
Abstract
Births in the prehospital setting are infrequent yet associated with increased odds of maternal and neonatal morbidity and mortality. There is limited understanding of the experiences of emergency medical services staff in handling these potentially high-risk situations. We explored the perspectives of ambulance personnel in Aotearoa New Zealand when responding to out-of-hospital births. Hato Hone St John Ambulance is the largest emergency medical services provider in Aotearoa New Zealand. Between October and November 2023, all Hato Hone St John frontline staff were invited to complete an online survey, including open text questions about their experiences and challenges attending unplanned births. Data was coded and organised into themes using NVivo software and the inductive approach to thematic analysis. One hundred and forty-seven responses were received and included in the survey. Participants encountered a range of challenges in providing intrapartum care in the prehospital setting. Two key themes were identified: (1) navigating complexity and uncertainty in unplanned births, and (2) practical challenges and unsuitable environments; with several subthemes demonstrating that the ambulance personnel responded to obstetric emergencies in diverse circumstances, diligently working to deliver optimal care for both mothers and neonates. This study describes novel challenges faced by ambulance personnel attending unplanned births in Aotearoa New Zealand alongside obstacles previously reported by emergency medical services in other jurisdictions. These findings may be invaluable in guiding further research, curriculum and resource development to better prepare ambulance personnel for the challenging and uncertain situations that characterise prehospital birth events.
Keywords
The vast majority of births occur in a healthcare facility, with 86% of births worldwide attended by skilled health professionals. 1 However, the onset and course of labour and delivery can be unpredictable. This occasionally results in births away from the intended location of delivery, en route to a hospital, or without the support of a midwife or other clinician trained in obstetric care. 2 In high-income countries, unplanned out-of-hospital births typically make up fewer than 1% of total births.2–4 While such births are infrequent, they carry increased risk of adverse maternal and neonatal outcomes, which escalate further when delivery occurs before full-term gestation.5,6 Population-based studies from a range of high-income countries suggest the risk of infant mortality in the perinatal period and up to one-year post-birth is 2–3 times higher for these births compared to those that take place in appropriate facilities.5,7,8 These effects were thought to be due to higher underlying morbidity in this cohort or lack of optimal healthcare, particularly for pre-term birth.5,7,8
The limited available research on women's experiences of these scenarios indicates that delivering in a vulnerable location and without skilled medical assistance can engender feelings of fear and anxiety in the labouring mother, contributing to a potentially traumatic birthing experience.9,10 Dietsch et al., 11 for example, found women in rural Australia had a variety of negative and risky experiences when required to relocate for childbirth in labour due to inadequate local maternity care, and Svedberg et al.'s 8 participants described physical and mental suffering as a result of unplanned out-of-hospital births in Sweden. Perceptions of unplanned out-of-hospital births are not universally negative, with some women describing the experience as dramatic but special in a way that was not always acknowledged by midwives. 12 Giving birth without a trained healthcare professional present could be an empowering event, particularly on reflection.9,10,12
Emergency medical services (EMSs) may be dispatched to people in labour for a variety of reasons, including to patients who are unaware they are in labour, do not have a healthcare provider to contact, have no transportation, or are experiencing medical emergencies related to birth complications. Generally, EMS involvement in unplanned out-of-hospital births is infrequent, but it often presents a range of obstetric complications for prehospital clinicians.6,13,14
While these cases comprised only 0.5% of the yearly caseload for an Australian ambulance service in 2010/2011, paramedics reported antenatal complications in 27% and maternal complications in 30%. 15 Interviews with frontline ambulance personnel in Norway and Australia revealed a shared perception of inadequate training, education and experience in assisting during out-of-hospital births.16,17 Other studies in the US and the UK have indicated that limited equipment available in an ambulance can hinder EMS in delivering optimal care for mothers and newborns in obstetric emergencies.18,19
Though out-of-hospital births are known to be challenging for EMS personnel, there is a dearth of published research exploring their experiences to inform training and improvements to service infrastructure. In Aotearoa New Zealand (NZ), EMS personnel with a wide range of training and experience may be dispatched to these incidents, from volunteer first responders through to postgraduate-qualified Critical Care Paramedics. NZ ambulance personnel follow standing orders set out in their Clinical Practice Guidelines, which provide recommendations for optimising patient care based on evidence and an analysis of benefits and risks. However, a recent document analysis of Australasian ambulance guidelines revealed unclear and inconsistent information for EMS responding to obstetric emergencies, indicating a misalignment with international best practice. 20 Therefore, there is a need to better understand how these guidelines translate into real-world practice in the context of attending out-of-hospital births.
Our aim was to explore EMS personnel's experiences of attending unplanned birth-related emergencies in NZ, with a focus on perceived challenges in these scenarios. Specific research questions were (1) What are the experiences of EMS personnel in NZ attending unplanned out-of-hospital births? And (2) What challenges do ambulance personnel encounter when responding to pre-hospital births?
Methodology
Qualitative approach
This research is underpinned by a constructivist paradigm, in which knowledge is co-constructed between researchers and participants, acknowledging that researchers are an inherent part of the knowledge produced rather than detached observers of an objective truth. In line with the constructivist approach, the study deepened understandings by exploring what holds meaning for participants in relation to the research questions, while remaining attentive to how the researchers’ positions and interpretations shape the inquiry.
For this study, we used inductive thematic analysis to generate core themes representing patterns of shared meaning in the participant responses, guided by Clarke and Braun's reflexive approach.21,22 Given the broad aims of this research and heterogeneity of the participant population, whose perspectives remain largely unexplored, a wide-lens approach was taken using an online survey. Online surveys are an expedient and low-cost method suited to this approach due to the ease of capturing a larger and more diverse range of responses compared to standard interviews.20,23 Despite their underutilisation in qualitative research, online surveys are capable of eliciting deep, rich data and have potential to capture participants’ perspectives by allowing them to use their own words in an anonymous format. 23 The authors established a transparent audit trail that documented the coding process and other methodological decisions to reinforce the dependability and integrity of the study outcomes. 24
Positionality and reflexivity
The first author is a doctoral candidate and a qualitative researcher with a background in women's health and public policy, and as such is interested in improving health-sector responses to women's needs. The last author is a previous first responder and an experienced mixed-methods researcher. Her perspective is influenced by experience on both sides of the patient/clinician relationship in a perinatal setting. The wider research team includes senior academics in paramedicine with involvement in paramedic student research and training programmes, and both clinical and administrative experience in the ambulance service. Together, the team brings an understanding of the challenges and expectations faced by ambulance personnel, as well as a wider view of ambulance systems and governance in the NZ setting.
We acknowledge the influence of our positionalities across academia and clinical practice on the analysis process. We exercised a reflexive stance towards opposing ideas, resulting in an iterative process of theme development, with open discussion and recognition of blind spots throughout. When interpretations differed, perspectives based on clinical experience were prioritised over ‘academic’ interpretations of these accounts, for example, based on expectations from previous research. In acknowledgement of the lack of ongoing input from research participants during data analysis, the research team aimed to stay close to the data to prioritise participants’ own perspectives of their experiences in line with the aims of this study. 21
Setting
Hato Hone St John (HHStJ) is the largest EMS provider in NZ, covering 90% of the country's population. In 2022, HHStJ responded to 2809 obstetrics-related emergency calls. These included unplanned out-of-hospital births, labour and intrapartum complications requiring a higher level of care than was available at the intended place of birth. Overall, obstetrics-related events account for around 0.8% of emergency ambulance incidents attended by HHStJ. 22 Recruitment took place between October and November 2023. In NZ, EMS work under standing orders called the Clinical Procedures and Guidelines 25 at three defined practice levels: Emergency Medical Technicians (diploma or degree qualified), Paramedics (degree qualified) and Critical Care Paramedics or Extended Care Paramedics (postgraduate qualified). Frontline EMS training pathways have evolved significantly over the last few decades, but current pregnancy and birth education focuses on clinical complications and their management. Formal ongoing training in these topics is acknowledged to be lacking, with education primarily driven by personal interest or on-the-job peer education (D Naylor, Auckland University of Technology, email communication November 2024). All clinical personnel can access medical advice by telephone through the national ambulance clinical desk service.
Participants
All current HHStJ staff and volunteers with road ambulance experience were eligible to participate in this study. As of January 2024, there were ∼1700 HHStJ personnel with authority to practice at Emergency Medical Technician level, 1000 at Paramedic level and 350 at an advanced Paramedic level. An additional 1500 were trained as first responders (certificate qualified), who hold no official authority to practice but are trained to carry out emergency care and may be dispatched on ambulances or alerted to nearby incidents.
Recruitment
EMS personnel were invited to participate through a link to a Microsoft® Forms survey in the HHStJ internal bulletin, which is sent to all ambulance personnel, inclusive of both paid and volunteer staff members. Uptake of the survey was higher than expected, and the survey was closed after 147 responses in consideration of resources allocated for data analysis and the quality of the data collected. During the data collection stage, responses were monitored each week by the first and second authors to gauge the diversity of the sample being recruited to ensure a range of ages, practicing locations, years of experience and qualification levels of participants. The final sample size was deemed sufficient based on qualitative reasoning: the data generated reflected a range of diverse and complex experiences and challenges, and the shared meanings interpreted as a result of initial descriptive coding by the first and second authors demonstrated that the data had conceptual depth and could produce meaningful themes. After discussion, authors agreed that further sampling was unlikely to strengthen the dataset or lead to further novel insights.
Dataset generation
The electronic survey (Supplemental Appendix A) was part of a larger piece of work examining ambulance staff experiences, knowledge and attitudes in the context of out-of-hospital births with EMS involvement. It included questions specific to this study as well as further questions for research and internal audit. Completion times ranged from 5 to 74 minutes, with an average time to completion of 34 minutes. Items analysed for this study were open text questions about participants’ previous experiences attending unplanned births, and their perceptions of these events. Participants were encouraged to provide details to questions such as, ‘Describe your experience attending an unplanned birth, including the circumstance, location, your role, and the challenges faced’, and ‘Please describe your emotions and thoughts around attending childbirth emergencies’. Further survey items covered EMS personnel's demographics; professional background, training and clinical experience; and views on unplanned births, knowledge and beliefs about treating women in labour emergencies, and administering pain relief. The survey was informed by an internal audit of medicines administered to women in labour by HHStJ personnel. The survey was developed in consultation with the HHStJ Clinical Audit and Research team and piloted with a small sample of paramedics (n = 7), first responders (n = 1) and researchers (n = 2) to ensure clarity of questions and appropriate flow of discussion before distribution.
Early survey responses were reviewed to ensure questions were eliciting responses in line with expectations about content and depth based on piloting, and no amendments were made.
Analytic approaches
The first and last authors initially read the survey responses several times to acquaint themselves with the data. Using NVivo software (QSR International), the first author coded the data by grouping respondents’ experiences, perceived knowledge, challenges and understandings of attending prehospital obstetric events. Next, the last author cross-coded the data and interpretations of the findings was discussed. The codes were grouped into potential themes in an iterative process involving discussion over several meetings between the first and last authors before agreeing on final themes and sub-themes. Feedback was sought from researchers in the HHStJ Clinical Audit and Research Team throughout the process, particularly when researchers felt that context about clinical decision making would be helpful for interpretation.
Reporting
The Reflexive Thematic Analysis Reporting Guidelines 26 were used to guide the final version of the manuscript. In addition, the qualitative description method 27 was used to include participant stories to add rich descriptions to the themes identified from the analysis.
Ethics approval
This study was approved by the Northern B Health and Disability Ethics Committee of New Zealand in October 2023 as an amendment to the Aotearoa New Zealand Paramedic Care Collection (ANZPaCC, 2022 FULL 1315). The survey included a disclaimer stipulating that collected data will be used both retrospectively for internal audit and prospectively for research. All research was conducted in accordance with the New Zealand National Ethical Standards for Health and Disability Research and Quality Improvement. 28
Analysis
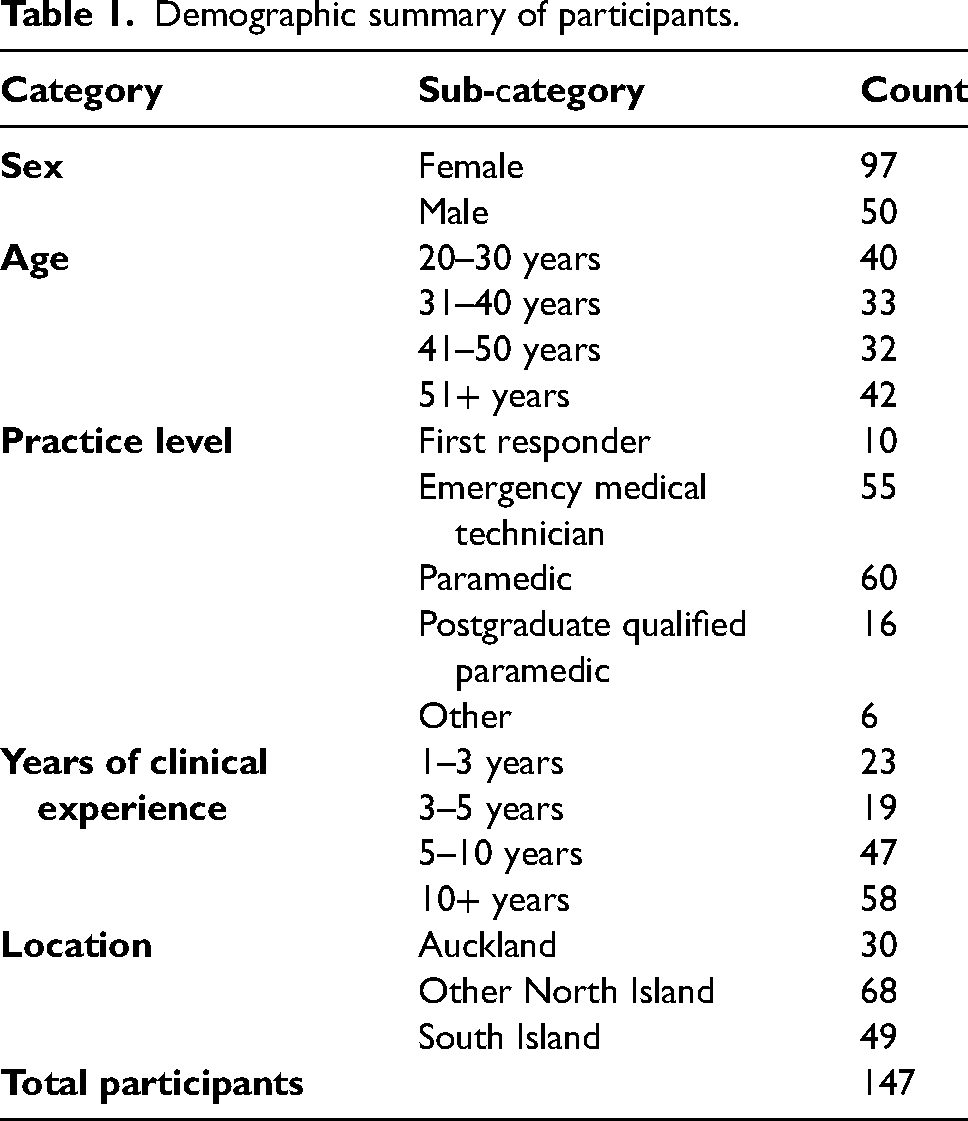
A total of 147 responses were analysed for this study. More respondents were female, and a broad range of ages, professional roles, years of experience and locations were represented (Table 1). New Zealand is geographically divided into North and South Islands, with approximately one-third of the country's population residing in the city of Auckland (North Island).
Demographic summary of participants.
Two main themes were identified from the analysis: (1) navigating complexity and uncertainty in unplanned births; and (2) practical challenges and unsuitable environments. Several lower-order themes are reported under each theme.
Theme one: Navigating complexity and uncertainty in unplanned births
Challenges described by clinicians in this study were frequently underpinned by a perceived lack of information. Participants were required to make clinical decisions with fragmented clinical information in what were often complex situations. As participant 32 summarised, the ‘Biggest challenge was not knowing gestational age of the baby and what complications we were going to face when we delivered baby. No prenatal care so again unsure of the health of baby’ (postgraduate qualified Paramedic, Other North Island). Participants commonly identified salient patient characteristics to contextualise the difficulty of managing patients with a lack of knowledge about their pregnancy, particularly those who were young or delivering in deprived or rural areas. For example, ‘All of my unplanned births were in the [high deprivation] area. A number of these patients had no idea they were pregnant, and therefore had received no care and had no idea how far along they were’ (Participant 48, Paramedic, South Island).
Ambiguous clinical impressions
EMS were frequently called under the impression of addressing abdominal or back pain for a female patient and found themselves unprepared for imminent birth. Many participants recounted scenarios in which the mother they attended was unaware of her pregnancy (also known as ‘cryptic pregnancy’) or denied being pregnant until labour became apparent either en route to the hospital or within minutes of the ambulance crew's arrival on scene. These women often had not received any antenatal care; therefore, gestational age and potential pregnancy complications were unknown to EMS personnel. Furthermore, these patients lacked a midwife or other maternity carer to contact for assistance which tasked EMS with providing lead obstetric care: The call was for non-traumatic back pain. The patient had a cryptic pregnancy and was not aware she was pregnant until I informed her that she was in labour. I was the senior clinician in attendance, we were 25 minutes to a maternity unit that didn’t have surgical facilities and an NNU [neonatal unit]. (Participant 33, Paramedic, Other North Island)
Participants described how lack of information about patients’ clinical picture influenced their decisions regarding drug administration, taking a cautious approach when there was suspicion that labour contractions might be presenting as stomach and back pain; ‘We withheld fentanyl for her abdominal pain because we were suspicious [she could be pregnant] and administered methoxyflurane instead’ (Participant 83, Paramedic, South Island). Concurrently, as illustrated by Participant 124 (EMT, Other North Island), when pregnancy and labour could not be confirmed as the cause of severe pain, they ‘had to keep an open mind that the patient could be having a serious, life-threatening medical event’.
Participants highlighted complex social and interpersonal factors that complicated their ability to assess obstetric situations and engage effectively with patients and their families, ‘especially if the family did not know’ (L3, paramedic, Auckland). Participant 123 (postgraduate qualified Paramedic, South Island) observed that in their experience ‘often the new mother does not acknowledge that they are pregnant or have just delivered a baby’.
Caring for young mothers
EMS described challenging scenarios in which teenage patients were in denial or concealing their pregnancies, and mostly perceived this to be out of fear of family reactions. Participants described feeling caught off guard by not having any prior information about the pregnancy and trying to transport the patient and parents safely to the closest hospital. In one particularly serious case, a female Paramedic with 10 + years of experience described attending to a young patient who had been impregnated under abusive circumstances and was in denial about her pregnancy. Many participants detailed the challenges of managing the mother's emotional needs and protecting her dignity and privacy while discreetly trying to provide care for the neonate. Attended an 18-year-old, 15 years ago that did not know or was in denial that she was pregnant. She had the baby on her own in the bathroom. The parents came home during the birth, and she was too scared to tell them and kept the baby quiet by nursing her. She called an ambulance from the bathroom and told them she didn’t want the parents to know she was pregnant as the father was a family member that had taken advantage of her. We had to sneak the baby out of house under my jacket and had a second crew attend who transported the mother… (Participant 32, Paramedic, Other North Island)
Remote and deprived communities
Another frequently cited factor that compounded concern among EMS in this study was responding to women in high-deprivation or remote parts of the country. Participants working rurally reflected on the additional challenges of high-pressure birthing situations when they were aware that access to additional resources was limited, and hospital facilities were a significant distance away. Alot of the unplanned births have happened a long way from a birthing unit and paramedic back up. While everything was ok, it was concerning that if something was serious then back up was often over an hour away. (Participant 95, Emergency Medical Technician, Other North Island)
Many also described low health literacy in some rural areas as a challenge in persuading patients to seek care or agree to be transported to a hospital. One emergency medical technician with less than three years of experience recounted the heightened emotions experienced when responding to an imminent birth in a rural part of the country, far from a birthing unit or hospital. It was their first experience with birth and was a highly confronting experience.
Theme two: Practical challenges and unsuitable environments
When asked about the challenges of providing intrapartum and neonatal care during prehospital deliveries, many participants articulated that limited equipment and unsuitable environments introduced practical challenges that exacerbated the pre-existing difficulties in the situation.
Limited equipment
The most cited concern was the lack of equipment in the ambulance to treat complicated births and neonates, particularly in cases of breeched birth, a tangled umbilical cord and a low heart rate. Many clinicians expressed concern about having limited tools in the ambulance to respond effectively in these situations, with one stating that ‘none of [their] equipment was suitable for the baby’ (Participant 25, Paramedic, South Island).
In high-risk obstetric situations, participants often had to improvise to meet the demands of the situation. Some focused on facilitating immediate skin-to-skin contact between the mother and newborn after birth. However, when the mother required urgent treatment, like in cases of post-partum haemorrhage, the limited equipment in the ambulance led participants to come up with creative solutions such as heating up the ambulance and using makeshift blankets to keep the neonate warm. Challenges with equipment was not having a blade to cut the cord. I needed to ‘chew’ through the cord with the scissors provided, which was frustrating given the patient was under CPR. Also, I wanted to keep the patient warm as the house was cold and it was winter, so I used the Gladwrap in the ambulance. The roll I had was a new one and very difficult to start up as it shredded. I ended up using the patient's industrial size wrap with a plastic blade attached. (Participant 75, Intensive Care Paramedic, South Island)
Participants also shared challenging experiences where the mother and neonate had to be driven to a birthing unit or hospital separately, necessitated by limited ambulance space. Many voiced concerns about the potential emotional impact this could have on the mother. Some working in rural settings described experiences where either the baby or mother were transported by helicopter due to the urgency of the complications they were presenting and the distance to the nearest hospital on road. This logistical challenge added an additional layer of complexity to the high-pressure situation. The midwife was coming but was approximately 45 mins away and we were based 2 hours away from a rural hospital and a birthing unit, 3 hours away from a major hospital. The contractions were 1 minute apart, and the baby was 10-days premature, so we were all feeling quite stressed. The midwife assessed the situation and asked for a helicopter to transfer the baby to NICU, she was treating it as having swallowed meconium. The baby was flown to [tertiary hospital], great for the baby but very distressing for Mum as she had to be transported by road. (Participant 34, Paramedic, Other North Island)
Unsuitable environments
Another obstacle identified by participants was providing intrapartum care in physically challenging environments such as homes with no electricity or heating and public areas. Participants described the added risks of delivering in an unplanned area such as navigating poorly lit homes for equipment they need and trying to keep the mother and neonate warm in cold winter conditions. In winter at 23:00 hours we were 20 minutes from scene and responded to an imminent birth. On arrival it was 2 degrees outside, and the front door was open. The house was cold, and the mother was standing in the bathroom with the neonate lying on the cold floor. I called for backup as the mother had a severe postpartum haemorrhage and the neonate required resuscitation. I was not sent assistance and had to manage the mother and neonate by myself during a 15-minute drive to the birth suite at hospital while the EMT drove. (Participant 25, Paramedic, South Island)
Other participants that assisted with delivery en route to the hospital voiced concerns about preserving the mother's dignity. Frequently, they found themselves needing to pull over on to the sides of busy roads, navigating the delicate balance between providing medical care while protecting the mother's privacy from bystanders. The challenge was keeping mum's dignity on the side of a busy road in [a busy suburb] … and needing to transfer to an ambulance as soon as possible, but this was difficult to do without exposing mum. (Participant 1, First Responder, North Island)
Discussion
There is a noticeable gap in the literature about the management of prehospital obstetric events by emergency management services.13,15 The aim of this study was to understand EMS’ experiences attending out-of-hospital births in NZ, with a focus on the challenges they perceived in managing these incidents. Participants described navigating diverse situations in which they had to provide intrapartum care and respond to a range of maternal and neonatal complications with limited resources and knowledge. EMS personnel described a lack of clinical information, equipment and resources to anticipate and address challenges related to delivery. Out-of-hospital births commonly occurred with patients who did not know they were pregnant or had not received antenatal care.
Providing care during labour was further complicated by a range of practical challenges, including unsuitable environments for a delivery and inadequate equipment to manage the birth and treat a newborn patient. Practical challenges were particularly concerning for clinicians in rural areas where assistance was often scarce or unavailable. Our two main themes intersected for EMS personnel working in remote locations as their heightened anxiety when faced with ambiguous and unpredictable scenarios was compounded by the awareness that access to resources such as backup crews or hospital facilities were not available at short notice.
Our findings are consistent with a small number of international studies acknowledging that the increased challenges in prehospital settings create heightened vulnerability and acuity for both obstetric patients and EMS personnel.6,16 Participants in our study encountered various challenges with birth events, including decision-making with limited clinical information, managing complicated births, navigating difficult environments and addressing practical issues due to scarce resources.
Incidences of maternal and neonatal complications are high in unplanned out-of-hospital births, and low-level obstetric risks may be exacerbated in the prehospital setting.2,15 As in previous research, 13 EMS personnel in our study frequently encountered complications and described the critical clinical skills and judgment they employed to navigate high-risk situations during out-of-hospital births. A handful of studies have reported that EMS may overlook women's emotional needs during unplanned labour 14 and misidentify risks of maternal complications by prioritising foetal concerns during assessments. 29 In contrast, participants in our study expressed concerted efforts to manage both the emotional needs of mothers and neonate physical needs through coordinated efforts between limited personnel.
While existing literature has afforded priority to prehospital care in urban areas, our study identified challenges in providing intrapartum care in rural settings within high-income countries. We also observed the events that our clinicians mostly recounted were situated in deprived and remote areas, suggesting that this is where the most challenging and impactful out-of-hospital births are happening, like previous research in Australia.6,30 Historically, discussions about these challenges have largely occurred against the backdrop of low-income countries with higher exposure to deprived economic settings and remote geography. 31
Our findings corroborate previous studies that have drawn attention to a major gap in obstetric training needed for EMS personnel, especially related to managing complications.16,17,32 However, the perspectives of EMS personnel in this study indicate the clinical focus of current training may fail to address the challenges that clinicians consider most important in the management of prehospital birth; acting with a lack of information and resources, and navigating emotionally complex and sensitive settings. Considering these findings, we have planned a second study to gain further insight from EMS about barriers and facilitators to managing birth events in the prehospital setting, and how these may be addressed or enhanced through training, changes to resourcing, or other organisational initiatives in NZ. Future research should also aim to engage stakeholders in antenatal care and ambulance resourcing to ensure that recommendations are feasible and actionable in the NZ context. Another under-researched area is the ∼5000 people a year who give birth in NZ and were not registered with a maternity carer until their third trimester or later (around 9% of births). 33 Our participant data suggests that a lack of antenatal care was common in patients in labour attended by ambulance personnel, but there is little quantitative data to understand the characteristics of people in NZ who experience unplanned out-of-hospital births, and which of them may be most at risk for poor maternal and neonatal outcomes.
Strengths and limitations
The Internet-based survey and convenience recruitment in this research enabled a large and diverse range of views and experiences with obstetric emergencies. This survey method was chosen to capture a broad range of perspectives from various geographical locations and levels of expertise, which may have been challenging to achieve through interviews due to time and location constraints. The anonymity afforded by an online questionnaire may have contributed to the detailed and candid responses to our open text questions, some of which covered sensitive topics. However, we acknowledge that our data do not represent the views of all EMS personnel that attend unplanned births in the prehospital setting and that face-to-face interviews may have allowed us to probe deeper into responses. We acknowledge that our insight into decision making processes within organisations responsible for training and for resourcing ambulance crews in NZ may influence our perspectives on what is desirable or feasible to overcome challenges identified by EMS personnel in this study.
Furthermore, we acknowledge that Māori women (the indigenous people of NZ) experience worse pregnancy and maternal outcomes including maternal mortality and suicide related to pregnancy, childbirth and postpartum experiences.34,35 As a result, their experiences and views of unplanned, pre-hospital births are likely to differ from non-Māori women, including their cultural concerns and needs. While patients’ perspectives were outside the scope of this research, our study may have benefited from intentionally exploring EMS’ experiences of providing care to Māori women and their whanau (family) during unplanned out-of-hospital births.
Conclusion
This is the first study in NZ, and one of the few worldwide, to explore EMS insights and perspectives about their experiences attending unplanned births in the prehospital setting. Although EMS staff in our study spanned a range of ages, qualifications and years of experience, most shared the perspective that unplanned births could be unpredictable and challenging events, often characterised by ambiguity and complexity both in terms of clinical presentations and environmental and social circumstances. Consistent with previous studies, participants often felt they had insufficient equipment and other resources to carry out optimal care and monitoring during the birth and postnatally. Our study also identified a lack of certainty and knowledge as being a key experience that threatened EMS’ ability to manage complex jobs and patients with confidence. Future research may explore how these factors and other concerns may be mitigated through training, education and resourcing for EMS services in NZ, with particular attention to how rural ambulance personnel and their patients could be better supported.
Supplemental Material
sj-pdf-1-pam-10.1177_27536386251345488 - Supplemental material for Ambulance personnel’s experiences with prehospital births: a qualitative study in Aotearoa New Zealand
Supplemental material, sj-pdf-1-pam-10.1177_27536386251345488 for Ambulance personnel’s experiences with prehospital births: a qualitative study in Aotearoa New Zealand by Vinuli Withanarachchie, Verity Todd, Bridget Dicker and Sarah E. Maessen in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386251345488 - Supplemental material for Ambulance personnel’s experiences with prehospital births: a qualitative study in Aotearoa New Zealand
Supplemental material, sj-docx-2-pam-10.1177_27536386251345488 for Ambulance personnel’s experiences with prehospital births: a qualitative study in Aotearoa New Zealand by Vinuli Withanarachchie, Verity Todd, Bridget Dicker and Sarah E. Maessen in Paramedicine
Footnotes
Acknowledgements
The authors would like to acknowledge the Hato Hone St John Emergency Medical Services staff who shared their experiences in this survey and provide exceptional intrapartum care during unpredictable prehospital birth events. We acknowledge Hato Hone St John for the support and resources provided during data collection and analysis.
Author contribution(s)
Declaration of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors VW, BD and SM are employed by Hato Hone St John. Verity Todd is an associate editor at Paramedicine. That author played no role in the editorial decision-making process, and the peer review of the article was conducted in adherence to the blind review policy of the journal.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research materials availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.