
Abstract
Introduction:
Atrial fibrillation (AF) is one of the most common arrhythmias in the general population and similar to other cardiovascular diseases, studies have shown that outcomes and treatment choices are often affected by gender and socioeconomic disparities.
Objectives:
This study aimed to investigate the differences in AF management and all-cause mortality based on gender and socioeconomic status.
Methods:
This cross-sectional analysis used a large, de-identified electronic health record (EHR)-based database, Explorys. covering over 60 million patient records between January 1, 2010 and October 31, 2019. We identified 1.7 million patients with AF using International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM) codes. Patients were stratified based on age, gender, insurance provider and type of AF therapy (medical vs. catheter ablation). The main outcomes were all-cause mortality and the type of treatment patient received.
Results:
Of the 1.7 million patients with AF we identified, 712,700 underwent catheter ablation. Females were significantly less likely to undergo catheter ablation compared with males for both paroxysmal AF (3.28% vs. 4.65%) and permanent AF (15.63% vs. 47.75%). Patients with Medicaid insurance were the least likely to receive catheter ablation (3.3%) compared with those with Medicare (46.5%) and private insurance (50.2%). Female patients had higher all-cause mortality as compared with male patients (10.64% vs. 7.82% for males; p < 0.0001) with the highest rate for female patients on Medicaid (Adjusted OR = 1.5; 95% CI: 1.4–1.6). In multivariable logistic regression adjusting for age group, AF subtype, and insurance category, female sex and Medicaid insurance remained independently associated with lower odds of receiving catheter ablation.
Conclusion:
In this large EHR-based analysis of patients with AF, female gender and Medicaid insurance were associated with lower use of catheter ablation and higher all-cause mortality. These findings highlight the need to better understand and address gender- and socioeconomic-based inequities in AF care and outcomes.
Introduction
Atrial fibrillation (AF), one of the most prevalent cardiac arrhythmias, poses a significant risk for ischemic stroke and is a major cause of morbidity and mortality worldwide. 1 With an estimated 37.6 million cases globally and a steadily increasing incidence, AF represents a growing public health challenge. 2 The management of AF typically involves medical therapy or interventions, such as cardioversion or catheter ablation. 1 Given the rising burden of this disease, it is essential to ensure equitable access to effective care, free from gender or socioeconomic biases.
Existing literature highlights significant disparities in AF management and outcomes based on socioeconomic status, race, ethnicity, and gender. 3 The effect of these inequities on the outcomes are complex and extend beyond the natural course of the disease. 3 In a meta-analysis of 30 studies of over 3.4 million participants, women with AF were shown to have higher all-cause mortality than men with AF. 4 Further, a study of Medicare patients showed that women, black and Hispanic individuals were less likely to receive advanced rhythm control therapies including cardioversion, antiarrhythmic drugs, and catheter ablations. 5 Rhythm control with antiarrhythmic medications or catheter ablation, in select patients with heart failure with reduced ejection fraction, has been shown to improve mortality and reduce hospitalizations.6–8
Despite the current evidence, there’s a need for a large-scale, real-world study to understand how gender and socioeconomic status combined, influence the management and mortality of AF. The current study aimed to investigate the socioeconomic and gender-based disparities in the management of AF and all-cause mortality.
Methods
This was a cross-sectional analysis of a large EHR-based commercial database, Explorys (IBM). 9 Explorys aggregates deidentified clinical data from 26 major health care systems across all 50 U.S. states and stores over 60 million unique patient records. Clinical data are standardized and mapped to common vocabularies, including SNOMED-CT for diagnoses and procedures. International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM) codes are mapped into the SNOMED-CT hierarchy, and procedure codes (including CPT) are similarly standardized. The platform is Health Insurance Portability and Accountability Act and Health Information Technology for Economic and Clinical Health compliant. The Case Western Reserve University/MetroHealth Medical Center Institutional Review Board deemed studies using Explorys as the dataset of record exempt from review because all patient information is deidentified.
The observation period for this analysis spanned January 1, 2010, through October 31, 2019. Patients with AF were identified using ICD-10-CM diagnosis codes corresponding to AF (I48.x series), which are mapped into SNOMED-CT within Explorys; the specific codes used are listed in Supplementary Table S1. Catheter ablation procedures for AF were identified using Current Procedural Terminology (CPT) codes commonly used for AF ablation (e.g., 93655, 93656). No free-text or natural-language search was performed.
For each patient meeting AF criteria, Explorys provides aggregate-level counts stratified by demographic and clinical categories. For this analysis, we obtained aggregate counts stratified by gender (male, female), age group, insurance provider (Medicare, Medicaid, private), AF subtype (paroxysmal vs persistent AF), and treatment with catheter ablation (yes/no). Insurance provider was used as a surrogate marker for socioeconomic status, recognizing that it is an incomplete measure.
For each gender and insurance type, we tabulated the number and proportion of patients undergoing catheter ablation and the number and proportion of deaths among those with AF and among those who underwent ablation. We further tabulated these measures separately for paroxysmal versus persistent AF and by age group.
Proportions of catheter ablation and mortality were compared between females and males across AF subtypes and insurance categories. Using binary logistic regression within Explorys, we compared outcomes across insurance types (Medicare vs. private, Medicaid vs. private, Medicare vs. Medicaid) and constructed a multivariable model with catheter ablation as the dependent variable and sex, age group, AF subtype, and insurance category as independent variables.
Results
Among the 1.7 million patients identified with AF, of whom 45% were female. Among this cohort, 712,700 patients underwent an AF ablation procedure. The baseline characteristics of the patients are not available as it was based on the aggregate data. Among patients with AF (paroxysmal and persistent), females were consistently less likely to receive catheter ablation for both paroxysmal AF (3.28% of females vs. 4.65% of males) and persistent AF (15.63% of females vs. 47.75% of males) Table 1.
Baseline Characteristics of Patients with Atrial Fibrillation (Aggregate-Level Data)

Dual Medicare–Medicaid eligibility was captured in the database and included in multivariable analyses, but is not shown separately in aggregate baseline tables due to reporting limitations of the Explorys platform.
The insurance type among patients with AF who received catheter ablation was Medicare in 46.5%, Medicaid in 3.3% and private insurance in 50.2% of patients. As shown in Figure 1, females had higher all-cause mortality across all insurance types (10.64% vs. 7.82% for males; p < 0.0001). The highest mortality was observed in female patients with Medicaid insurance group compared with female patients in the private insurance group (Adjusted OR = 1.5; 95% CI: 1.4–1.6) as shown in Figure 2. Moreover, the lowest all-cause mortality was observed in privately insured male patients. Among patients who underwent catheter ablation, females had a higher all-cause mortality rate compared with males (10% vs. 7%, respectively). As shown in Figure 3, mortality rates for both genders increased with age, with a consistently higher mortality observed in Medicaid patients across all age groups. In multivariable logistic regression adjusting for age group, AF subtype, and insurance category, female sex remained significantly associated with a lower likelihood of undergoing catheter ablation. Medicaid insurance and older age were also independently associated with reduced odds of ablation, while private insurance was associated with higher likelihood of receiving catheter ablation. These adjusted findings are consistent with the unadjusted patterns observed in the aggregate data.

All-cause mortality stratified based on gender and insurance type.

Forest plot for odds ratio mortality stratified based on insurance type and gender.
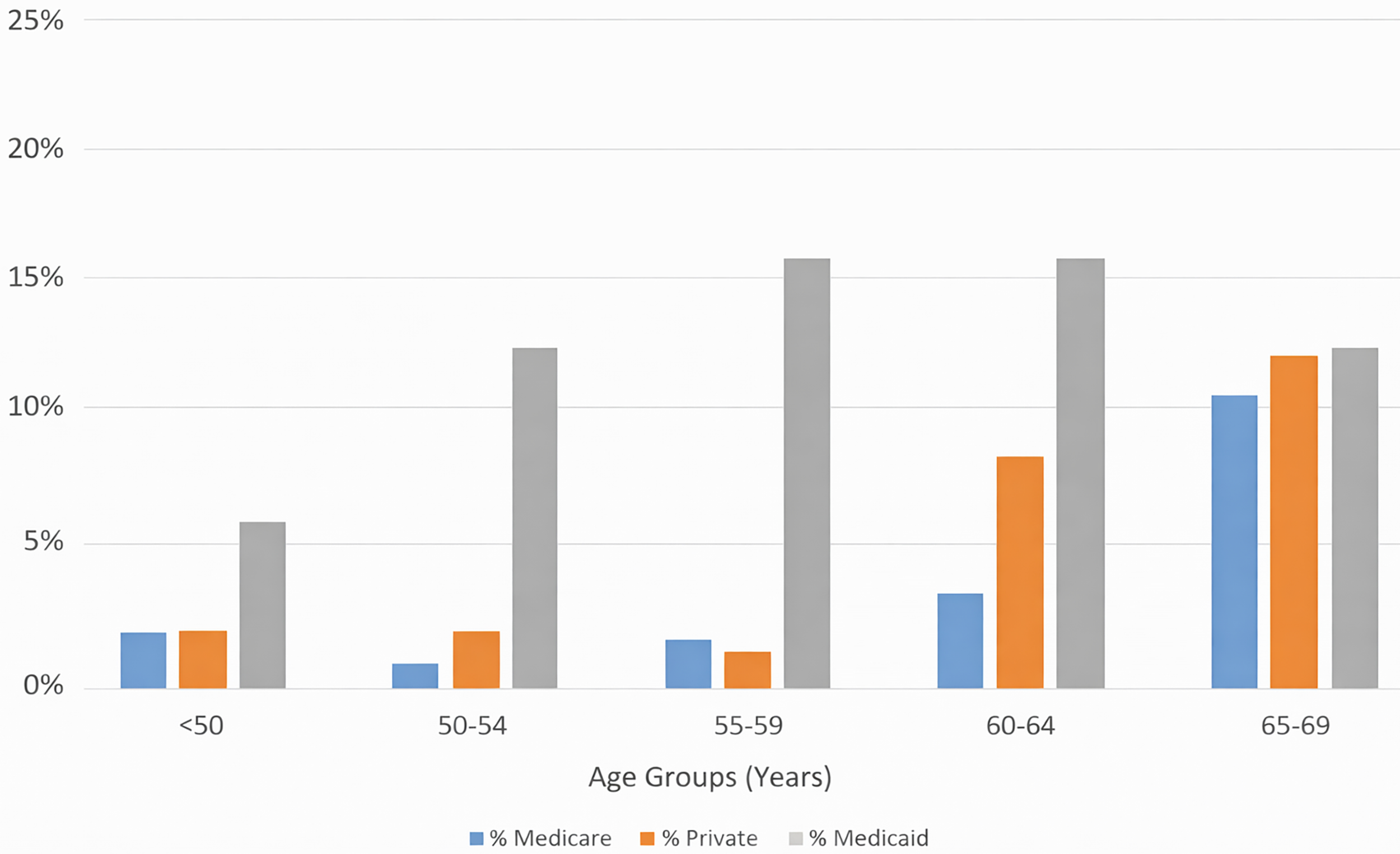
All-cause mortality in different age groups stratified based on insurance type.
Discussion
In this cross-sectional study of patients with AF utilizing a large-scale, real-world patient database, there was a significant difference in all-cause mortality based on gender. Our findings align with a growing body of literature highlighting sex differences in cardiovascular disease outcomes and management that disproportionately affect women.10–12 It has been shown that delineating the risk factors that are unique to women is crucial to bridging the treatment gap and improving cardiovascular outcomes in females. 13 The same disconnect applies to AF, where gender, race, and socioeconomic status still seem to affect mortality and the choice of management. 3 The higher all-cause mortality we observed in females with AF is consistent with a 2016 meta-analysis by Emdin et al., which also reported a higher risk of all-cause mortality for females (OR 1.12, 95% CI 1.07–1.17). 4
The gender-based disparity in choice of AF therapy is a critical finding of this study. Our results, showing that females are less likely to receive catheter ablation, are consistent with previous research; one study found that females were less likely than males to receive catheter ablation as a therapy (Adjusted HR 0.65; 95% CI 0.63–0.68; p < 0.001). 5 This is particularly concerning given the proven benefits of catheter ablation. For example, in patients with heart failure with reduced ejection fraction, randomized clinical trials have shown improved outcomes, including mortality.6–8 Moreover, some small studies have demonstrated its superiority of catheter ablation over antiarrhythmic medications in patients with AF with heart failure in maintaining sinus rhythm and improving left ventricular systolic function.14,15 Compounding this disparity, studies have shown that females are also less likely than males to be prescribed oral anticoagulants despite having a similar CHA2DS2VASc score, particularly for those under 75 who have a comparable adjusted risk of ischemic stroke.5,14
Prior studies have similarly demonstrated sex-based and socioeconomic disparities in the use of rhythm control strategies for AF. In a large registry analysis, Piccini et al. reported that women were significantly less likely to undergo catheter ablation despite having comparable symptom burden and stroke risk profiles, suggesting systemic referral and treatment biases rather than clinical appropriateness alone. Additionally, a meta-analysis by Al Halabi et al. evaluating catheter ablation in patients with AF and heart failure demonstrated substantial mortality and hospitalization benefits, underscoring the clinical consequences of unequal access to advanced rhythm control therapies. Together, these findings reinforce that the lower utilization of catheter ablation observed in women and socioeconomically disadvantaged populations may contribute directly to the higher mortality rates identified in our study.15,16
Furthermore, our findings suggest that socioeconomic factors likely contribute to disparities in AF management and outcomes. Patients insured by Medicaid were less likely to receive catheter ablation and had higher all-cause mortality than those with Medicare or private insurance, and the highest mortality was observed in women insured by Medicaid, indicating a potential “double disadvantage” of gender and socioeconomic vulnerability. However, insurance status is an imperfect proxy for socioeconomic status, and we were unable to assess other important domains such as income, educational attainment, employment, or neighborhood-level deprivation. These limitations underscore the need for future studies with more granular socioeconomic data to better characterize and address these inequities.
The main strength of this study is the use of a large dataset consisting of 1.7 million patients, which provides a robust and generalizable foundation for delineating these disparities. This large sample size allowed for powerful statistical analyses and the identification of significant differences that might be missed in smaller studies. However, several limitations must be acknowledged. As a cross-sectional study, our analysis can establish associations but not causality. The deidentified nature of the Explorys database precluded access to individual-level patient characteristics such as specific comorbidities, which could act as confounding factors. Furthermore, information on individual procedure-related complications was unavailable. The reliance on ICD-10-CM codes, while standard, is subject to coding errors and misclassification bias.
Conclusion
In this large-scale, cross-sectional study of patients with AF, we identified significant gender and socioeconomic disparities in both AF management and all-cause mortality. Female patients and those with Medicaid insurance were less likely to receive catheter ablation and experienced higher mortality rates. These findings underscore the urgent need for further research to delineate the root causes of these inequities. Addressing these disparities is crucial to ensuring equitable and optimal care for all patients with AF.
Authors’ Contributions
All authors participated in the research and preparation of the article as per the International Committee of Medical Journal Editors.
Footnotes
Acknowledgment
Author Disclosure Statement
All authors have no conflicts of interest to disclose.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.