context of their engagement, is distinctive within healthcare. Furthermore, it is the workspace which contributes significantly to both defining and influencing behavioural processes and social interactions. 27 Campeau 27 identifies this turbulent aspect of paramedic practice, that is, the management of the out-of-hospital scene and its distinguishing environment, as the key characteristic that both defines and dictates paramedic practice.
The management of an out-of-hospital scene involves many physical and technical practices however it remains essentially a model of paramedic social processes. Campeau's 27 Space Control Theory of Paramedic Scene Management (SCTPSM) remains unique within the literature as the only theory identified that attempts to define the paramedic workspace in terms of its social interactions. The SCTPSM defines the scene management practices of paramedics into five fundamental categories of social processes that interact and evolve to allow the goal of scene manipulation and patient care. While this manipulation operates universally during paramedic scene activity, with varying degrees of experience and influence, it is a constant, with far-reaching effects on patient and scene outcomes. 27 It is these social processes that link the paramedic, the patient, and potentially the development of OV which this study seeks to explore.
Methods
Research design and paradigm
The aim of this study was to examine the phenomenon of OV from the perceptions and experiences of paramedics exposed during out-of-hospital healthcare. Based on this objective, a qualitative approach was applied, utilising the concepts of analytic presuppositions and theoretical framework; methodology and methods congruence; and rigour as identified by Caelli et al. 28 to ensure credibility. The research design of this study, including all elements of data collection and analysis, was undertaken against the principles of generic qualitative research within the paradigm of constructivism. The notion of a constructivist paradigm is based on the premise that individuals understand and respond to the objective world through the influence and existence of a wide variety of experiences. 29 A generic qualitative approach was selected due to the outward focus of the study. This outward focus, as opposed to phenomenology's inwards analysis of cognitive processing, is centred around the tangible experiences, opinions, and reflections of participants. 30 Importantly, a generic qualitative approach is congruous with the SCTPSM framework through a shared foundation of concepts, models, and sociology and psychology theory. 28 The SCTPSM theory utilises the sociological viewpoint of symbolic interactionism to explain behaviour as an individual's unique way of reacting to their interpretation of a situation. 31 Furthermore, this interpretation is characterised by the reciprocal relationship of the individual to their environment.
Data collection
Data collection occurred by means of an in-depth, semi-structured interview process with influence from the SCTPSM aiding in the construction of the interview agenda (Appendix A). Data collection commenced on the 29th of April 2019, and was completed on the 3rd of July 2019. All interviews were conducted in-person and undertaken by the primary researcher. Following each interview, a reflective memo was created to document professional appraisal, personal emotions, and areas for further exploration. Any developing themes were also reflected on and documented. All transcripts were entered into the research data management software NVivo 12 for further analysis. The authors acknowledge paramedic OV can be perpetrated by an array of groups or individuals and for a variety of reasons. Indeed, the complexity of paramedic scene management can require the simultaneous management of a selection of these individuals. Rather than isolating these individuals, an inclusive approach was identified as providing the most benefit. Therefore, to avoid confusion, the term ‘patient’ was utilised within the data to describe any perpetrator of paramedic OV.
Recruitment
Paramedics employed by two Australian state-based EMS organisations, namely the Queensland Ambulance Service (QAS) and Ambulance Victoria (AV) were invited to participate in the study via dissemination through individual specific research or clinical governance departments. Participants who expressed a desire to participate in the study contacted the researcher directly by email or telephone. Paramedics from the New South Wales Ambulance Service (NSWAS) were also considered. However, the NSWAS declined study support. The EMS were invited based on large active populations of paramedics and documented issues of paramedic OV.32–34 To be eligible for inclusion, participants required exposure to an OV incident within the healthcare context of their paramedic responsibilities. To capture a comprehensive representation of the phenomenon the study included both physical and verbal forms of aggression in the definition of OV.
Participants
Through purposeful sampling, 25 paramedics were recruited for participation, with a diverse collection of gender, experience, and geographical locations selected. Seventeen participants were recruited from QAS and eight from AV. The number of participants (N = 25) is principally acknowledged as a sample size sufficient to allow a thorough examination of a study's research characteristics. 35 Total participants included 16 males and nine females, three critical care paramedics and 22 advanced care paramedics. Sixteen of the paramedics were recorded as working in an urban environment, classified as the city and surrounding areas, while nine were recorded as rural. The mean age of the participants was 43.5 years (range 25 to 62 years), with a mean work experience of 15.7 years (range 2 to 40 years). To preserve the confidentiality of the paramedics involved in the interview process, all participants were assigned a pseudonym through the generation of a unique professional code. These codes were utilised for all elements of data collection and analysis.
Data analysis
Analysis of the data was approached via a general inductive methodology. A general inductive style was chosen over other more structured methodologies for its ability to explore the data while still allowing findings to develop from any prominent outcomes. 36 The data analysis and coding for this study utilised in vivo to assist in the generation of first- and second-cycle coding through which evolved supported categories and themes. 37 The second cycle coding procedure employed a focused coding methodology to identify the most prominent codes from the first cycle. The salient codes were aligned to specific categories from which parent codes, child codes, sub-categories and sub-sub-categories were created. The implementation of memo writing also further refined and guided this data analysis process. The study utilised the strategies of Morse et al. 38 and the approaches integrating methodological coherence, sample appropriateness, concurrent collection and analysis of data, and data verification and theory development to assist in the application of research reliability and validity.
Researcher characteristics and reflexivity
The authors acknowledge an extensive background in paramedicine, through either an operational or educational capacity. The lead researcher is a critical care paramedic within an Australian EMS, with over 21 years of operational experience. All authors have experienced the nature and characteristics of paramedic OV and recognise that this awareness may have influenced the collection and analysis of the data. Regular de-briefing between the authors assisted in the introspection and awareness of this process.
Ethics approval
Ethical clearance was obtained through the Queensland University of Technology Human Research Ethics Committee, approval number 1800000763, with additional approval attained through the relevant EMS organisations of participants.
Results
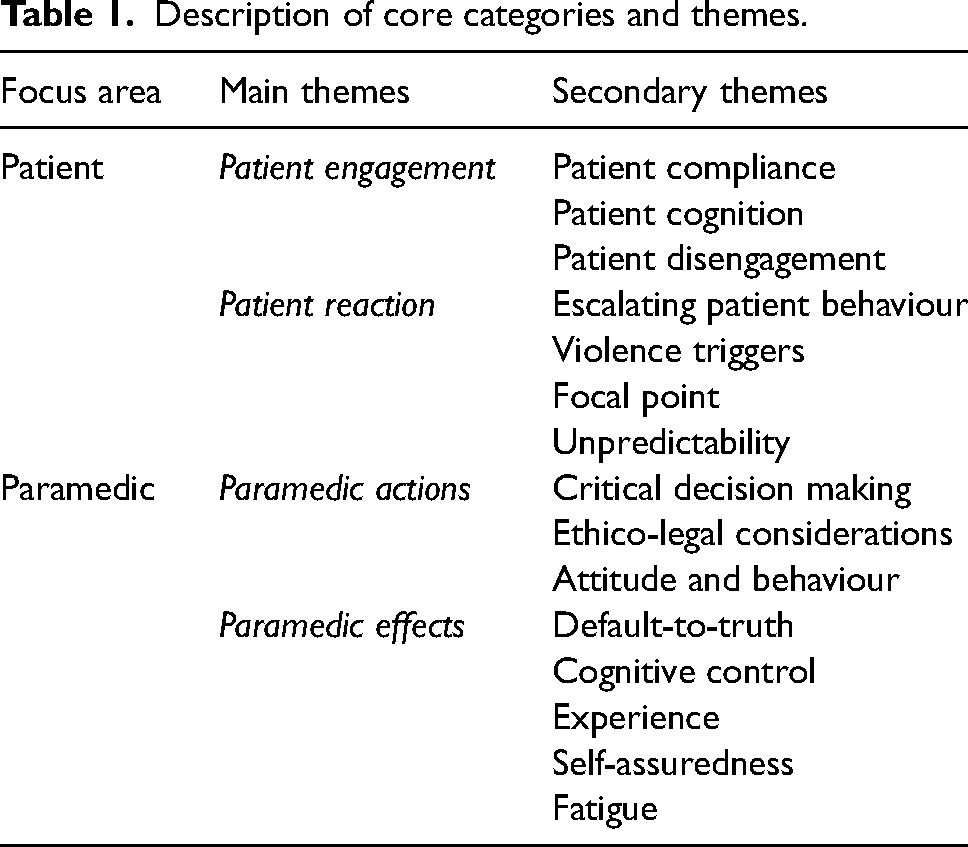
Using the SCTPSM as a lens for this research exposed the social constructs of paramedic scene management and the bilateral and complex interpretation of aggressive behaviour. The participants’ descriptions of violence involved an array of patients, contexts, settings, and influences. The principal concepts that emerged from the data, that of the patient and the paramedic, represent distinct ideas that characterise the specific roles, interaction, and context of paramedic OV development and its mitigation (Table 1).
Description of core categories and themes.
The patient
The main themes that emerged from the patient construct, patient engagement and patient reaction describe the actions of the patient towards the paramedic during the development of violent behaviour. Specifically, the themes correlate to the ability of the patient to participate in social interaction and their subsequent response to this engagement.
Patient engagement
Patient engagement acknowledges the psychological and physical connection, or lack thereof, established between the patient and the paramedic to enable the process of care. Patient engagement may comprise many forms of social interaction, including both verbal and nonverbal interactions, and be either direct or indirect in nature. Examples of patient engagement may include voiced communication and collaboration, conformity with direction, or even a lack of resistance to assessment and treatment. Even though the timing of this connection may vary due to the nature of the patient's injury or illness, the act of paramedic–patient engagement is a crucial predisposing element for the development of violent behaviour. The interview process further identified three patterns of behaviour which were critical to the development of paramedic OV. These patterns were secondarily themed patient compliance, patient cognition, and patient disengagement.
Patient compliance
One of the most common patient characteristics identified by paramedics prior to violence escalation was the absence of explicit hostility. In contrast to the conventional perception of an overtly aggressive or violent patient, paramedic OV was typically identified to present with a patient amenable to assessment and treatment. The initial display of patient compliance to the paramedic is important and demonstrates not only the concept of a bilateral social process but also the deterioration of that process through unrecognisable or unexpected events. (The patient's) behaviour in the early stages wasn’t aggressive or violent or threatening. It was somewhat subdued really and there was consent obtained early on. D37MA13U We sort of agreed that she was calm and compliant and that was even something we said to the police, said look, she's talking to me, she's letting me do observations, she's compliant. N47MA19U
Patient cognition
A key factor in the ability of paramedics to establish a social connection with the patient is the capacity of the patient to both understand and react to that interaction. A deterioration in a patient's level of cognition was acknowledged as not only compromising communication and decision-making processes but also influential in the development of violent behaviour. Presentations within out-of-hospital healthcare which may influence a patient's cognition include alcohol and drug intoxication, mental health, trauma, and social issues. I honestly think it was delirium. He didn't set out to get me. I don't think he knew what he was doing at the time. T47MA10U He wasn't in the space to understand and I guess if I think about that, well that's not just behavioural. T54MA24R
Patient disengagement
The engagement of the patient to the words and actions of the paramedic is critical to the continuing maintenance of scene management and healthcare. A breakdown in the relationship between the paramedic and the patient disrupts social processes and the ability of the paramedic to respond and react to the requirements of the patient. Furthermore, without the ability to effectively communicate, the palliation of heightened or aggressive behaviour through mitigation strategies becomes increasingly difficult. A disengagement, either physical or psychological, was frequently identified as a precursor to the escalation of violent behaviour. He was sitting up or turning around to sit on the side of the stretcher. Maybe even also his reluctance to listen. It almost seemed like he had disengaged with me and what I was saying. E41MA15U I said, we're here now. What's happened? (the patient) was just, no, go away … we did sort of try to just be, like, what's going on? What's happened? Can we do anything for you? It was just a brick wall from her. R25FA02R
Patient reaction
In contrast to the establishment of social interaction, the theme of patient reaction identifies the response of the patient to paramedic behaviour during assessment, treatment, and transport. Importantly, the actions of the patient do not occur spontaneously, but rather as a direct result of the decisions and procedures of paramedic care. Four secondary behaviours of patient reaction were categorised from the data and were acknowledged as key events to the evolution of OV. Three of these events, escalating behaviour, violence triggers, and focal point, identify patient behaviour preceding hostility, while the fourth, unpredictability, addresses a critical element of this behaviour. An important feature of patient reaction is the tendency of this category to be affected by the influences of patient engagement. This effect is evident in individuals with diminished cognitive processing, where impairment from factors such as alcohol consumption may reduce their capacity to moderate or rationalise behaviour.
Escalating behaviour
The transition of a patient towards a verbal or physical demonstration of violence against a paramedic is rarely a simple or linear process. This is reflected in the nature of violence manifestation where paramedics disclosed that while escalating aggressiveness was common, a patient's behaviour was just as likely to proceed through to a sudden escalation or ‘snap’. The irregularity of this behaviour was identified by paramedics as an inconsistent and unreliable indicator of OV. It started verbal, and then body language and then some actions started to reflect that, with the tearing off of the leads, an incidental strike and making moves to get out of the car. N56MA15U Nothing to say that he was upset. No swearing at me, nothing prior. Just zero to 100. N31FA11U
Violence triggers
The suddenness of a patient to a direct expression of violence against a paramedic is rarely the result of a premeditated act. Undertakings of aggression, compelled by patients in response to a danger or threat, are often closely linked to social interaction. The reactions or ‘triggers’ are linked to deep rooted primal instincts and can result in behaviour that is rapid and inconsistent with the perceived level of threat. Violence triggers can include, insult, injustice, self-defence, protection of family, property or loved ones, restraint, confinement, or impediment of objectives.
39
I've not ever been assaulted before. I kind of felt that I was really good at reading situations and I'm a self-proclaimed wuss, so I won't go into these situations. But yeah, I obviously said a trigger word to him. Y41FA17U I can talk most people around to those things, but definitely, it was me. Wasn't my partner and it wasn't really the police. It was me. I was the person that'd taken away – given something against his will. T54MA24R
Focal point
It was identified by paramedics that as opposed to a confrontation towards both paramedics on a crew, acts of aggression were predominantly directed towards a single officer. Fundamental to behaviour was the establishment of a focal point for their attention and the exclusion of other external attention sources. Though this can occur at any time or location, even with other individuals or the police nearby, it represents an acute and dynamic change in the patient's pattern of behaviour. Typically, this type of behaviour is preceded by an element of social deterioration prior to initiation. Then just before she lunged, her focus was purely just on my partner. E35FA05R Police came and a single responder (critical care paramedic) came as well. So we got out with the police and she just continued. Mainly at me, not my partner. R25FA02R
Unpredictability
The out-of-hospital care environment and the patients who inhabit its space are imbued with the uncertain and the unknown. The complexities of human behaviour and the characteristics through which patients engage, react and respond are influenced by their individual principles formed through background, education, culture, religion, and morals. With these limitations there is no clear means to comprehend how an individual might react to a given situation. This is reflected through the perceptions of paramedics that some violent behaviour may be both unpredictable and unavoidable. That's what really spun me out about this particular job, is that there was no fist clenching. He made good eye contact. He spoke well. He was even probably polite. The first time he raised his voice was when he jumped off the bed. By the time I actually heard it, he was on top of me. Y41FA17U This was the first time I've been put in harm’s place in the work environment where there was no indication of it prior. And the fact that I'd already been there for 20 min, and his demeanour hadn't changed. H32MC11R
The paramedic
The central focus area of the paramedic represents the influence of the clinician on the development of patient-initiated hostility and the influence of key stressors on this process. In contrast to the previous area of the patient, which reflects how a patient connects and interacts, the themes of the paramedic reveal the processes which generate the patient response. The progression of an EMS tasking requires paramedics to undertake a myriad of key decisions to facilitate the effective treatment and transport of an ill or injured patient. These decisions begin prior to arrival on the scene and continue until the patient has been discharged from paramedic care. Critically, the decisions made by the paramedic during this period can influence both scene management practices and the development of OV. Categories were organised against the influences of either paramedic actions or effects.
Paramedic actions
The theme of paramedic actions is comprised of three key areas of paramedic decision-making and actions in response to scene management evolution and include critical decisions, ethico-legal considerations, and attitude and behaviour.
Critical decisions
The ability of a paramedic to undertake critical and time-sensitive decisions provides important junctures to the direction of patient care and can be critical to the development of violent behaviour. These decisions, typically based on limited knowledge regarding the individual and the context of their care, can be profound in their consequences. Choices based on paramedic traits including personality, training and experience are critical to the decision-making process, however, there are also external pressures to these decisions e.g., legal considerations, which can dramatically influence this judgement. I guess it's that hard decision to make, isn't it, these people come over and you try and engage or not engage. Before you know it, you're arguing with drunk people who are impossible to negotiate with. E28FA07U So that's why I stepped in and I figured the safest way of stepping in was to remove the ability to drive off. There was no – perhaps I did a stupid thing, who knows, but at the time it was for the right reasons. N46MA19U
Ethico-legal considerations
EMS and Paramedics are accountable for the way they provide care to the ill and injured within the community. This accountability, which is guided by legislation, and organisational ethics and standards, imparts significant influence on paramedic–patient engagement. An important feature of paramedic decision-making is the effect of these ethico-legal considerations on the way in which paramedics choose to administer care. Paramedics identified misperceptions regarding their rights in the treatment or non-treatment of aggressive patients as a point of confusion and even danger. Understandably the organisation puts the wellbeing and safety of their staff (first). But then are we putting ourselves at risk if something happens to the patient while in our care? I'm just struggling to find a middle line right there. E41MA15U I thought, well, this guys on the road. Maybe from my own point – if I'm there, and he gets hit by a car, I've got some responsibility and some accountability for that as well. N52MA17U
Attitude and behaviour
Attitude and behaviour describe the manner in which a paramedic thinks and the physical manifestation of that process through their associated conduct and actions. Not only will the demeanour of the paramedic affect the initial patient interaction but its influence will extend to the decision-making processes that define the interaction. Of all the themes that comprise paramedic self-determination and the evolution of OV, it is the disposition of the paramedic that is of the greatest importance. The (data terminal goes) off, and (paramedics can) start to lose their mind on the way to the job which means they walk in already with a distorted, closed view on what's going on, and create bedlam when they get there; just either in their attitude, in their demeanour, (or) in the way things come across. H55MC30U A lot of situations get out of control just with verbal and non-physical aggression. I think something we could probably focus on more is … what role we play in not necessarily causing these situations but contributing to them. E28FA07U
Paramedic effects
In contrast to purposeful paramedic actions, paramedic effects refer to elements largely outside the self-determination of the attending paramedic and represent influences that either directly or indirectly affect decision-making. Paramedic effects are comprised of two intuitive elements, Default-to-truth and cognitive control, and three personalised elements, experience, self-assuredness, and fatigue. Notably, the effect of these influences on paramedics and their work practices is unique, and paramedics remain constantly vulnerable to these biases throughout the course of patient interaction.
Default-to-truth
The concept of default-to-truth represents a challenging obstacle for paramedics and their ability to manage patient hostility. Default-to-truth is an innate cognitive bias that presumes that the words and actions of individuals are inherently truthful.
40
This position, while essential for paramedic practice and the management of a patient's injury or illness, exposes paramedics through a misguided belief that patients will not target them with violent behaviour. I'm not going to move away from you. I'll give you a bit of space, but I think you're just a bit confused and postictal and I think you're sick … it's just hard and I try in this job, I think, to give people the benefit of the doubt. R25FA02R It is hard but I'm always conscious. I always give people a second chance, right? I've always had that attitude. L37FA12U
Cognitive control
Cognitive control refers to the cerebral processes that allow for a diverse and adaptive range of performance functions. Cognitive control is an essential element of OV mitigation practices as it allows an individual to countermand instinctive impulses and supports goal-orientated decision-making. Though education and training can help in controlling cognitive load, paramedics acknowledged the difficulty in managing these emotions while attempting to rationalise and problem-solve heightened situations. It's almost like an out-of-body experience. I sort of talked about it with another girl at work, who I've worked with, and she's been the victim of domestic violence. She said it's quite similar. You have this out-of-body experience, where you're thinking about all this other stuff, apart from what's actually going on. N52MA17U (It's a) pretty big amygdala response; you're in flight or fight but you've still got to work through the process. N53MC35R
Experience
Paramedic experience represents a refined ability to use high-level communication and interpersonal skills to know when and how to act, and is obtained only through innumerable hours of patient interaction and management.
41
Experience is highly valued within paramedic practice due in large to the isolation and lack of oversight that characterises its practice. Experience was acknowledged by paramedics as a critical aspect of scene management practices and the manipulation of aggressive or violent patients. As I say, good judgement comes from experience, experience comes from bad judgement … I hate to say this but sometimes it's only through experience, and through getting it wrong and surviving it, that you get better at deciding how you do things. H55MC30U A bit more of it was more experience and having done it before and having been in situations like this before. N53MC35R
Self-assuredness
Despite its perceived benefit, the role of experience and its connection with paramedic OV is problematic. The paramedics interviewed for this thesis had an average work experience profile of over 15 years, yet their previously acquired knowledge was unable to effectively mitigate their OV incident. Self-assuredness refers to the misplaced confidence of a paramedic to manage a patient without the prospect of aggression due to their perceived experience in similar situations. Though there are many factors that can increase the risk of self-assuredness, at the core of the trait is the overconfidence that comes from previous safe patient interactions. We were just working through this very familiar job. We weren't trying to escalate anything. We weren't trying to start something. It – we were just trying to get through it. We've gone through all this before. It was a very similar scenario that we've done a hundred times. S35MA10U Put my mug up there and say, this is a guy, who has been in the job for 15 years, he was a former soldier. He knew the ropes and it surprised him N52MA17U
Fatigue
One of the most readily identifiable features of reduced paramedic performance and the onset of paramedic OV is the mental and physical effects of fatigue. Fatigue is a common issue within paramedic practice due to the 24 hour, 7-days-a-week rostering that ensures continual community medical care. Paramedics highlighted the challenges of maintaining concentration and patient engagement when affected by fatigue, and even more so if compounded by hunger or poor diet. Of course, it was coming towards the end of a nightshift, it was an overtime shift. I was tired, probably don't have as much of a heightened sense of awareness as I would at other times. E28FA07U You know, you are always tired on nightshifts, and you really have to dig deep sometimes. Take some really big breaths and go okay, I've got to get this out. L37FA12U
Discussion
Social interaction is the dynamic interplay of communication and connection that occurs between individuals or groups to facilitate collaboration. 42 Without this exchange, there is no social relationship and no interaction or engagement between the paramedic and patient during care. Central to the development of any social interaction is the explicit influence of the individuals towards the process, with the most prominent individuals in out-of-hospital healthcare being the patient and the paramedic. The ability of the paramedic to engage with the patient and the patient's reaction to this engagement can profoundly alter not only the behaviour associated with the interaction but also the associated progression of scene management objectives. Although most patient engagement and reactions to paramedic scene management processes are cooperative and amiable, there are elements of the social interaction process which are closely associated with paramedic OV.
The results section of this study provides a framework of paramedic–patient influences through which the evolution of paramedic OV may occur. In isolation, the themes of the paramedic and patient represent important elements of the OV process however when these themes are considered against their correlating healthcare relationship their importance to violence mitigation is evident. The significance of this position is its connection to a key principle of healthcare practice, that of interpersonal relations and their influence on the trajectory of patient behaviour. 43 The interpersonal relationship between a clinician and a patient is the foundation of all clinical care and the framework through which a patient's healthcare experience can be explained and rationalised. 43 Presented within the domain of professional nursing practice, Peplau's 43 interpersonal theory postulated a contextual health philosophy that social interactions between individuals can be observed, described, understood, and if harmful, altered. Peplau's 44 theory identifies the clinician–patient relationship as a unique category of interaction, where instead of a dominant social association, the interaction occurs as a mutual undertaking of healthcare. The clinician–patient relationship comprises a bilateral connection which is utilised to identify the presenting problem, understand the problem within its construct, and appreciate, apply, and evaluate remedial measures. Such is the importance of this relationship, that Peplau, 44 places this bond at the centre of healthcare practice. Though established from the nursing milieu, Peplau's, 44 theory transfers innately into paramedic practice as the model is centred on the clinician-patient interaction experience. The emphasis on interpersonal relations and associated verbal and non-verbal communication allows the application of the model in any area of healthcare where a lived experience approach may apply. 43
Interpersonal theory describes the necessary social framework and reciprocal connection between a clinician and patient. 44 However, the paramedic-patient relationship in isolation does not determine violence initiation. It is the influence of this relationship within its context, including both the injury/illness and the situational environment, that defines and dictates this engagement. Social interaction is dependent on the constant interchange of expectations and perceptions of one party (i.e., the patient) with the tangible response behaviour of the other (i.e., the paramedic). 44 Within healthcare, the encumbering role of illness and injury on the clinician–patient relationship is considerable and places additional stress on patients outside of the presenting complaint. Patients experiencing health disorders are often required to manage relationships with health professionals, pain and incapacitation, new environments, maintenance of self-image, interaction with friends and family, and preparation for uncertainty. 45 Furthermore, perceived inequalities in social class, ethnicity, gender, and other social differences further exacerbate these demands. 46 Too often, the interpersonal needs of the patient are neglected by the healthcare worker in the urgency of diagnosis and treatment, thereby cultivating an atmosphere of anxiety and disconnection between the participants.44,47 In regard to OV, it is essential for paramedics to maintain control over the stimuli, messages, and cues that they present to a patient. Patients will define the actions and behaviour of paramedics, both verbal and nonverbal, constantly and often instinctively. Although this conduct forms part of social interaction and generally occurs without consequence, seemingly innocuous behaviour towards vulnerable patients, particularly those under great stress, who are ill and/or experiencing psychiatric problems, can result in a misconstruction of motives and intentions with potential violent results.44,46,48
A model of OV and the influences of the paramedic, the patient and the context of their interaction was first conceptualised by Nijman et al. 49 through their study on aggression in psychiatric hospitals (Figure 1). While the clinician–patient relationship had been identified as a precursor to violence prior to Nijman et al. 49 the authors were influential in establishing the interplay of the three distinct determinants in the process. The model of aggression developed by Nijman et al. 49 establishes the patient, the environment, and the staff as essential incendiary stressors in the development of OV. First, the patient and their underlying mental cognition, including emotional reasoning e.g., anxiety, substance abuse, and neurocognitive disorders e.g., dementia, that provides the core element in this process.49,50 Second, the environmental attribute of hospitalisation (or, as in the case of paramedicine, the out-of-hospital scene) with unfamiliar and confined surroundings with often reduced privacy and invasive procedures, that inevitably heightens the internal pressures on the patient. 49 This is the same stress that Knor et al. 25 and Pourshikhian et al. 1 termed “event shock” in their descriptions of the causal conditions of paramedic OV. Last, the staff or clinicians, through problematic interpersonal communication and conduct, inflexible care pathways, self-determination, and behavioural inconsistencies that provide the social stress and ultimately the impetus for aggressive behaviour.49,50 The model of patient aggression as expressed by Nijman et al. 49 is profound in the sense that it does not apportion responsibility for the violent act upon the disease or injury itself, but rather the processes including the treatment, the setting, and the interpersonal relations, as the provocation to this behaviour.
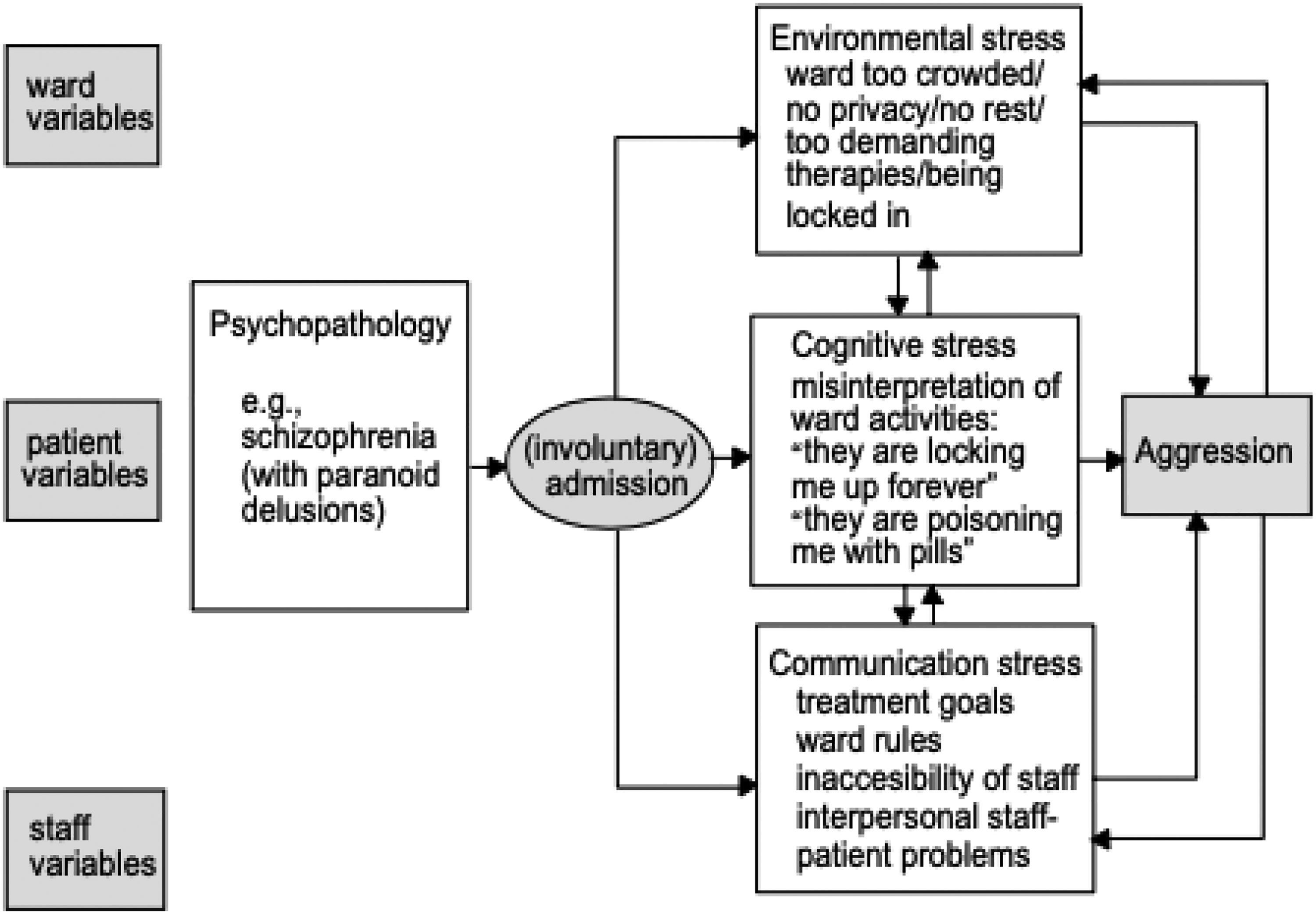
Model of aggression in psychiatric hospitals. 50
The acknowledgement that paramedic OV extends beyond a simple manifestation of hostility and is rather a dynamic representation of the interplay between the patient, the paramedic, and their current environment is significant. Positioning acts of paramedic OV as a mutual process represents a considerable shift in the way that aggressive and violent behaviour is understood, predicted, and mitigated within EMS. The mutual position provides a contextual setting for the evolution of paramedic OV but also expands the comprehension of why individuals may engage in violent behaviour.51,52 This shift acknowledges that the hostility generated by a paramedic–patient interaction is frequently the result of diverse organisational and individual influences, including professionalism, fatigue, an inability to compromise, cognitive deficits, and job demands.53,54 When this perspective is applied to OV mitigation strategies, not only can it result in improved patient-centred care, but it can actively decrease the elements that aggravate interpersonal violence.19,46
However, the acknowledgement of a bilateral rationale towards paramedic OV does present a challenge to EMS organisations and paramedics. First, the acknowledgement encourages individual paramedic self-reflection and their role and responsibilities within out-of-hospital healthcare. Second, the social processes and ‘soft skills’ such as communication, required to undertake these tasks remain often underappreciated and unarticulated within the health professional skill-set.47,55 Last and critically, it compels EMS to recognise that existing practices of paramedic OV mitigation including coercive control techniques of restraint and chemical sedation may be actively contributing to the evolution of patient hostility and violence.44,51
Despite these difficulties, perhaps the greatest challenge for paramedic OV mitigation is the premise of unpredictability. Unpredictability is endemic within paramedic practice due to the vast array of environmental, patient, paramedic and contextual variables which pervade any social interaction. 27 It is essentially impossible to know how an individual will react in a situation, even before the consideration of elements which may further influence cognition including drug and alcohol use, or psychiatric illness.1,25 Such is the impact of these features that they form a pattern of inevitability which may all but preclude the complete prevention of violent and aggressive behaviour. 56 Though the concept of unpredictability may appear to render a degree of futility towards mitigation practices, its acknowledgment can provide alternate insights into this phenomenon through such concepts as risk assessment and management. 57
As a final point, it is important to acknowledge that the paramedic theory of practice, Campeau's 27 SCTPSM, was instrumental in the comprehension of paramedic OV through its description of social processes and their relationship to scene management practices. While the objective of the study was not to assess the validity of the SCTPSM model, its limitations towards the influence of both the paramedic and the patient on scene management are significant. Though modification of the SCTPSM model is warranted, its discussion is constrained within this space. It is anticipated that further research will address this shortcoming.
Limitations
The utilisation of one-on-one semi-structured interviews as the method of data collection may have resulted in some potential distortion of the data. Participants may have exaggerated some elements of their experience to enhance their inclusion in the study or alternatively they may have altered aspects to defend themselves against any potential unethical or unprofessional accusations. Additionally, the data obtained may have been vulnerable to the assumptions of the authors regarding the management or mitigation of paramedic OV. Last, as the study was focused on the perceptions of paramedics within Australian-based EMS agencies, the findings may not be generalisable to all paramedic systems.
Conclusion
Acknowledgement of the social processes involved in paramedic OV represents a notable shift in the representation of violent and aggressive behaviour during healthcare. Not only does it shift the emphasis away from individual culpability, but it recognises that a bilateral, interactive paramedic–patient relationship is part of this process. Critically, this interaction does not occur in a vacuum and the paramedic–patient relationship must be comprehended within the context of the setting in which it occurs. The implications of these findings should encourage EMS organisations away from reactive OV mitigation strategies and towards interventions that increase paramedic awareness and their ability to engage within dynamic social milieus. This resulting cultural shift could provide not only a more equitably human-centred management regime but could be the medium through which a potential decrease in the elements that aggravate interpersonal violence is made possible.
Footnotes
Declaration of conflicting interests
Author Scott Devenish is a member of the Editorial Board of Paramedicine. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Notes
Correction (October 2025):
In this article, “Declaration of conflicting interests” section has been updated.
Appendix A
How long have you worked as a paramedic? Can you provide a brief description of your work environment? e.g., Metro/rural, high density, low socio-economic. Can you tell me about the OV incident? Was it a patient's home, street, or ambulance? Time of day? Reason for call e.g., assault, illness, drug/alcohol intoxication? How would you describe the initial scene assessment and management of the OV incident? Were there any safety concerns prior to arrival on the scene? Do you believe there was any misinformation (e.g., dispatch) regarding the perpetrator, scene or scene safety? Do you believe there were any elements of safety compromised in order to undertake patient care? Were the police present at the OV incident? If so, how was the communication and management plan between agencies prior to the OV incident? Was the perpetrator(s) identified as a potential threat prior to the OV incident? What de-escalation techniques (if any) were undertaken in order to try and defuse the situation prior to the OV incident? Do you believe there were any internal contributing factors such as stress, fatigue, or hunger that led to the OV incident? Do you believe there were any external contributing factors such as the presence of bystanders or the police that may have led to the OV incident? Do you believe that attempting to distract the perpetrator(s) through techniques such as temporary removal from the scene, or involvement in a patient care capacity could have made a difference to the OV incident? Do you believe that any physical environment manipulation to create a barrier e.g., equipment location or patient care location i.e., airway seat in an ambulance, could have prevented the OV incident? Did you have any warning or sense of danger prior to the OV incident? If so, can you recall any of these? Do you believe that isolation i.e., single response paramedic or distraction i.e., task focus, played a role in the OV incident? If the OV incident occurred as part of a two-person response, do you believe the second officer could have played a greater role in preventing the OV incident? Is there anything else you would like to add or clarify before we finish this interview?