
Abstract
Keywords
Background
The COVID-19 pandemic severely disrupted healthcare systems, making it difficult for patients to access care, including emergency care services. In England, visits to Emergency Departments (EDs) decreased by nearly 50% in April 2020 compared to April 2019. 1 Hospitals admitted fewer patients with severe conditions, such as ST-Elevation Myocardial Infarction (STEMI) 2 and stroke. 3 Furthermore, a survey of 12 ambulance services across the United Kingdom (UK) observed a reduction in the frequency of emergency (999) calls. 4 Simultaneously, two ambulance service trusts reported abrupt increases in the incidence of and deaths from Out-of-Hospital Cardiac Arrest (OHCA).5,6
Ambulance service trusts implemented new measures during the pandemic to protect patients and ambulance staff, including the use of Personal Protective Equipment (PPE) and the release of regular updates on the latest COVID-19 information. 7 These instructions included clinical updates on Aerosol Generating Procedures (AGPs) performed by paramedics, such as endotracheal intubation, 8 which presented a heightened risk of viral transmission. However, these procedural changes introduced operational challenges, requiring all ambulance personnel to adapt in response to the demanding COVID-19 conditions.
Most research to date on OHCA during the pandemic has been quantitative, offering valuable epidemiological insights into incidence, ambulance care processes or survival outcomes.9–12 However, such studies do not take into account the first-hand accounts of paramedics as they deliver life-saving, frontline care amidst unprecedented operational pressures of the pandemic. In the UK, recent qualitative research highlights several challenges encountered by ambulance care personnel during COVID-19, such as the burden of PPE, risk of infection and psychological impacts.13,14 However, these studies explored the experiences across different emergency presentations and did not specifically focus on OHCA – a time-critical, complex emergency condition that poses distinct clinical, operational and ethical challenges for ambulance staff.
For example, Rees et al. interviewed paramedics in Wales during the early waves of the outbreak, raising concerns about crew safety, clinical decision-making and PPE quality – concerns that emerged from broader emergency care contexts, not specifically limited to OHCA. 13 Also, Barrett et al. surveyed UK ambulance staff working in clinical and non-clinical roles, highlighting widespread psychological distress levels and low confidence in their preparedness to use PPE and handle the complexity of the COVID-19 crisis. 14 Coppola et al. offered valuable insights into resuscitative efforts during the pandemic, examining ambulance staff views on communication, procedural changes and perceptions of personal risk. 15 Their sample included a range of prehospital care roles and was conducted in the mid-phase of the pandemic period. Building on this body of research, our study focuses on frontline paramedics and captures their experiences across all waves of the pandemic.
By narrowing the focus to OHCA patients, we aim to offer a more detailed account of how pandemic conditions shaped paramedics’ working practices, mental well-being and perspectives on resuscitation outcomes.
Methodology
Design
This study is an exploratory qualitative study using a critical realist reflexive thematic analysis of semi-structured interviews with UK paramedics. We have prepared this study in accordance with the Reflexive Thematic Analysis Reporting Guidelines (RTARG), which was recently developed by Braun and Clarke (Supplementary Material). 16
Philosophical underpinnings and research paradigm
This study is underpinned by a critical realist approach to reflexive thematic analysis, which holds that reality exists independently of human perception but is only ever imperfectly knowable. Therefore, our understanding of it is mediated by social, cultural and historical factors. 17 Also, it recognises that these experiences and events shared by participants are influenced by deeper mechanisms, including organisational, institutional or societal ones, which may not be directly observable or measurable. For that reason, this study aimed to discover and explore both participants’ experiences and the underlying structural mechanisms behind those experiences.
While the ontological and epistemological philosophical stance is grounded in critical realism, some elements of constructivist-informed thinking are reflected in the use of reflexive thematic analysis.18–21 These include meaning-making, researcher subjectivity and reflexivity, which support and augment, rather than contradict, critical realism's concern with socially constructed knowledge and deeper explanation. These features are seen as analytical resources, not as a separate research paradigm.
Reflexive thematic analysis was selected to explore not just what participants said in the interviews but also why those events occurred, enabling identification of both semantic (descriptive) and latent (deep) codes and themes. This aligns with retroduction, a key feature of critical realist analysis, which infers deeper causal mechanisms. 17
The researcher's clinical background as a paramedic informed the analytic process, in line with reflexive thematic analysis’ emphasis on researcher reflexivity as an analytical strength. 19 This approach supports a flexible and methodologically coherent framework for exploring how paramedics experienced resuscitation and OHCA care during the pandemic and what caused those experiences.
Participants and setting
Frontline UK National Health Service (NHS) paramedics who attended OHCA events during the COVID-19 pandemic were eligible to participate in the study. The aim was to explore UK paramedics’ experiences during the pandemic in order to understand how their prehospital care experiences and resuscitation practices evolved over time in response to changing pandemic circumstances. COVID-19-related health measures – including lockdowns – framed the context of these experiences. Participants’ prehospital experience levels were recorded as Newly Qualified Paramedic (up to 2 years post registration), experienced (2–10 years) and senior (+10 years). These labels or categories were assigned alongside anonymised participant identifiers in all quotes to offer clinical context and help the reader interpret how views may vary by experience level. They were not used as actual paramedic role definitions but as a practical aid to support understanding of individual experiences.
Recruitment
Recruitment started in late September 2022 and ended in March 2023. Participants were recruited by the study's advertisement being posted on X (formerly Twitter) using a bespoke account and through academic networks associated with the research team, including academic and clinical collaborators within the [details omitted for double-blind reviewing]. Potential participants who contacted me (A.A.) and expressed their interest received a participant information leaflet via e-mail. Participants confirmed their willingness to participate by replying to the email and gave verbal consent before the start of the interview.
Sampling
Sampling strategy combined elements of both convenience and purposive methods. 22 Participants were initially recruited through X (formerly Twitter) and via academic networks. Within this convenience sample, purposive selection criteria were then applied to ensure that only frontline UK paramedics with hands-on, direct involvement in resuscitation care following OHCA during the COVID-19 pandemic were included. This approach ensured that participants could offer information-rich and contextually relevant insights into OHCA care under challenging pandemic conditions. Core demographic data collected included age group, gender, years of prehospital experience and academic qualifications, as per the approved ethical protocol. Details on regional location, trust affiliation or formal job role were not formally recorded. However, participants occasionally referred to their roles and locations during interviews, which revealed diversity in operational contexts and geographical settings.
As a medium-sized project, the recommended sample size for this study was up to 20 participants from the UK.23,24 The exact sample size needed for this study was informed by information power, an emerging criterion for qualitative sampling that considers several factors, including sample specificity, quality of dialogue and study aim. 25 In other words, the more data-rich and highly specific the study sample is, the fewer participants are required to provide sufficient data for theme development. As data collection progressed, the study sample yielded substantial information-rich data that is relevant to the study aims. 25 This informed the decision to discontinue data collection.
Dataset generation
One-on-one semi-structured interviews were conducted between September 2022 and July 2023 using a secure videoconferencing platform (Microsoft Teams, Version 1.6.00.12455). The interview guide was informed by the study aims and by published literature on OHCA epidemiology and the impact of COVID-19 and then modified through an iterative practice of conducting two pilot interviews with paramedics (Supplementary Material). We audio-recorded all remote interviews and reviewed the automatically generated Microsoft Teams transcripts for accuracy. Each transcript was given a unique study identification number and a random letter to identify the transcripts. Participants completed a university-based survey form (Qualtrics, Provo, UT; Version September 2022) and provided information on years of ambulance experience, age, gender and academic qualifications.
Data analysis
We conducted a thematic analysis, informed by Braun and Clarke framework.19,26 We also conducted the data analysis via NVivo (Release 1.7.1) by being fully immersed in and familiar with the interview transcripts, and subsequently started coding, assigning labels or descriptions to segments of data that answered the research question. 27 The coding process was inductive. 28 To support the learning of a novice researcher and act as ‘critical friend’, 29 a second researcher (C.H.) independently coded a proportion of the transcripts. In qualitative research, a critical friend is a trusted colleague who provides constructive critique to improve rigor and reflexivity. Later, A.A. met with C.H. in person to discuss and review the initial codes and themes.
Reflexivity and positionality
We used Braun and Clarke's reflexive thematic analysis which does not adhere to a rigid method but instead requires thoughtful and reflexive engagement with the data throughout the analysis.16,19 Codes and themes were actively co-constructed through my ongoing reflection on how my perspectives and assumptions shaped my interpretation and analytical decisions.
My positionality as a practicing paramedic outside the UK, with no managerial role over participants, helped foster an environment of openness and trust during interviews. Because I was not in a position of authority over them, participants likely felt more comfortable sharing their personal accounts and challenging resuscitation scenarios honestly and openly, without concern about judgement or professional repercussions.
C.H. is a co-author who has clinical experience in critical care settings. Our shared professional backgrounds indeed enriched the interpretation and enhanced analytic insights. Although she did not conduct the interviews, C.H. was mindful not to impose her academic authority over my interpretive process. We maintained a reflexive and open dialogue to preserve the independence of my analysis.
Reflexivity was embedded in my iterative engagement with the interview transcripts. Regular team meetings with co-authors who acted as ‘critical friends’, where I reflected on my own interpretations, receiving feedback aimed at deepening and improving analytic insight rather than achieving agreement or consensus. 29
This approach ensured that analytic decisions were critically examined and clearly reported. These practices are in line with RTARG and Braun and Clarke's guidance.
Ethical considerations
The study obtained ethical approval from [specific details pertaining to ethics approvals were omitted to facilitate a blind peer-review]. Informed consent was obtained from study participants, who were frontline paramedics and not patients in this study. Verbal consent was obtained and recorded at the beginning of each interview.
Results
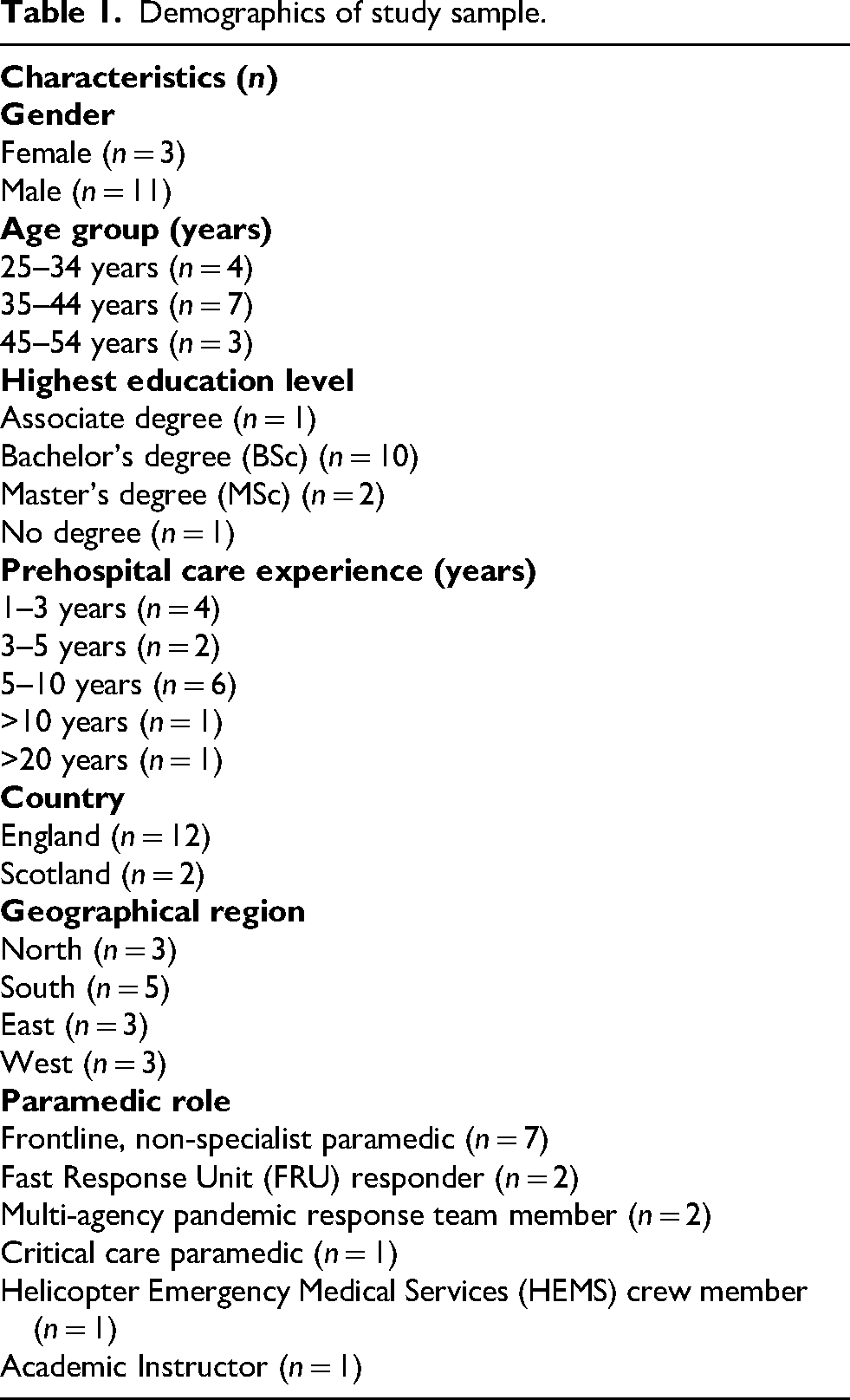
We interviewed fourteen paramedics from Scotland and England, each having responded to and treated OHCAs during the pandemic. The study sample reflected a range of age groups, experience levels and academic qualifications. Moreover, participants’ narratives revealed operational and geographical diversity, with representation from several regions across England and Scotland. However, no data was collected on the specific ambulance trusts participants were affiliated with.
Participants held a range of positions and paramedic roles, including non-specialist paramedics, critical care paramedics, Helicopter Emergency Medical Services provider and members of specialist multi-agency pandemic response teams (Table 1).
Demographics of study sample.
Six paramedics who initially expressed interest were not included in the final study sample: one consented and scheduled an interview but later withdrew (did not attend and did not respond to follow-up); one made contact team after recruitment had closed, and four did not respond to follow-up emails to confirm participation.
After conducting 12 interviews, we achieved sufficient information power. We conducted two additional interviews to confirm this, and data collection was stopped once it was clear that the study sample held adequate information power to address the research question. Participant characteristics, including geographic distribution and roles, are detailed in Table 1.
The mean interview duration was 60 min (range 40–104 min). Seven themes were identified in the analysis of the interview transcripts. The themes were (1) ‘delayed delivery of care’, (2) ‘issues around PPE use’, (3) ‘hindered communication’, (4) ‘dynamic guidelines’, (5) ‘changes in care-seeking behaviour’, (6) ‘heightened psychological distress’ and (7) ‘positive aspects of the pandemic’ (Figure 1).
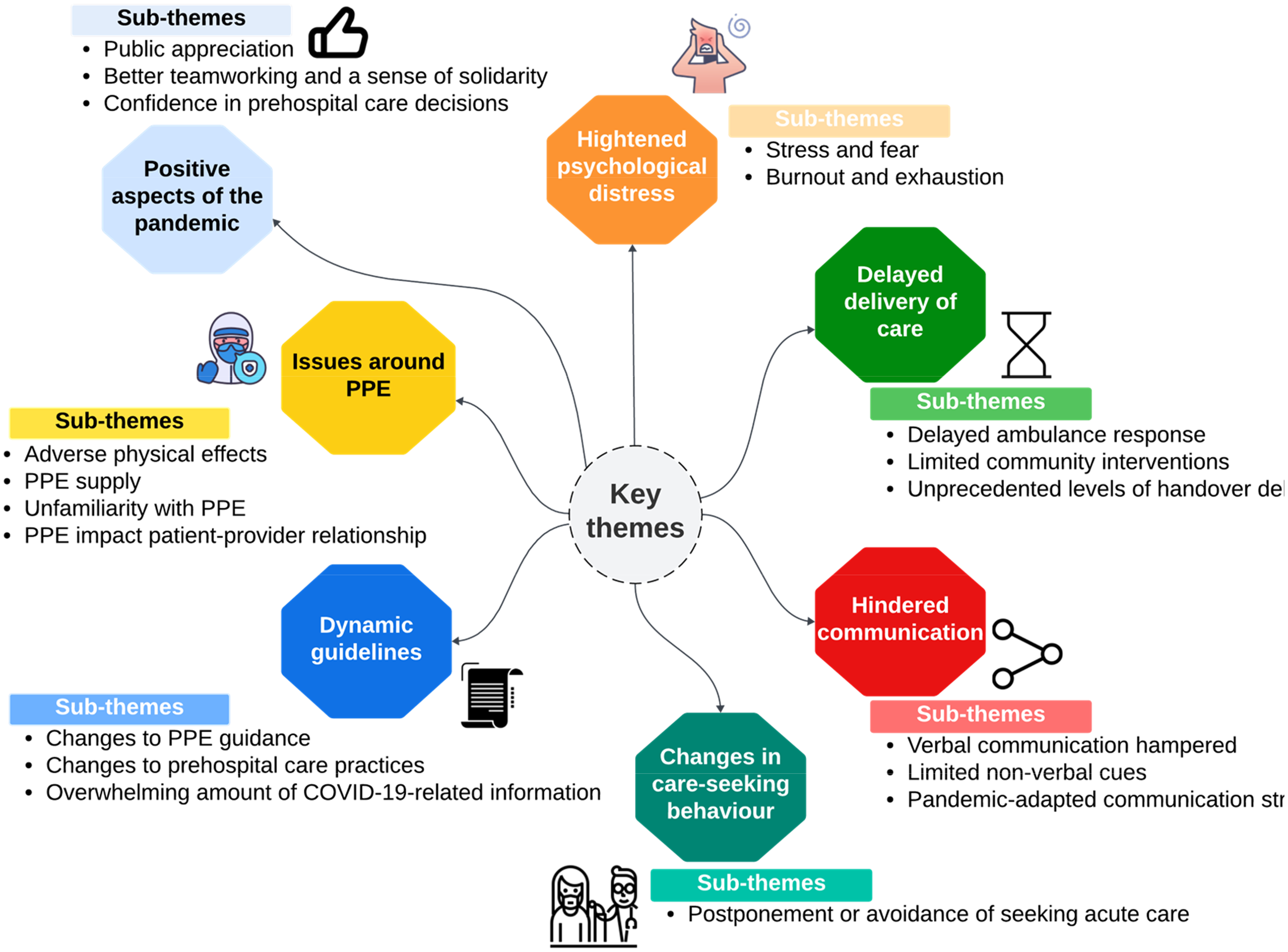
A thematic map illustrating the main themes, sub-themes and supporting codes.
Theme 1: ‘Delayed delivery of care’
All participants reported delays in OHCA patient care delivery during the COVID-19 pandemic, either before being dispatched to the patient, upon arrival at the patient's location, or at the hospital handover. Participants described three key factors behind the delays in OHCA care delivery: delayed ambulance response, limited community response and unprecedented handover delays in the hospital ED.
Sub-theme 1.1: Delayed ambulance response
Participants held differing perspectives regarding the reasons for the delayed ambulance response; however, they collectively agreed that putting on PPE before patient contact was the primary reason OHCA patient care took longer during the pandemic. Some felt that taking additional time to put on protective clothing seemed counterintuitive to how they would typically respond to emergencies: ‘You’re standing there putting masks on and suits and everything, and it goes against our natural instincts. Our instinct is to go towards the problem as soon as we can, and show that we are there and take over, so that a person knows they’ve got help, cos they just want that relief that someone is there, and instead, they can see us there, but not quite with them, and that was difficult.’ (Participant V – senior paramedic)
A few participants described that the delays in wearing different PPE could result in significant harm: ‘The staff wearing the PPE caused delays in patient treatment significantly to the point of the treatment became sort of futile, and we almost met ROLE [Recognition of Life Extinct] criteria by the time that PPE had been put on.’ (Participant Z – experienced paramedic)
Resource issues and staffing shortages and the subsequent increase in paramedics’ workload due to the spread of COVID-19 were amongst the factors that put further strain on ambulance services and disrupted the rapid emergency care response: ‘When you lose so many staff to sickness, you can’t work; you have no resilience in the system.’ (Participant X – experienced paramedic)
Two participants attributed delays to other pandemic-related indirect impacts, such as long wait times for 999 calls to be answered by emergency medical dispatchers: ‘There was another case where a patient was in his 30 s, and it took 11 min to answer the 999-call for a confirmed cardiac arrest.’ (Participant U – experienced paramedic)
Sub-theme 1.2: Limited community response
Participants expressed conflicting opinions regarding the public's willingness to initiate cardiopulmonary resuscitation. Some reported observing bystanders commencing CPR on their family members, whilst several others described some degree of hesitancy to start CPR: ‘A lot of people were arresting in front of their family members, and obviously, you work on your family members. They could be infected with the worst disease, but people would just carry on, whereas, if it was a stranger, you’d be less likely to.’ (Participant R – newly qualified paramedic)
Lockdown, stay-at-home orders, public health messaging and COVID-19 news had possibly created unintended psychological distress which, in turn, altered the way members of the public responded to OHCA events: ‘For example, a bystander CPR for a sort of stranger that's collapsed, people might be reluctant to assist, especially during the height of the pandemic when COVID was seen as almost a death sentence and figures that people were seeing on the television and constant graphs.’ (Participant N – experienced paramedic)
Community First Responders (CFRs) are trained volunteers who provide immediate medical assistance in certain emergencies before the ambulance service arrives. Many participants were unaware that CFRs no longer attended emergency incidents during the pandemic. Many participants perceived such abrupt changes as confusing and unexpected: ‘There were a few jobs I went to where I assumed there would be a CFR on-scene because of where we were, and I was told the CFR wasn’t working.’ (Participant T – experienced paramedic)
Sub-theme 1.3: Unprecedented levels of handover delays at ED
Many participants described ambulance crews waiting outside hospitals or treating patients in hospital corridors waiting for a transfer of care to hospital staff. Such long wait times at hospitals left paramedics dissatisfied: ‘There is nothing more frustrating than sitting at hospital with a patient in the back of your ambulance and hearing a general broadcast on the radio for a cardiac arrest.’ (Participant U – experienced paramedic)
Theme 2: ‘Issues around PPE use’
All participants felt that OHCA care delivery was restricted by the cumbersome nature of PPE. Other concerns included PPE-related adverse physical effects, supply issues and inadequate PPE knowledge. Personal protective equipment affected all aspects of communication and disrupted the patient–provider relationship.
Sub-theme 2.1: Adverse physical effects
Participants experienced varying levels of physical discomfort associated with PPE use, including restricted movement, sweating, breathing difficulty, physical fatigue, restricted peripheral vision and hearing problems. Some raised concerns, such as heat-related issues during the summer or being in confined spaces, which created unsafe working conditions: ‘I had a lot of colleagues faint during cardiac arrest, and we had to keep an eye on each other and say, ‘Right, you go out, go and get some water, take everything off, and then come back.’ It was awful. It was horrible.’ (Participant V – senior paramedic)
Sub-theme 2.2: PPE supply
Issues around PPE supplies and the rationing of PPE stocks at ambulance stations persisted for some time during the first wave of COVID-19, causing several participants to feel worried about their safety and leading to frustration because of how rapidly PPE stocks were depleted: ‘PPE was a challenge in the lack of it, and then having to blue light across [place] to deliver PPE to staff on a cardiac arrest, for example, because there weren’t adequate stocks in certain places.’ (Participant S – experienced paramedic)
One of the participants had other concerns due to the lack of properly fitting PPE, which hindered their ability to perform emergency procedures effectively: ‘So, I am quite short. I would be wearing an extra-large sometimes, so having to try to tweak it up so I am not falling over, making my job three times as hard.’ (Participant V – senior paramedic)
Sub-theme 2.3: PPE impact on provider–patient relationship
Personal protective equipment use also affected social interactions with patients and their relatives during the pandemic. Participants felt that PPE impeded interpersonal connections, and they were therefore unable to effectively build trust and rapport with patients’ loved ones: ‘But they [the family] were freaked out by just our appearance; you know, we’d sort of walked in looking like the bad guys from E.T.’ (Participant T – experienced paramedic)
Sub-theme 2.4: Unfamiliarity with PPE
Although most participants reported receiving some PPE training early in the pandemic, a few participants were unfamiliar with the required level of PPE for emergencies: ‘It was completely foreign, having to use PPE, full stop. I remember my training was: we have this bag, it has stuff in it, it will just go out of date. You don’t need to worry about it. That was it, literally, my training on levels of PPE. It was like, wear a glove; if they’re really minging, wear an apron, and that was it.’ (Participant R – newly qualified paramedic)
Theme 3: ‘Hindered communication’
Personal protective equipment complicated verbal and non-verbal communication both between ambulance crews and family members of OHCA patients and amongst the crew themselves during on-the-scene resuscitation. A few participants developed new communication strategies to improve communication skills and strengthen the patient–provider relationship when wearing PPE.
Sub-theme 3.1: Limited non-verbal cues
Participants frequently reported that interactions with others whilst wearing respirator hoods or suits were extremely difficult because they could not see facial features or read lips, thus heightening relatives’ fears and further complicating communication with other ambulance crews: ‘If you had to lip-read, you can’t do it, and that causes a problem.’ (Participant W – experienced paramedic)
Some participants noted that PPE indeed interrupted non-verbal communication cues, namely, eye contact, body language and facial expressions. Using PPE when delivering patient care on-scene – particularly face masks, respirator hoods or helmets – limited providers’ ability to show care through body language.
One participant reported that they occasionally needed to raise their voice or even shout in order to overcome communication barriers. This was mainly to make up for the loss of non-verbal cues. During resuscitation, the lack of simple gestures such as nodding, smiling and physical touch to family members, combined with restricted vision and muffled voices, caused simple interactions to seem cold and stressful, which amplified emotional distress. ‘There was an awful lot of shouting at some poor, you know, grief-stricken patient or patient's partner because we were all suited up.’ (Participant T – experienced paramedic)
Others struggled to provide physical reassurance to OHCA patients’ families where normally, before the pandemic, to show empathy, they would have held the hand of a family member who had lost a loved one: ‘Also, you know, we are tactile, so I put my hand, you know, I will put my arm around an old lady while I am making her tea because her husband of 80 years is dead. If I am shouting at her and not allowed to touch her, it is really, really, really, difficult.’ (Participant V – senior paramedic)
Sub-theme 3.2: Verbal communication hampered
Personal protective equipment generally obscured facial features, so most participants struggled to speak to, hear or even recognise other ambulance personnel. Face masks and respirators muffled providers’ voices and reduced their speech clarity. Moreover, members of the ambulance service were unable to identify each other because name badges and clinical roles were partially concealed, leading to several instances of miscommunication and creating further delays in resuscitation efforts and scene management: ‘You’d walk in, and you just had five people wearing a white suit and you didn’t know if you had paramedics, you didn’t know if you had doctors, you didn’t know if you had technicians. As a leader, you can’t make decisions about how you’re going to run a scene if you don’t know who you got.’ (Participant P – newly qualified paramedic)
Sub-theme 3.3: Pandemic-adapted communication strategies
As the pandemic continued, a few participants developed creative communication solutions to help establish rapport with patients and relatives and to connect effectively with ambulance personnel. For example, some paramedics wrote their initials or names along with their rank on their protective suit: ‘So, the first things I would do if the arrest was up and running was to ask everyone's name and their grade and write it with a sharpie [permanent marker pen] on their uniform.’ (Participant U – experienced paramedic)
Theme 4: ‘Dynamic guidelines’
Participants experienced rapidly changing working conditions and highlighted frequent policy changes around PPE, termination of resuscitation rules, conveyance decisions and resuscitation protocols.
Sub-theme 4.1: Overwhelming amount of COVID-19-related information
Paramedics felt stressed due to the changing nature of COVID-19 knowledge and the constant updates circulated frequently by ambulance trusts, making it increasingly difficult to keep track of the latest evidence on OHCA and COVID-19: ‘So, there was an enormous information overload, and it was very, very difficult to keep a track of. You generally could do a night shift, go home, go to bed to come back in, and something could change during the day while you were asleep.’ (Participant X – senior paramedic)
Sub-theme 4.2: Changes to PPE guidance
Some participants reported daily or weekly changes in PPE guidance, particularly regarding AGPs, which led to stress, inconsistent work practices and uncertainty: ‘The guidelines were changing so often. You could be on a shift for two days in a row and have totally different guidelines. The evidence-base seemed to be very disputed, especially around intubation and some of the aerosol-generating procedures, which I think caused a lot of anxiety.’ (Participant M – experienced paramedic)
Sub-theme 4.3: Changes to prehospital care practices
Several participants described their decision-making process around resuscitation, transport and ceasing resuscitative efforts becoming more pragmatic, due to how strained ambulance services were, which resulted in altered prehospital care practices: ‘We made more sensible decisions in terms of the greater good for more people rather than just focusing, “I’m with this individual, it's all about this individual, do the best for this person”.’ ‘It was more about thinking common sense here; there's a lot of people that need us.’ (Participant V – senior paramedic)
Theme 5: ‘Changes in care-seeking behaviour’
Participants were concerned about a pattern change in the public's behaviour regarding when to call the ambulance services during the pandemic. Hesitation to call 999, delays in seeking emergency care or complete healthcare avoidance were commonly reported by participants.
Sub-theme 5.1: Postponement or avoidance of seeking acute care
Several participants felt that patients and relatives chose not to seek emergency care or delayed calling an ambulance either to avoid being exposed to the virus or to protect hospitals from being overburdened: ‘He’d been complaining to his wife about a little bit of chest pain that had been niggling him, but he didn’t want to cause a fuss or anything. People were trying to just sort of play the game for the NHS and try not to put any pressure.’ (Participant Y – newly qualified paramedic)
Mixed public health messaging and a perceived risk of contracting the COVID-19 virus in the hospital were amongst the reasons why patients or relatives, in several instances, delayed contacting the ambulance service about or ignored serious symptoms, leading to worsened patient outcomes or even death: ‘He’d had this niggly chest pain all day, but he’d ignored it because he wasn’t going to ruin [person] birthday; it was the first time the family were together. Anyway, obviously, you can predict what happened. It went on, he felt more and more unwell. Family, in the end, called for help. By the time we got there, he was having a massive MI [myocardial infarction]. We took him into hospital, he arrested on the way, and he died. The hospital was very much like, “Well, actually, if we’d got him here this morning, it was just one blocked artery, we could have put a stent in, he’d have still been here”.’ (Participant P – newly qualified paramedic)
Theme 6: ‘Heightened psychological stress’
Most participants reported experiencing several troubling psychological symptoms, including fear, anxiety, fatigue, burnout and mental exhaustion.
Sub-theme 6.1: Stress and fear
Heavy workloads, unpredictable work patterns, staffing issues and media coverage of COVID-19 contributed to heightened stress levels amongst the participants. Contracting COVID-19 and spreading it to family members was the most common fear or worry reported – to the point where some participants decontaminated or removed their uniform before going into their home to protect their loved ones: ‘I know other colleagues who went home and basically stripped and put all of their clothes into essentially a bin bag to go straight into the washing machine when they got home.’ (Participant Z – experienced paramedic) ‘It was stressful for people; not so much the effect on them - it was the effect on their loved ones, like, my mom's poorly.’ (Participant U – experienced paramedic)
Sub-theme 6.2: Burnout and exhaustion
Treatment of and communication with OHCA patients and their relatives whilst wearing PPE took a heavy toll on both the physical and psychological well-being of participants. Many of them faced pandemic-related stressors, such as increased service demand, stringent COVID-19 measures and increased family and caretaking responsibilities; they reported an impact on work–life balance that resulted in them exploring potential alternative careers: ‘It just put a lot of extra stresses, and the stresses outside of work can instantly relate to what's going on in work and have a negative effect. You get into work, you get a cardiac arrest, and that's when you need to be on top of your game, but you’re not…. Because you’re tired, because you had to deal with kids, you had an argument before you left.’ (Participant W – experienced paramedic) ‘Pressures caused some to look for alternative careers, which would say typically primary care or in-hospital jobs. Just because those have got some benefits like predictable finish times and predictable workloads, which we may not have.’ (Participant Z – experienced paramedic)
Theme 7: ‘Positive aspects of the pandemic’
Participants reported some positive aspects during the pandemic, including a sense of solidarity and positive workplace culture within the ambulance service, displays and gestures of public support towards healthcare providers and paramedics and improved confidence in care decision-making.
Sub-theme 7.1: Public appreciation
Many participants felt valued and recognised countless gestures of appreciation from members of the public, boosting participants’ morale: ‘What we found was the generosity of the public was immense. If you didn’t want to prepare food for work, you didn’t have to because there would always be food at the station provided and donated by the public.’ (Participant X – senior paramedic)
Sub-theme 7.2: Better teamworking and sense of solidarity
Despite the increased emotional toll and distress experienced by participants whilst working under pandemic conditions, many found interacting with colleagues at ambulance stations an important source of peer support and camaraderie. Several participants reported being able to help the community and simultaneously socialise at work during lockdown as a privilege: ‘We pulled together as a team when the going got tough, and therefore, together as a team, I think it really helped us grow.’ (Participant M – experienced paramedic) ‘It was a really good chance to mix and socialise with colleagues, chat about the jobs that we’ve been to or debrief, and then recognise that we’re in that sort of privileged position to not be in full lockdown. Obviously, I went home and maintained the guidelines, but I got this escape route to get out and go to my ambulance stations and drive an ambulance all day. It felt like a real positive.’ (Participant Z – experienced paramedic)
Sub-theme 7.3: Confidence in prehospital care decisions
Such difficult circumstances brought about several positives such as resilience and professional growth. Participants collectively reported higher exposure to resuscitation attempts during the pandemic, and that, in turn, significantly improved their resuscitation abilities: ‘I was doing two or three a day sometimes. If you’re exposure is more frequent, you’re slicker: you’re better at it, you’re more efficient. I would say the quality of resuscitation now is better than it was pre-pandemic.’ (Participant V – senior paramedic)
Higher exposure to OHCA resuscitation boosted several participants’ confidence levels and led to greater autonomy in making prehospital on-the-scene decisions, particularly decisions around the termination of resuscitation efforts: ‘I suppose, for us, we develop skills, our ability to remotely assess the futility of cardiac arrest. When we work on the scene or, you know, the decision making you've got, you know you're able to make these decisions and weigh them up in a way that gave you more confidence because you were exposed to so many of these calls, and you did develop some more awareness of it.’ (Participant X – senior paramedic)
Supporting data for all the themes are displayed in Supplementary Material.
Discussion
Principal findings
There were negative impacts on OHCA care delivery and profound impacts on paramedics’ working practices during the pandemic, including delays in prehospital care delivery, PPE-related challenges, ineffective communication and frequent changes to the guidelines, as well as factors contributing to heightened stress and burnout levels.
Despite numerous obstacles hindering resuscitation efforts during COVID-19, treating OHCA patients and working on the frontline resulted in several positive outcomes. Many participants reported instances of public support, camaraderie and strengthened relationships within the ambulance service.
It is important to note the degree of similarity in paramedics’ experiences, specifically regarding PPE usage, communication issues, procedural changes and pandemic-related operational disruptions during OHCA care. These shared experiences emerged clearly through the illustrative quotations and the themes presented in the findings. For instance, emotional distress, fear and PPE challenges were common amongst participants, irrespective of their experience levels or academic qualifications. That said, participants reflected on the resilience of the ambulance services and the overall NHS healthcare systems. Some had a positive outlook and were confident that their ambulance services could enhance their prehospital resources for future outbreaks by drawing on lessons learnt from the COVID-19 crisis. Others acknowledged clear progress in PPE sourcing and prehospital decision-making but adopted a more cautious stance and were concerned about the limited operational resilience of ambulance services to face the surge in service demand; they also stated a number of pre-existing systemic vulnerabilities, such as inadequate staffing and shortages in hospital capacities, which were laid bare by the stressors of the COVID-19 pandemic.
Comparison with existing literature
Our findings highlight profound psychological and emotional impacts on UK paramedics providing OHCA care and resuscitation during the recent pandemic. These experiences are in line with Coppola's findings, 15 who reported significant impact on emotional state and overall well-being amongst ambulance staff, but our study adds depth by showing that prolonged stress made some paramedics consider leaving the entire profession or seeking alternative roles, highlighting workforce retention issues that arose during COVID-19.
Issues and challenges related to PPE were also common. Consistent with Eaton-Williams and Williams, 30 participants voiced concerns over inconsistent and frequently changing PPE guidance, which complicated infection control practices, impaired prehospital decision-making and hindered communication with family members during resuscitative efforts. Supporting this, Aengst et al.31,32 found that PPE muffled providers’ voices, obscured body language and impacted rapport-building – experiences seen and reflected in our findings where PPE limited verbal communication and compromised vision and physical touch. These issues highlight the need for pandemic-adapted PPE kit and innovative communication strategies, such as see-through masks and anti-fogging eye shields. Some paramedics adapted during the pandemic by using armbands or markers on protective suits to improve team communication during stressful resuscitation scenarios.
In line with our findings, a Swedish study noted ambulance nurses’ increased competence over the pandemic but documented physical burden of PPE, especially in warm environments, possibly affecting care delivery. 33 Additionally, recent evidence also suggests that extensive PPE training could enhance frontline workers’ confidence and adherence to guidelines.34,35 Our participants reported difficulties staying up-to-date with evolving COVID-19 evidence, leading to substantial variation in practice and reduced trust in ambulance services. This highlights the importance of clear, pandemic-adapted clinical guidelines to better prepare healthcare workers effectively during stressful pandemic conditions.
Despite widespread public support and camaraderie within the ambulance service, participants reported concerning levels of psychological distress. In Pakistan, frontline workers used various coping strategies such as selective sharing of emergency call details, religious coping and limiting exposure to COVID-19 news. 36 Our findings underscore the critical interaction between peer support, organisation-level well-being resources and individual coping, advocating for holistic approaches to support frontline prehospital providers’ psychological health during global health crises and future pandemics.
Importantly, our study also reveals much less reported positive outcomes: a strong sense of solidarity or unity, increased confidence in prehospital care decisions and improved resuscitation practices resulting from repeated exposure to OHCAs. Such findings reflect a paradox somewhat overlooked – even though COVID-19 put significant psychological and operational burdens on paramedics, it also fostered adaptive resilience and growth. This enriches understanding of paramedic working practices and conditions during COVID-19 by integrating operational, emotional and organisational dimensions. These insights inform practical strategies for ambulance workforce support and future pandemic preparedness.
Strengths and limitations of the study
Participants from different UK ambulance services brought significant expertise to the study, offering recounting experiences and scenarios of OHCA care delivery. The study adds to the limited evidence base of paramedic experiences during the pandemic. The sample included participants with a range of characteristics we purposively selected and with diverse prehospital experiences. Most participants were men, potentially resulting in underrepresentation of female voices in this study.
A major strength of this paper lies in the study's approach to sample adequacy. Guided by Malterud et al.'s concept of information power, the decision to conclude recruitment and data collection after fourteen interviews was based on the specificity of the study aim, the relevance and richness of participants’ narratives, and the depth of the data generated, rather than numerical thresholds. 25
Our findings are situated within the UK ambulance service context and are intended to offer contextually grounded insights. Whilst the findings may be transferable to similar prehospital settings in the UK, they are not intended to be applicable internationally due to differences in ambulance service systems and differing governmental pandemic management strategies. Also, it is possible that the findings may not be transferable to all regions of the UK, as the participants represented many but not all UK ambulance services.
Social media platforms are a promising and emerging avenue for clinical research recruitment. 37 However, it is possible that the views of participants recruited via social media channels differ from those who are not actively engaged in social media.
This study has several methodological limitations that need to be acknowledged. Recruitment was conducted through X, a platform commonly used by UK paramedics and academic researchers, which facilitated access to an engaged audience. However, relying on a single social media platform to recruit participants may have limited reach, possibly excluding those less active online or ones who do not use X. To address this, the study advertisement was also circulated by the research team through various professional networks, which may have helped broaden its reach beyond X platform. The study advertisement included the lead researcher's email, allowing interested individuals to contact the research team directly. Although the study advertisement was posted via X, the study information could have been shared beyond this platform by participants or colleagues, but this cannot be confirmed.
While this paper focused only on paramedics as the population, rather than all frontline ambulance staff, this decision was guided both by pragmatic decisions – such as the need for a well-defined and specific sample within the scope of the study – and by the lead author's experiential knowledge as a practicing paramedic. This professional background offered contextual understanding of paramedic practice during OHCAs, supporting a more focused and allowing a contextually grounded exploration of their care experiences. Although other prehospital care staff, such as emergency medical technicians and emergency care assistants, are integral to OHCA care and play key roles in resuscitation, their exclusion reflects the study's design rather than a judgement about their role. Future research could include a wider range of ambulance care roles to further explore the team-based nature of prehospital resuscitation. Despite these limitations, the findings provide detailed, contextually relevant insights into paramedics’ experiences of OHCA care during the pandemic.
Implications
This study highlights the need for PPE standards and additional training programmes on appropriate PPE practices, incorporating lessons learnt during the pandemic. There is a need to explore or develop pandemic-adapted strategies to protect the ambulance workforce from viral transmission and simultaneously help support effective communication in challenging prehospital emergencies such as OHCA. Moreover, there is a need to better support frontline paramedics and prehospital staff so as to help them engage with available well-being support services, and to potentially develop tailored well-being interventions to help them cope with burnout and symptoms of emotional fatigue.
Conclusion
Our findings suggest a recurrent set of challenges experienced by various frontline prehospital paramedics, irrespective of work setting, clinical grade or experience level. These could be due to systemic vulnerabilities within the ambulance service or barriers associated with the recent global outbreak. Participants’ consistent challenges identified within the ambulance services during the pandemic emphasise the need to protect and prioritise the well-being of frontline prehospital providers, especially under pandemic and extraordinary circumstances; to ensure effective sourcing of and proper training in the use of PPE kits; to adopt creative ways of communication whilst wearing PPE; and to establish robust and reliable communication channels in pandemic settings within the ambulance services. Addressing these issues is vital to enhance and strengthen the resilience of frontline healthcare professionals in delivering high-quality care under extraordinary circumstances. This study contributes to the growing body of literature by offering an in-depth, meaningful exploration of paramedics’ experiences caring for OHCAs during the COVID-19 pandemic, offering valuable insight into the operational realities of prehospital care within a challenging and evolving healthcare landscape. It highlights how changing clinical guidelines, care delays and disrupted communication shaped resuscitation practices on the frontline care pathways. Importantly, the findings also capture positive dimensions of care delivery, including a sense of solidarity and improved resilience. Together, these insights offer a more nuanced understanding of how UK paramedics adapted in challenging COVID-19 times, with clear implications for future emergency planning and workforce support.
Supplemental Material
sj-docx-1-pam-10.1177_27536386251380855 - Supplemental material for Paramedics’ experiences of treating Out-of-Hospital Cardiac Arrest (OHCA) patients during the COVID-19 pandemic in the United Kingdom (UK): A qualitative reflexive thematic analysis
Supplemental material, sj-docx-1-pam-10.1177_27536386251380855 for Paramedics’ experiences of treating Out-of-Hospital Cardiac Arrest (OHCA) patients during the COVID-19 pandemic in the United Kingdom (UK): A qualitative reflexive thematic analysis by Abdulkarim A. Almazrua, Christopher M. Smith, Terry P. Brown and Claire A. Hawkes in Paramedicine
Footnotes
Acknowledgments
The authors would like to acknowledge all study participants, without whom the authors would not have been able to complete and publish this study.
Ethical considerations
The study obtained ethical approval from the University of Warwick's Biomedical and Scientific Research Ethics Committee (BSREC) (Application reference no: BSREC 119/21-22).
Consent to participate and consent for publication
Informed consent was obtained from all study participants to take part in this study and for anonymised quotes to be used in publications, participants were frontline paramedics, and no patients were involved in this study. Verbal consent was obtained and recorded at the beginning of each interview.
Author contribution(s)
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Abdulkarim A. Almazrua is funded by a PhD studentship from King Saud University in Riyadh, Saudi Arabia. Terry P. Brown is employed by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration West Midlands, University of Warwick. Terry P. Brown, Christopher M. Smith and Claire A. Hawkes are investigators for the national Out-of-Hospital Cardiac Arrest (OHCAO) project, which is funded by the British Heart Foundation and Resuscitation Council UK. Christopher M. Smith is a NIHR Clinical Lecturer in Emergency Medicine and has volunteer roles at the Resuscitation Council UK, European Resuscitation Council (ERC) and the International Liaison Committee on Resuscitation (ILCOR). Claire A. Hawkes holds grants from NIHR Health and Social Care Delivery Research (HSDR), Research for Patient Benefit (RfPB) programmes and the Resuscitation Council to conduct other research about OHCA.
Data availability statement
Due to the in-depth nature of the interviews, there is always a risk of identification of participants through contextual detail that exists in such qualitative data (interview transcripts), so they are not made available for public use. For further information, please contact the lead author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.