
Abstract
Background
Chronic pain is highly prevalent among the global population and has a significant impact on a patient's livelihood in multiple areas. Chronic pain is now more widely recognised as a standalone medical condition by most healthcare disciplines, separate from that of acute pain. This has allowed for the development of a unique evidence-based approach to caring for these patients, which incorporates the biological, psychological, and social dimensions in which chronic pain transverses. However, in the paramedic practice setting, chronic pain has received scant mention. This knowledge gap leaves many paramedics operating without guidelines suitable for the care of chronic pain patients or an epidemiological foundation describing the incidence or treatment requirements of this patient cohort. Most importantly, the perspectives and experiences of chronic pain patients who are treated by paramedics have yet to be investigated which is vital to ensure relevant care.
Aims
To describe and understand the experience of patients requiring ambulance attendance for chronic pain-related complaints.
Methods
Six participants were enlisted using convenience sampling. Participants responded, via Zoom, to an inductive, semi-structured interview. Analysis was performed using qualitative reflexive thematic analysis with a non-positivist, constructive approach.
Results
The themes identified were ‘the impact of stigma’ and ‘inadequate paramedic education’. Most participants shared similar attitudes and experiences regarding paramedic management, expressing dissatisfaction with the current standard of practice in relation to chronic pain complaints.
Conclusion
Patients experiencing chronic pain are underserved by the standard of care being offered in this practice setting. Concerns raised by patients centred around the impact both stigma and educational understanding have on treatment. These findings indicate a need for further research, including the revision of guidelines and consideration of the patient perspective to be conducted in this area.
Introduction
Chronic pain, also known as persistent pain, is a complex condition that greatly affects the quality of life of 20% to 30% of people globally. 1 Chronic pain is defined as pain that persists beyond the expected healing time, where the pain recurs or persists for more than three months.1,2 This type of pain can be the result of surgery, injury, disease or be idiopathic.1,2
The International Association for the Study of Pain updated the definition of pain in 2020 to better reflect the unique clinical course of chronic pain. 3 Historically, chronic pain was not considered a unique disease classification, and as such was often inadequately treated through models intended for acute pain. 4 Acute pain which can be explained linearly with the biomedical model is described as an unpleasant and dynamic experience, usually in response to tissue trauma and the related inflammatory process which has protective properties and survival value.3–5 Chronic pain, however, is best viewed using the biopsychosocial model which incorporates the influence of psychosocial well-being with the experience of pain, utilising interventions coordinated holistically through a multidisciplinary team of healthcare professionals (HCPs).4,6
The impact of chronic pain is vast. Chronic pain has a large economic burden due to medical costs and lost productivity. 4 Patients with chronic pain report ill-health in multiple areas (psychological, cardiovascular and pulmonary systems), which can have a detrimental impact on activities of daily living, work, sleep and interpersonal relationships.7,8
Despite its large impact, chronic pain is poorly understood and managed in non-specialist settings, such as paramedicine.9–11 A literature review of research describing paramedic management of patients experiencing chronic pain was undertaken prior to this study as a related project. The review failed to identify peer-reviewed research that investigated the patient experience of paramedic care where the chief complaint was chronic pain. In Australia (the setting for this study) during the 2017–2018 year, chronic pain accounted for over 105,000 hospitalisations and has resulted in a six-fold increase in general practitioner (GP) and emergency department (ED) presentations. 2 Despite this increased prevalence, there is no published data which states the incidence of chronic pain presentation to Australian ambulance services. 9 Only three of the eight Australian jurisdictional ambulance services include a dedicated chronic pain guideline for paramedics.12–19 Furthermore, no reference to pain management is made in the ‘Professional Capabilities for Registered Paramedics’ and the approved accreditation standards, both of which guide the tertiary level (Bachelor's degree in paramedic science as the entry-level) education of Australian paramedics.20,21 In the paramedic practice setting, patients with chronic pain are often reliant on acute pain care pathways, leaving them without evidence-based management proven to have better outcomes.3,4,9
It is unknown how this apparent lack of foundational education and guidelines for clinical practice affects patients. To address this knowledge gap, this study aims to understand and document the patient experience of paramedic care in relation to chronic pain complaints. The following research question was formulated; ‘What is the experience of patients with chronic pain who are treated by paramedics?’
Brainstorm representation from codes to themes.
Method
Design
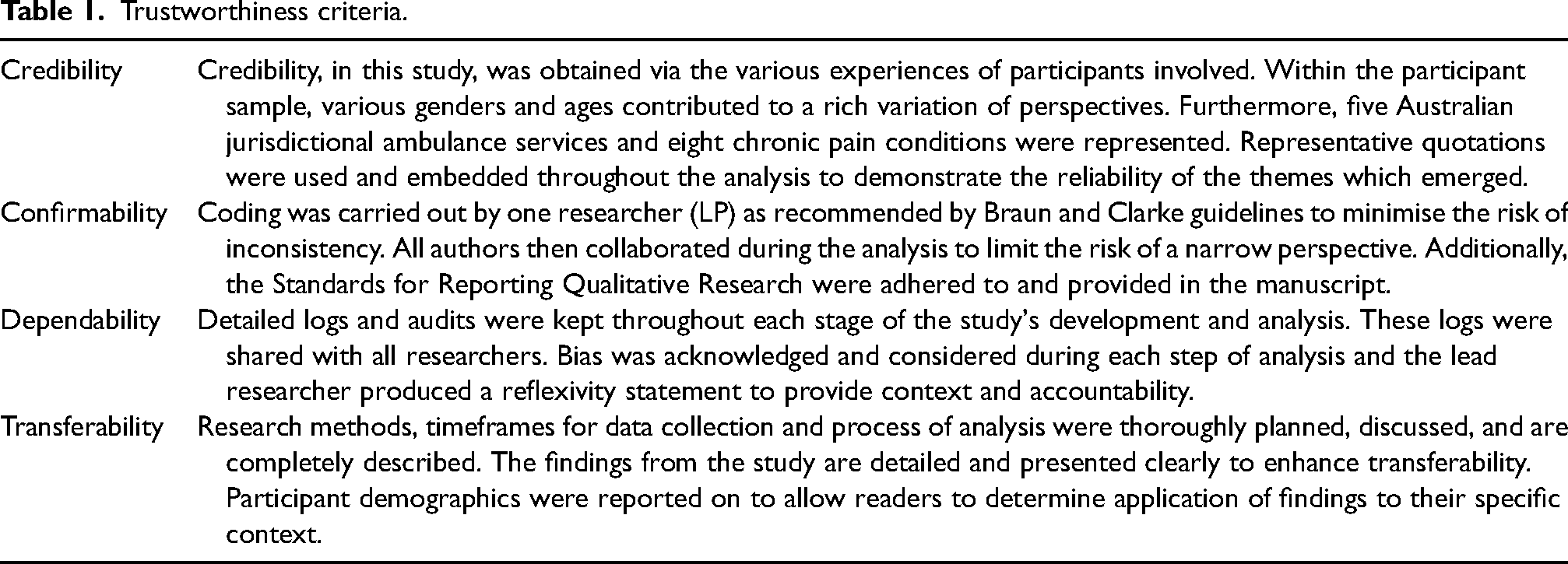
This is a qualitative study using reflexive thematic analysis (RTA) as outlined by Braun and Clarke.22,23 Analysis was conducted using an interpretivist paradigm (or ‘Big Q’ approach). 23 An interpretivist paradigm has been described as non-positivist and reflexive.22,23 A non-positivist approach was selected so that participants could express their reality through their individual experiences. 24 The philosophical underpinning was constructivism, which acknowledges that there is no single reality. 24 Rather, knowledge is constructed from individual experiences which requires an exploration of multiple perspectives, consistent with the principles of RTA.23,24 This was actioned by considering both semantic and latent codes and researcher reflexivity throughout inductive analysis of the interview transcripts. 23 Semi-structured interviews were conducted via Zoom based on an initial set of seven questions. To ensure the integrity of the study, the four criteria of trustworthiness (credibility, confirmability, dependability and transferability) and the Standards for Reporting Qualitative Research were adhered to and documented in Table 1 and Supplemental Appendix 1, respectively.25,26
Trustworthiness criteria.
Researcher perspective and reflexivity
LP – is a paramedic working in an Australian capital city with three years of career experience. She has additionally collaborated closely with people diagnosed with chronic pain in her four years of experience as a support worker in the disability sector. These factors influence the analysis in many ways. Some benefits of her experience include insight into the paramedicine side of chronic pain management. She has a foundational knowledge of paramedic practice as well as access to a wide range of resources and perspectives within the paramedicine community. On the other hand, she does not have lived experience of being diagnosed with chronic pain and is described as an ‘outsider researcher’. 24 It is appreciated that this may yield some distrust and apprehension by participants, especially those who feel they have been mistreated by paramedics. For these reasons, the research team felt RTA would be the most appropriate method to analyse the data collected. RTA allows for data to be expressed in a respectful and diligent manner which reflects the lived experience of participants and welcomes researcher influence. 23 Furthermore, all members of the research team have varied experience in the field of paramedicine, allowing for reflexivity. Researchers RL and TA are both practising paramedics with TA holding a Master's degree in the field. BL is a paramedic with decades of on-road experience. BL also holds a PhD in paramedic management of pain. Lastly, KB is the director of paramedic research at Monash University.
Interview questions
Development of the interview guide for this study began with researchers brainstorming topics and questions of interest as recommended by Braun and Clarke. 27 The main area of interest for researchers was the patient journey, beginning with exploring what prompts patients to call an ambulance, the treatment received by paramedics, the attitude and knowledge base of paramedics and the resultant outcome of ambulance attendance (transport to hospital, referral decision, and refusal of transport).
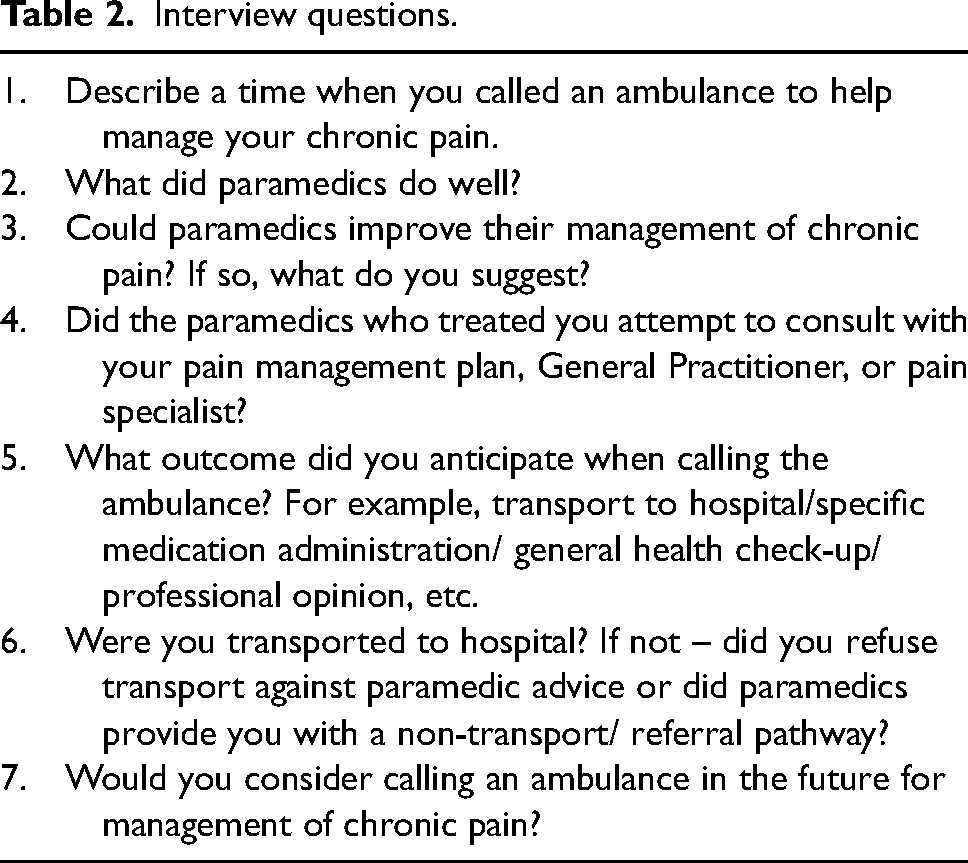
Seven questions were selected for use in the interviews (see Table 2). The opening and closing questions were considered to bookend the patient's journey. 27 Questions were presented in a semi-structured format. The interview questions were designed to initiate open discussion rather than facilitate a deductive analysis of the narratives based on the researcher's prior hypothesis relating to the outcomes of interest. 27 Questions that followed from the opening set reflected the principles of RTA, which requires the interviewer to be responsive to the interviewee's accounts of their experiences rather than strictly adhering to a predetermined script. 27 Most questions were open-ended, allowing for follow-up by the researcher and participant. When yes/no questions were used, they established a topic of discussion (improving management/holistic approach/transport decisions), going on to then facilitate dialogue between researcher and participant. For example, the yes/no question of ‘Were you transported to hospital?’ had immediate follow-up by the researcher regarding what transport disposition was utilised by paramedics (hospital, referral, or refusal) and enabled the participant to describe their experience or attitude towards the outcome. Furthermore, follow-up questions were used in question 4 asking participants if they felt paramedic consultation was beneficial (if answered yes) or would potentially be beneficial (if answered no). No participants interviewed gave single-word responses to the questions asked.
Interview questions.
Sampling strategy
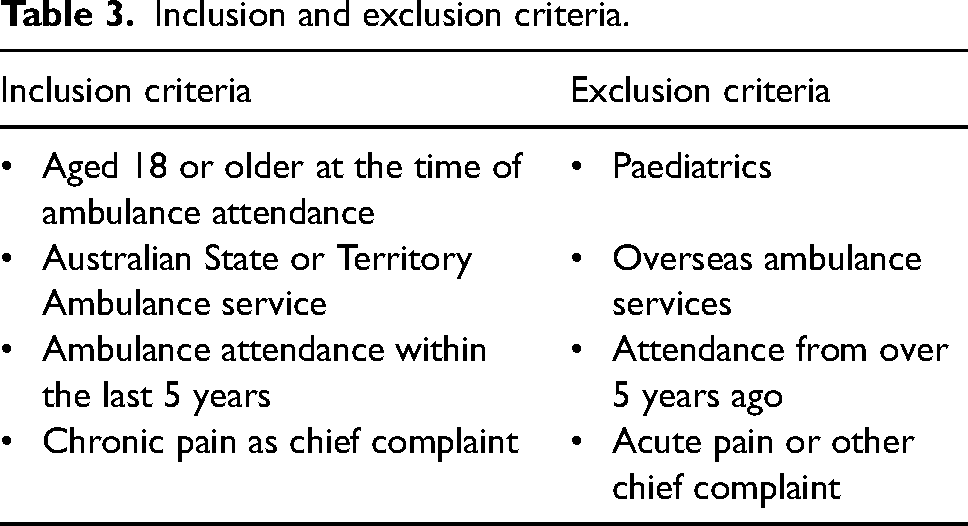
Participants who received management from Australian paramedics in the last five years for chronic pain as their chief complaint were eligible to be included in the study. A five-year window was pragmatically selected to allow participants to recount what was important to them during their episode of care, in line with current standards of practice. As this study is focused on the patient experience as opposed to intricate aspects of each call-out, there is less pressure on the issue of recall bias. 28 The setting for this study is Australia. In Australia, each State and Territory has its own ambulance service funded by the relevant state or territorial government. While all Australian paramedics are registered under the Australian Health Practitioner Regulation Agency, each service has its own unique guidelines and operational procedures. 29 To be included in this study, participants were able to have received care from any jurisdictional ambulance service, demographics of each service provider were recorded to further account for potential differences in experience. Convenience sampling was used to recruit participants in this study. Suitable participants were identified through ‘expression of interest’ flyers disseminated by Chronic Pain Australia and the Australian Pain Management Association, peak-body advocacy groups for chronic pain patients in Australia. This strategy was used to minimise potential researcher influence on the sample. 27 Snowball sampling then supplemented the original recruitment as the flyer was then shared and redistributed on social media to other chronic pain support groups. Prospective participants were directed from the flyer to a survey using Qualtrics software via a Quick Response code. The survey screened participants against inclusion and exclusion criteria (Table 3). Suitable participants were then contacted via email. To verify participants, researchers allowed individual participants to identify themselves as living with chronic pain and define chronic pain as the main reason for ambulance attendance in their own subjective terms. 27
Inclusion and exclusion criteria.
Data collection and processing
Interviews were conducted with participants from August to October 2022 by researchers LP and RL. Participants were invited to relay their lived experiences of paramedic attendance during a chronic pain episode. The duration of interviews ranged from 14 to 45 min and averaged 22 min. Braun and Clarke argue that, unlike some other methods of qualitative enquiry, data saturation is not a relevant concept in RTA as coding cannot reach a fixed endpoint based on the number of interviews. 30 Instead, the interviewer applies judgements about the coding endpoint, and the need to recruit additional participants, based on their interpretive analysis of the data arising from their contextual and theoretical focus. 30
All interviews were conducted via the video-conferencing platform ‘Zoom’. Audio and video from the interviews were recorded and the ‘auto-transcribe’ function on Zoom was used. Interview footage was watched by two researchers (LP and RL), and transcripts were de-identified and checked for accuracy against the auto transcript.
Data analysis
Data analysis for this project followed the six phases of RTA as outlined by Braun and Clarke.22,23 Following familiarisation via watching/rewatching and transcribing interviews, initial coding was undertaken by one author (LP). Coding was done manually by highlighting features of interest and utilising an inductive approach to derive themes from the dataset itself.22,23 Reflexivity was an ongoing consideration throughout coding. Codes interpreted remained relevant to the research question which centred around the current experience of patients and the potential for paramedics to improve in this area. Codes were exported into a colour-coordinated table. Codes were then refined before being reviewed by and discussed with a second author (TA) to confirm that the codes generated were reflective of the data obtained. Larger patterns in the codes were identified and then grouped into meaningful themes and subthemes. Themes were mapped using an illustrative brainstorm incorporating the colour-coordinated codes.
Ethics
Ethics approval was obtained from the Monash University Human Research Ethics Committee (MUHREC) reference #32237. Written informed consent was obtained from all participants prior to interviews.
Results
In total six participants completed interviews. The demographic characteristics of all participants are summarised in Table 4. Participants ranged in age from 31 to 60 years and were seen by paramedics from five different jurisdictional ambulance services. The diagnoses aligned with the chronic pain were diverse.
Demographic characteristics of participants.
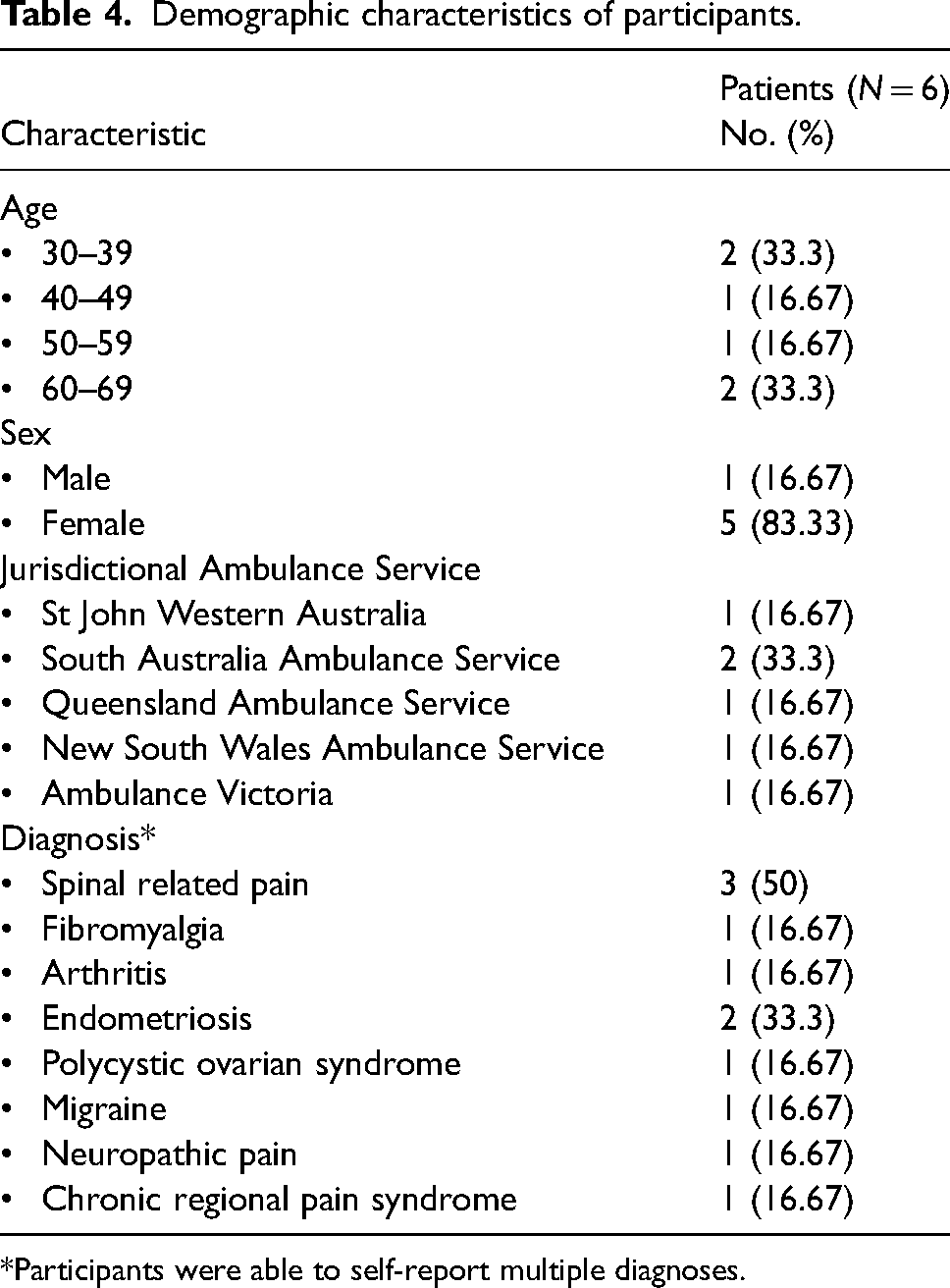
*Participants were able to self-report multiple diagnoses.
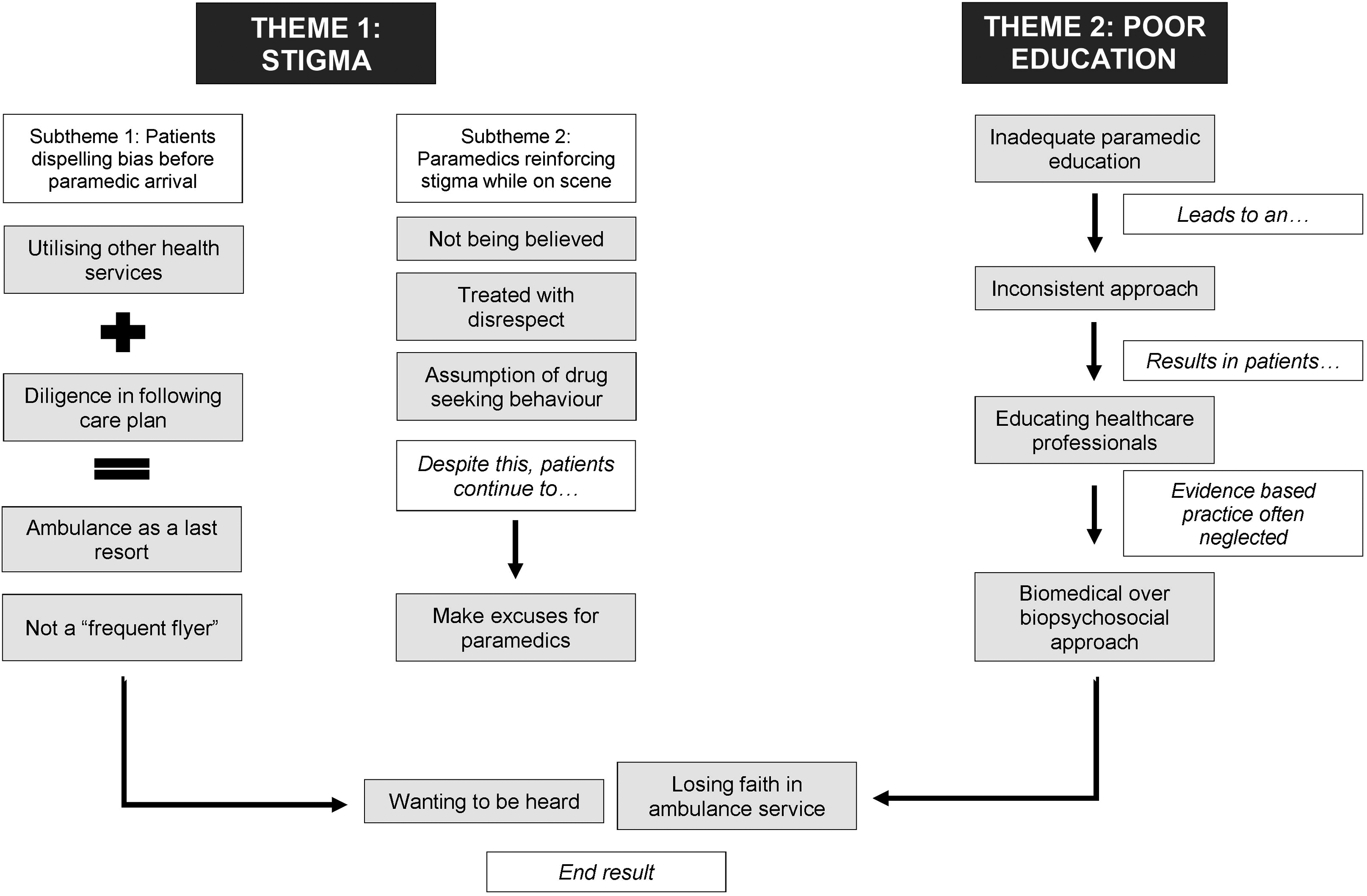
Two overarching themes were identified: patient experience of stigma and inadequate paramedic education (see Figure 1).
Theme 1: Patient experience of stigma
A key theme which featured across all interviews was the notion of stigma. Participants report arduously doing the groundwork to reduce stigma prior to paramedic arrival only to report the reinforcement of bias by paramedics while on scene.
Subtheme 1: Attempts to dispel stigma by patients
All participants described awareness of the stigma by healthcare professionals towards those living with chronic pain. Most participants assumed paramedics would arrive at their call-out harbouring some preconceived biases regarding their chronic pain. Some participants attribute this to previous interactions with paramedics (P01, P03, and P04) while others describe it as the result of interactions with other settings (P02 and P04) such as taking a long time to get a diagnosis and treatment by a triage/ED staff.
Participants consistently stated they only used ambulance services as a last resort to distance themselves from the bias that they are ‘frequent flyers’. Participants describe apprehension in the decision to call an ambulance even after exhausting all other available resources such as family/friends, taking prescribed medication and visiting non-emergency healthcare settings. Most participants interviewed state they’ve only called ambulances two or three times in the past year. It's when I’ve got to a point where I have done all the things I’m supposed to do. All the things that are prescribed by my GP and my pain doctors, and it's just beyond my capability of trying to solve this particular problem. (P04) If I can’t move as a single parent, I can’t do that to my kids… I have to call, it's a last resort. I have no one who can move me. If my legs are out, I can’t drive myself, I can’t get in an Uber, it's truly a last resort. (P05)
Participants described diligence in following their prescribed pain plan and reported that they regularly engaged with numerous other healthcare providers to manage their chronic pain. These detailed and patient-specific care plans involve strict medication regimes and appointments with multidisciplinary teams composed of GPs, pain specialists, physiotherapists, and psychologists. To me my first response is always my primary care providers, GP, physiotherapists, exercise physiologist and pain specialists. They’re the best to go to and then from there, if I can’t get myself out of the home or mobilise myself, then it's hospital. (P06) I have a flare management plan. It's sort of like, if my pains flaring, we do this medication, then this one, you know. I’ll move for a bit, stretch, turn up my spinal cord stimulator. Then take a bit more Palexia, I might do an anti-inflammatory injection or a ketamine lozenge. That sort of stuff, and if that's not settling, then it has to be Emergency Department. (P05)
One participant described calling a 24/7 at-home doctor service during a chronic pain flare-up. Despite attempting to engage with a non-emergency service, an ambulance was arranged for them anyway.
Subtheme 2: Stigma reinforced by paramedics on scene
After the difficult decision to call an ambulance had been made, participants described their pain as being viewed sceptically by paramedics. This scepticism is noted to have many consequences including feelings of humiliation and embarrassment, perceived impact on the provision of analgesia, ease of communication and overall satisfaction.
Across all interviews, the most common shared experience between participants was the assumption by paramedics that they were ‘drug-seeking’. Participants described feelings of relief and reassurance at paramedic arrival. However, when it is surmised that they are ‘drug-seeking’, participants recounted those initial feelings being replaced by apprehension. They described having to state and justify their requirement for paramedic attendance, rather than being viewed as patients requiring healthcare. One participant recalled paramedics ‘instantly’ asking ‘what medication are you seeking’ when revealing their chronic pain diagnosis (P05). Another participant described ‘snarky’ comments made by paramedics while looking through their medication list (P04). Similarly, one participant stated that they feel an ‘attitude shift’ by paramedics once their chronic pain history is disclosed (P06). The same participant described the attitude shift affecting the quality of their care by paramedics. It doesn’t seem to matter how much [pain medication] I take, or if I’ve had it that day or not. Once they find out you’re on short acting pain medication, they’re not really all that interested in settling down your pain and getting you stable before moving you; they just sort of man-handle you. (P05)
Participants also described paramedics not believing their report of pain during assessment and management. Comments such as ‘they didn’t believe me’ were repeated consistently across interviews.
Two participants described the same looks they have received from paramedics on occasions when they felt they have not been believed. ‘There's a look that they get between the two partners’ and ‘they have these side glances between you and the hospital staff and themselves’. (P05 and P03)
Theme 2: Inadequate paramedic education
Another key theme identified was the impact of inadequate paramedic education. Participants described experiences where paramedics seemed to be unaware of the pathophysiology, pharmacology, and evidence-based management of chronic pain. This led to what patients described as ineffective management and left patients devising their own educational handouts for when paramedics attended them to fill in the gaps of knowledge.
Some participants were under the impression that Australian paramedics were more educated on chronic pain during their training. Multiple participants were aware that most Australian paramedics are educated to a university standard and expressed a desire for expansions to their training including chronic pain education. Now that universities are involved with the training of paramedics, they can actually study chronic pain just like all the GP's and everyone else is expected to. A subject on pain management. (P04)
Two participants referenced the intricacies and differences of chronic pain, in comparison with acute pain as reasons why paramedics should be educated on the subject. Participants also expressed a desire for principles consistent with a holistic, biopsychosocial approach to be used by paramedics. One participant stated it would have been beneficial if paramedics employed ‘stress reduction techniques’ (P01) while another hoped that future paramedics would be trained on the ‘psychology of chronic pain’ and the significant impact it has on their daily life (P05). Another participant stated despite the complexities surrounding chronic pain management, even in the tertiary hospital setting, paramedics should be better equipped to recognise the condition in their practice. But when it comes to paramedics, they find it hard to recognise, there's not always an obvious sign… I do have some empathy, it's not an easy thing to treat, even on the wards. (P05)
A common experience expressed by participants was having a ‘cheat-sheet’ ready for when paramedics arrived. Participants stated that at the time of paramedic attendance, they were in too much pain to effectively communicate fundamental educational information to paramedics, so a pre-prepared document was necessary as, in their experience, paramedics lacked awareness regarding their condition. Participants described preparing histories on the basic definitions, pathophysiology, and evidence-based management principles for paramedics to review. These histories were described to be available as printed documents or phone apps, ready for paramedic arrival. Participants stated this was to supplement – the knowledge gaps they had come to expect from paramedics, ensuring appropriate care.
Almost all participants described vast inconsistencies between paramedics on different occasions ambulances attended them. Participants stated that the mixed experiences went beyond normal variances expected between callouts and had a great impact on medication administration, transport, and the overall level of care.
One participant recounted two juxtaposing experiences in management by paramedics for their chronic pain (P05). On one occasion they were treated respectfully and felt as though their chronic pain was medicated appropriately by paramedics. The other experience left the patient feeling judged and as though their pain was not ‘settled down’. This participant questioned whether the more positive experience was the result of being attended to by a critical-care paramedic, a more senior practitioner who has had more formal education than a paramedic with less clinical experience. The participant stated the critical-care paramedic seemed to have knowledge of higher-order concepts such as drug tolerance versus drug dependence and the psychosocial nature of chronic pain. Many participants stated they felt the paramedic approach would be more consistent if there was a standardised education on holistic pain management during paramedic training. You do find some lovely paramedics who are open, who don’t have that judgement or bias, who have seen something similar to this – but you don’t know who you’re going to get, the education level… I would not call again unless there was further training. (P03)
Discussion
This study explored the experience of patients who are treated in the paramedic practice setting for chronic pain-related presentations. Two connected themes were identified which gave insight into the patient experience and largely voiced feelings of dissatisfaction and hesitancy by participants. It was found that participants felt underserved by the level of care provided by Australian paramedics in relation to their chronic pain. For most participants, although necessary, paramedic attendance resulted in a negative experience. To the author's knowledge, this is the first qualitative study investigating the experience of patients suffering from chronic pain who are cared for by paramedics.
Participants described carrying the weight of stigmatising interactions with paramedics. As a result, participants adjusted their behaviour in the hopes of dispelling bias for future encounters. Up to 38% of people affected by chronic pain experience internalised stigma – this stigma may be shaped by other experiences with HCPs outside the paramedic profession and may influence and shape future perceptions of paramedic encounters. 31 Stigma attached to chronic pain patients has been well documented in literature on healthcare settings outside paramedicine including medical clinics and emergency departments.32–34 This stigma, which is rooted in multiple areas, is evidenced by patients who experience it and HCPs who perpetuate it.32–34 The application of the biomedical model in the assessment and management of chronic pain has been linked with HCPs' dismissal of a patient's self-report of pain. 35 Viewing chronic pain under the same lens as acute pain leads to HCPs questioning the validity of a patient's pain in the absence of ‘a clear basis in tissue pathology’, stigmatising a patient's experience as imagined.34,35 Additionally, chronic pain patients ubiquitously report feeling as though providers assume them to be ‘drug-seeking’ without sufficient evidence.36,37 This stigma impacts the provider–patient relationship and has been linked to communication breakdown, the ‘underassessment and underestimation of pain’ and poorer physical and psychological well-being of patients.34,35 Although there is little published literature on paramedics succumbing to this stigma in their management of chronic pain, evidence from one study shows paramedics are less likely to offer analgesia to patients with chronic pain. 38 Some studies suggest that chronic pain is associated with frequent use of emergency healthcare services.39,40 Participants in this study describe awareness of this correlation and express this as stigmatising and a barrier to optimal care. This echoes the sentiment expressed by participants in other studies who stated they only attended emergency departments to manage their chronic pain when they had ‘no other choice’.11,41
Theme 2 explored participants’ frustration in relation to the lack of paramedic education on chronic pain. While research shows that the education of HCPs on evidence-based chronic pain assessment and management is linked to improved patient outcomes, paramedic-specific resources and guidelines are scarce.42–44 As described above, many ambulance service guidelines and standards set for paramedic education neglect to include chronic pain.12–19 The inclusion of a dedicated chronic pain guideline in the paramedic practice setting has been achieved elsewhere. The Joint Royal Colleges Ambulance Liaison Committee (JRCALC) guideline used by paramedics in the National Health Service (United Kingdom) includes thorough, evidence-based models of assessment and care of patients with chronic pain. 45 JRCALC references the biopsychosocial model, a multifaceted approach and the unique pathophysiology and pharmacology of chronic pain. 45 Inclusion of guidelines for the assessment and care of patients with chronic pain by ambulance services may ease the burden on patients to educate and inform HCPs and influence the stigma experienced by patients. Furthermore, targeted interventions that have been shown to help health professionals recognise and control for potential effects of cognitive and affective bias on decision-making are recommended to improve the assessment and care of individuals experiencing pain, including chronic pain.
Clinical implications of findings
During interviews, participants clearly articulated their desire to be listened to. These feelings can be attributed to the misunderstandings and preconceived notions they were subjected to by paramedics in their interactions. These findings highlight the potential benefit chronic pain patients could experience through further research, including the incidence of presentations of this cohort to ambulance services and paramedic perspectives on education and training being conducted in this area. Additionally, a revision of some jurisdictional ambulance guidelines is warranted so they reflect standards of evidence-based practice, including incorporation of the biopsychosocial model. Pedagogical tools have been developed to support the teaching of biopsychosocial concepts in health education settings. 46 This alternative model to the historical biomedical focus of illness and disease is also relevant to other areas of paramedic practice, and as such this approach to understanding the patient's experience of their health status should be embedded in paramedic curricula. This would be benefited by being coupled with enhanced paramedic education at the university level. This education would ideally incorporate in its design and delivery, the perspectives of patients with extensive, first-hand experience of chronic pain. 47 The integration of patients’ lived experiences in formal education has been shown to improve patient outcomes and service delivery by opening communication between parties, addressing power imbalances, and building trust. 47 These actions would help to address concerns raised by participants in this study.
Limitations
Due to the underrepresentation of chronic pain in paramedicine, there was limited access to a defined population of patients experiencing chronic pain who present to ambulance services. Nevertheless, the six participants recounted experiences that revealed consistent themes throughout the interview process.
While there is no clear guidance on the optimal length of an interview using this study method, it is acknowledged that more themes may have been coded if the participants engaged in longer interviews providing further understanding. The research team felt the experiences shared through the interviews yielded great insight, and participants, regardless of interview duration consistently repeated similar experiences.
The sample of participants also lacked gender diversity with the recruitment of only one male participant. Although chronic pain affects females at a higher rate than males, this sample size is not representative of the general population. Future research should make recruiting more participants, especially males and diverse populations, a key priority.
Interviews were conducted using the video-conferencing application ‘Zoom’. Using Zoom had many strengths including enabling researchers to interview geographically dispersed participants. However, some research has indicated that while conferencing apps like Zoom are often preferred by participants in comparison with email or telephone interviews, many participants would prefer to conduct face-to-face interviews, citing technological difficulties and rapport-building. 48 Acknowledging this, researchers gave detailed instructions on how participants could access Zoom and allowed participants to voice any difficulty or apprehension they had in accessing or using the application for the interviews.
Logistical challenges associated with the recruitment of participants led to a decision not to pilot the interview questions with people who met inclusion criteria. Instead, face and content validity were assessed by the authors who have experience in pain management research and qualitative research in the paramedic practice setting.
Conclusion
Chronic pain is a complex disease process which transverses biological, psychological, and social dimensions of well-being. Management of chronic pain can be complex; however, effective management of chronic pain has been shown to improve overall patient satisfaction, quality of life and management of pain. In this small study, we have identified opportunities for improvements in the care of patients experiencing chronic pain. Ingrained notions of bias and stigma coupled with an incomplete education on the holistic nature of pain are leaving some patients reluctant to call ambulances in the future. The development of evidence-based guidelines should be explored to help address concerns raised by the accounts provided in this study, improving the overall patient experience.
Supplemental Material
sj-docx-1-pam-10.1177_27536386231220966 - Supplemental material for Chronic pain in the paramedic practice setting – a qualitative study of patients’ perspective
Supplemental material, sj-docx-1-pam-10.1177_27536386231220966 for Chronic pain in the paramedic practice setting – a qualitative study of patients’ perspective by Lucinda Peacock, Rachel Lewandowsky, Kelly Ann-Bowles, Bill Lord and Tim Andrews in Paramedicine
Footnotes
Acknowledgements
The authors are thankful to all participants who kindly gave their time and voices to this project.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Kelly-Ann Bowles is an editor of Paramedicine.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.