
Abstract
Background:
The Athlete Fear-Avoidance Questionnaire (AFAQ) is a validated instrument that measures athletes’ fear and avoidance behaviors after an injury, particularly regarding their sporting activities.
Purpose:
This study aimed to adapt and validate the AFAQ for Arabic-speaking recreational players (AFAQ-Arabic) after anterior cruciate ligament reconstruction (ACLR).
Study Design:
Cohort study; level of evidence: 3.
Methods:
The AFAQ underwent translation and cross-cultural adaptation according to the Beaton guidelines. A total of 104 male recreational players who had undergone ACLR completed the AFAQ-Arabic, the Fear-Avoidance Belief Questionnaire (FABQ), and the Numerical Pain Scale (NPS). To assess test-retest reliability, a subset of 38 recreational players were asked to complete the AFAQ-Arabic twice, 1 week apart. Statistical tests were conducted to test the internal consistency, reliability, and convergent validity of the AFAQ-Arabic.
Results:
The AFAQ-Arabic demonstrated high internal consistency (Cronbach alpha, 0.854) and excellent test-retest reliability (intraclass correlation coefficient, 0.885) (95% CI, 0.784-0.942; P < .001). Minimal floor (4.8% scoring the minimum) and ceiling effects (1% scoring the maximum) were observed. Convergent validity showed significant positive weak correlations between the AFAQ-Arabic and (1) the FABQ-Physical Activity (r = 0.340; P < .01), (2) the FABQ-Work (r = 0.272; P < .01), and (3) the NPS (r = 0.383; P < .01). Cross-cultural adaptation of the AFAQ-Arabic revealed linguistic and cultural relevance.
Conclusion:
Our study demonstrated that the AFAQ-Arabic was a reliable and valid tool for assessing fear avoidance in Arabic-speaking recreational players after ACLR. Future studies are needed to measure athlete fear-avoidance in injured Arabic-speaking athletes to understand its psychological aspects in rehabilitation and potentially aid in tailored interventions for improving outcomes.
Keywords
Anterior cruciate ligament (ACL) injury is one of the most common knee injuries among athletes and recreational players (eg, basketball, soccer, football, and gymnastics).28,34,49 Previous research has found no differences in the incidence rates of ACL injuries or meniscal tears between athletes and nonathletes 12 but found a high risk of ACL injury among recreational soccer players. 17 In Saudi Arabia, the incidence rate of knee injuries stands at 23.2% among college male students—a significant figure compared with other countries. 1 For example, the injury rate was only 10.4% among adolescent female soccer players in Australia, 31 and 28 per 100,000 persons in the United States. 21 ACL injuries are commonly associated with specific movements—such as sudden changes in direction, jumping, pivoting, and/or cutting tasks 10 —and/or ligament laxity in nonathletes. 11 Previous studies across various regions of Saudi Arabia revealed that sports-related activities accounted for the highest number of ACL injuries,1,3,4,5,15 with higher prevalence in sports such as basketball, soccer, football, gymnastics, and/or field hockey. 24
The Athlete Fear-Avoidance Questionnaire (AFAQ) 19 is a valuable instrument for assessing fear-avoidance-related beliefs in athletes and is available in Brazilian Portuguese, 18 Italian, 32 and Urdu. 40 However, its application in Arabic-speaking populations is limited, particularly in the context of post anterior cruciate ligament reconstruction (ACLR), which remains a gap in the current literature. ACLR is a common surgical intervention for ACL injury, with over 100,000 procedures performed annually in the USA, costing >3 billion dollars each year. 27 In Canada, the incidence of primary ACLR increased from 40.6 to 51.2 per 100,000 people aged ≥10 years, with a greater annual increase for women (1.8%) compared with men 38 (0.96%). ACLR and its rehabilitation typically focus on physical factors, but psychological elements such as kinesiophobia and fear avoidance also play a critical role in the recovery process. 45 Approximately 45% to 60% of athletes with an ACL tear return to their preinjury level of competition.8,30 Growing evidence suggests that psychological factors may account for the variability in returning to competition.14,16,36 Athletes and recreational players often fear reinjury, which can lead to avoidance of key rehabilitation activities and premature return to play because of concerns about losing their sporting autonomy or recreational participation. 2 These fear-avoidance beliefs align with the Fear-Avoidance Model, 48 which suggests that those who fear pain and reinjury—including postoperative pain—may avoid physical- and work-related activities. 2
Recreational players from Arabic-speaking countries may face challenges such as language barriers when seeking medical or psychological support. Arabic-speaking populations face unique challenges in managing ACL injuries, influenced by cultural attitudes toward rehabilitation and varying levels of health literacy. These factors can significantly affect how individuals perceive and respond to their injuries. Simply translating an assessment tool like the AFAQ into Arabic fails to address these cultural nuances, potentially compromising its effectiveness. Therefore, validating a culturally adapted version is essential to accurately assess the psychological impact of ACL injuries in this demographic, ultimately improving patient care and outcomes. This study aimed to cross-culturally adapt and assess the reliability and validity of the AFAQ in the Arabic language (AFAQ-Arabic) for use by Arabic-speaking recreational players after ACLR. We hypothesized that the AFAQ-Arabic would demonstrate good internal consistency, excellent test-retest reliability, and acceptable convergent validity—similar to the original AFAQ.
Methods
Participants
The sample size was determined based on guidelines recommending at least 10 participants per question in a survey.6,7 The original version of the AFAQ scale comprises 10 questions. 19 Therefore, at least 100 Arabic-speaking recreational players who had undergone ACLR were required for this study. In this study, recreational players were included if they met the following criteria: (1) age ≥18 years; (2) ACLR with or without meniscal injury; (3) at least 3 months post-ACLR at the time of data collection; (4) recreational activity before the ACL injury (5 on the Tegner Activity Level Scale) 35 ; and (5) ability to read and write in Arabic. The exclusion criteria were as follows: (1) a history of knee injuries preceding the current ACL injury; (2) injuries to both ACLs; and (3) multiligament reconstruction (figure 1). Ethical approval was obtained from the research ethics committee of Majmaah University before data collection (IRB No. MUREC-HA-01-R-008; Date: June 19, 2023). We contacted potential participants, provided a detailed explanation of the study procedures, and obtained their informed consent before participation. Participants completed an internet-based survey using Google Forms.
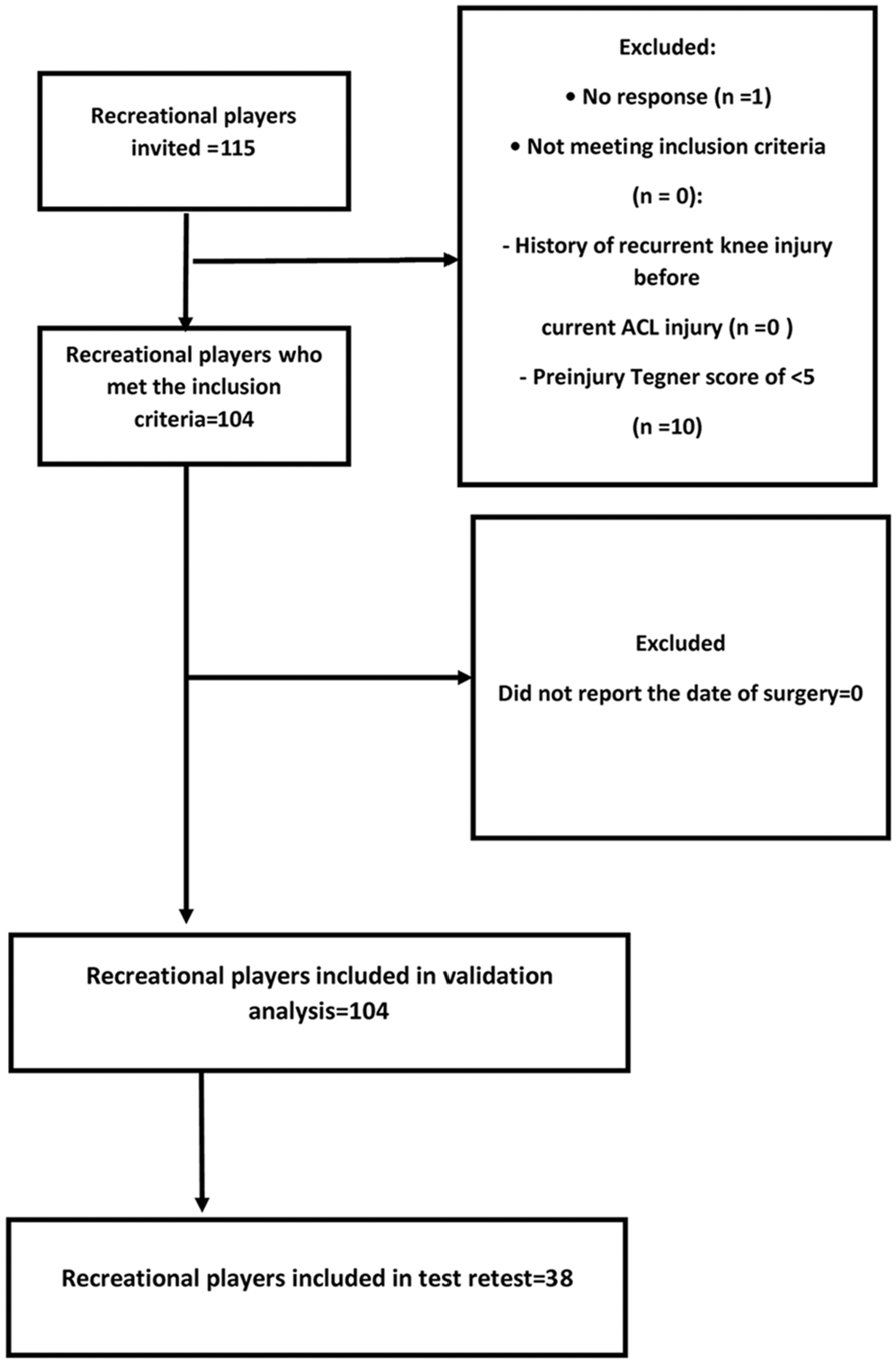
A flowchart illustrating participants’ invitations and enrollment. ACL, anterior cruciate ligament.
Translational and Cross-Cultural Adaptation of the AFAQ into Arabic
Translating and adapting the AFAQ into Arabic followed the Beaton guidelines for cross-cultural adaptation of self-report measures. 9 The translation of the AFAQ into Arabic—including both the first and second versions (T1 and T2)—was completed by 2 physical therapists who are native Arabic speakers with postgraduate degrees and proficiency in English, enabling them to accurately translate the questionnaire. Subsequently, the initial translated versions by the 2 physical therapists were subjected to meticulous scrutiny and deliberation with a third bilingual physical therapist (T3). This step was performed to detect and correct any conceptual inaccuracies or inconsistencies, culminating in the creation of a cohesive Arabic rendition of the scale. Following this, the T3 version was translated back into English by another 2 native English speakers who also spoke Arabic (B1 and B2) without any knowledge of the original version of the AFAQ. Subsequently, a consensus meeting was held among all translators to finalize the Arabic version of the AFAQ. Ultimately, a preliminary investigation was performed involving a small group of 5 recreational players who had undergone ACLR at least 3 months before our study. The pilot study included recreational players who completed the AFAQ-Arabic and offered their feedback regarding the scale’s content to propose suggestions and corrections.
For the test-retest reliability assessment, participants were instructed to complete the AFAQ-Arabic twice with a 1-week interval in between. A reminder was sent through email to participants who did not respond. For data collection, the Google Forms platform was utilized, and participants were recruited from Majmaah University and Riyadh Second Health Cluster-King Khalid Hospital in Majmaah, Saudi Arabia. Research findings were disseminated through social media and within physical therapy clinics. To assess convergent validity, we validated the AFAQ-Arabic against 2 instruments—the Numerical Pain Rating Scale (NPRS) and the Fear-Avoidance Beliefs Questionnaire (FABQ) (both available in Arabic). The AFAQ-Arabic contains 10 items with a 5-point response scale that reflects the fear of returning to sports. The NPRS measures pain intensity on a scale validated in Arabic. 46
Instruments
Athlete Fear-Avoidance Questionnaire (AFAQ)
The AFAQ was developed through a systematic process that involved a literature review, expert consultation, and pilot testing with college students undergoing rehabilitation for various injuries. 19 Drawing upon established fear-avoidance scales used in clinical and occupational settings, the AFAQ was specifically tailored to capture fear-avoidance behaviors and beliefs relevant to athletes recovering from sports-related injuries. 37 The primary purpose of the AFAQ is to provide sports medicine professionals—including athletic therapists and trainers—with a standardized measure to assess fear avoidance in recreational players undergoing rehabilitation. The reliability of the AFAQ was determined using internal consistency and test-retest reliability. 19 The validity of the AFAQ was established through various methods—including content validity, 33 construct validity, 20 and the Italian version of AFAQ criterion-related validity. 32
Fear-Avoidance Beliefs Questionnaire
The FABQ is a commonly used self-reported measure designed to assess beliefs and attitudes related to fear avoidance in athletes experiencing musculoskeletal pain, particularly low back pain. It was developed by Lethem et al 29 in 1983 and subsequently revised by Waddell et al. 47 in 1993. The FABQ aims to evaluate how individuals perceive physical activity and work-related activities about their pain. It consists of 2 subscales—the Physical Activity (FABQ-PA) subscale and the Work (FABQ-W) subscale.
The FABQ-PA consists of 5 items and assesses beliefs about the harmfulness of physical activity for one's pain condition. Participants rate their level of agreement on a Likert scale with statements such as “Physical activity makes my pain worse.”
The FABQ-W also includes 5 items and evaluates beliefs about the impact of work-related activities on one's pain. Participants respond to statements such as “My work involves activities that I am afraid might cause a flare-up of my pain.”
The FABQ has demonstrated good reliability and validity across various populations and settings. 25 Studies have reported high internal consistency for both the FABQ-PA and the FABQ-W, indicating that the items within each subscale measure the same underlying construct of fear-avoidance beliefs. 26 In addition, the FABQ has shown evidence of construct validity through correlations with measures of pain intensity, 41 disability, and psychological factors (eg, anxiety and depression). 39
Numerical Pain Rating Scale
The NPRS is a commonly used tool among healthcare professionals for assessing pain intensity. 22 This scale asks participants to rate their pain on a scale from 0 to 10, with 0 representing no pain and 10 indicating the worst pain imaginable.
Primary and Secondary Outcomes
The primary outcome of the study was the cultural adaptation and validation of the AFAQ in Arabic—including assessing its internal consistency, reliability, and validity in recreational players with ACL-reconstructed knees. The secondary outcome was the preliminary analysis of fear-avoidance behaviors in these athletes, as measured by correlations between the AFAQ-Arabic and related scales—such as the FABQ and the NPS.
Statistical Analyses
Descriptive analyses include means and standard deviations for numerical data and percentages/frequencies for categorical data. To estimate the potential floor and ceiling effects in the AFAQ-Arabic score distribution, we examined the percentage of participants with the lowest or highest scores 44 to ≤15%. For internal consistency of the AFAQ-Arabic scale, a Cronbach alpha test with a value that falls between 0.70 and 0.95 indicates adequate internal consistency. Test-retest reliability was assessed using 2-way random intraclass correlation coefficients (ICCs) for absolute agreement, with corresponding 95% CIs. 44 Reliability was categorized as excellent if ICC ≥0.75, good if 0.40 ≤ ICC < 0.75, and poor 43 if ICC < 0.40. Expressing the absolute measurement error of the AFAQ-Arabic as the standard error of measurement (SEM = SD pooled standard deviation √ [1 – ICC]). 23 The minimum detectable change (MDC) was manually calculated by calculating the pooled SEM and obtaining the ICC for agreement using a 2-way mixed model in the SPSS software (IBM). Construct validity between the AFAQ-Arabic with FABQ-PA, FABQ-W, and NPRS total scores was evaluated using Spearman correlation (strong: r ≥ 0.5; medium: 0.3 ≤ r < 0.5; weak: r < 0.3). 13 All analyses were conducted using the SPSS software Version 20.0 (IBM).
Results
Cross-Cultural Adaptation
The AFAQ-Arabic scale was successfully translated into Arabic, and participants reported no issues with understanding the questions. The back translation revealed no significant linguistic or grammatical problems, and the clarity of the questions remained intact without the need for specific cultural adaptations.
A total of 105 recreational players who underwent ACLR were invited, and 104 male participants completed our study. Out of the 104 included participants, 38 completed our study twice for test-retest reliability purposes. Participants were retested on the AFAQ-Arabic. Nearly half of the included participants (n = 50; 48.1%) engaged in football after ACLR. The mean time since ACLR participation in our study was 24.3 ± 24.5 months, ranging from 3 to 108 months. Table 1 provides the remaining demographic details of the recreational players.
Demographic and Clinical Data of the Included Participants (n = 104, All Men) a

Data in the table are presented as mean ± SD for continuous variables and n (%) for categorical variables. The continuous variables include age, height, weight, duration since surgery, AFAQ scores, retest AFAQ scores, FABQ-PA, FABQ-W, NPS, and hours spent in activity per week. Categorical variables include the type of activity (soccer, walking, soccer and running, soccer and weightlifting, weightlifting, running, and other sports), injured side (right, left), dominant side (right, left), and type of injury (ACL only, ACL with meniscus). ACL, anterior cruciate ligament, AFAQ, Athletes Fear-Avoidance Questionnaire, FABQ-PA, Fear-Avoidance Believe Questionnaire-Physical Activity; FABQ-W, Fear-Avoidance Believe Questionnaire–work; NA, not applicable; NPS, Numerical Pain Scale.
Floor and Ceiling Effect
In our analysis for the AFAQ-Arabic, the floor and ceiling effect criteria were set such that >15% of participants congregating at the extreme ends of the score spectrum would suggest floor or ceiling effects. 44 The mean score for the scale was 28.3 (9.1), spanning a range from 10 to 48. Notably, only a modest 4.8% of participants (n = 5) attained the minimum score of 10, while only 1 participant (1%) achieved the maximum score of 48. These findings suggest an absence of substantial floor or ceiling effects, aligning with the designated criterion. This indicates that the newly translated AFAQ-Arabic scale is capable of capturing a diverse range of participant responses.
Internal Consistency
In the reliability assessment of the 10-item scale, the Cronbach alpha was 0.854. This high Cronbach alpha value indicates a robust level of internal consistency and reliability among the items, confirming the scale’s reliability in measuring the targeted construct. Item-total statistics suggest that the removal of item 4 would enhance the scale’s reliability (Cronbach alpha value, 0.862). The ICC for single measures and mean measures revealed a higher ICC of 0.854 for mean measures and 0.369 for single measures, signifying strong agreement when considering the mean rating across multiple measures.
Reliability
The test-retest reliability of the AFAQ-Arabic scale demonstrated excellent reliability scores, with an ICC of 0.885 (95% CI, 0.784-0.942; P < .001). This high ICC value indicates strong agreement and consistency in participant responses (n = 38) between the initial test and the retest, reinforcing the reliability of the AFAQ-Arabic scale over time. The narrow confidence interval further enhances the precision of this reliability estimate. The pooled standard deviation of scores from the test and retest was 9.746, and the SEM was 0.374, resulting in an MDC of 1.07 units with a 95% CI ranging from 0.327 to 1.813.
Convergent Validity
The Spearman rho correlation matrix reveals significant relationships among the key variables in our study. The AFAQ-Arabic score demonstrates a positive correlation with both the FABQ-PA (r = 0.340; P < .01) and the NPRS (r = 0.383; P < .01), indicating that participants with higher levels of activity limitations due to pain may also report increased pain-related fear and heightened numerical pain scores. The FABQ-PA and FABQ-W exhibit a significant positive correlation (r = 0.422; P < .01), emphasizing the interconnectedness between physical- and work-related fear-avoidance beliefs. The positive correlation between the FABQ-W and the NPRS (r = 0.396; P < .01) suggests that participants with higher work-related fear-avoidance beliefs may also experience elevated pain levels as measured on the NPRS. The NPRS shows significant positive correlations with the AFAQ-Arabic (r = 0.383; P < .01), FABQ-PA (r = 0.426; P < .01), and FABQ-W scores (r = 0.396; P < .01), highlighting the association between numerical pain scores and activity limitations and fear-avoidance beliefs.
Discussion
This study translated, culturally adapted, and validated the Arabic version of the AFAQ (AFAQ-Arabic) among Arabic recreational players after ACLR. Our major findings demonstrated that the Arabic version of the AFAQ exhibits high internal consistency (0.854), reliability (0.885), and convergent validity and can be used with Arabic-speaking recreational players after ACLR for fear-avoidance assessment.
The AFAQ-Arabic demonstrated high internal consistency with a Cronbach alpha of 0.854, indicating strong reliability among the questionnaire items. This aligns with the iterative nature of scale development, emphasizing continuous improvement for optimal psychometric performance. Similarly, the original questionnaire developed by Dover and Amar 19 reported a Cronbach alpha of 0.805. The AFAQ was also adapted into Brazilian Portuguese, with a reported 18 Cronbach alpha of 0.90, and the Italian version reported 33 an internal consistency of 0.78.
Our test-retest reliability analysis showed an ICC of 0.885. This high ICC value signifies strong agreement and stability in participant responses over time, reaffirming the reliability of the AFAQ-Arabic scale regarding consistently capturing fear-avoidance beliefs. In alignment with our findings regarding the ICC of the AFAQ-Arabic, a cross-cultural adaptation in Brazilian Portuguese reported 18 an ICC of 0.85. Similarly, the Italian version of the AFAQ reported 33 an ICC of 0.95. The absence of significant floor or ceiling effects in the AFAQ-Arabic scale highlights capturing a wide range of participant responses effectively. The calculated SEM of 0.374 and MDC values of 1.07 offer valuable insights into the absolute measurement error, which is crucial for interpreting participants' score changes over time. However, the Italian version of AFAQ reported 33 an MDC of 4.04 units, revealing that the Arabic version of AFAQ was more sensitive to change over time. On the other hand, an Urdu version of AFAQ, conducted among 160 participants with low back pain, reported an MDC value of 1.263 and a SEM of 0.433, which aligns with our findings. 40
The statistically significant positive yet weak correlations (range, 0.3-0.4) observed between the AFAQ-Arabic, FABQ-PA, and NPRS underscore the construct validity of the AFAQ-Arabic. These correlations suggest that while there is a relationship between these scales, they measure distinct constructs of pain. Specifically, the AFAQ captures the dimension of pain related to fear-avoidance behaviors, whereas the FABQ measures the dimension related to fear-avoidance beliefs. These significant associations are in line with the theoretical underpinnings of fear-avoidance beliefs, thereby providing compelling evidence of the scale's capacity to capture pertinent psychological aspects (avoidance behaviors) of pain. The original developer of the AFAQ 19 reported a significant correlation with the FABQ-PA but not with the FABQ-W. However, our study found a significant positive correlation with both FABQ-PA and the FABQ-W. This discrepancy may be attributed to differences in participant demographic characteristics; the original study included nonworking college students involved in various sports, while our study focused on working recreational players with ACLR. Likewise, a study involving 133 college students with musculoskeletal injuries reported a positive moderate correlation between the Italian version of the AFAQ and various measures—including the NPRS, the Pain Catastrophizing Scale, 42 and subscales of the FABQ. 47
While our study establishes the reliability and validity of the AFAQ-Arabic among recreational players after ACLR, it still presents some limitations that warrant consideration. This study’s focus was on a specific patient population, and all included participants were men, which may limit the generalizability of our findings to female patients. Female recreational soccer players were not included in our study because of the predominance of male participation in soccer within the region. The Saudi Arabian women’s national football team, known as “the Green Falcons,” was officially established in 2021, with their first competitive match in February 2022. Consequently, female football players—including those with ACL injuries—were not available for inclusion in our study. Future research should include female football players to improve the sensitivity and cultural accuracy of the questionnaire. Despite the poor response rate, with only 38 participants completing the test-retest, this sample size was deemed sufficient for assessing the reliability of the translated questionnaire. Future research should also explore the responsiveness of the AFAQ-Arabic to interventions and assess its predictive values for functional outcomes in diverse patient populations.
Conclusion
Our study demonstrated that the AFAQ-Arabic was a valid and reliable tool for assessing fear avoidance in Arabic-speaking recreational players after ACLR. Future studies are needed to measure athlete fear-avoidance in injured Arabic-speaking athletes to understand its psychological aspects in rehabilitation and potentially aid in tailored interventions to improve outcomes.
Footnotes
Acknowledgements
The authors would like to thank the Deanship of Scientific Research at Majmaah University for supporting this work under Project number No. R-2024-1375. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Final revision submitted September 18, 2024; accepted October 24, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: The Deanship of Scientific Research at Majmaah University supported this work under Project number No. R-2024-1375. The AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Majmaah University (MUREC-Jun.19/COM-2023/23-5).