
Abstract
Acute coronary syndrome (ACS) makes up a substantial healthcare burden. Previous research has demonstrated that women fare worse than men across a range of hospital-based ACS processes and outcomes. In the prehospital setting, the 12-lead electrocardiogram (ECG) can identify critical ACS cases and speed access to definitive treatment. However, studies on rates of ECG acquisition among patients at risk of ACS in the prehospital setting have shown that women receive the test less frequently than men. The purpose of this study was to investigate the reasons for observed gender differences in rates of ECG acquisition in the prehospital setting. This is a cross-sectional study of paramedics in an urban emergency medical service agency. An experienced qualitative researcher conducted 26 semi-structured interviews. Using a subjectivist inductive approach, the study team analyzed interview transcripts following the six-step process described by Braun and Clarke (2006). Qualitative rigor was maintained through consistent review, discussion, and revision at each stage. Four themes were identified among diverse views around the 12-lead acquisition. (1) Safety (feelings of physical comfort and psychological safety related to administering a 12-lead). (2) Knowledge (subject-matter knowledge involving the protocols and procedures as well as self-knowledge of participants’ own practice). (3) Training and learning (perceptions of foundational training and on-the-job learning, and how those have influenced their perceptions of how to care for patients experiencing ACS). (4) Professionalism (perceptions of behavior and attitudes and how they influence patient care). These four interrelated themes were integrated to represent a model of prehospital cardiac care. This study addressed a gap in the literature by documenting prehospital providers’ attitudes and beliefs around cardiac care. The resulting model of prehospital cardiac care offers both a template for evaluating the equity of current treatment and a road map for improvement.
Introduction
Cardiovascular disease and acute coronary syndrome (ACS) make up a substantial healthcare burden worldwide.1–4 Although deaths and disease prevalence disproportionately affect low- and middle-income countries, the experience of high-income countries has shown that early identification and prompt treatment can, among other interventions, reduce ACS mortality.1–3 Despite these benefits, more recent research has shown that women fare worse than men in ACS management. Specifically, women are less likely to be identified as at risk of cardiovascular disease, less likely to receive preventative care, less likely to be diagnosed with ACS, and more likely to suffer adverse events or to die after diagnosis.5–10
Observed gender differences in outcomes of patients with cardiac conditions were characterized as the “Yentl syndrome” in the early 1990s. 11 Referencing the movie of the same name, this commentary highlighted the impact of viewing cardiac disease through the lens of male presentations: women were recognized as sick only when they acted like men. Current literature shows that gender disparities in this field have persisted to the present day. Women experiencing ACS are more likely to have been told their symptoms were not related to a cardiac problem (53.54% vs. 36.%, p < 0.001). 3 Women diagnosed with an ST-elevation myocardial infarction (STEMI) are less likely to be treated within recommended timeframes than men (OR 0.85, 95% CI: 0.80–0.91), 9 and men are more likely than women to be treated with coronary angiography overall (OR 1.64, 95% CI: 1.11–2.44).3,5 Among other outcomes measures, major adverse events have been shown to be less likely among men (OR 0.67, 95% CI: 0.56–0.80), and studies tracking mortality after percutaneous coronary intervention (PCI) demonstrate consistently lower rates for men than for women (2-year mortality, odds of death among men, OR 0.71, 95% CI: 0.63–0.79). 7 Possible explanations for the gap in observed outcomes include both physiological and social factors.5,9,11–13 As an example, a recent survey of knowledge among women in the United States about cardiovascular disease illustrates how cultural assumptions about ACS could contribute to systematic bias: 45% of women did not know that cardiovascular disease was the leading cause of death among women, and women, in general, perceived a range of barriers and stigmas associated with seeking medical care and maintaining a schedule of regular check-ups. 12
Efforts to improve patient outcomes in ACS have emphasized the importance of early recognition and transport. Guidelines commonly recommend that patients be assessed with a 12-lead electrocardiogram (ECG) within 10 min of medical contact, and, in cases of a STEMI, receive definitive care within 90 min. 14 In areas with established emergency medical services (EMSs), various systems have been implemented to integrate STEMI identification and treatment into prehospital care.15,16 It is now common for prehospital providers to perform and interpret 12-lead ECGs, communicate with hospital-based cardiologists, and transport patients directly to facilities capable of providing definitive care, bypassing emergency departments. In some areas, these prehospital system interventions have demonstrated significant decreases in time to treatment and commensurate improvements in patient outcomes.17,18
Despite improvements in ACS outcomes from integrated systems of care, it is possible that women and men do not receive the same benefit. In one study of patients with diagnosed myocardial infarction, women were less likely to have received a prehospital 12-lead than men (OR 0.88, 95% CI: 0.83–0.92); another study of patients treated by paramedics with a working diagnosis of ACS showed similar results (OR 0.50, 95% CI: 0.40–0.63).19,20 A recent EMS quality-improvement (QI) project confirmed a similar gender gap in rates of prehospital electrocardiogram (ECG) acquisition across all potential complaint categories (including patients who complained of chest pain, but also of less common symptoms such as shortness of breath or general weakness). 21
While gender inequity has been quantitatively demonstrated among numerous high-level studies, comparatively little research has examined reasons for observed differences. Similarly, few studies have investigated gender disparities in ACS care in the prehospital setting (as compared to in-hospital), despite the importance of integrated systems to patient outcomes. To address these gaps, this study aims to investigate the reasons for observed gender differences in rates of ECG acquisition in the prehospital setting.
Methods
Study design and methodology
This is a qualitative study of frontline personnel (paramedics and firefighter–paramedics) in a mid-sized Canadian urban EMS agency. The design of this research is predicated on the position that when studying practitioner perspectives, there is no one objective truth. 22 This epistemological foundation is appropriate since the prehospital context and specifically, the work of paramedics is often dynamic, complex, and varies depending on the type of call they respond to. As a result, this study used a subjectivist inductive approach, 23 since there are multiple meanings associated with the practice of delivering prehospital care, and by extension, paramedic practice. Qualitative methods were also congruent with the collaborative analysis and exploration of the workplace experiences of paramedics’ perceptions of ECG acquisition.
Research team and context
Interviews were conducted by an experienced qualitative researcher based in an academic institution and whose research program focuses on the workplace learning of first responders. The remaining research team members have various work roles and qualifications with the EMS agency, such as training officer/research coordinator (whose experience includes being a doctoral candidate), QI officer (advanced care paramedic), or medical supervision and direction (who also is an emergency medicine physician).
The Winnipeg Fire Paramedic Service provides an emergency medical response within Winnipeg – a city of approximately 750,000 in Manitoba, Canada – and responds to approximately 80,000 medical calls a year with basic life support (BLS) first response and dual BLS and advanced life support (ALS) follow-up. Under national certification guidelines, BLS and ALS providers in this service are termed Primary and Advanced Care Paramedics, respectively. Among all paramedics and firefighter–paramedics in this service, approximately 22% identify as women.
Sampling and recruitment
A combination of purposeful and convenience sampling was used to identify a range of study participants based on work role and gender. Participants were contacted by the third author during work hours and informed of the study’s purpose. Once consent was obtained, interviews were scheduled and conducted over the telephone and digitally recorded using a digital voice recorder.
Data collection
We used semi-structured, in-depth interviews as our primary source of data collection (see Appendix A for the interview guide). A draft interview guide was structured around perceptions of care protocols related to ACS, gendered approaches to administering 12-leads, and how 12-lead acquisition amongst women in the prehospital setting could be improved. The draft guide was piloted to encourage open dialogue, and clarity, and to ensure leading questions were avoided. The interview guide evolved over time as necessary to incorporate emerging concepts or suggestions from the participants. Since interviews were conducted during work hours, participants were allowed to take time to interview via telephone in a separate room to ensure privacy. Two interviews had to be cut short due to work-related interruptions, but were completed later in the day in both instances.
Data analysis
The digital audio recordings of the interviews were transcribed by a professional transcription service. As the first step in the analysis process, each team member, upon receipt of the transcripts, separately reviewed and familiarized themselves with the data following the six-step process outlined by Braun and Clarke. 24 In step 2, the research team met to generate initial codes from our interpretations of the interview data. Extensive memos and meeting notes were collected during our meetings to ensure there were no significant differences, redundancies, or errors through this initial familiarization process. In step 3, the research team met on multiple occasions to discuss our interpretations of the themes from the data set and then proceeded to step 4, which involved reviewing potential themes to further refine the coded data set. This reflexive approach aimed to ensure a rich and thick description of the interview data rather than focus on the consensus of meaning. In step 5, we defined and named themes from our analysis. Step 6 involved the production of a written report and conference presentations congruent with our integrated knowledge-translation strategy. Throughout the analysis process, trustworthiness was achieved by utilizing a shared Excel spreadsheet of our interpretation of the data and resultant themes to ensure confirmability and dependability. Member checking was not performed with the participants per se but incorporated into the interview via a question and answer by the interviewer to ensure participants' responses were aligned with the intended meaning of the question. Triangulation of the data, moreover, was also achieved by ensuring the research team met frequently and consistently to review, debate, and refine the data, to discuss our mutual interpretations of the data, and to debrief each other throughout the analysis process.
Ethical approval
Ethical approval for this study was provided by the University of Winnipeg (HE: 14461).
Results
Description of participants
Twenty-six (n = 26) paramedics were interviewed between May 2021 and August 2021 (Table 1). Twenty participants were men. Fourteen worked as firefighter–paramedics, 10 as paramedics, and two as field supervisors. Participants’ median age was 33 (interquartile range: 30–40) and years of experience was 10 (interquartile range: 5–13). The interviews ranged from 25 to 65 min with an average interview length of 47 min. Quotations in the findings section are identified only by randomly generated pseudonyms.
Participant demographics.
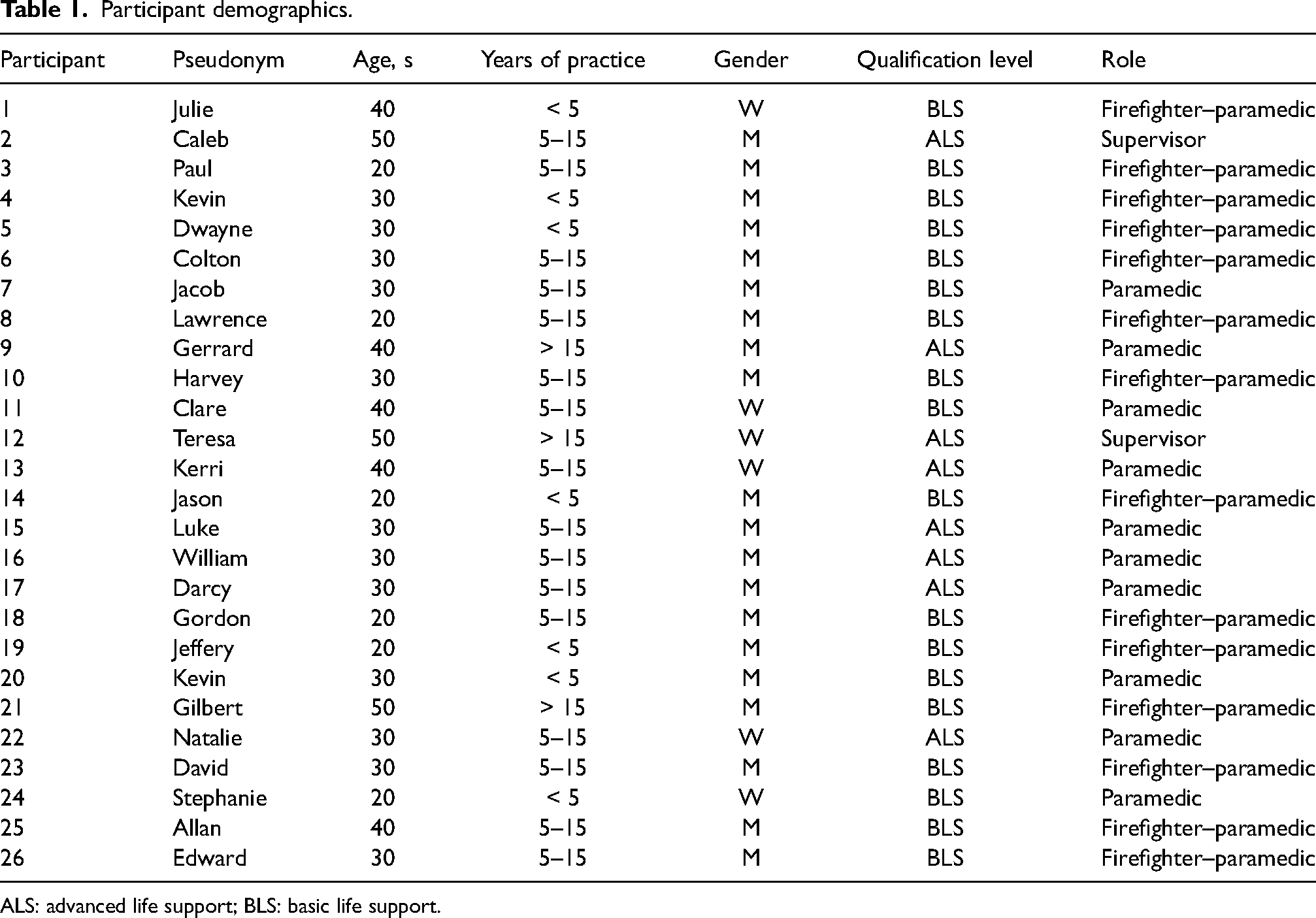
ALS: advanced life support; BLS: basic life support.
Qualitative findings
We identified four themes from our interpretation of the interview data. The first and core theme is safety and encompasses feelings of physical comfort and psychological safety related to administering a 12-lead. The second theme is of knowledge and includes core subject-matter knowledge involving the protocols and procedures with acquiring a 12-lead as well as self-knowledge of participants’ own practice. Thirdly, training and learning involves the participants’ perceptions of formal education and on-the-job learning, and how those have influenced their perceptions of how to care for patients experiencing ACS. The fourth and last theme—professionalism—expresses participants’ perceptions of conduct and communication and how they influence patient care.
Safety
The theme of safety involves feelings of physical and psychological safety related to the 12-lead acquisition. Specific sub-themes include hesitancy or discomfort on the part of the paramedic; perceptions of patient comfort; concerns for privacy; sensitivity to patient circumstance, identity, or expression; and notions of liability or risk. Gender difference and gender concordance (between provider and patient, among providers) appeared commonly among all sub-themes. We consider safety to be foundational. One paramedic, for instance, concisely summarized how gender interacts with a complex mix of implicit and explicit attitudes, preconceptions, and judgments while administering a 12-lead: It's like a weird power dynamic being a male and doing that procedure on a female … I think there are ways to do that respectfully, but I mean, if I was a dude, it would be something I’d be thinking about. (Julie)
Many participants felt that paramedics in general might hesitate to acquire a 12-lead on a woman or feel uncomfortable while doing it. Although many participants attributed these feelings to others, few described hesitation or discomfort in themselves. Decision-making was portrayed as a balance between perceptions of needing the assessment and occasional discomfort with performing the task. Participants suggested reasons for hesitation that ranged from simple inexperience to discomfort with gender discordance. It is also important to note that participants emphasized their belief that any delay would be minimal, and that patients who require the assessment receive it.
Paramedics’ perceived comfort with acquiring a 12-lead ECG was strongly influenced by their perceptions of patient comfort. One participant, for instance, noted that it's not necessarily comfortable for us as first responders. I would say [it is] more comfortability for the patient. You don’t know what they’re comfortable with. (Colton) I don’t know if it's more of a comfort thing for me or if it's just me trying to see if I can make the patient comfortable, but [if I have a female partner], I’ll ask if she doesn’t mind doing the 12-lead. But like I said, most of the time, I think with a lot of the female employees that I’ve worked with, they kind of just jump in there and do it right away, rather than me. (Darcy)
Many participants acknowledged the frequent gender imbalance between providers and patients and the potential effect this has on the process of assessment and administering a 12-lead. As one participant stated, [acquiring a 12-lead is] largely related to the patient and their comfort with this as well. You know, we've had patients where there's the four of us [men] and then they’ll ask, “Is there not a woman around?” (Edward)
Almost all participants acknowledged the importance of privacy. Most participants, for example, shared that if patients were in public places, they would either establish a private area at the site of patient interaction (e.g. with blankets) or wait to perform the assessment in another room or inside the ambulance. Similar accommodations would extend to acquiring a 12-lead in a home by limiting the number of people in the room or ensuring that a patient had a trusted friend or family member present. Participants expressed sensitivity to religious and cultural backgrounds. In these instances, however, participants offered fewer specific examples and were willing to acknowledge their knowledge gaps: I’ll be the first to admit I’m not overly aware of all the specifics of everyone's culture, but I do understand that there are different expectations when you’re in someone's house, right? (Harvey)
A final area to acknowledge amongst the participants was the concern expressed about how acquiring a 12-lead could expose them to liability or risk. Collectively, these covered a spectrum of concerns. On one end of the spectrum, several participants expressed the importance of always assessing patients in pairs, a practice summed up by one senior practitioner as the “two-deep” approach (Caleb). In the middle of the spectrum, several participants acknowledged the influence of broad social justice movements, such as #MeToo, on how they approached work. Lastly, on the opposite end of the spectrum, this awareness took shape more as a perceived risk to their personal integrity and livelihood. Some participants expressed concerns about being accused of inappropriate or unprofessional conduct. At this end of the spectrum, and compared to other responses, these views appeared to be preoccupied with potential consequences: I think that maybe some of the reluctance—it's that guys are like, “wow, you know, if suddenly she decides that I'm, you know, putting my hand or finger or sticker in the wrong spot, I'm going to lose my job.” That's a huge factor … Well, if I don't have to do this [acquire a 12-lead] and I can still get away with it and keep my job and not have to deal with any of the potential issues, then we’ll try to do that. You know? Guys are under the microscope big time. And, yeah, I guess the guys are going into self-preservation mode with everything now. Functionally, it's taking a toll on people. (David)
Knowledge
The theme of knowledge was interpreted broadly and encompasses sub-themes that include specific knowledge of ACS protocols, general knowledge of sex- and gender-based differences in presenting signs and symptoms, and participants’ own self-knowledge of potential gender bias in care.
We found that many participants were up to date with protocol changes (although some remarked on ‘change fatigue’ associated with frequent updates). These changes emphasized broader indications for a 12-lead beyond chest pain, as well as the direction for prompt assessment. Moreover, several participants communicated their understanding that women experiencing ACS can present with subtle symptoms not usually associated with the traditional description of chest pain. One participant, for instance, shared: I’m conscious that female chest pains or a cardiac event in a female can often present differently than in a male, so I will ask more questions about pain sites to females. Probably I’m a little bit more thorough with asking about jaw pain, arm pain, shoulder blade pain when it comes to females, or being [aware] that they might not have pain at all. (Kerri)
Participants differed in their belief that care provided to patients might differ based on the gender of the patient. Relatedly, there were differing perceptions and understandings with the term bias. In our estimation, it is likely that, for some participants, it carries pejorative connotations of personal dislike that would be seen as failings; for others, it could be acknowledged as either a reflection of unconscious conditioning (and therefore only blame-worthy if unexplored or ignored) or as a characteristic of a system, or both. As we reviewed the data, we found that some providers acknowledged observing differences in care among other paramedics but not themselves. Alternatively, several participants described a bias in the system but not individual providers. As the following quotation demonstrates, when participants took an opportunity to reflect, it appeared they acknowledged the potential for gender bias in patient care: Right or wrong, there is a difference, I guess. We’re a little bit more willing to open up a man's shirt than we are a woman. Again, I guess that could be right or wrong. I guess he's entitled to privacy as well. But I’m going to say there's likely a difference. (Edward)
Training and learning
All participants agreed that their education and training had influenced their perceptions of how to provide care to patients experiencing ACS. Participants shared diverse experiences that make-up sub-themes under the general theme of training and learning. These include memories from their formal training before entering the profession as well as reflections on informal, on-the-job learning (including foundational experiences). Additionally, a small number of participants had extensive and detailed thoughts on techniques associated with acquired a 12-lead on a woman, and many offered specific suggestions for training and improvements to reduce gender disparity.
With respect to formal schooling, participants’ recollection of the amount of time devoted to gender-specific training in ACS spanned a narrow range. For some, it was none. Others recalled a small amount of time with only one or two specific tips, such as how to lift the left breast for placing V4. No participant recalled performing the skill either on a woman or on a female mannequin. In general, training was described as brief, to the point of being “an after-thought” (Jason), or simply “unisex” or “gender-neutral” (Edward). When describing practicing lead placement, one participant summed up the value of the exercise: And then we [practiced on each other]. Actually, I think I was used as a training aid. Leads were placed on my chest. And that's fine, that encompasses half of the population and you've learned well for half the population. (Edward) I’ll never forget that call … I think the biggest thing is we could have just cancelled that call and she could have died within hours to days from that STEMI. And she was just your regular flu-like symptoms … So that was an eye-opener and that's made me very conscientious when I’m looking at ACS. (Teresa)
All providers who described similar events emphasized the personal nature of how they have retained and interpreted the experience. While these recollections all feature some memorable event, it is possible that those who described these experiences are inclined to self-reflection and value on-the-job learning.
The procedural skills of performing a 12-lead ECG on women made up a substantial sub-theme related to training. A small number of detailed observations conveyed how deeply some participants considered the subject. For these participants, performing a 12-lead on a female patient required a deliberate approach and considered a range of situational and patient-centered factors beyond what might be required for a male patient. Participants frequently noted the need to consider a patient's anatomy, and the accommodations required to place the precordial leads accurately. These considerations include positioning, anatomical landmarking, removing a bra, and lifting the left breast, with additional forethought given to both elderly and large-breasted patients. Specific techniques mentioned included using the back of the hand to move the left breast, adjusting access to minimize a patient's exposure (such as placing V1 and V2 through the shirt collar, and V3–V6 from underneath), and moving the patient to a location that facilitates access (such as a sofa, bed, or the stretcher) before starting. Overall, the participants who commented on explicit techniques for acquiring 12-leads on women conveyed that the process was not simple, automatic, or achievable without care and deliberate planning.
When given an opportunity to offer suggestions for addressing differences in care, participants suggested more focused professional development. In some cases, this was interpreted as training in basic knowledge, such as physiologic differences in risk factors or disease characteristics. One participant verbalized the concept of unconscious or subconscious bias and the importance of disclosing this practice: [It would help to know] that this is happening so people are aware of it either consciously or subconsciously happening … Then we can maybe see our own subconscious biases that we can address while we’re on the calls. (Kevin)
Moreover, almost all participants endorsed the idea of female mannequins as a training aid, and some felt that being instructed by women would add further value to training and learning. Some BLS providers mentioned that they would be more invested in the process if trained and authorized to interpret 12-leads in addition to acquiring them. Significantly, most participants advocated for more women in the paramedic workforce as a fundamental starting place for addressing gender gaps in assessment.
Professionalism
Woven throughout the interviews, many participants commented on various ways in which paramedics’ conduct and attitudes can influence patient care. We believe these observations share a common thread of professionalism. Among different attributes of professionalism, the following were identified as sub-themes: professional conduct, respectful communication with the patient, and examples of unprofessional behavior.
In the specific context of performing a 12-lead, participants emphasized how approaching the procedure in a clinical, professional way could alleviate their own discomfort and the patient's expressed or intuited concerns. Some cited the protocol as a source of support: I think it helps that a protocol came out just saying it's expected. This is part of your job. This has to be done within a certain length [of time]. Because then it's just like, “No, this is just a professional test, right? This is what we do. There are no sexual connotations here. This is an important part of giving you the best treatment possible.” (Julie) I’ve got into paramedicine because I wanted to be treated and act like a professional … I have my own personal experiences with being overly sexualized as a female, so I would never want a female to feel that way. So I just always want to make sure that when I’m performing a medical procedure that has anything to do with one's gender—one way or the other—that I’m always very respectful and professional. (Natalie)
For many participants, a professional approach centered on clear communication with the patient. These paramedics emphasized the need to explain the rationale for a 12-lead, what the procedure involves, and that the patient consents. One participant, for instance, shared an awareness of building rapport to develop trust within a patient interaction: You just have to be a crafty wordsmith and make an environment where you build rapport and people are comfortable with you and you have this air of professionalism, and you have a good handle on discretion … You just have to make them feel comfortable with your presence when you’re by yourself. (William)
We found that the theme of professionalism also included unprofessional or less-than-professional behavior. During the interviews, participants were provided an opportunity to reflect on circumstances that might challenge their decision-making to acquire a 12-lead, and many acknowledged barriers. Participants who had supervisory responsibilities consistently expressed the notion that not completing a thorough assessment will, “get you in the end” (Teresa) or “bite you in the butt if you’re not careful” (Caleb)—sentiments connected to experience and foundational learning events. In a small minority of cases, participants spoke about the inter-personal conflict that arose from decisions around acquiring a 12-lead. In these cases, BLS providers expressed that they could be “run down” or “given shit” for how they placed the leads or their decision either to acquire a 12-lead or to delay one until ALS arrived. These participants felt that the 12-lead sometimes became a lightning rod for other workplace issues, functioning as an excuse for others to find fault with their skills or conduct. These situations were described as counter-productive to good patient assessment, with negative feedback directly connected to future “doubt” or “hesitancy.” (Lawrence).
A model of equity in prehospital 12-lead ECG acquisition
The four identified themes each contain separate but related ideas under a common meaning. Each contributes to our understanding of prehospital cardiac care in general, and 12-lead ECG acquisition specifically. Collectively, these themes combine like puzzle pieces to form a picture of prehospital cardiac care (see Figure 1). In our understanding, the theme of safety occupies a central spot, but each other theme has a unique location, occupying its own space and linked to the rest with interlocking connections. Conceived in this way, safety acts as a keystone: with many distinct and related nodes, it interacts with others around the circle and locks the entire picture into place. At the same time, the theme of safety is not depicted with any color or outline; it occupies white or negative space, and its borders are defined by the themes around it. Seen this way, safety also passively arises from the presence of and connections among training, knowledge, and professionalism, and attention and deliberate actions related to those themes create a safe space that would not otherwise exist. Overall, the figure represents findings on this topic in a way that represents the equity of care provided. Puzzle pieces that fit well and smoothly together represent themes that are present, well-considered, and integrated with others in practice. These create a good picture. Alternatively, pieces of the puzzle might show cracks, bad fits, and misalignment, creating a disjointed or broken picture. This would represent elements of care that are not seamlessly integrated, but which show gaps in care and room for improvement.

A model of equity in prehospital 12-lead electrocardiogram (ECG) acquisition.
In the case of these findings, the quality of the picture can be assessed by the connections and disconnection among themes. Among participants in this study, there were strong connections between those who showed high levels of knowledge—whether related to protocols or their self-awareness and comfort with notions of self-reflection and bias—and their expressed feeling of comfort in performing the skill. Similarly, those with more experience, confidence in their practice, or with strong foundational learning events, also spoke with more assurance about how they approach and manage cardiac calls. Those most comfortable were also those most aware of how their bearing and leadership sets both an explicit example and implicitly professional tone that contributes to equitable care.
Findings from this study also reveal areas of disconnection among the included themes. Several participants described situations where paramedics felt uncomfortable acquiring a 12-lead or might hesitate in choosing to do one but were unwilling to entertain the possibility that those feelings might bias care. There was a strong disconnection in responses to a direct question about possibly inequitable care: many answered flatly, “no”; for others the response was, “absolutely, yes,” or at least consideration that it might be possible. In a small number of instances, views shared by participants revealed instances of inter-personal or inter-professional conflict and appeared to run counter to conventions of professional conduct in health care.
Discussion
The purpose of this study was to investigate the reasons for observed gender differences in rates of ECG acquisition in the prehospital setting. The findings were grouped into four interconnected themes: safety, knowledge, training and learning, and professionalism. This thematic scheme informs a model of prehospital cardiac care that can represent the equity of treatment provided through the interactions among its elements. The data included in this study show strong connections among these themes but also areas of disconnect or gaps and can be interpreted as describing a system that performs well across many areas but has substantial room for improvement.
This study was motivated by findings that rates of ECG acquisition in possible cases of ACS are lower among women than men.19–21,25 Although not widely studied, this topic has been investigated in a small body of related research. Surveying volunteers who received a 12-lead, Wallen et al. 26 speculated that gender differences in acquisition rates might reflect several sources of bias. These include the possibility of a paramedic not considering ACS, as well as hesitancy on the part of the paramedic to expose a woman's chest or on the part of a woman to consent to the procedure. They conducted their study to investigate women's preferences for electrode placement and attitudes toward the gender of the paramedic. Among 50 healthy volunteers, 52% preferred electrode placement on the left breast as opposed to underneath. A small minority (6%) stated they would decline the procedure if offered only by men, but all respondents said they would accept the procedure from any provider if it would reduce the time to definitive treatment. Within the survey, respondents expressed confidence in the professionalism of paramedics and the importance of the procedure in the context of a possible medical emergency. The authors conclude, “It is possible that paramedics are more concerned with the acceptability of acquiring an ECG than women are themselves.” 26 (p852)
This conclusion speaks directly to the frequent observation within the current study that paramedics assume a woman would prefer to have another woman perform the 12-lead. While commonly expressed, this view was qualified with the belief that the procedure happens if necessary. Taken together, participants in both studies appear concerned about how the procedure might be perceived, especially when performed by a man on a woman but acknowledge the importance of medical assessment in a potential emergency. While the effect of patient-paramedic gender concordance has not been extensively studied in the prehospital setting, a few papers have considered this effect on patient satisfaction in other contexts. A recent study on mortality among female heart attack patients found that female patients were least likely to survive when treated by male physicians, even when accounting for a variety of potential confounding factors. 27 This effect was attenuated in cases where male physicians worked in emergency departments (EDs) with higher proportions of female physician colleagues or in proportion to the number of female patients seen by male physicians in the recent past 27 In the ED context, other research indicates that women are more satisfied with their care when it is delivered by a woman. 28 Despite these findings, other outcomes in other settings have shown mixed results.29–31 The effect of patient-paramedic gender concordance in prehospital care deserves further study.
The other principal finding in the survey conducted by Wallen et al. addresses electrode placement among women. Although the precordial electrode V4 is commonly placed under the left breast,32–34 it has been shown that placement on top of the left breast is more reliable and more likely to be anatomically correct without substantially affecting the amplitude of the tracing.32,35 Nevertheless, guidelines continue to recommend placement below the breast, while noting the variability in placement that can result from differences in individual anatomy. 33 The clinical consequences of misplacement as a result of female anatomy have been documented in various cases resulting in false negative and false positive findings.36,37 Few studies, however, have applied this knowledge or assessed prehospital practice, especially among women. Of note, a recent observational study assessed the accuracy of paramedic electrode placement using only a male volunteer. 38 The authors justify this choice by speculating that observed inaccuracies—already significant in a straight-forward case—would likely be greater had they introduced the “complexities” of female patients. 38 (p12)
As with ECG acquisition, few studies have explored detailed reasons for observed gender gaps in acute prehospital cardiac care. One exception is a recent public survey that investigated why women might receive bystander CPR less frequently than men. 39 The authors of this study grouped responses into three major themes to explain lower rates of intervention: the sexualization of women's bodies (including fears of accusations of sexual assault); a belief that women are more susceptible to injury; and mistaken assessment of distress. 39 Although derived from different participants and a different clinical scenario, these findings share common ground with the current study. Challenges associated with identifying and interpreting symptoms of ACS among women appeared often among our participants. Additionally, hesitancy related to exposing a woman's chest was also commonly noted, and the fear of ECG acquisition being interpreted as inappropriate figured prominently among a small minority. Authors of the survey study noted further that “bystander” was almost always interpreted as a man among their respondents. 39 In response to these findings, they advocate for clear instruction and policy statements to reduce bystanders’ fears of prosecution and for initiatives to normalize women performing CPR. 39
The model of equitable prehospital cardiac care described by these results can be used not only as a framework for evaluation, but also as a roadmap for future improvement. There is a clear opportunity for additional study and training related to how paramedics (and other healthcare providers) understand different meanings of bias and the extent to which individuals feel reluctant or willing to acknowledge systemic as compared to individual bias. Additionally, individual instances of attitudes or behaviors that are not consistent with best practices reveal that diverse views exist and that these would remain hidden if not for discussing these topics. That these sentiments were offered freely indicates a lack of self-consciousness. It is our view that training and education have a role in setting an explicit standard and would be expected to effect change.
This study also demonstrated clear gaps between training and paramedics’ ability to enter the workforce at a basic level and acquire 12-leads in a professional manner among all patients. Many participants spoke to their inexperience and immaturity in their early career, as well as their lack of training in gender-specific techniques. While junior practitioners in any field require experience and on-the-job training to become proficient, it is apparent that some of the observed gender-based gaps in assessment could be addressed at the training level—whether by specific technical instruction or as a case study in larger topics such as professional communication and patient interaction. Participants were clear that some explicit technical instruction is required but is not currently being taught. Furthermore, connections that currently exist between training and professionalism through mentorship, coaching, and foundational learning events could be formalized and leveraged in a more basic curriculum.
The comfort that experienced providers conveyed with elements of the technique of 12-lead acquisition sets the stage for the communication and conduct that marks a professional approach. Providers with high levels of knowledge and experience (sometimes described as the “reps”) conveyed that they are capable of seamlessly performing the skill while at the same time establishing the tone of the scene, talking patients through the procedure, and setting them at ease. There was, however, a disconnect between participants’ leadership on cardiac calls and their knowledge and comfort level with patients with non-binary orientation, identity, or reproductive development (sexual and gender minority, SGM). A small but emerging body of research into health disparities among SGM patients has shown higher likelihoods for relevant conditions as compared to non-SGM counterparts, including hypertension (8%), cardiovascular disease (14%), myocardial infarction (33%), and stroke (24%). 40 A survey of SGM individuals reported that nearly half the respondents had chosen not to visit an ED for an acute condition, partly for fear of discrimination or past experiences. 41 Members of SGM groups have observed treatment from healthcare providers that aligns with documented bias in terms of symptom recognition in ACS. 42 The overall level of SGM literacy in this service is unknown, and training in this area was not suggested by any participant. Although not widely studied, the topic represents an important area for future research and training, especially in adapting communication techniques studied in the ED to the out-of-hospital setting.43,44
There are several limitations to the study presented here. The findings of this qualitative research are not automatically transferable to other areas of prehospital medicine. We intended these findings to be generative to other researchers in the field of paramedic research, rather than generalizable, and we believe that this study contributes to this line of inquiry. Another limitation involves methodology since this study only used interviews. We believe that these in-depth interviews provided a detailed perspective of those working on the front lines of paramedic practice. It is possible, however, that these perspectives may be limited by the small sample size and perspectives shared about sex and gender in 12-lead acquisition. Future research involving follow-up interviews and focus groups is warranted.
This study addressed a gap in the literature by documenting prehospital providers’ attitudes and beliefs around 12-lead acquisition, especially among women patients. These attitudes contributed to a model of prehospital cardiac care—a model that incorporates four themes and provides both a template for evaluating the equity of current treatment and a road map for improvement. In the future, this model may prove adaptable to similar investigations in other areas, in turn promoting and developing inclusive and patient-centered paramedic care across the professional practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.