
Abstract
Objective:
This study aimed to adapt and validate the Arabic version of the American Shoulder and Elbow Surgeons (ASES) Standardized Shoulder Assessment Form for assessing shoulder disabilities in the Libyan-Arab population.
Methods:
A cross-sectional study design was employed, involving 108 participants with shoulder conditions from rehabilitation centers in Misrata, Libya. The ASES form underwent translation and cultural adaptation following established guidelines, including forward translation, synthesis, back-translation, expert review, and pilot testing. Psychometric validation included assessments of reliability, convergent and discriminant validity, and agreement using Cronbach’s α, Intraclass Correlation Coefficient (ICC), and Bland-Altman analysis.
Results:
The Arabic ASES form demonstrated excellent internal consistency (Cronbach’s α = .90) and high test-retest reliability (ICC = 0.95). Convergent validity was confirmed by significant correlations with the DASH (r = −.867, P < .001), ADL (r = .522, P < .001), VAS (r = −.480, P < .001), and SF-MPQ (r = −.554, P < .001). Discriminant validity was supported by weak, non-significant correlations with unrelated constructs such as self-efficacy, sleep quality, and stress. Bland-Altman analysis indicated minimal systematic bias between repeated measurements.
Conclusion:
The Arabic ASES form is a reliable, valid, and culturally appropriate tool for evaluating shoulder disabilities in Arabic-speaking populations, particularly in Libya. Its cross-cultural validation supports broader applicability across diverse Arabic-speaking contexts, enhancing clinical and research utility.
Keywords
Introduction
Shoulder pain and dysfunction are among the most common musculoskeletal complaints worldwide, significantly impacting individuals’ quality of life and their ability to perform daily activities. 1 Epidemiological studies estimate that the lifetime prevalence of shoulder pain ranges from 7% to 26%, with higher rates observed in older adults and populations engaged in repetitive overhead activities. 2 This condition is a major contributor to disability, with approximately one-third of all consultations in primary care settings attributed to shoulder problems. 3 Furthermore, patients with shoulder conditions often return for repeat consultations, increasing the burden on the public healthcare system. 4
To reduce the impact of shoulder injuries on individuals and society, it is essential to optimize the quality and duration of rehabilitation and prevention programs. Evidence supports the effectiveness of various physiotherapy approaches in shoulder rehabilitation. 5 Physiotherapists commonly use measurement tools before, during, and after treatment to plan and evaluate rehabilitation programs. Functional assessments are a key method for measuring the effects of musculoskeletal injuries on an individual’s life. 6 While assessments often focus on muscular strength and joint range of motion, these metrics have limited correlation with functional status in activities of daily living (ADLs) and work-related tasks. 7 Over the past decades, numerous questionnaires have been developed for functional shoulder evaluation. A systematic review by Aldon-Villegas et al 8 identified 32 validated functional assessment scales specific to shoulder problems. Of these, the American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form (ASES) emerged as one of the most widely used shoulder outcome tools in clinical practice and research. 9
The ASES Standardized Shoulder Assessment Form has been shown to be a reliable, valid, and responsive tool for evaluating shoulder function and pain.10 -12 Originally developed in English, the ASES form has undergone numerous translations and cultural adaptations to facilitate its use across diverse linguistic and cultural contexts, including Italian, 13 Portuguese, 11 Dutch, 14 Greek, 10 Chinese, 15 and German populations. 16 Each adaptation has demonstrated the importance of tailoring the instrument to the unique cultural and clinical settings of the target population.
In the Arab world, the first Arabic adaptation of the ASES form was developed and validated by Yahia et al 17 in Tunisia. While their study provided an essential step in introducing this standardized assessment to Arabic-speaking populations, its generalizability to other regions, including Libya, remains uncertain. The cultural, linguistic, and healthcare system differences between Tunisia and Libya may limit the applicability of the Tunisian-dialect version in the Libyan context. Yahia et al 17 themselves acknowledged several limitations in their study, including limited generalizability of their findings to broader Arabic-speaking populations. This gap highlights the need for a more comprehensive evaluation of the ASES form within other Arabic-speaking contexts to ensure its reliability and validity across the Arab world.
Previous research on cultural adaptations of the ASES form in non-Arabic languages has emphasized the necessity of robust psychometric evaluation. For example, the German version demonstrated strong reliability (α = .90) and validity through correlation with the Disabilities of Arm, Shoulder and Hand (DASH) scores, underscoring its suitability for German-speaking populations. 16 Similarly, the Greek version highlighted the importance of test-retest reliability using intraclass correlation coefficient between initial assessment and reassessment of the ASES score. 10 Furthermore, the Brazilian version of the ASES recommended using the Bland-Altman plot as a visual method to assess measurement stability across two measurement time points. 11 These studies provide a framework for developing a culturally adapted version of the ASES form tailored to the Arabic unique cultural context.
This study aims to perform cross-cultural adaptation and psychometric validation of the ASES form for the Libyan-Arab population. Adapting the ASES to the Libyan-Arabic context will contribute to the growing body of evidence supporting the ASES form’s universal applicability and ensure that Libyan healthcare professionals and researchers have access to a reliable, valid, and culturally appropriate tool for assessing shoulder disabilities. This will enhance the quality of patient care and facilitate better integration of Libyan findings into the global literature on musculoskeletal disorders.
Methods
Study Design
This study employed a longitudinal observational design to translate, culturally adapt, and validate the Arabic version of the ASES form for use in the Arab population. The study involved translation and cultural adaptation of the ASES form, followed by psychometric validation, including assessments of reliability, validity, and applicability. Ethical approval was obtained from the researchers’ institutional review board, and all participants provided written informed consent prior to participation.
Translation and Cultural Adaptation
The translation process started after obtaining written permission from the American Shoulder and Elbow Surgeons Society, the original ASES developers.18,19 The translation and adaptation procedure followed established guidelines for cross-cultural adaptation of self-report measures. 20
Translation: The original English version of the ASES form was translated into Arabic by two independent bilingual translators familiar with medical terminology.
Synthesis: A synthesized Arabic version was developed through consensus between the translators.
Back-Translation: The synthesized version was back-translated into English by two independent translators blinded to the original scale.
Expert Review: A panel of healthcare professionals, including two musculoskeletal physiotherapists, an orthopedic surgeon, and a linguist, reviewed the pre-final Arabic version for semantic, cultural, and conceptual equivalence. Any disagreement between the translations was resolved by consensus of the expert review committee members.
Pilot Testing: The pre-final version was tested on a sample of 10 participants with shoulder disabilities to ensure clarity, comprehensibility, and cultural relevance. Minor adjustments were made based on feedback on item 7 of the form.
Psychometric Validation
Participants
A total of 108 participants with shoulder disabilities were recruited from outpatient rehabilitation centers in Misrata city, Libya. Eligible participants were Arabic-speaking adults aged 18 to 70 years, clinically diagnosed with shoulder conditions such as rotator cuff tears or frozen shoulder. The diagnosis was confirmed through physical examination and patient referrals. Participants were required to complete the self-reported ASES form and provide informed consent. Exclusion criteria included systemic conditions affecting shoulder function (eg, rheumatoid arthritis), shoulder surgery within the past 2 years, or cognitive or communication impairments that could interfere with questionnaire completion.
Sample Size Estimation
The sample size for this study was calculated based on the guidelines for psychometric validation studies, ensuring sufficient power to assess reliability and validity metrics. For reliability testing, an intraclass correlation coefficient (ICC) of at least .90, with a precision of ±.10, a confidence level of 95%, and 2 repeated measures, was targeted. Using Bonett’s formula for ICC sample size estimation, 21 a minimum of 51 participants was required. To ensure robust assessment of convergent and discriminant validity, additional considerations were made to include at least 5 to 10 participants per item in the ASES questionnaire, leading to a minimum requirement of 100 participants for both reliability and validity analyses. 22 Accounting for potential dropouts or incomplete data, we collected data from 108 participants.
Data Collection
Demographic data, including age, sex, marital status, education, occupation, and injury type and location, were collected. Participants also completed the Arabic ASES form, along with validated questionnaires, as outlined in the subsequent section.
The American Shoulder and Elbow Surgeons (ASES) Questionnaire
The ASES form is a widely used self-report tool designed to assess shoulder pain and functional status. 19 It consists of 2 sections: the first focuses on pain intensity, measured using a 10 cm Visual Analog Scale (VAS), with scores ranging from 0 (“no pain”) to 10 (“worst pain imaginable”). The second section evaluates functional ability in 10 daily activities (ADL), such as putting on a coat and lifting objects. Each activity is rated on a 4-point Likert ordinal scale (0 = “unable to do,” 1 = “very difficult,” 2 = “somewhat difficult,” 3 = “not difficult at all”). The total ASES score ranges from 0 to 100, with higher scores indicating better shoulder health and less pain. The total score can be calculated using the following formula:

The Disabilities of the Arm, Shoulder, and Hand (DASH) Questionnaire
The DASH is a validated questionnaire designed to measure upper extremity disability and symptoms. 23 The QuickDASH, a shortened version with 11 items, was utilized in this study. Participants rated their ability to perform daily tasks (eg, opening a jar, pushing open a heavy door) and the severity of symptoms (eg, pain, tingling) on a 5-point Likert scale (1 = “no difficulty” to 5 = “unable to do”).
The QuickDASH score was calculated by summing responses, adjusting for up to 1 missing item, and transforming the score to a 0 to 100 scale, with higher scores indicating greater disability. Known for its reliability and sensitivity to changes in upper limb function, the QuickDASH is a practical and efficient tool, validated in numerous populations for assessing functional impairments. 24
Activities of Daily Living (ADL) Scale
The ADL scale was used to assess participants’ functional independence in performing basic self-care activities. The scale evaluates 6 domains: bathing, dressing, toileting, transferring, continence, and feeding. Each item was scored using a modified response format tailored to the Arabic version (0 = “dependent,” 0.5 = “partially independent,” 1 = “completely independent”). 25 The total score, calculated by summing individual item scores and converting to a percentage, ranged from 0 to 100, with lower scores indicating greater dependence.
Short-Form McGill Pain Questionnaire (SF-MPQ)
The SF-MPQ was used to assess pain intensity and quality. This validated tool includes 15 descriptors divided into sensory and affective components, rated on a 4-point scale (0 = “none” to 3 = “severe”). 26 Additionally, it includes a Present Pain Intensity (PPI) index, rated on a 6-point scale (0 = “no pain” to 5 = “excruciating pain”). We used the Arabic version, previously developed and validated among musculoskeletal patients, with good reliability and validity indicators (Cronbach α = .74). 27
Perceived Stress Scale (PSS-10)
The PSS-10 measures participants’ perceived stress over the past month, focusing on feelings of unpredictability and lack of control. 28 This 10-item scale uses a 5-point Likert format (0 = “never” to 4 = “very often”), with total scores ranging from 0 to 40. Higher scores indicate greater perceived stress. The validated Arabic version was used in this study with a Cronbach’s α of .74. 29
PROMIS Sleep Disturbance Scale
The PROMIS Sleep Disturbance Scale (short form, version 8b) was utilized to assess sleep quality and disturbance. 30 Participants rated their experiences over the past 7 days on 5-point scales (eg, 1 = “never” to 5 = “always”). The validated Arabic version (Cronbach’s α = .70) was used in this study. 31
Self-Efficacy 6-Item Scale (SE6S)
The SE6S, based on Bandura’s Social Cognitive Theory, evaluates participants’ confidence in managing health-related challenges. 32 Each of the 6 items is rated on a 10-point scale (1 = “not confident” to 10 = “totally confident”). The validated Arabic version (Cronbach’s α = .79) was used in this study. 33
Quality Assurance
To address potential sources of bias, the study employed a rigorous translation and cultural adaptation process for the ASES form, including forward translation, synthesis, back-translation, expert review, and pilot testing to ensure semantic and cultural equivalence. An interdisciplinary expert panel minimized individual biases, while pilot testing on a representative sample addressed ambiguities. Psychometric validation involved comparisons with validated instruments (eg, DASH, VAS), enhancing construct validity. Clear inclusion and exclusion criteria ensured a homogeneous sample, reducing confounding variables, while robust data analysis techniques, such as Bland-Altman analysis confirmed reliability and minimized systematic measurement bias.
Data Analysis
Descriptive statistics were used to summarize demographic and clinical characteristics of the study sample. Cronbach’s α was used for internal consistency, and values above .70 were considered acceptable. Test-retest reliability was assessed using Intraclass Correlation Coefficient (ICC) values using a 2-way mixed-effects model, ranging from 0 to 1. 34 A value of 1 indicates perfect reliability, while thresholds classify reliability as very high (0.90-0.99), high (0.70-0.89), moderate (0.50-0.69), low (0.26-0.49), and negligible (0.00-0.25). 35
Convergent validity was assessed by examining correlations between the ASES form and DASH, VAS, SF-MPQ, and ADL using Pearson’s r. Correlations were considered statistically significant when correlation coefficient values were >.40 and P-values <.05. 36 Discriminant Validity, which refers to correlations with unrelated constructs, including self-efficacy, sleep quality, and stress, were assessed to confirm that the ASES form measures shoulder-specific constructs without overlap. Weak correlations (r < .30) were anticipated.
Lastly, a Bland-Altman plot was used to evaluate the absolute agreement and detect systematic bias between the 2 assessments. This analysis visually displayed the agreement between test occasions (time 1 and time 2), aiding in identifying outliers. The 95% limits of agreement of the mean difference was used to assess systematic bias, with zero within the CI indicating no significant bias between measurements. 37 The 95% limits of agreement (LOA) examined natural variation over time, with narrower LOA indicating greater stability. 38
Results
Demographic Characteristics
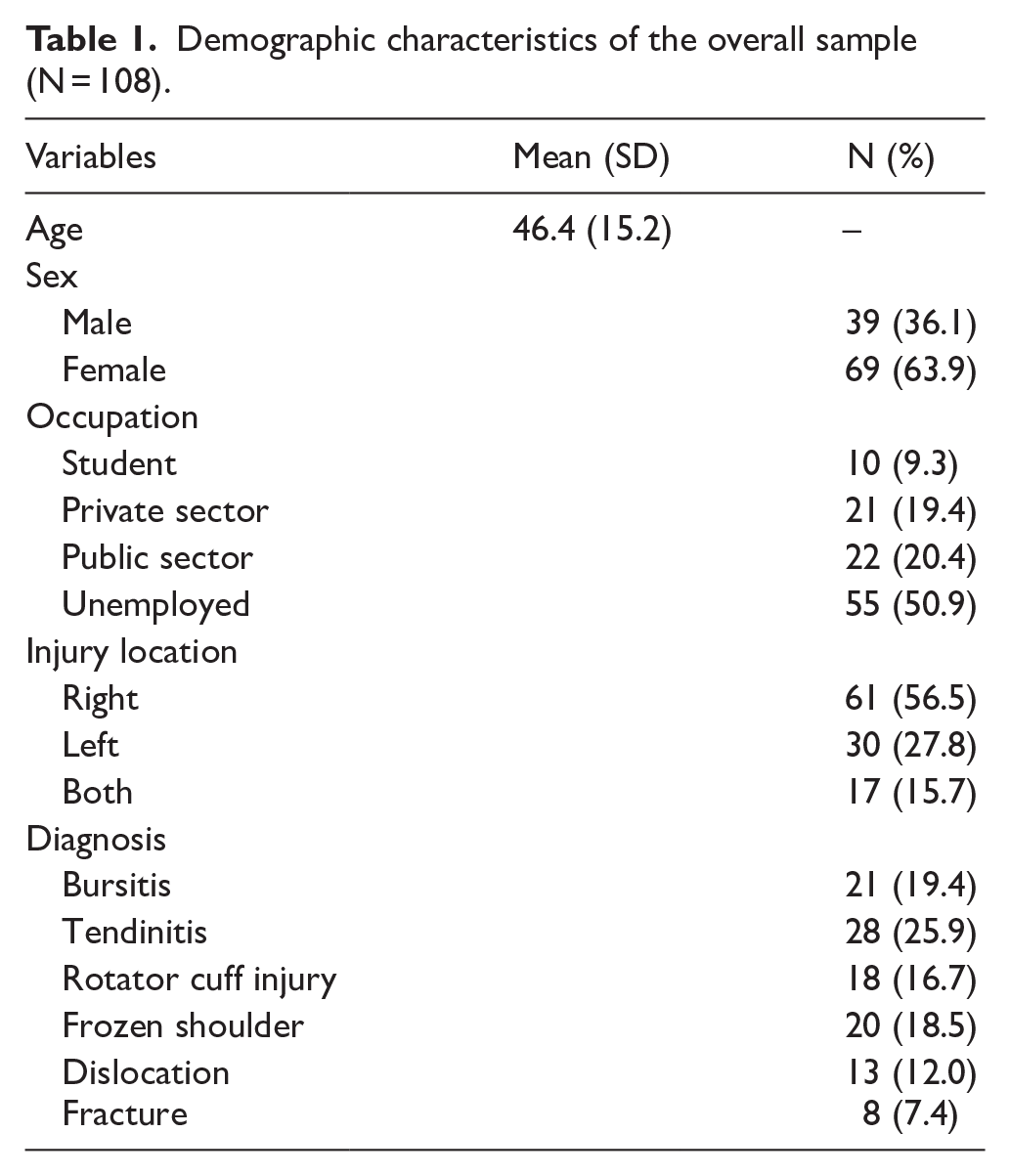
As presented in Table 1, a total of 108 participants were included in the study, with a mean age of 46.4 years (SD = 15.2, range: 18-70 years). About two-thirds of the participants were female (63.9%), while males accounted for 36.1% of the sample. Most shoulder injuries affected the right side (56.5%), followed by the left side (27.8%), while 15.7% reported bilateral involvement. The most common injury among participants was Tendinitis (25.9%), followed by Bursitis (19.4%) and Frozen Shoulder (18.5%).
Demographic characteristics of the overall sample (N = 108).
Reliability
Internal Consistency
The internal consistency of the Arabic version of the ASES form was excellent, with a Cronbach’s α of .90. An item-by-item analysis indicated that the removal of any single item would not significantly reduce the overall reliability, with Cronbach’s α values ranging from .89 to .90 for individual items.
Test-Retest Reliability
Test-retest reliability demonstrated a high correlation between measurements at 2-time points (r = .95, 95% CI: 0.915-0.970; P < .001), indicating excellent stability and reproducibility over time (See Table 2).
Test-retest reliability results.

Validity
Convergent Validity
The Arabic ASES form showed good convergent validity, with significant correlations with related constructs. A strong negative correlation was observed with the DASH score (r = −.867, P < .001), indicating that as ASES scores increased, disability scores decreased. Moderate positive correlations were found with the ADL score (r = .522, P < .001), demonstrating alignment with functional measures. Similarly, moderate negative correlations were observed with the VAS (r = −.480, P < .001) and the SF-MPQ (r = −.554, P < .001), supporting the scale’s sensitivity to pain-related disability (See Table 3).
Convergent validity results.
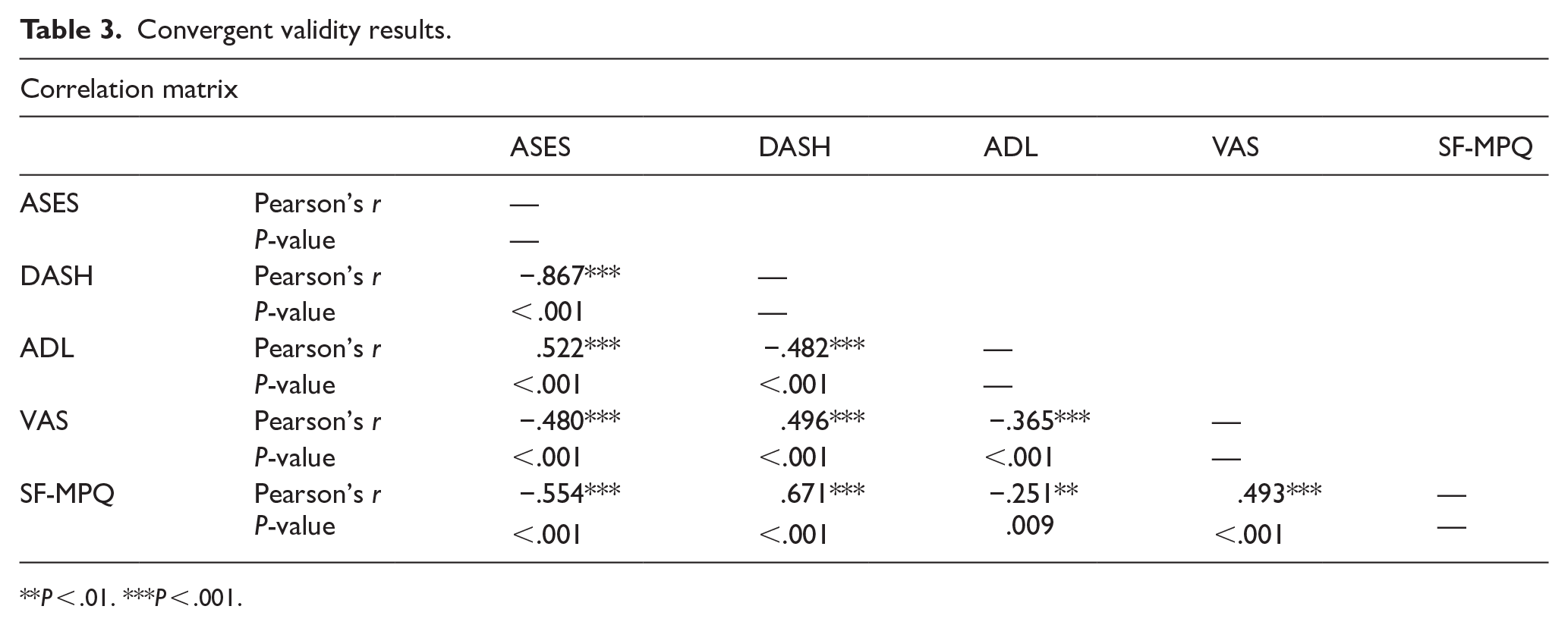
**P < .01. ***P < .001.
Discriminant Validity (Divergent Validity)
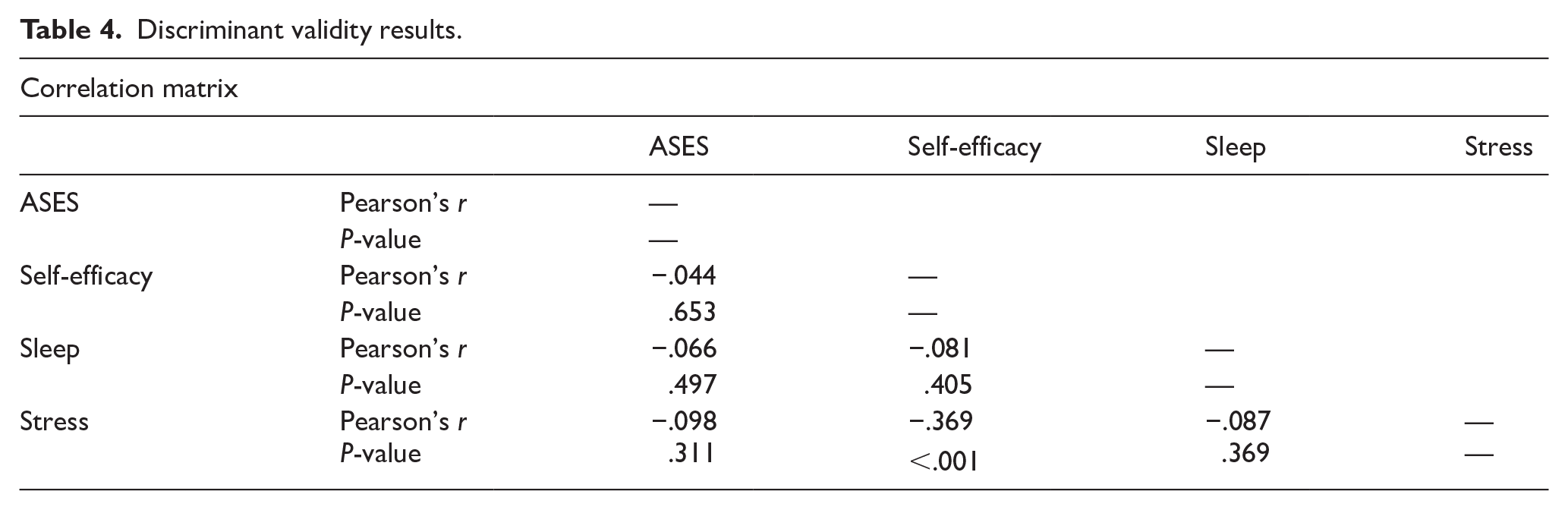
Discriminant validity analysis confirmed the scale’s specificity, as correlations with unrelated constructs such as self-efficacy (r = −.044, P = .653), sleep quality (r = −.066, P = .497), and stress (r = −.098, P = .311) were weak and statistically non-significant (See Table 4).
Discriminant validity results.
Agreement Analysis
The Bland-Altman analysis was performed to assess the agreement between 2 measurements of the ASES in the Arabic context. The analysis revealed a mean bias of −2.11, with 95% limits of agreement ranging from −3.24 to −0.979. This indicates that, on average, the second measurement is slightly lower than the first, demonstrating minimal systematic error between the 2 assessments. The small magnitude of the bias suggests a high level of consistency between repeated ASES measurements, implying good agreement and repeatability of the ASES scores (See Table 5 and Figure 1).
Bland-Altman analysis results.

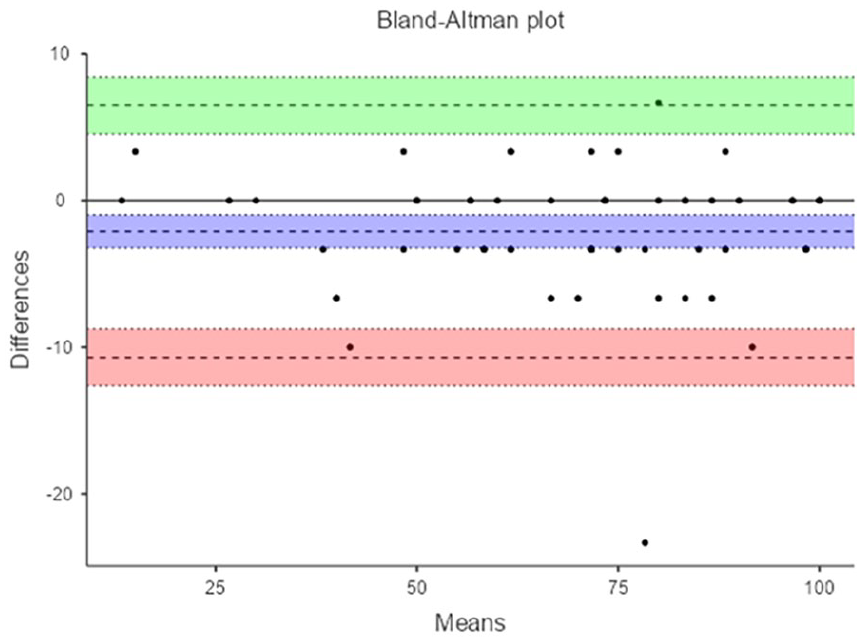
Difference between Time 1 and Time 2 measurements.
Discussion
This study aimed to evaluate the psychometric properties of the Arabic ASES form for use in Arab countries. The results revealed that the Arabic ASES demonstrates good psychometric properties for assessing shoulder disabilities in the Arabic-speaking population, with high reliability and satisfactory validity supporting its use in clinical and research settings. The translation process into Libyan-Arabic was seamless, with minimal disagreements between translators. These findings confirm that the Arabic ASES form is a robust instrument for evaluating shoulder disabilities in Arabic-speaking populations, particularly in Libya, aligning with prior successful adaptations of the ASES form into other languages and highlighting its cross-cultural validity and clinical utility.
Specifically, the Arabic ASES demonstrated excellent internal consistency comparable to previously validated versions in other languages, such as the Dutch and Portuguese versions.11,14 This high internal consistency reflects the scale’s reliability in measuring shoulder-related functional impairments. Moreover, the test-retest reliability confirms the stability of the Arabic ASES over time. This value aligns with findings from other versions, such as the Chinese and German adaptations, which also demonstrated high test-retest reliability.15,16
The convergent validity of the Arabic ASES was supported by strong correlations with established measures, such as the DASH, which is in line with results from the Greek and Italian adaptations of the ASES.10,13 These findings highlight the scale’s capacity to measure functional disability consistently across different populations. The moderate correlations with VAS and SF-MPQ further emphasize its sensitivity to pain-related constructs, which is a critical feature for assessing the multifaceted nature of shoulder disabilities.
As part of the psychometric validation of the Arabic version of the ASES, discriminant validity was also evaluated to determine whether the instrument accurately measures shoulder-specific function without overlapping with unrelated psychological or behavioral constructs. The analysis demonstrated weak and statistically non-significant correlations with theoretically unrelated measures, including general self-efficacy, sleep quality, and stress, as detailed in Table 4.
These findings support the scale’s discriminant validity by confirming that the Arabic ASES maintains conceptual specificity. The constructs selected for comparison—self-efficacy, sleep quality, and perceived stress—are relevant to overall well-being but are not expected to directly influence shoulder-specific symptoms or functional limitations. 39 For example, while stress or sleep disturbances may indirectly affect musculoskeletal health or recovery, 40 they are not components of the physical and functional domains targeted by the ASES. Similarly, general self-efficacy reflects a broad belief in one’s capabilities across various life domains, rather than task-specific functional performance related to the shoulder. 41
By demonstrating a lack of significant association with these unrelated constructs, the Arabic ASES exhibits strong construct clarity, ensuring that it does not inadvertently measure generalized psychological states. 42 This is particularly important in clinical and rehabilitation contexts, where accurate, culturally adapted assessment tools are needed to evaluate physical function without interference from other factors.
While the Tunisian-Arabic version of the ASES by Yahia et al 17 provided a valuable foundation for its use in Arabic-speaking populations, our study addressed several limitations noted in their adaptation. Yahia et al 17 primarily focused on translating the scale into the Tunisian dialect, limiting its use to a specific geographic region. In contrast, our study employed a comprehensive validation process, utilizing the standard Arabic language spoken in most Arab countries and conducting robust convergent and discriminant validity assessments. We demonstrated the scale’s specificity by confirming weak and non-significant correlations with unrelated constructs such as self-efficacy, sleep quality, and stress, which were not evaluated in the Tunisian study. Furthermore, while Yahia et al’s sample was representative of a Tunisian clinical population, it may not fully generalize to other Arabic-speaking populations due to regional and cultural differences. By validating the scale in Libya using the standard Arabic language, our study offers a broader perspective on its applicability across diverse Arabic-speaking contexts. This broader generalizability, essential given the cultural and healthcare system differences among Arab countries, enhances the credibility, applicability, and utility of the Arabic ASES, establishing it as a reliable and culturally adaptable tool for assessing shoulder disabilities across various Arab nations.
Clinical Implications
The availability of a validated Arabic version of the ASES form significantly enhances the capacity of clinicians and researchers to accurately assess shoulder disabilities in Arabic-speaking populations, addressing a critical gap in culturally and linguistically appropriate measurement tools. Its strong psychometric properties, including high reliability and validity, make it an indispensable resource for both cross-sectional evaluations and longitudinal monitoring, allowing for precise tracking of patient progress and treatment outcomes over time. Furthermore, its alignment with internationally recognized measures, such as the DASH and ADL scales, ensures comparability across studies and facilitates the integration of findings into global research frameworks. This compatibility promotes international research collaborations and enables benchmarking of regional outcomes against global standards, thereby contributing to a more comprehensive understanding of shoulder disabilities in diverse cultural contexts. By offering a robust and culturally adaptable assessment tool, the Arabic ASES form empowers healthcare providers to deliver more targeted and effective care, ultimately improving patient outcomes in Arabic-speaking regions.
Limitations and Future Directions
This study established the reliability and validity of the Arabic version of the ASES; however, a few limitations should be noted. First, the questionnaire was administered in Standard Arabic, which, although widely understood, may not be fully accessible to individuals from ethnic minorities or those who primarily speak regional dialects. This linguistic limitation could affect the inclusivity and applicability of the tool across all segments of the Libyan population. Another limitation concerns the inclusion of older adults with potentially low literacy levels, who may have encountered difficulties comprehending some questionnaire items. Although their inclusion was intended to enhance the generalizability of the findings across age groups and to assess the tool’s performance in both younger and older Libyan adults, advancing age may influence response reliability. It is important to note, however, that participants over the age of 65 constituted a small proportion of the sample. The age range of participants was 18 to 70 years, with a mean age of 46.4 ± 15.2 years, indicating a broadly representative adult sample.
Future research should consider validating the Arabic ASES across different Arabic-speaking countries and dialects to improve its cultural and linguistic adaptability. Cross-cultural validation studies are particularly important for identifying and addressing semantic, idiomatic, or conceptual discrepancies that may arise in diverse Arabic dialects. Researchers are also encouraged to examine the tool’s psychometric properties in specific subgroups, such as individuals with limited literacy, low education levels, or those living in rural or underserved regions.
Moreover, longitudinal studies are needed to evaluate the tool’s sensitivity to change and its responsiveness to interventions over time. This would enhance its utility in clinical and rehabilitation settings. Digital adaptations of the ASES (eg, mobile or web-based versions) should also be explored to facilitate broader access, especially among younger populations and those in remote areas.
Conclusion
The Arabic version of the ASES is a reliable, valid, and culturally appropriate instrument for assessing shoulder disabilities in Arabic-speaking populations. Its good psychometric properties align with findings from previous adaptations in other languages, confirming its utility in clinical and research settings. Expanding its use across diverse Arabic-speaking contexts and evaluating its responsiveness to interventions will further solidify its role in shoulder disability assessment.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the participants who contributed their time and effort to this study. We also acknowledge the valuable support provided by the administrative staff and colleagues who assisted in the logistics of this research. Special thanks to the ASES development team for creating the original questionnaire that served as the basis for this study.
Ethical Considerations
The study adhered to the principles of the Declaration of Helsinki. All study materials were reviewed and approved by the research ethics committee of the Department of Physiotherapy, Faculty of Medical Technology, Misrata, Libya [Ref# EXT. 16 - 2023].
Consent to Participate
All participants were required to agree to participate and sign an informed consent before proceeding. Confidentiality was maintained by anonymizing all data.
Author Contributions
Both authors contributed equally to the planning and data collection procedures of this research. The first author conducted the data analysis and drafted the initial version of the manuscript. Both authors reviewed and approved the final version.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is freely available by formal request directed to the corresponding author.