
Abstract
Introduction
Historically, Emergency Medical Service (EMS) systems have optimised the response to patients already in out-of-hospital cardiac arrest (OHCA) when the EMS call is made over patients at imminent risk of OHCA. 1 Research investigating recognition of patients already in OHCA before the EMS call is connected has mainly focused on barriers to recognition of OHCA and dispatch protocols. 2 The main barrier to a call-takers’ recognition of OHCA has been found to be breathing status assessment, 2 with an additional barrier to recognition found to be the caller's emotional status. 3 Enablers to OHCA recognition are a calm caller, call-taker communication skill and the implementation of a dispatch protocol. 2 Recent research has investigated key indicator symptoms of patients in OHCA and concluded that changes to the dispatch protocol would result in too many false positives and that instead the focus should be on call-taker adherence to the dispatch protocols. 4 Machine learning models focusing on OHCA recognition have been investigated, but to date have not shown improvement in performance in real world practice. 5 In the recent literature qualitative linguistic analysis has shown promise in understanding how call-takers and communication training and strategies could improve OHCA recognition. 6
Where patients suffer an OHCA, for each second perfusion is absent the probability of a good outcome diminishes. 7 Of equal importance to those who have already suffered an OHCA, and with a better chance of survival with a good neurological outcome, are those patients who are at high risk of OHCA who would benefit from early intervention. The European Resuscitation Council (ERC) Guidelines 2021 8 and the Chain of Survival in OHCA identify the importance of the recognition, during the EMS call, of patients who are at imminent risk of OHCA so that EMS staff can be dispatched to arrive as quickly as possible to either treat the cardiac arrest as soon as it occurs or, better still, prevent it from happening through the provision of early treatment. 4
The ERC Guidelines 2021 8 specifically reference prodromal symptoms and specify the importance of recognising chest pain of a cardiac origin and myocardial ischaemia before a patient collapses to allow EMS to arrive quickly and improve survival. EMS witnessed OHCA are a select group of patients who suffer an OHCA after the EMS call and provide a good opportunity to understand any warning symptoms that proceed the OHCA. Common prodromal symptoms have been reported to be dyspnoea, chest pain, syncope and gastrointestinal symptoms. 9
Our previous research has identified that there is limited research addressing the challenge of call-taker recognition of patients who are alive when the EMS call is initiated, but who subsequently deteriorate and suffer an OHCA. 10 There is limited knowledge of the epidemiology of patients who suffer an OHCA after the EMS call is connected, and little is understood concerning the recognition and response to this patient group and how it can be improved. The aim of this descriptive retrospective data analysis was to understand the current EMS call triage, EMS response and survival of patients who suffer an OHCA after the EMS call.
Methods
Study design
We report a descriptive retrospective data analysis of EMS calls where the patient suffers an OHCA after the EMS call is connected to understand the EMS call triage, EMS response and survival of this patient group.
Setting
This study was completed in a United Kingdom (UK) National Health Service (NHS) EMS provider. This EMS provider serves a population of 5.5 million people across 10,000 square miles 11 and provides an Advanced Life Support response. In this setting, Medical Priority Dispatch System (MPDS) 12 is used in EMS call triage. EMS calls are triaged by a non-clinically trained call-taker with clinical support available and categorised as Category 1–5. A Category 1 is for time critical life-threatening events and has an average response time target of 7 min. A Category 4 is less urgent with a 90th percentile response target of 3 h 13 and Category 5 is triaged by a health care professional.
Data sources
Data included two years of local OHCA cardiac arrest registry data, 1st January 2018 to 31st December 2019, linked to computer aided dispatch (CAD) data. The OHCA registry data included every patient attended where the patient suffered an OHCA and resuscitation was attempted by EMS staff. National Health Service Hospital Trusts reliably report the survival status of all OHCA patients to ambulance services for the purposes of national reporting. The survival status is recorded in the EMS OHCA registry by an ambulance service data officer. Data was cleaned and coded in Excel 14 before import into IBM SPSS 26. 15
Participants
Patients aged 18 years and over who had suffered an OHCA of any cause were included for analysis. Patients were excluded from the analysis if the time of the OHCA was not recorded.
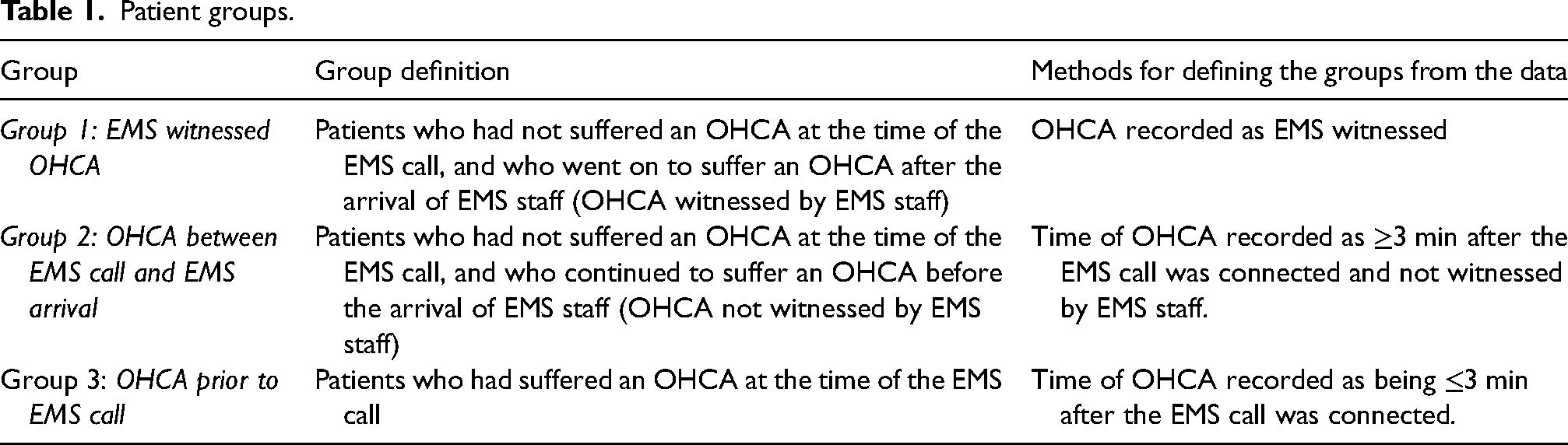
Patients were allocated into three main groups: Group 1 (G1) EMS witnessed OHCA; Group 2 (G2) OHCA between EMS call and EMS arrival and Group 3 (G3) already suffered an OHCA at the time of the EMS call. Group categorisation was determined using the time of OHCA recorded by attending EMS personnel. The groups are further detailed in Table 1.
Patient groups.
Bias
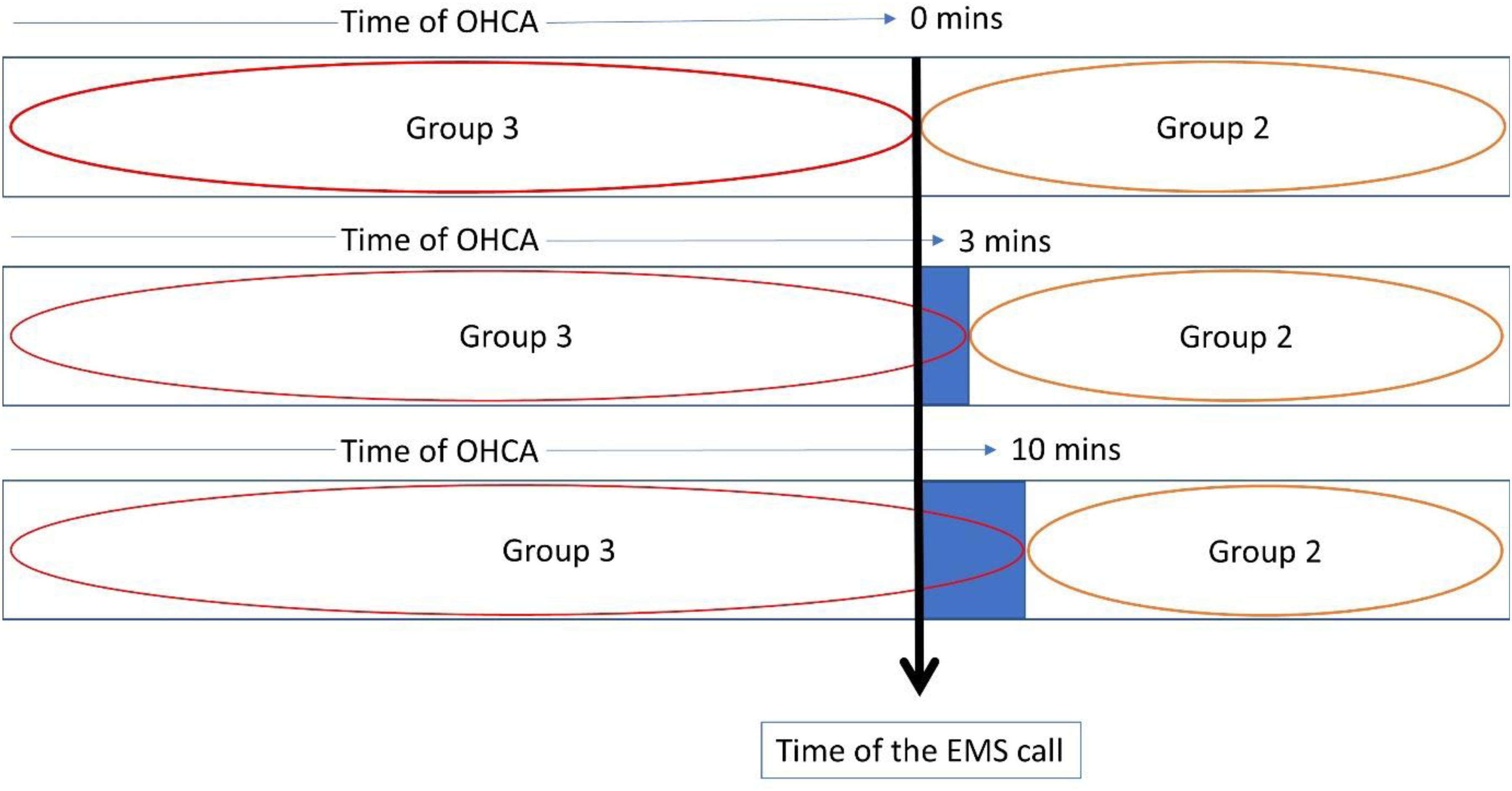
Allocation of patients into groups was determined by the time of OHCA and whether the OHCA was EMS witnessed. This data is recorded on the electronic clinical record by attending EMS staff. As the time of OHCA is not always accurately recorded, where a patient's OHCA was unwitnessed by EMS, patients who had a time of OHCA greater than three minutes after the EMS call connected were labelled as not in OHCA at the time of the EMS call and patients who had a time of OHCA recorded as less than three minutes after the EMS call was connected were grouped as having suffered an OHCA at the time of the EMS call. The cut-off time of three minutes was chosen because it was judged to have the best chance of allocating patients to the right groups, but also because under “dispatch on disposition” which was introduced during the English Ambulance Response Programme (ARP) and allowed call-takers extra time to ask questions before deciding the appropriate response, it was the maximum time between call connect and response time clock start. 16
Quantitative variables
The data fields extracted from the local EMS OHCA registry and the CAD and imported into SPSS are detailed in Supplementary Table 1.
Statistical methods
Descriptive statistics including mean, median and interquartile range for continuous data and percentages for categorial data are reported. An omnibus chi-square test of association was used to assess whether a factor varies with EMS Group (giving rise to one p-value per factor). Sensitivity of conclusions relative to missing data is reported. In these analyses, patients who suffered their OHCA after the EMS call were compared with patients who were in OHCA at the time of the EMS call. Analysis investigated patient variables, OHCA characteristics, OHCA outcomes and EMS process.
Sensitivity power calculations indicate that under a worst-case scenario, the achieved sample sizes have 80% power to detect an 8-percentage point difference between Group 1 and Group 2, 90% power to detect an 8-percentage point difference between Group 2 and Group 3, and 99% power to detect an 8-percentage point difference between Group 1 and Group 3. Under the same scenario, 80% power is afforded, for an 8-percentage point difference between Group 1 and Group 2, a 7-percentage point difference between Group 2 and Group 3, and a 5-percentage point difference between Group 1 and Group 3.
Sensitivity analysis
The 3-min time point cut off in relation to the timing of the OHCA affected patients who suffered their OHCA between EMS call and EMS arrival (G2) and patients who had suffered an OHCA at the time of the EMS call (G3). A sensitivity analyses tested the robustness of the findings in these groups. In addition to the 3-min time point, analyses were completed where the time of OHCA was ≥0 min and ≥10 min after the time of the EMS call, and this is illustrated in Figure 1. The sensitivity analyses were applied to test the robustness of findings where there was not a large difference between the groups.
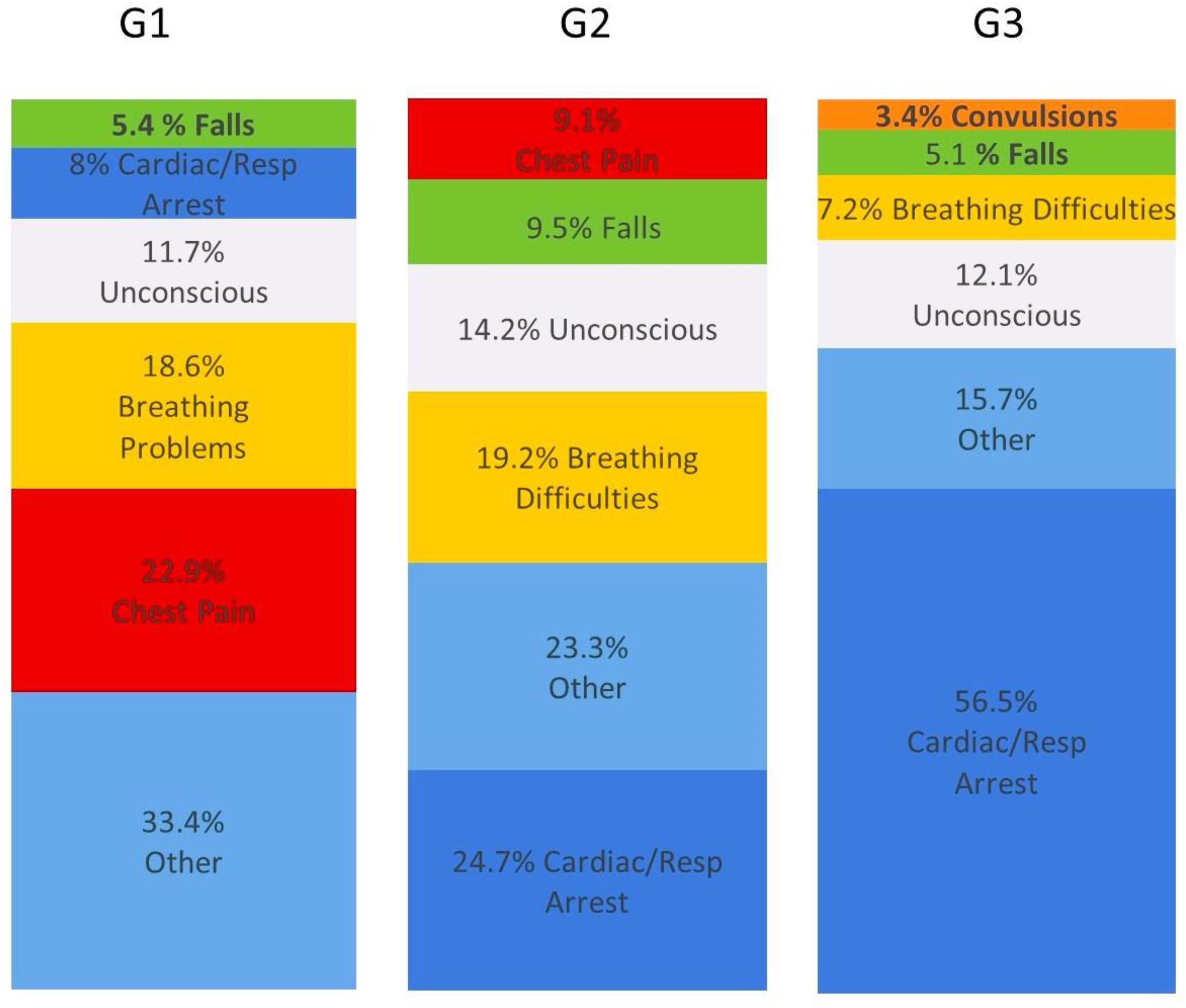
Most common initial MPDS category cards for G1,G2 and G3 . “Other” is a combination of AMPDS codes appearing in small quantities
Ethics approval
For this retrospective study, using routinely collected and fully anonymised data, research ethics committee approval to complete the study without informed patient consent was received from the University of the West of England (UWE REC REF No: HAS.20.05.182). We also contacted the NHS Health Research Authority, which indicated that additional NHS Research Ethics Committee approval was not required in this case. All methods were performed in accordance with the relevant guidelines and regulations.
Results
Participants
There were 7302 patients aged 18 or over resuscitated by EMS during the data reporting period. There were 3057 (41.9%) patients with no recorded time of OHCA that were excluded from the study leaving 4245 patients included in the analyses.
Descriptive data
The number of patients allocated to each group and patient characteristics are detailed in Table 2.
Patient grouping and descriptive data. P-values are for the omnibus association between each OHCA characteristic and OHCA group.
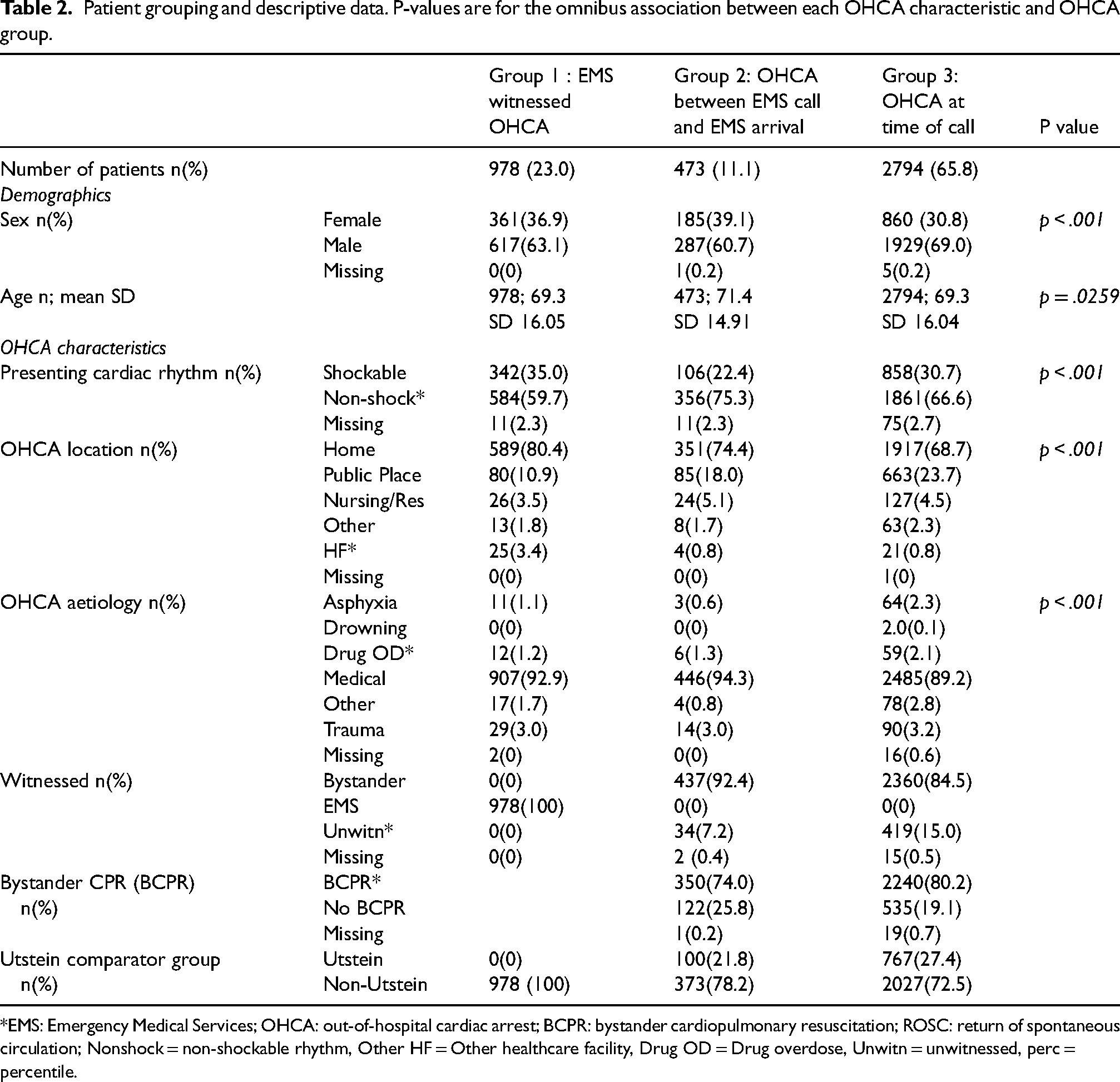
*EMS: Emergency Medical Services; OHCA: out-of-hospital cardiac arrest; BCPR: bystander cardiopulmonary resuscitation; ROSC: return of spontaneous circulation; Nonshock = non-shockable rhythm, Other HF = Other healthcare facility, Drug OD = Drug overdose, Unwitn = unwitnessed, perc = percentile.
Outcome data
Outcome data is detailed in Table 3.
Outcome data. P-values are for the omnibus association between each outcome and OHCA group.
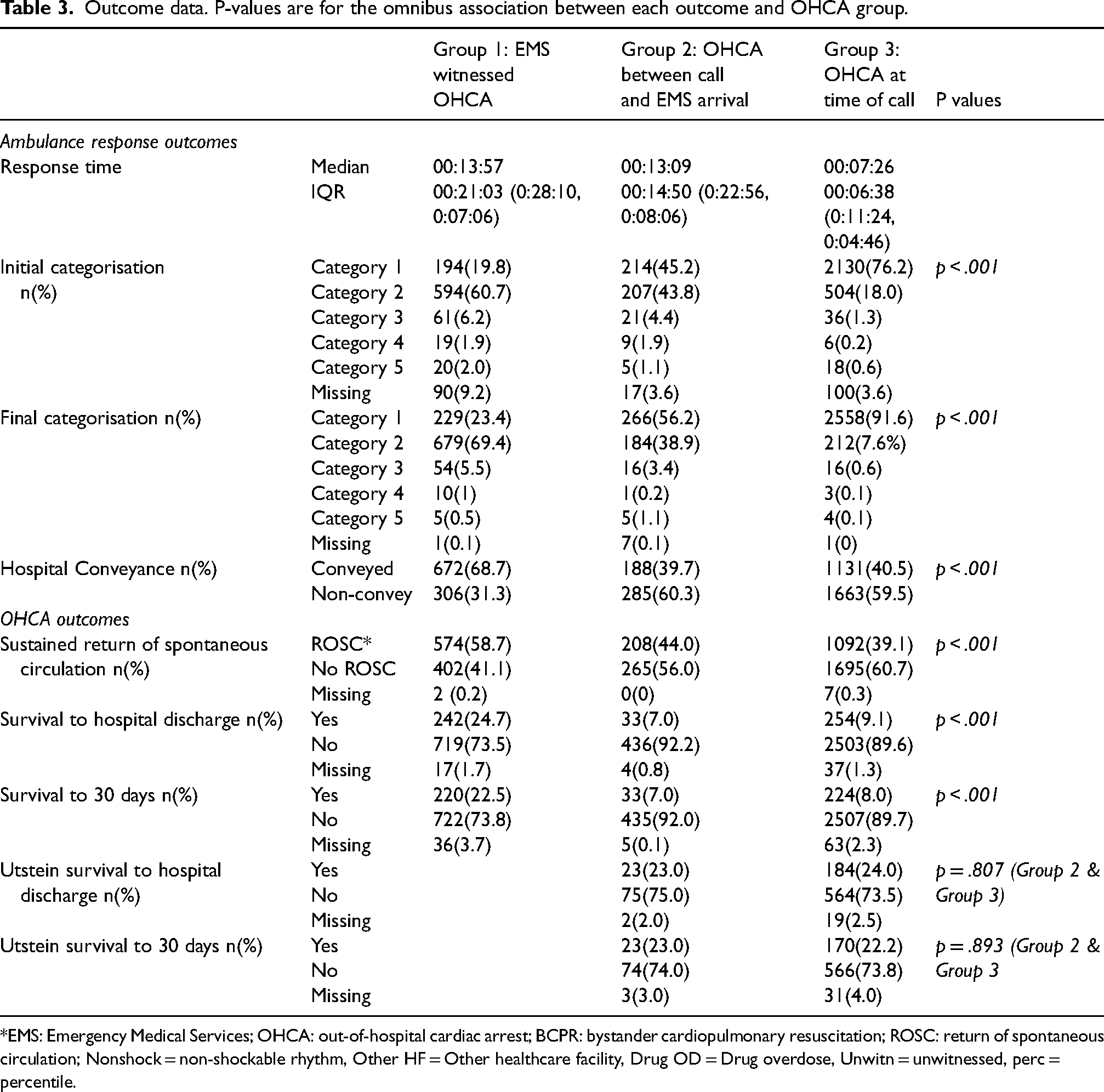
*EMS: Emergency Medical Services; OHCA: out-of-hospital cardiac arrest; BCPR: bystander cardiopulmonary resuscitation; ROSC: return of spontaneous circulation; Nonshock = non-shockable rhythm, Other HF = Other healthcare facility, Drug OD = Drug overdose, Unwitn = unwitnessed, perc = percentile.
Main results
Patient characteristics
Table 2 reports patient characteristics. More men (66.7%) are in the dataset than women (33.1%). Proportionally more women (39.1%) are in the OHCA between EMS call and EMS arrival group than the EMS witnessed group (36.9%) and the OHCA at time of call group (30.8%) (p < .001). Age distribution is similar across groups, but those in G2 who suffered an OHCA between the EMS call and EMS arrival (mean 71.4) are on average two years older than in the EMS witnessed group (mean = 69.3) or in the group who suffered an OHCA before the EMS call (mean = 69.3) (p < .001).
Out-of-hospital cardiac arrest characteristics
Table 2 reports OHCA characteristics. The percentage of patients presenting with a shockable rhythm differs between groups and is statistically significant (p < .001). This observation is robust in the sensitivity analysis (Table 3). Patients who suffer an OHCA between the EMS call and EMS arrival have the lowest percentage of patients presenting in a shockable rhythm.
More patients have a bystander witnessed OHCA in the group where a patient suffered an OHCA between the EMS call and EMS arrival than patients who had already suffered an OHCA at the time of the EMS call, however the latter group had a higher percentage of patients receiving bystander CPR.
Out-of-hospital cardiac arrest outcomes
Table 3 reports OHCA outcomes. There is a statistically significant difference in survival to 30 days between patients who suffered an EMS witnessed OHCA (22.5%) and patients who suffered an OHCA between the EMS call and EMS arrival (7.0%).
EMS response
Patients who suffer an OHCA after the EMS call is made have a comparably longer response time than those patients already in OHCA at the time of the EMS call. Response times relate closely to the categorisation of calls with the highest number of calls triaged as Category 1 in G3 who suffered an OHCA before the EMS call (91.6%) compared to EMS witnessed OHCA (23.4%) and patients who suffer an OHCA between the EMS call and EMS arrival (56.2%) . Figure 1 indicates that the predominant MPDS card category in EMS witnessed OHCA is chest pain compared to cardiac/respiratory arrest in both of G2 and G3.
Sensitivity analysis
Supplementary Table 2 indicates the numbers of patients in each group in the sensitivity analyses.
The sensitivity analyses, described in Figure 2, indicate that the finding of there being a statistically significant difference in presenting rhythm between groups is robust. Patients who have suffered an OHCA at the time of the EMS call are more likely to have a shockable rhythm and those who suffer an OHCA between the EMS call and EMS arrival are less likely to have a shockable rhythm than statistically expected. The sensitivity analyses are summarised in Table 4. When the sensitivity analyses were conducted on patient outcomes to include survival to hospital discharge and survival to thirty days there was not a statistically significant difference between G2 and G3 over the range of scenarios. With the 3-min cut off applied to sustained ROSC there is no compelling robust evidence that ROSC differs between G2 and G3.
Description of the sensitivity analyses
Results sensitivity analyses between group 2 and group 3.

*ROSC: return of spontaneous circulation.
Discussion
Analysis compared the characteristics and outcomes of patients who had not suffered an OHCA at the time of the EMS call to patients who had already suffered an OHCA at the time of the EMS call, with important findings. Patients who suffer an OHCA after the EMS call is connected receive a lower priority response and a significantly longer response time than those patients who have already suffered an OHCA at the time of the EMS call. Patients who suffer an OHCA between the EMS call and EMS arrival have very poor outcomes and this is because the first link in the chain of survival breaks down. Subsequently the EMS response is poor and lifesaving interventions of telephone cardiopulmonary resuscitation and a community response are not actioned.
Immediate treatment by EMS staff following OHCA is linked to improved survival. 17 The comparatively high survival rate in the EMS witnessed OHCA group links to the high incidence of cardiac symptoms in this group and the associated increased chance of survival found in Lee et al.'s Korean study. 18 In Lee et al.'s study, 18 51.5% of the cardiac symptom group presented in a shockable rhythm and achieved the best rate of survival to discharge with a good neurological outcome (42.7%). In our study the EMS witnessed OHCA group had a shockable rhythm rate of 35%, marginally higher than those patients who arrested between the EMS call and EMS arrival (30.7%), but not close to the rate described by Lee et al. 18
Previous research by Nishiyama and colleagues 19 identified that 40% of victims of OHCA displayed symptoms prior to their arrest. In OHCA of cardiac origin the most frequent symptoms prior to OHCA were breathing problems, followed by chest pain and fainting. In OHCA of non-cardiac origin the most common symptoms prior to OHCA were breathing difficulties with chest pain rarely presented. In this study early contact with EMS was associated with better neurological outcomes. Nehme and colleagues 20 investigated the specific group of EMS witnessed OHCA of presumed cardiac cause. In this study 41.5% complained of breathlessness and 29.2% with arm, or shoulder pain prior to collapse. Delays in activating EMS following the onset of symptoms were associated with a reduction in patient survival.
The timing of the EMS response to OHCA is a critical factor in survival. The rapid response time to patients already in OHCA at the time of the EMS call is linked to the call triage and the focus of EMS to prioritise patients who have already suffered an OHCA over those patients at imminent risk of OHCA. Poor survival in this group is likely to be associated with the time delay between suffering an OHCA and the arrival of EMS. For each minute of OHCA, without any treatment, the chance of survival diminishes by 5.5% per minute. 21 The impact of a delay in treating OHCA and associated poor outcomes have been well documented.22,23 A delay in EMS response increases the time to lifesaving treatments such as early defibrillation and early cardiopulmonary resuscitation (CPR), and where a patient initially presents in a shockable rhythm this may progress to a non-shockable rhythm before EMS arrival. 24 Patients who arrested between the EMS call and EMS arrival could show significant improvement in survival if the recognition of imminent OHCA and response to these patients was optimised.
Future research could usefully address: educating members of the public to recognise the symptoms of a patient at high risk of OHCA and the immediate contact of EMS to report the symptoms; modifying the EMS call-taking system so that call-takers are better able to monitor for deterioration in a patient's condition during the call and staying on the call where patients are deteriorating; further exploration of prodromal symptoms where patients are at imminent risk of OHCA and ways to better identify these high risk patients during the EMS call.
This novel study provides new insights into the characteristics, EMS response and outcomes of OHCA patients who have not suffered an OHCA at the time of the EMS call, and who have a relatively high chance of survival, if responded to appropriately. This is a group of patients that are underserved in the existing literature. There is also a possibility that a group of patients are missing from the data because they do not fit the resuscitation criteria of EMS staff, and resuscitation is not attempted as a result meaning these patients would not be included in the local registry. This study did not collect clinical data and future studies that examine the clinical data of patients who are alive at the time of the EMS call and who later suffer an OHCA would support understanding and identification of this important patient group.
Limitations
This is a descriptive exploratory study without pre-declared hypotheses. In common with the view expressed by Rothman 25 and Althouse 26 and others, the reported p-values are unadjusted for multiplicity and have been used to aid the description of the data. For this reason, the p-values are unadjusted irrespective of the number of p-values reported and it is acknowledged that such an approach could contribute to an increase in false findings and the results should be interpreted as exploratory findings. It is also acknowledged that the analyses are based on limited retrospective data and the analyses, and therefore p-values, are unadjusted for confounders. This too can impact on the strength of conclusions. There are well-documented disadvantages of using retrospective data that apply to this study including missing data and confounding factors. 27 In terms of missing data, a large group of 3057 patients were excluded from the main analysis because of the missing time of the OHCA that is required to understand if the patients had already suffered an OHCA at the time of the EMS call and this may have led to some bias in the study. Where data was included for analysis the amount of missing data is given in Table 2 and Table 3 and is a small percentage with remedial action not considered necessary.
An additional limitation is that OHCA registry data analysed relates to 2018-2019 data. There was a delay to publication of this study as it was one study of a PhD programme that was completed during the Covid-19 pandemic with challenges to completion and dissemination activities. The findings of this study remain contemporaneous due to the increasing system pressures impacting on emergency healthcare systems. EMS in the UK face consistent handover delays at hospital and lengthy response time delays to patients in all categories. Patients are facing unacceptable risks and the importance of identifying those at most risk of OHCA remains vitally important. 28
The scene of an OHCA is emotionally charged and chaotic and this compounds errors in recording accurate data such as the time of the OHCA. Patients were defined as having not suffered an OHCA at the time of the EMS call where their OHCA was recorded as being equal to, or greater than, three minutes after the time the EMS call, and this decision affected both G2 and G3. Where the OHCA was witnessed by EMS staff (G1) there was no doubt that this group had not suffered an OHCA at the time of the EMS call, because EMS witnessed OHCA is accurately recorded. The sensitivity analyses tested the findings where the 3-min cut off was changed to 0 or 10 min.
Conclusion
In this single EMS system, EMS response times were significantly shorter for patients who had already suffered an OHCA at the time of the EMS call in comparison to those patients who continued to suffer an OHCA after the EMS call was connected. Our findings indicate that EMS have an ongoing challenge identifying patients who are at high risk of OHCA and categorising them appropriately. Inappropriate call categorisation of these patients in turn leads to delayed response times and poor outcomes. Outcomes in patients that suffer an OHCA after the EMS call, which is unwitnessed by EMS (G2), have especially poor outcomes. Further research is required to understand how to optimise the EMS response to patients at imminent risk of OHCA.
Supplemental Material
sj-docx-1-pam-10.1177_27536386241302116 - Supplemental material for Understanding the emergency medical service response to patients who are at imminent risk of out-of-hospital cardiac arrest
Supplemental material, sj-docx-1-pam-10.1177_27536386241302116 for Understanding the emergency medical service response to patients who are at imminent risk of out-of-hospital cardiac arrest by Kim Kirby, Paul White, Sarah Voss and Jonathan Benger in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386241302116 - Supplemental material for Understanding the emergency medical service response to patients who are at imminent risk of out-of-hospital cardiac arrest
Supplemental material, sj-docx-2-pam-10.1177_27536386241302116 for Understanding the emergency medical service response to patients who are at imminent risk of out-of-hospital cardiac arrest by Kim Kirby, Paul White, Sarah Voss and Jonathan Benger in Paramedicine
Footnotes
Acknowledgements
The authors would like to thank Dr Sarah Black and South Western Ambulance Service NHS Foundation Trust for their support with data reporting and data linkage.
Authors’ contributions
I can confirm that all authors (KK,PW,SV,JB) have made substantial contributions to all of the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, (3) final approval of the version to be submitted.
Declaration of conflicting interests
The lead author Dr Kim Kiby is an Associate Editor of Paramedicine. All other authors have no competing interests to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The lead author, Dr Kim Kirby, has completed a Clinical Doctoral Research Fellowship funded by the National Institute for Health and Care Research in the UK (ICA-CDRF-2018-04-ST2-007). This manuscript is an output from this fellowship funding.
NIHR (grant number ICA-CDRF-2018-04-ST2-007).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.