
Abstract
Background:
Achilles tendinopathy is a prevalent musculoskeletal condition that limits activity and performance. The Victorian Institute of Sport Assessment–Achilles (VISA-A) questionnaire is the gold-standard patient-reported outcome measure for symptom severity, but no comprehensive Arabic validation has been available.
Purpose:
To translate, culturally adapt, and validate the VISA-A into Arabic (VISA-A–Arabic) and to examine its psychometric properties in a broad population.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
The VISA-A was translated and culturally adapted following international guidelines. A total of 139 participants were recruited: 60 healthy participants, 47 healthy at-risk participants, and 32 patients with Achilles tendinopathy. All participants completed the VISA-A–Arabic and the 36-item Short Form Health Survey (SF-36) at baseline; the VISA-A–Arabic was re-administered after 1 to 3 days. Internal consistency, test-retest reliability, construct validity, measurement error, and known-group validity were evaluated.
Results:
The VISA-A–Arabic demonstrated acceptable internal consistency (Cronbach α = 0.73 [95% CI, 0.65-0.80]) at baseline and good test-retest reliability (intraclass correlation coefficient = 0.76 [95% CI, 0.68-0.83]). Construct validity was confirmed by a strong correlation with the SF-36 Physical Component Summary (r = 0.63; P < .001) and a weak correlation with the SF-36 Mental Component Summary (r = 0.33; P = .02). Known-group validity showed significantly lower VISA-A–Arabic scores at baseline in patients with Achilles tendinopathy (54.8 ± 20.9) compared with healthy (85.9 ± 10.6) and healthy at-risk (92.7 ± 8.0) participants (F(2,136) = 87.6; P < .001; η2 = 0.56). The standard error of measurement was 10.3, and the smallest detectable change at the individual level was 28.4. No floor effects were observed, and ceiling effects were minimal in the Achilles tendinopathy group.
Conclusion:
Our study showed that the VISA-A–Arabic is a reliable and valid instrument for assessing Achilles tendon–related symptoms and function. Unlike earlier Arabic validation efforts limited to patients, this study included a larger and more diverse cohort and incorporated additional psychometric analyses (standard error of measurement, smallest detectable change, Bland-Altman plot). These findings provide stronger evidence for the clinical and research application of the VISA-A–Arabic across Arabic-speaking populations.
Keywords
Achilles tendinopathy is a common musculoskeletal disorder affecting both athletes and nonathletes. It is characterized by pain, stiffness, and functional limitations, with a prevalence estimated at 2.16 per 1000 person-years.2,17,25 Recovery can be prolonged and incomplete, often requiring structured rehabilitation.3,7,9,20,23,24 Patients with diabetes are particularly susceptible.5,14,18 Because symptoms and disability vary considerably among patients, reliable outcome measures are essential for monitoring progress and evaluating treatment effectiveness.6,8,11,12
The Victorian Institute of Sport Assessment–Achilles (VISA-A) questionnaire is a disease-specific patient-reported outcome measure developed to assess the severity of Achilles tendinopathy. 21 It consists of 8 items that evaluate pain, function, and activity level. Lower scores indicate more severe symptoms and greater functional limitations, while higher scores reflect fewer symptoms and better function.
Since its development in English, the VISA-A has been translated and validated in multiple languages, including Swedish, 24 French, 13 Italian, 16 German, 15 Turkish, 8 Spanish, 11 and Danish. 12 These adaptations have consistently confirmed the VISA-A as a reliable and valid tool for assessing Achilles tendon–related disability. More recently, Alshewaier et al 4 published the first Arabic-language adaptation of the VISA-A, reporting excellent internal consistency (Cronbach α = 0.94) and test-retest reliability (intraclass correlation coefficient [ICC] = 0.98).
While Alshewaier et al’s 4 work marked an important milestone, their study included only patients with Achilles tendinopathy, limiting the scope of validation. Our study built on this foundation by recruiting a larger and more diverse cohort (n = 139) comprising healthy participants, healthy at-risk participants, and patients with Achilles tendinopathy. Furthermore, we applied additional psychometric analyses, such as the Bland-Altman plot, standard error of measurement (SEM), and smallest detectable change (SDC), to provide clinicians and researchers with interpretability metrics not previously reported. These enhancements ensure a more comprehensive validation of the Arabic version of the VISA-A (VISA-A–Arabic) and strengthen its clinical and research applicability.
The purpose of this study was to translate, culturally adapt, and validate the VISA-A questionnaire for Arabic-speaking patients with Achilles tendinopathy while extending prior work by providing broader sampling and more detailed psychometric testing. We hypothesized that the VISA-A–Arabic would demonstrate acceptable reliability, strong construct and known-group validity, and a minimal measurement error, supporting its use in clinical and research settings among Arabic-speaking populations.
Methods
The VISA-A questionnaire was translated and culturally adapted into Arabic following the internationally accepted guidelines proposed by Beaton et al. 6 The process included forward translation, synthesis, backward translation, an expert committee review, and prefinal testing on 10 bilingual volunteers. Minor modifications were made to produce the final Arabic version (VISA-A–Arabic). Ethical approval was obtained from the institutional review board of King Saud University (No. E-19-4315). Written informed consent was obtained from all participants before enrollment.
A total of 139 participants were recruited for psychometric testing. They comprised 60 healthy participants (asymptomatic), 47 healthy at-risk participants (those who scored ≥5 on the Physical Activity Level Scale), 10 and 32 patients with Achilles tendinopathy diagnosed clinically—based on examination findings of localized tendon pain, tenderness, and pain during loading—by a physician (≥5 years) or a physical therapist (≥3 years) with clinical experience. Inclusion criteria were age ≥18 years, ability to read and write Arabic, and provision of informed consent. Exclusion criteria included previous Achilles tendon ruptures, systemic inflammatory conditions, or neurological impairments affecting lower limb function.
At baseline, all participants completed the VISA-A–Arabic and the Arabic version of the 36-item Short Form Health Survey (SF-36). 1 The VISA-A–Arabic was then re-administered after an interval of 1 to 3 days to assess test-retest reliability.
All analyses were performed using SPSS (Version 21; IBM). Internal consistency was assessed using the Cronbach alpha, with a value between 0.70 and 0.95 considered acceptable.19,26 Test-retest reliability was assessed using the Pearson correlation coefficient and ICC(2,1), supported by Bland-Altman analysis. Construct validity was examined using correlations with SF-36 domains, with strong correlations expected for the Physical Component Summary and weak correlations for the Mental Component Summary. Known-group validity was evaluated with 1-way analysis of variance and effect size estimation. The measurement error was estimated using the SEM and SDC in the Achilles tendinopathy group. 22 Floor and ceiling effects were assessed, with a threshold of 15% considered acceptable. 26
Results
Participant characteristics are summarized in Table 1. Patients with Achilles tendinopathy were older (36.1 ± 12.8 years) compared with healthy (28.0 ± 4.9 years) and healthy at-risk (28.2 ± 6.0 years) participants. The body mass index was higher in the Achilles tendinopathy group (28.5 ± 5.8 kg/m2) compared with the healthy (25.4 ± 5.6 kg/m2) and healthy at-risk (25.0 ± 6.4 kg/m2) groups.
Participant Characteristics a
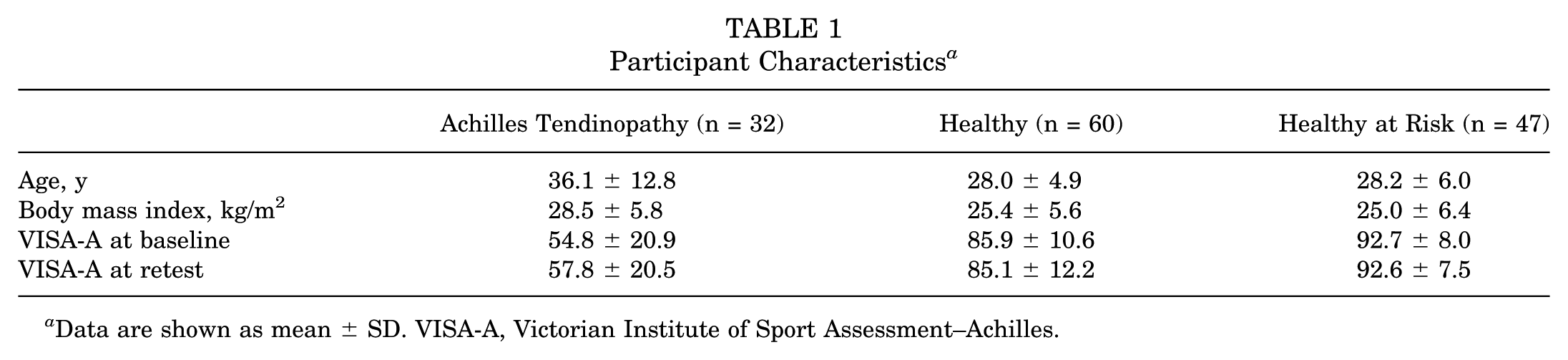
Data are shown as mean ± SD. VISA-A, Victorian Institute of Sport Assessment–Achilles.
VISA-A–Arabic scores demonstrated clear group differences. At baseline, patients with Achilles tendinopathy scored 54.8 ± 20.9 compared with 85.9 ± 10.6 for healthy participants and 92.7 ± 8.0 for healthy at-risk participants. At retest, scores were 57.8 ± 20.5, 85.1 ± 12.2, and 92.6 ± 7.5, respectively. These group comparisons are illustrated in Figure 1.

Baseline VISA-A–Arabic scores by group. Boxplots show medians, interquartile ranges, and outliers for the Achilles tendinopathy, healthy, and healthy at-risk groups. Individual data points are overlaid to illustrate the score distribution.
The VISA-A–Arabic demonstrated acceptable internal consistency, with a Cronbach alpha of 0.73 (95% CI, 0.65-0.80) at baseline and 0.70 (95% CI, 0.61-0.78) at retest. Corrected item–total correlations ranged from 0.22 to 0.74, with item 7 showing the weakest relationship, consistent with previous adaptations. Structural analysis confirmed a dominant single factor explaining over half of the variance. Test-retest reliability was good, with a Pearson r of 0.76 and ICC(2,1) of 0.76 (95% CI, 0.68-0.83). Bland-Altman analysis showed a mean difference of +0.32 and limits of agreement of −25.9 to +26.5, as displayed in Figure 2. The main psychometric results are summarized in Table 2.

Bland-Altman plot of VISA-A–Arabic total scores (n = 139). Differences between test and retest are plotted against their mean. The blue dashed line indicates the mean difference (+0.32), while orange dashed lines indicate the limits of agreement (−25.9 to +26.5).
Psychometric Properties of Arabic VISA-A a

The 95% CI is shown in parentheses. ICC, intraclass correlation coefficient; SDC, smallest detectable change; SEM, standard error of measurement; VISA-A, Victorian Institute of Sport Assessment–Achilles.
Construct validity was confirmed through correlations with SF-36 domains. The VISA-A–Arabic correlated strongly with the Physical Component Summary (r = 0.63) and with individual domains including Bodily Pain (r = 0.56), Role-Physical (r = 0.56), and Physical Functioning (r = 0.49). Associations with mental domains were weaker: Mental Health (r = 0.21), Social Functioning (r = 0.28), and Role-Emotional (r = 0.26). The Mental Component Summary correlation was also weak (r = 0.33). These results are presented in Table 3.
Correlation of Arabic VISA-A With SF-36 Domains a
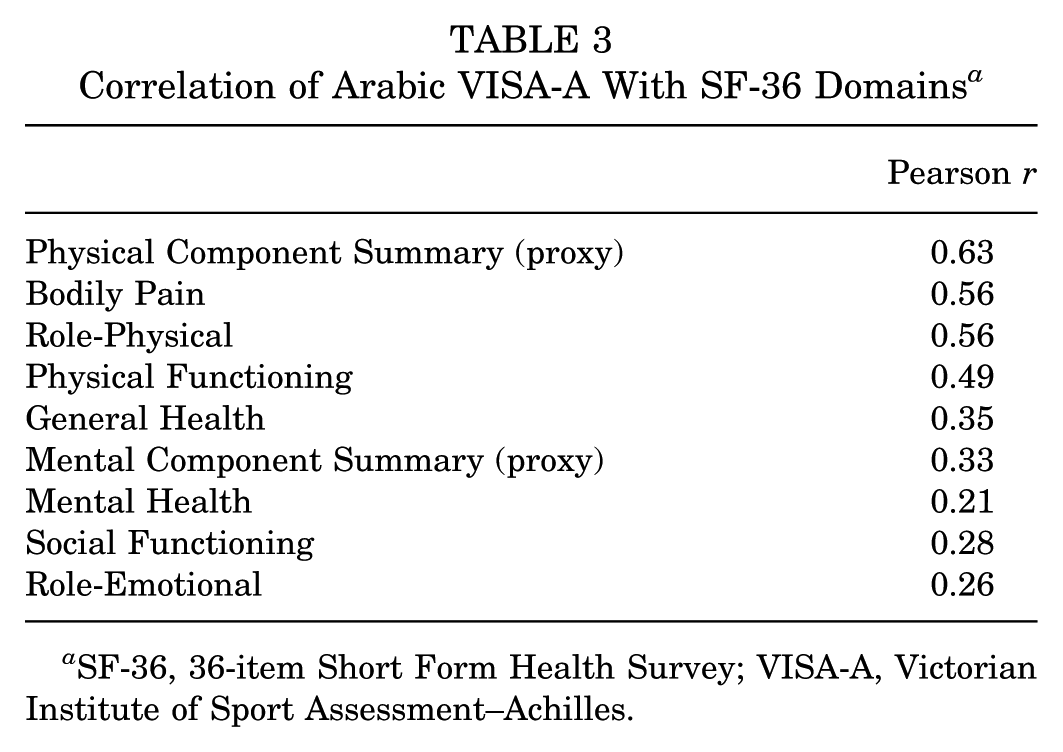
SF-36, 36-item Short Form Health Survey; VISA-A, Victorian Institute of Sport Assessment–Achilles.
Known-group validity was strongly supported. One-way analysis of variance confirmed significant group differences in VISA-A–Arabic scores (F(2,136) = 87.6; P < .001; η2 = 0.56). Post hoc comparisons revealed large effect sizes, with a Cohen d of 2.07 between patients with Achilles tendinopathy and healthy participants, 2.59 between patients with Achilles tendinopathy and healthy at-risk participants, and −0.72 between healthy and healthy at-risk participants.
Floor and ceiling effects were minimal. No participants scored at the floor (0), and ceiling effects were absent in the Achilles tendinopathy group. Among healthy participants, 5% reached the maximum score, while in the healthy at-risk group, 19% did. Although expected in the healthy and healthy at-risk groups, ceiling effects in patients with Achilles tendinopathy remained below the 15% threshold considered acceptable. Additionally, measurement error analysis showed an SEM of 10.3, corresponding to an SDC of 28.4 at the individual level and 5.0 at the group level in the Achilles tendinopathy group.
Discussion
Our study demonstrated that the VISA-A–Arabic showed acceptable internal consistency (Cronbach α = 0.73), good test-retest reliability (ICC = 0.76), and strong known-group validity (F(2,136) = 87.6; P < .001; η2 = 0.56). These findings confirm the scale's ability to discriminate between healthy, at-risk, and symptomatic people.
This study presents a comprehensive validation of the Arabic version of the VISA-A (VISA-A–Arabic). The results confirmed that the VISA-A–Arabic is reliable, valid, and able to discriminate effectively between healthy, at-risk, and symptomatic people. The inclusion of 3 distinct participant groups strengthens the evidence for known-group validity and extends the clinical applicability of the tool beyond tendinopathy populations alone.
Our internal consistency (Cronbach α = 0.73) and test-retest reliability (ICC = 0.76) fall within the acceptable range for patient-reported outcome measures. These values are somewhat lower than those reported in the recent study by Alshewaier et al 4 (Cronbach α = 0.94; ICC = 0.98). Several factors may explain this discrepancy, including differences in study design, sample characteristics, and retest intervals. Notably, Alshewaier et al 4 restricted their validation to a patient-only cohort, while our study included a more heterogeneous sample, which may naturally yield greater score variability and lower reliability indices. Importantly, our findings align with reliability estimates from other VISA-A translations, such as the German (Cronbach α = 0.74) 15 and Turkish (Cronbach α = 0.66) 8 versions, supporting the robustness of our results.
A key contribution of the present study is the addition of interpretability metrics not previously reported in Arabic adaptations. We calculated the SEM (10.3) and SDC (28.4 for individual; 5.0 for group), providing clinicians with thresholds to distinguish real change from the measurement error. Bland-Altman analysis further confirmed acceptable agreement between test and retest administrations. These analyses extend the utility of the VISA-A–Arabic for both clinical monitoring and research trials in which sensitivity to change and reproducibility are essential.
Construct validity was confirmed by strong correlations with SF-36 physical domains and weaker correlations with SF-36 mental domains, consistent with the intended measurement construct of the VISA-A. Known-group validity was further supported by significant between-group differences, with large effect sizes distinguishing symptomatic from nonsymptomatic participants. Ceiling effects were observed in the healthy and healthy at-risk groups but were minimal in the Achilles tendinopathy group, consistent with findings from other language versions.12,13,15,16
This study has limitations. The Achilles tendinopathy group was relatively small compared with the healthy and healthy at-risk groups, which may reduce the precision of subgroup estimates. Responsiveness and the minimal clinically important difference were not evaluated, which should be addressed in future longitudinal studies. Additionally, our validation was limited to Arabic speakers in Saudi Arabia, and further testing in broader Arabic-speaking populations is warranted.
This study confirms that the VISA-A–Arabic is a reliable and valid instrument for assessing Achilles tendon–related symptoms and function. By including a broader participant base and providing interpretability metrics such as the SEM, SDC, and Bland-Altman plot, this work complements and extends the earlier study by Alshewaier et al. 4 Together, these findings strengthen the evidence base for using the VISA-A–Arabic in both clinical practice and research across Arabic-speaking populations.
Conclusion
The VISA-A–Arabic was successfully translated, culturally adapted, and validated. This provides clinicians and researchers with additional interpretability metrics and stronger evidence for the VISA-A–Arabic’s reliability and validity. The VISA-A–Arabic is therefore recommended for use in both clinical practice and research, with future studies encouraged to establish responsiveness and the minimal clinically important difference.
Footnotes
Acknowledgements
The project was funded by KAU Endowment (WAQF) at king Abdulaziz University, Jeddah, Saudi Arabia. The authors, therefore, acknowledge with thanks WAQF and the Deanship of Scientific Research (DSR) for technical and financial support.
Final revision submitted November 9, 2025; accepted November 14, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the institutional review board of King Saud University (No. E-19-4315).