
Abstract
Introduction
Scientific inquiry is critical in any healthcare profession. 1 It can provide epidemiological information, direction for patient safety efforts, evidence on outcomes of treatment, data on patterns or trends of care, insight into healthcare costs and use, as well as workforce characteristics and behaviour. 2 Research is therefore at the heart of a profession's work to understand itself, progress and evolve, and facilitate the provision of safe and effective patient care.
Paramedicine may be described as:
3
(p.3566) … a domain of practice and health profession that specialises across a range of settings including, but not limited to, emergency and primary care. Paramedics work in a variety of clinical settings such as emergency medical services, ambulance services, hospitals and clinics as well as non-clinical roles, such as education, leadership, public health and research. Paramedics possess complex knowledge and skills, a broad scope of practice and are an essential part of the healthcare system. Depending on location, paramedics may practice under medical direction or independently, often in unscheduled, unpredictable or dynamic settings.
Given that paramedicine is a relatively new profession, scientific inquiry has been described as being in its infancy, however, the past few decades have seen substantial growth in research activity.4,5
In the realm of research, there is a prevalent concern associated with the challenges posed by the expansion of research ecosystems, encompassing issues related to infrastructure, collaboration, funding, and methodological expertise. As research environments grow rapidly, an emerging issue is the potential lack of coordination, cooperation, and collaboration among stakeholders.6,7 This can lead to inefficiencies, redundancy in research efforts, the compartmentalisation of research endeavours, and a notable absence of clear research direction and focus. Furthermore, despite an increase in research activities, the overall significance and potential impact of this research may be constrained due to design limitations stemming from various factors, including inadequate infrastructure, limited methodological expertise, funding shortages, and scalability constraints. 8
One strategy proposed to address these limitations and optimise the production of evidence within a particular discipline involves the development of a national or international research agenda. This approach promotes collaboration among stakeholders both within and outside the discipline to create a comprehensive list of research priorities using consensus-building methods. This strategy has a well-established track record and has been successfully employed in numerous health and medical professions, such as medicine, podiatry, nursing, midwifery, occupational therapy, and physiotherapy.9–14 In the context of paramedicine, similar national or regional research agendas have been developed in various countries/regions over the past two decades, including the United States, the United Kingdom, Europe, Ireland, Canada, and the Netherlands.15–23 However, it's essential to note that while these agendas hold conceptual importance, their actual outcomes and impact remain unclear, with only one of the aforementioned agendas undergoing longitudinal follow-up to assess progress. 23
In an Australian context, the first attempt at determining paramedicine research priorities was made by Tippett et al. 24 using a modified face-to-face conference consensus approach. Over the ensuing two decades, Australian and New Zealand paramedicine has evolved considerably to become a registered health profession with mandated university entry-to-practice education and considerable research capacity. 25 Tertiary paramedicine education programmes are now offered by 20 universities, housing an estimated 161 paramedicine academics of whom approximately 30 have completed Doctoral research training. 25 In 2015, with reference to these two decades of evolution, O’Meara et al. 8 argued again for a national Australasian research agenda and proposed a roadmap to achieving it. Seven years later, the Australasian College of Paramedicine commissioned this present suite of research spanning two components: the identification of barriers and enablers to research in paramedicine; and the creation of a research agenda with associated priorities. The first component investigating barriers and enablers was completed in 2022, 26 the second is described herein.
The primary aim of this prospective research project was to create a stakeholder-informed, consensus-derived paramedicine research agenda for Australia and New Zealand. The secondary aim was to prioritise the research items on the agenda.
Methods
Study design
The Delphi consensus method incorporated methodological guidance proposed by Okoli and Pawlowski. 27 Several consensus methodologies were considered including the nominal group technique (NGT) and RAND/UCLA Appropriateness Method (RAM); a Delphi process with modifications as detailed below was considered most suitable. It allowed for a large number of participants, could be conducted online without geographical limitations, and enabled equity in contributions from the expert panel without dominance by any individual participant. 28 The study was grounded in a constructivist paradigm, acknowledging that the outcomes of a consensus process are a constructed truth, and with a relativist ontological stance, acknowledging there may be multiple truths of which the resultant agenda is but one. The study is reported in adherence to guidance on the Conducting and REporting of DElphi Studies (CREDES) reporting guideline. 29
The study used consensus methodology, consisting of three phases. Phase 1, or the preparatory phase, was a cross-sectional survey of Australian and New Zealand paramedicine stakeholders. One aim of the survey was to generate items from which a provisional list of perceived research priorities could be formed. Although participants of the Delphi process were permitted to propose further agenda items, the separate initial survey to form the initial list of agenda items constituted a modification to the Delphi process. Phase 2 consisted of three online Delphi consensus ‘rounds’ to generate a research agenda. Phase 3, a further modification to a pure Delphi process, consisted of one round of consensus voting to determine the importance and establish priorities amongst the final agenda items. A schematic diagram of the overall process is provided in Figure 1.
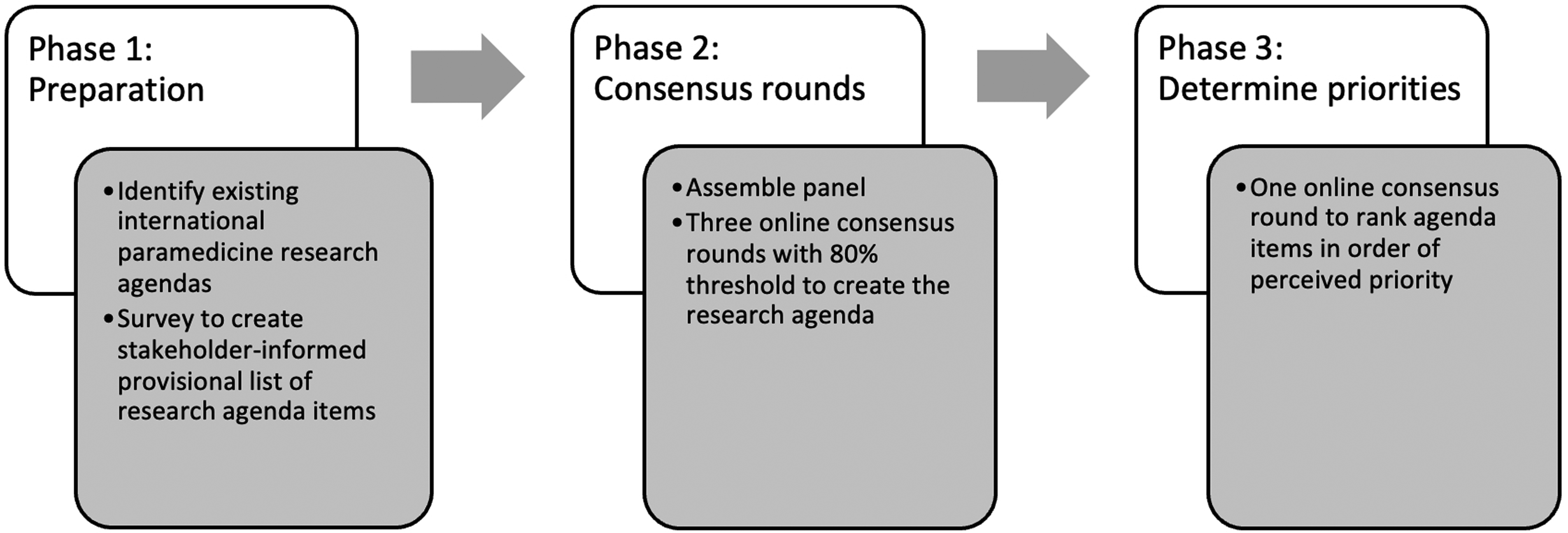
Study design and phase progression.
Setting
The setting was the Australian and New Zealand paramedicine profession. The likeness of the paramedicine systems and profession between these two countries provides an argument for a shared paramedicine research agenda. The Australian and New Zealand paramedicine profession spans the jurisdictional ambulance service sector, the private paramedicine sector, and the tertiary education sector. There are eight state and territory ambulance jurisdictions with monopolised service delivery in each state or territory of Australia, and two ambulance jurisdictions in New Zealand. The vast majority of the estimated 21,000 Australian and New Zealand paramedics are employed in these jurisdictional services, with a small but growing private sector sitting adjacent to it. Some jurisdictions supplement their paid workforce with volunteer ambulance first responders. Australian and New Zealand paramedicine operates an Anglo-American ambulance model, in which degree-qualified paramedics work independently of direct medical oversight. 30 The profession is served by a relatively large tertiary education sector as outlined above.
Phase 1 – Preparatory phase
Study design
The preparatory phase used a cross-sectional study design in which an online survey was used to create a list of research agenda items as perceived by key paramedicine stakeholders. The methodology for the survey has been previously described by Ross et al. 26 An overview is provided here, and further details are available upon request.
Participants
The participants were paramedicine profession stakeholders in any role who engage closely with the paramedicine profession. Participants were eligible if they were from Australia or New Zealand and engaged in the profession as a clinician, educator, manager, or researcher.
Instrumentation and data collection
Data were collected online using the Qualtrics (Qualtrics, Provo UT, USA) survey platform. The data collection period spanned 11 weeks, from 15 November 2021 through to 31 January 2022. The survey instrument was tailored specifically for this study and asked respondents via free text to list their perceived research priorities, as well as barriers and enablers to paramedicine research. There was no limit to the number of priorities able to be listed. The instrument is available in Ross et al. 26
Data analysis
The qualitative open response free text data were analysed using NVivo (QRS International, Doncaster, Australia). A thematic analysis was conducted utilising Braun and Clarke's six-phase approach: data familiarisation, generating initial codes, searching for themes, reviewing themes, defining and naming themes, and producing a report. 31 A more detailed description of the analysis is provided in Ross et al. 26
Phase 2 – Online Delphi rounds
Establishment of the expert panel
Scientific literature provides limited guidance on defining an ‘expert’ for consensus methods,32,33 which presents challenges in fields like paramedicine, where clear standards for expert selection are lacking. 34 The literature outlines essential attributes for identifying experts, including experience, certification, knowledge application, peer recognition, critical thinking, judgment reliability, discrimination ability, and consensus with other experts. 32 We broadly applied these criteria in the selection of our expert panel. We acknowledge the potential for bias with this approach and recognise the possible limitations it may introduce to this study. To mitigate this risk of bias, we applied a three-reviewer selection process as detailed below.
We sought experts from four key stakeholder categories: clinical, education, management, and research. Forming our expert panel followed a three-step approach. First, respondents to the cross-sectional survey were invited to self-nominate if interested. Those who did, provided information about their professional standing in paramedicine and practice area. Two researchers (NB and MT) independently assessed their suitability, with discrepancies resolved through discussions. When consensus was unattainable, a third researcher (PS) was consulted. Second, the research team assembled a list of key individual stakeholders across the four participant categories and targeted these with individual invitations. A provisional panel arising from steps one and two was assembled and analysed for representativeness. The third step involved the targeted recruitment of experts to ensure as much balance as possible in the final panel where imbalances in gender, category of practice, and region of practice had been identified within the panel.
The Delphi consensus process
The consensus process was conducted over three rounds spanning three months between April and June 2022, using the Welphi online survey platform (Welphi, Lisbon, and Portugal). For Round 1 (R1), the expert panel was provided the provisional list of perceived priorities generated in the preparatory phase. They were also provided a package of stimulus material consisting of published paramedicine research agendas from the Netherlands,22,23 the United Kingdom, 17 and Canada. 21 As well as voting for the inclusion or exclusion of items on the provisional list, expert panel members were permitted to add additional items to the provisional agenda list in R1 based on the stimulus material received beforehand or from their own expert experience. Adding items was only permitted in R1.
For each item, panellists were asked to rate agreement regarding inclusion in the agenda using a 5-point Likert scale (Strongly Agree, Agree, Neutral, Disagree, and Strongly Disagree). A five-point scale was chosen over a 3- or 4-point scale for ease of use and to allow panellists to express their feeling adequately. 35 For the purposes of consensus, agreement resulting in inclusion consisted of combining ‘Strongly Agree’ and ‘Agree’. Disagreement, resulting in exclusion, consisted of combining ‘Disagree’ and ‘Strongly Disagree’. Whilst no standardised definition of consensus exists for Delphi studies, 36 a consensus threshold of 80% was adopted in line with most common practice. 29 Items achieving >80% consensus were added to the final agenda and not subjected to further assessment. Those with 80% consensus of non-relevance were removed from the agenda list completely and not subjected to further assessment.
Those for which consensus was not achieved, together with any new items proposed, progressed into the second round of voting (R2). In R2, the process was repeated with the same consensus thresholds applied; those not achieving consensus agreement or disagreement progressed to Round 3 (R3). In R3, this process was repeated. On completion of R3, items yet to reach consensus were examined to explore changes in consensus values between rounds. Those yet to achieve consensus demonstrated no progressive change in the level of agreement, hence a pragmatic decision was made to terminate the consensus due to a low likelihood of consensus value with further rounds.
Phase 3 – Determination of prioritisation and importance
A fourth round of online voting was conducted using Qualtrics (Qualtrics, Seattle, Washington, USA) to establish the importance and prioritisation of items in the research agenda. 37 The final consensus-derived research agenda was sent out to the expert panel who were asked to engage in the prioritisation of items by identifying 10 items they believed were of the most importance. The weight of the importance was calculated by the cumulative scoring of the number of times the research area was included in a panellist's top 10 list. The rank was determined by the cumulative scoring; rank 1 indicated the research area was the most selected item in the panellists’ top 10 list.
Clustering of agenda items
As a final step, the agenda items were sorted into research clusters by one researcher (PS) and verified by the rest of the research team. This was an inductive process, and the purpose of the clusters was purely for presentation and dissemination purposes.
Ethical approvals
The research was designed with alignment to the human research principles of the Helsinki Declaration. Formal ethics approval was sought from and granted by the Western Sydney University Human Research Ethics Committee (HREC Approval Number H14650).
Results
Phase 1 – Cross-sectional survey
There were 341 responses to the survey. The characteristics of respondents have been previously reported by Ross et al. 26 Following thematic analysis, a provisional agenda consisting of 109 perceived research priorities was created for submission to Phase 2.
Constitution of the expert panel
Sixty-three phase 1 survey respondents expressed interest in engaging on the expert panel for phases 2 and 3. Following a review of EOIs including claim to expertise, 34 were deemed eligible. Sixty-four identified experts in Australian and New Zealand paramedicine were concurrently invited to participate in a targeted recruitment, of whom 29 were recruited. Therefore, the final expert panel, drawn from the expressions of interest (EOIs) from Phase 1 and targeted selection, consisted of 63 members. The characteristics of the expert panel are described in Table 1. Despite efforts to ensure balance, the panel had greater representation from Australia compared to New Zealand, and a majority had a primary area of paramedicine practice from the Eastern states of Australia (New South Wales, Queensland, and Victoria). There was good balance across the four key stakeholder groups.
Characteristics of the expert panel (N = 63).
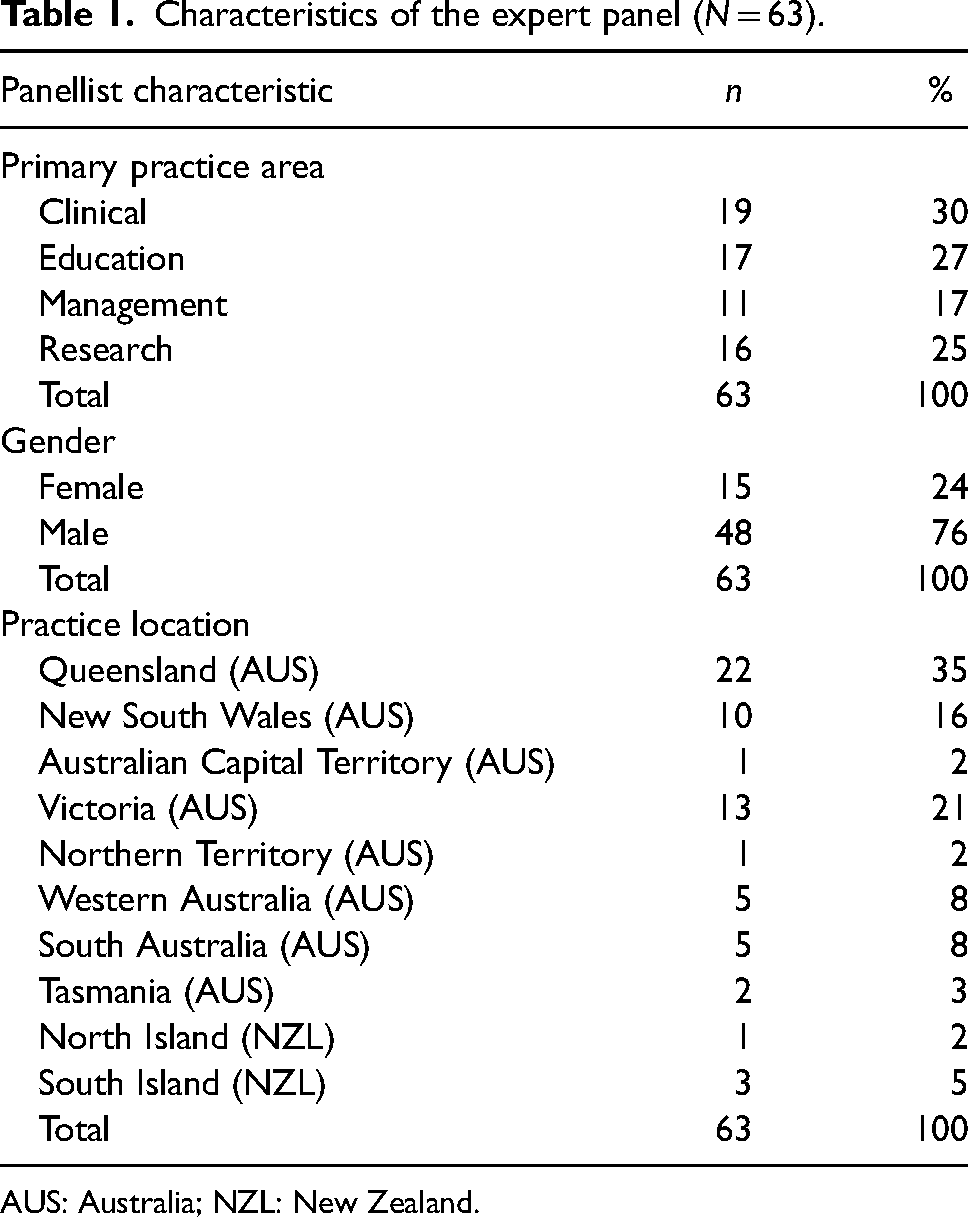
AUS: Australia; NZL: New Zealand.
Consensus results and progression by round
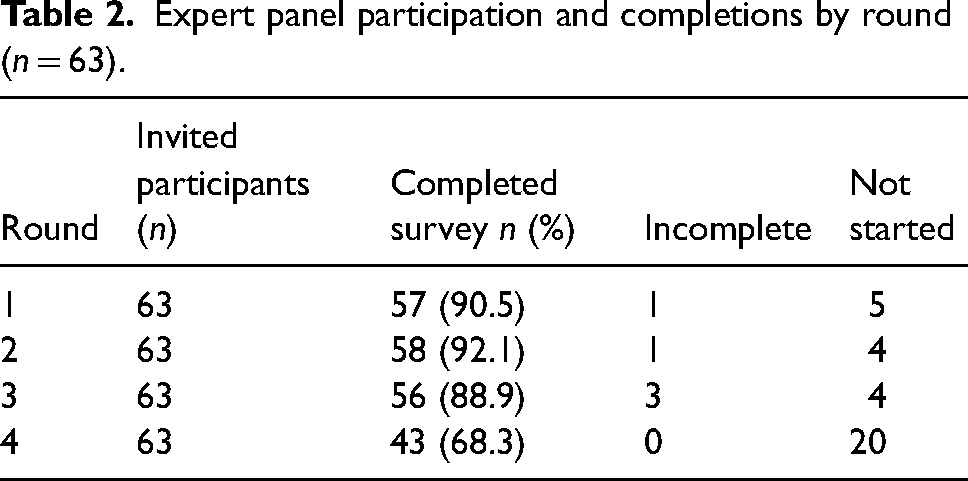
There was high engagement from the expert panel across all rounds (Table 2). Round 1 commenced with 109 research agenda items, of which 18 achieved consensus. Round 2 commenced with 112 items, consisting of 91 non-consensus items carried forward from R1 and 21 additional priorities suggested by panel members. Eleven items achieved consensus. Round 3 commenced with 101 items carried forward from R2. From R3, eight items achieved consensus. The final number of items achieving consensus and constituting the final research agenda was 37. The flow of items and consensus results are illustrated in Figure 2.
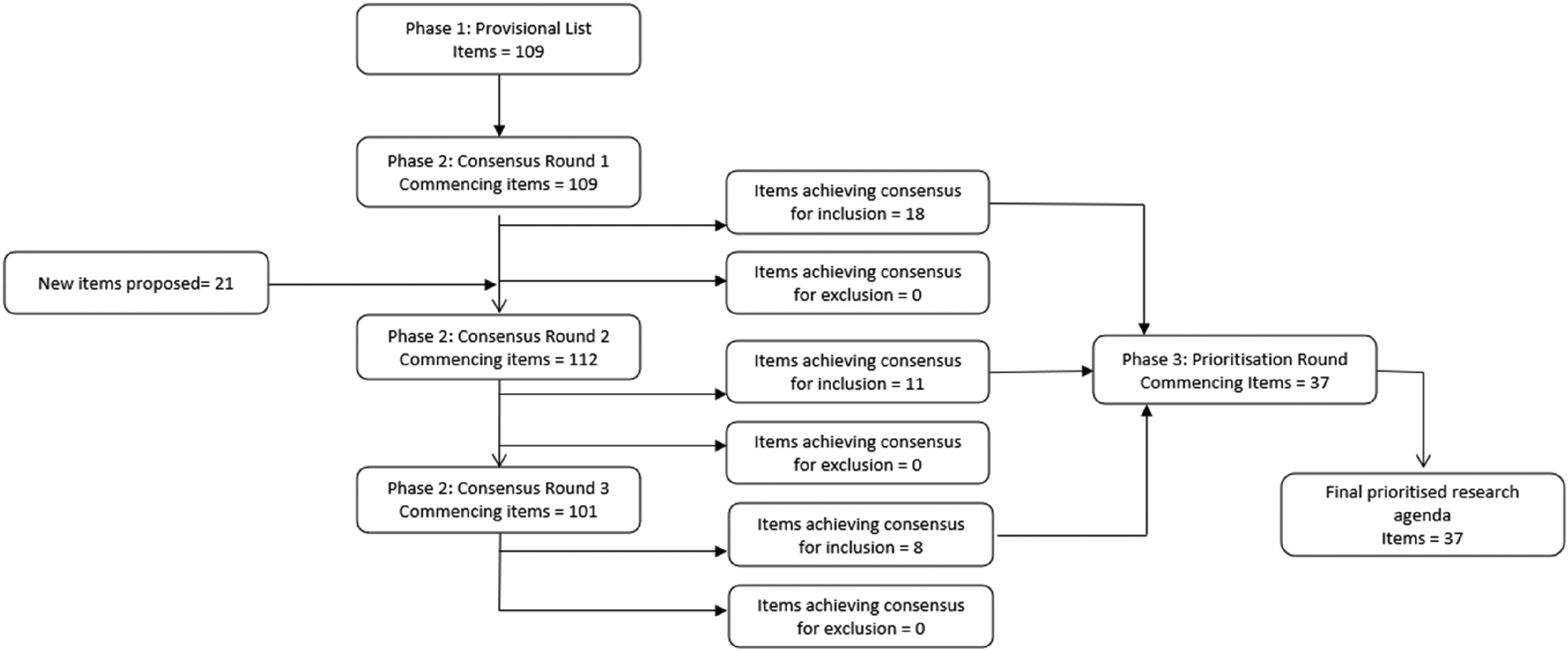
Consensus process item flow.
Expert panel participation and completions by round (n = 63).
Final research agenda and priorities
The final research agenda of 37 items and their order of panel-perceived priority are described in Table 3. These 37 items were sorted into six research clusters to facilitate presentation and dissemination: ‘Safety & Quality’, ‘Systems & Processes’, ‘Expanded Roles and Practice Settings’, ‘Education & Training’, ‘Workplace Culture & Wellness’, and ‘Clinical Pathways & Models of Care’. These clusters are illustrated in Figure 3.
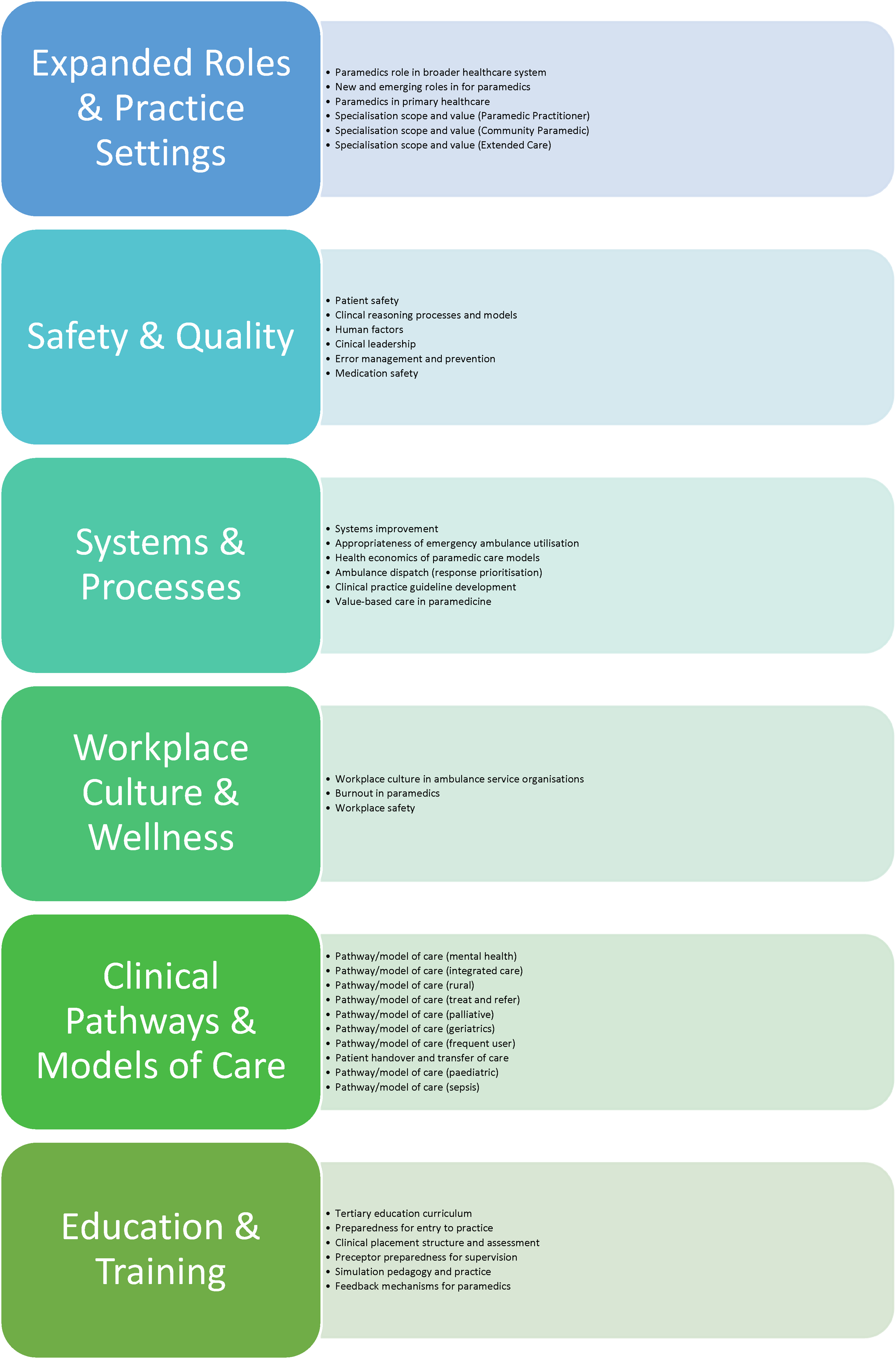
Research agenda items by cluster (clusters and items are not shown in prioritised order).
Priority rank, consensus level, and round achieved.
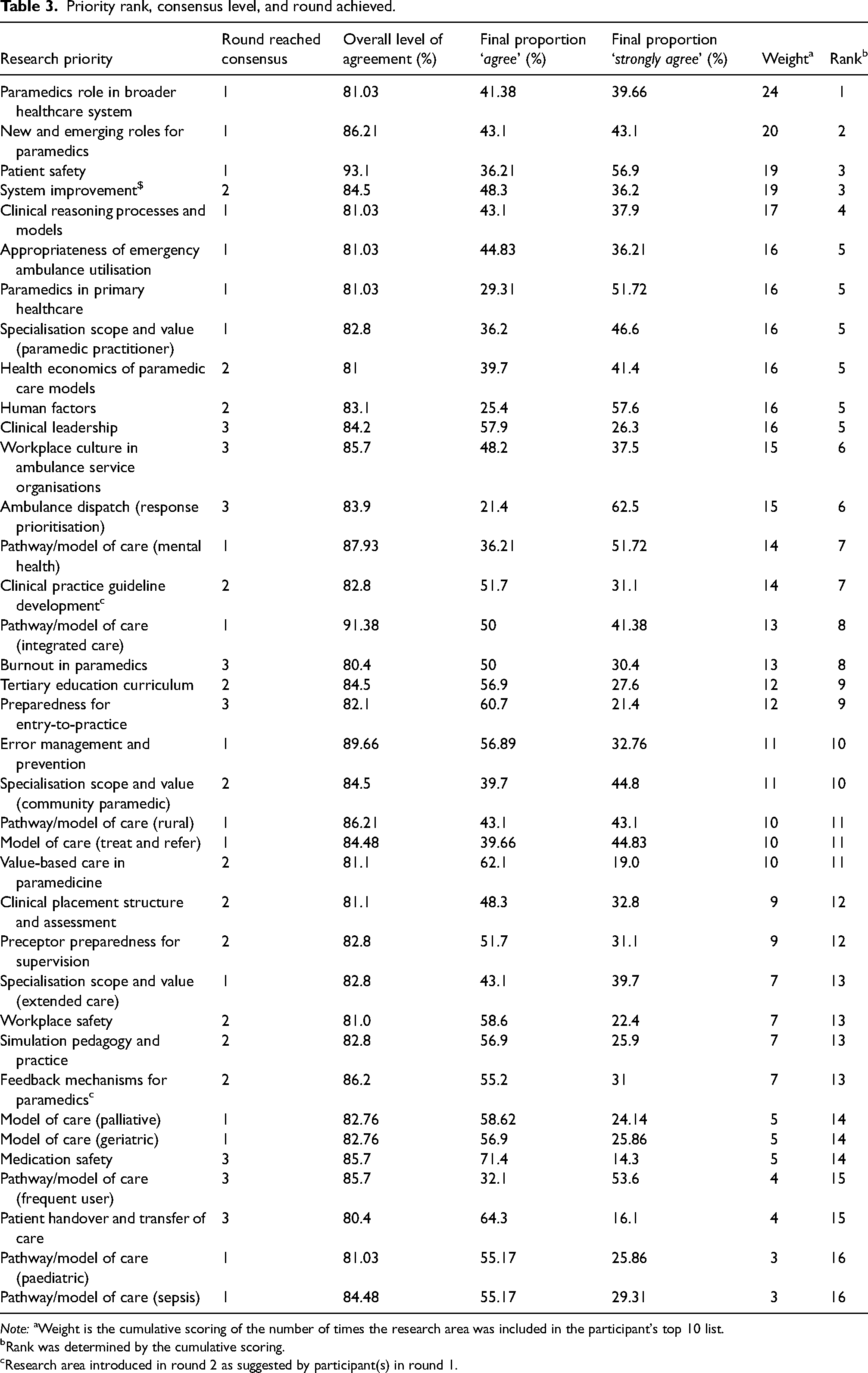
Note: aWeight is the cumulative scoring of the number of times the research area was included in the participant's top 10 list.
Rank was determined by the cumulative scoring.
Research area introduced in round 2 as suggested by participant(s) in round 1.
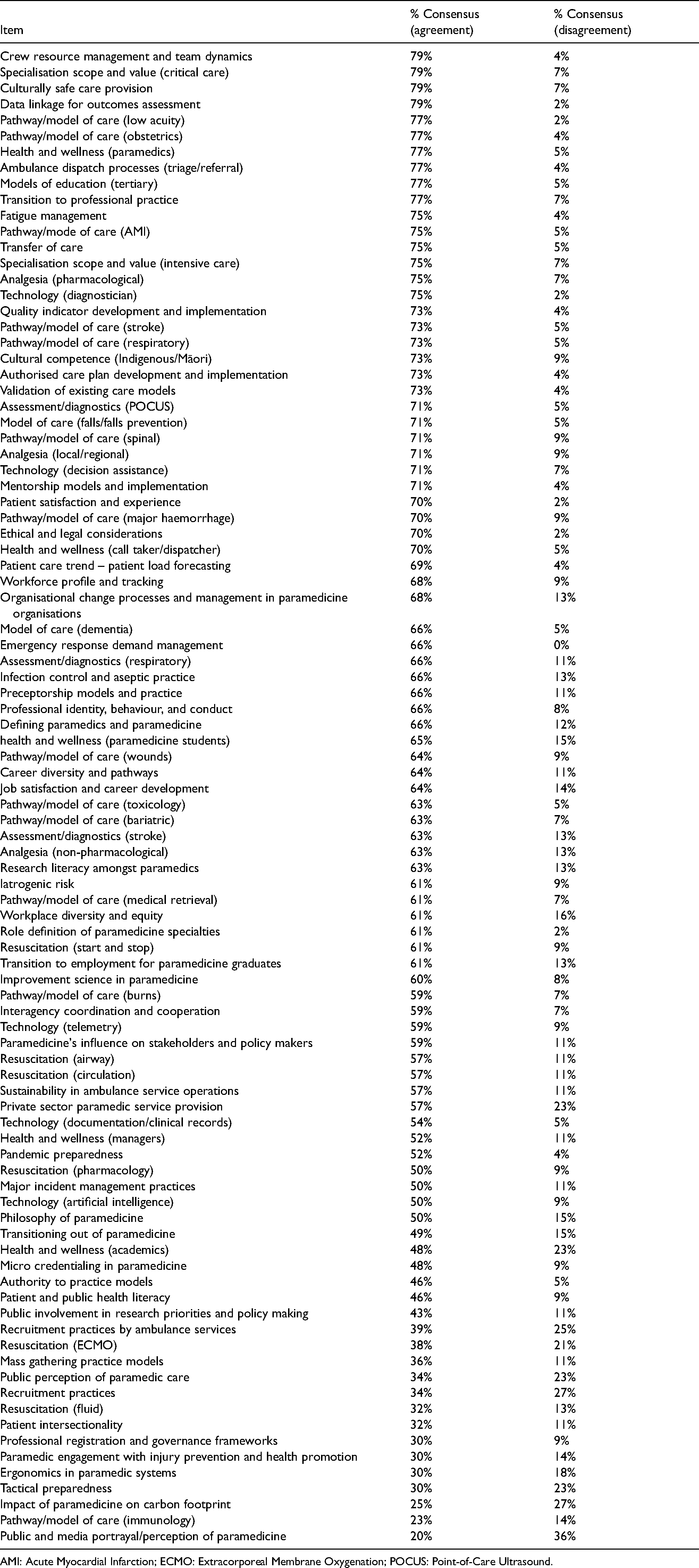
The remaining 93 items that did not achieve consensus are available in Appendix 1.
Discussion
Using consensus methodology informed by a survey of Australian and New Zealand paramedicine stakeholders and a large expert panel, this research proposes a 37-item prioritised research agenda for paramedicine in Australia and New Zealand.
The proposed agenda represents a contemporary roadmap for Australian and New Zealand paramedicine research and comes almost two decades after the first and only other attempt to do so by Tippett et al. 24 In that earlier work, participants at a national Australian research symposium participated in focus groups, the content of which underwent thematic analysis to identify research areas requiring future attention. After a working group was formed, it concluded six months later that defining a national research agenda was beyond its scope. As a result, the outcomes of the project remain undocumented, leaving no means to evaluate the impact of the initiative.
Expanded roles and practice settings
Prominent within the current proposed agenda was a cluster of items (n = 6) relating to expanded roles and emerging practice settings. This result may be reflective of the rapidly evolving nature of Australian and New Zealand paramedicine, triggered initially by its inclusion as a registered health profession in the healthcare practitioner regulation schemes, and more recently the health system and workforce challenges in the post-COVID-19 pandemic era. The potential value and role of paramedics outside of jurisdictional ambulance services are increasingly recognised domestically and internationally, with prominent examples being paramedics in primary healthcare38–41 and new jurisdictional service models such as community paramedicine.42–45 There is clearly a strong appetite for greater examination of paramedics’ role in the broader healthcare system, in or outside of jurisdictional ambulance service organisations, and the impact of these initiatives on systems and patients; 38 this specific item was prioritised first amongst all those on the agenda, and related items featured heavily amongst the top priorities. The result is timely given the Australian Federal Government's apparent intent to include paramedics working at the ‘top of scope of practice’ external to jurisdictional ambulance services in the proposed redesign of primary healthcare infrastructure. 46 It is imperative future research arising from this cluster investigates impact and outcomes; the discipline must not be satisfied simply with change having occurred but seek to substantiate hypotheses of effectiveness and benefit. There are several comparative topics for future study in the Canadian research agenda from 2013, 21 such as ‘the role of the paramedic in various health settings’, ‘role of EMS in health protection and promotion’, and extended scope/community paramedicine programmes. Similarly, the UK agenda addressed ‘managing change resulting from service re-organisation, service development and working across service boundaries in emergency medical services (EMS)’. 17
Safety and quality
With a cluster of six items, safety and quality featured prominently in the final agenda. Comparatively, safety also featured strongly in the Canadian research agenda from 2013 but garnered little attention in that of the Netherlands.22,23 The prominence of patient safety and clinical reasoning items within this cluster may be due to the recent transition to the national profession regulation schemes which are at their core a mechanism for assuring safety. Currently, there appears to be a relatively low volume of research exploring clinical reasoning/decision making in Australian and New Zealand paramedicine. A 2019 narrative review exploring paramedic decision making, judgement and cognitive reasoning identified six research articles, of which only two were of Australasian origin. 47 It has been argued that paramedicine continues to draw heavily from the emergency medicine literature in regard to attempting to understand how paramedics think; the cluster of items identified in this agenda reinforces the need to develop models specific to paramedicine grounded in paramedicine data. 48 Similarly, the need to focus on patient safety in paramedicine was identified by participants in recent work to develop Australian prehospital care quality indicators. 49 Out of the total 526 quality indicators charted in an initial scoping review of that project, only 14 (2.7%) addressed patient safety elements highlighting a need for developing safety-orientated quality indicators. This stood in stark contrast to 75 (14.3%) of the quality indicators describing response times or other time intervals, and 66 (12.5%) relating to aspects of ambulance service deployment. 50
Systems and processes
Most of the six agenda items clustered under ‘Systems and Processes’ were highly prioritised by panellists. Together with ‘patient safety’, ‘system improvement’ ranked third in the prioritised list and arguably encapsulates the other items within the cluster. The high priority placed on this item might indicate the necessity of treating improvement as a distinct science within paramedicine research. Marshall et al. 51 describe the irony that can be found in many healthcare improvement projects whereby the urge to act can easily overwhelm the need for evidence to inform that action and the lack of a scientific approach might result in outcomes that are exactly the opposite of what was intended by the improvement efforts. Emergency ambulance utilisation, health economics, response prioritisation, and clinical practice guideline development are arguably topical issues that require scientific quality improvement efforts to be addressed robustly. A scientific approach through academic and industry collaboration is needed which emphasises innovation, measurement of meaningful performance, and spread through services and systems more broadly to generate learning about what changes produce the intended effects.
Workplace culture and wellness
Paramedic wellness and culture spanned a smaller but important cluster of three items. The broad item ‘workplace safety’ received a priority ranking of equal 13th from 37 items, although it received reasonable research attention in the past decade in a suite of Australian research predominantly by Maguire et al.52–55 Most of that research appears to focus on occupational injury and/or workplace violence, important no doubt, but representing only one area within a broader constellation of concepts falling within the health and wellness space. The other two items within this cluster, ‘Workplace culture in ambulance service organisations’ and ‘Burnout in paramedics’, appear to be unique or at least more explicit in our agenda compared to those of the UK, 17 Canada, 21 and the Netherlands,22,23 although this may be due to the profession holistically becoming more concerned about wellbeing in recent years and our agenda being more current rather than due to any geographical or system differences.
Clinical pathways and models of care
This cluster includes several patient-specific pathways and models of care, defined geographically, demographically, aetiologically, or otherwise. Integrated care and mental health were ranked highly. A recent scoping review of paramedics in integrated models of care 56 found that paramedics are often the link between acute and chronic care, play a key role in case finding within health systems, and can make considerable contributions to public health initiatives. Of the 137 documents included in the review, only eight originated from Australia and two from New Zealand, reiterating the need for research on the features, approaches, and outcomes of integration in pathways and models of care where Australian and New Zealand paramedics are involved. Whilst there are similarities between this cluster and items of all previously mentioned international research agendas, specific attention to the recognition and treatment of sepsis is shared across the Canadian, 21 Dutch,22,23 and our Australian and New Zealand agendas.
Education and training
Finally, and similar to a content area in the Canadian agenda, 21 several included agenda items formed an ‘Education and Training’ cluster. Although well-established in Australia and New Zealand, the tertiary paramedicine education sector continues to be challenged by issues including infrastructure and resourcing, funding, work-integrated learning capacity, research capacity, and sustainability of the paramedicine academic workforce.25,57 Many of this cluster's research agenda items echo these previously identified challenges. Whilst tertiary qualifications are mandatory to acquire paramedic registration with the Australian Health Practitioner Regulation Agency and a requirement for employment with the majority of Australian and New Zealand ambulance jurisdictions, the research agenda items apply not only to university education but equally to paramedic education and training provided elsewhere. The growing demand for ambulance services and healthcare systems places increasing pressure on training provided within ambulance services or other healthcare organisations employing paramedics,58,59 and thus several agenda items in this cluster require equal attention from industry as they do from the tertiary education sector.
The production of an agenda represents a meaningful and tangible visualisation of research priorities as determined by the profession's experts, but it is not in and of itself an endpoint. More accurately, it signifies a beginning, the first step on a path towards a more coordinated, collaborative, and efficient paramedicine research environment in Australia and New Zealand. It is important to highlight that the agenda presented herein is not a mandate and does not seek to lock all paramedicine research into the items within it. Rather, it should serve to promote focus, stimulate discussion, and as a point of reference to help guide researcher and research team decisions on where to allocate their time and effort. It should be a mechanism to promote collaboration and enhance inter-institutional and inter-sector engagement and partnership in pursuit of high-powered collaborations capable of being competitive in funding applications and resource allocations. It does not seek to devalue small local research projects driven by an individual's personal interest or passion; rather it aims to encourage a shift in focus towards, to coin a phrase, the ‘higher hanging fruit’ on the research tree, fruit that is only accessible through greater collaboration and research concentration.
Promotion, dissemination, and profession-wide recognition and adoption of a research agenda is essential to its likelihood to achieve and create impact. A strategic approach to these is essential to ensure the agenda permeates all sectors within the profession, one which should include local and national forums to discuss the agenda and deconstruct each item into clearer research questions and ‘priorities within the priorities’.
Finally, funding bodies within or adjacent to the profession should seek to align grant programmes with the agenda to promote concentration and focus, whilst seeding impetus for greater collaboration and pooling of expertise and resources.
Limitations
These results should be viewed in light of several limitations. First, the cross-sectional survey constituting Phase 1 of the project, from which the initial provisional list of items emerged, attracted a modest response rate and was dominated by responses from Queensland, Victoria, and New South Wales. In one sense, this is reasonable given these are the largest focal points for paramedicine in Australia in terms of the location of practice for registered paramedics. 60 In another, it may represent a lack of input from other jurisdictions in which perceptions of priorities might be different. A specific response rate cannot be determined; whilst the number of registered practitioners in Australia is known, it is not possible to quantify the number of individuals engaged in paramedicine across the stakeholder groups. Similarly, and despite best efforts to ensure proportional balance amongst panellists in phases 2 and 3, several groups were underrepresented. Furthermore, the paradigm of consensus research is relativist and constructionist. It produces one truth in terms of the agenda, and whilst that truth is grounded in the knowledge and expertise of a broad selection of paramedicine experts, it remains possible that other perspectives may not have been captured. However, a robust methodology was used that incorporated contemporary guidance, resulting in a valid product. Response rates of expert panellists across the Delphi process remained high, increasing the validity of the final output.
Conclusion
Using a consensus methodology and drawing from a broad range of stakeholders, a 37-item Australian and New Zealand paramedicine research agenda with item prioritisation has been developed. The items fall within six clusters: ‘Safety & Quality’, ‘Systems & Processes’, ‘Expanded Roles and Practice Settings’, ‘Education & Training’, ‘Workplace Culture & Wellness’, and ‘Clinical Pathways & Models of Care’. These focal areas align with current strategic policy areas facing the profession relating to heath service redesign, expanding scopes of practice, worker health and wellbeing, and systems of care. Engagement with the agenda by industry and other key stakeholders may lead to greater collaboration, enhanced cooperation, increased research efficiency, and production of research capable of meaningful and tangible impact.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Paul Simpson is the Editor in Chief at Paramedicine, and at the time of this research a member of the Australasian College of Paramedicine National Research Advisory Committee. Robin Pap is Chair of the Australasian College of Paramedicine National Research Advisory Committee and an Associate Editor at Paramedicine. Louise Reynolds, Nigel Barr, and Linda Ross are members of the Australasian College of Paramedicine National Research Advisory Committee and are Associate Editors at Paramedicine. None of these authors played any role in the double-blinded peer review or editorial decision-making relating to this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Australasian College of Paramedicine (grant number NA).
Appendix 1. Non-consensus items
| Item | % Consensus (agreement) | % Consensus (disagreement) |
|---|---|---|
| Crew resource management and team dynamics | 79% | 4% |
| Specialisation scope and value (critical care) | 79% | 7% |
| Culturally safe care provision | 79% | 7% |
| Data linkage for outcomes assessment | 79% | 2% |
| Pathway/model of care (low acuity) | 77% | 2% |
| Pathway/model of care (obstetrics) | 77% | 4% |
| Health and wellness (paramedics) | 77% | 5% |
| Ambulance dispatch processes (triage/referral) | 77% | 4% |
| Models of education (tertiary) | 77% | 5% |
| Transition to professional practice | 77% | 7% |
| Fatigue management | 75% | 4% |
| Pathway/mode of care (AMI) | 75% | 5% |
| Transfer of care | 75% | 5% |
| Specialisation scope and value (intensive care) | 75% | 7% |
| Analgesia (pharmacological) | 75% | 7% |
| Technology (diagnostician) | 75% | 2% |
| Quality indicator development and implementation | 73% | 4% |
| Pathway/model of care (stroke) | 73% | 5% |
| Pathway/model of care (respiratory) | 73% | 5% |
| Cultural competence (Indigenous/Māori) | 73% | 9% |
| Authorised care plan development and implementation | 73% | 4% |
| Validation of existing care models | 73% | 4% |
| Assessment/diagnostics (POCUS) | 71% | 5% |
| Model of care (falls/falls prevention) | 71% | 5% |
| Pathway/model of care (spinal) | 71% | 9% |
| Analgesia (local/regional) | 71% | 9% |
| Technology (decision assistance) | 71% | 7% |
| Mentorship models and implementation | 71% | 4% |
| Patient satisfaction and experience | 70% | 2% |
| Pathway/model of care (major haemorrhage) | 70% | 9% |
| Ethical and legal considerations | 70% | 2% |
| Health and wellness (call taker/dispatcher) | 70% | 5% |
| Patient care trend – patient load forecasting | 69% | 4% |
| Workforce profile and tracking | 68% | 9% |
| Organisational change processes and management in paramedicine organisations | 68% | 13% |
| Model of care (dementia) | 66% | 5% |
| Emergency response demand management | 66% | 0% |
| Assessment/diagnostics (respiratory) | 66% | 11% |
| Infection control and aseptic practice | 66% | 13% |
| Preceptorship models and practice | 66% | 11% |
| Professional identity, behaviour, and conduct | 66% | 8% |
| Defining paramedics and paramedicine | 66% | 12% |
| health and wellness (paramedicine students) | 65% | 15% |
| Pathway/model of care (wounds) | 64% | 9% |
| Career diversity and pathways | 64% | 11% |
| Job satisfaction and career development | 64% | 14% |
| Pathway/model of care (toxicology) | 63% | 5% |
| Pathway/model of care (bariatric) | 63% | 7% |
| Assessment/diagnostics (stroke) | 63% | 13% |
| Analgesia (non-pharmacological) | 63% | 13% |
| Research literacy amongst paramedics | 63% | 13% |
| Iatrogenic risk | 61% | 9% |
| Pathway/model of care (medical retrieval) | 61% | 7% |
| Workplace diversity and equity | 61% | 16% |
| Role definition of paramedicine specialties | 61% | 2% |
| Resuscitation (start and stop) | 61% | 9% |
| Transition to employment for paramedicine graduates | 61% | 13% |
| Improvement science in paramedicine | 60% | 8% |
| Pathway/model of care (burns) | 59% | 7% |
| Interagency coordination and cooperation | 59% | 7% |
| Technology (telemetry) | 59% | 9% |
| Paramedicine's influence on stakeholders and policy makers | 59% | 11% |
| Resuscitation (airway) | 57% | 11% |
| Resuscitation (circulation) | 57% | 11% |
| Sustainability in ambulance service operations | 57% | 11% |
| Private sector paramedic service provision | 57% | 23% |
| Technology (documentation/clinical records) | 54% | 5% |
| Health and wellness (managers) | 52% | 11% |
| Pandemic preparedness | 52% | 4% |
| Resuscitation (pharmacology) | 50% | 9% |
| Major incident management practices | 50% | 11% |
| Technology (artificial intelligence) | 50% | 9% |
| Philosophy of paramedicine | 50% | 15% |
| Transitioning out of paramedicine | 49% | 15% |
| Health and wellness (academics) | 48% | 23% |
| Micro credentialing in paramedicine | 48% | 9% |
| Authority to practice models | 46% | 5% |
| Patient and public health literacy | 46% | 9% |
| Public involvement in research priorities and policy making | 43% | 11% |
| Recruitment practices by ambulance services | 39% | 25% |
| Resuscitation (ECMO) | 38% | 21% |
| Mass gathering practice models | 36% | 11% |
| Public perception of paramedic care | 34% | 23% |
| Recruitment practices | 34% | 27% |
| Resuscitation (fluid) | 32% | 13% |
| Patient intersectionality | 32% | 11% |
| Professional registration and governance frameworks | 30% | 9% |
| Paramedic engagement with injury prevention and health promotion | 30% | 14% |
| Ergonomics in paramedic systems | 30% | 18% |
| Tactical preparedness | 30% | 23% |
| Impact of paramedicine on carbon footprint | 25% | 27% |
| Pathway/model of care (immunology) | 23% | 14% |
| Public and media portrayal/perception of paramedicine | 20% | 36% |
AMI: Acute Myocardial Infarction; ECMO: Extracorporeal Membrane Oxygenation; POCUS: Point-of-Care Ultrasound.