
Abstract
Objective
In the first STROKESTOP atrial fibrillation screening study, participation was influenced by socio-demographic and geographic factors. To improve uptake in the second study, two screening sites were added, closer to low-income neighbourhoods which had very low participation in the first study. This paper aims to analyse the geographic and socio-demographic disparities in uptake in the second trial and compare the results with the first trial.
Methods
Inhabitants of the Stockholm region born in 1940 and 1941 were randomised 1:1 to be invited to screening or serve as controls. Medical history, blood samples and single-lead-ECG were collected. Invitee’s residential parish was used for geo-mapping analysis of the geographical disparities in participation, using hierarchical Bayes methods. Individual data for participants and non-participants were obtained for the socioeconomic variables: educational level, disposable income, immigrant and marital status.
Results
Higher participation was observed in those with higher education, high income, among non-immigrants and married individuals. Participation between the first and second studies improved significantly, where additional screening sites were introduced. These improvements were generally significant, in each population group according to socio-demographic characteristics.
Conclusion
Decentralisation of screening sites in an atrial fibrillation screening program yielded a significantly positive impact on screening uptake. Adding local screening sites in areas with low uptake had beneficial impact on participation across a wide spectrum of socio-demographic groups. Decentralised screening substantially increased the screening uptake in deprived areas.
Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia and a major cause of cardiovascular mortality and morbidity. 1 In Sweden, it affects at least 2.9% of the population aged >20. Prevalence increases with age, reaching 9.7% at age 70–79. 2 The global burden of AF is likely to increase, as the prevalence is expected to double within the next 30 years due to expected demographic shifts. 3 AF is a known risk factor for heart failure, dementia and death, 4 , 5 as well as ischaemic stroke. 6 In high-risk patients, stroke risk can be reduced by at least two-thirds with oral anticoagulant therapy. 7 Stroke can be the first clinical manifestation of AF, as AF can be both asymptomatic and intermittent. 8 Screening for AF has been proposed in the European Society of Cardiology guidelines, and in the AF-SCREEN International Collaboration white paper from 2017, although large, randomised outcome studies are still needed to strengthen this case. 9
An important factor for screening success is uptake. Previous studies have shown that the likelihood of attending a screening program is correlated to socioeconomic status.10,11 In a sub-study to the STROKESTOP study (SS1), in which socio-demographic differences of the participants were studied, participation was significantly influenced by socio-demographic factors. 12 Lower education level, lower income level and immigrant status were all associated with lower uptake. Gender did not influence participation. Geographical inequalities in the screening participation beyond socio-demographic characteristics were also observed. In investigating new strategies to address inequalities in screening uptake, preventive efforts in socioeconomically disadvantaged neighbourhoods may be worthwhile. 13
The findings from SS1, a study of AF-screening among Swedish participants aged 75, 14 were considered when designing the STROKESTOP II study (SS2) protocol. 15 One major intervention was decentralised screening. Two screening sites were added in SS2, located closer to low-income neighbourhoods with a very low participation in SS1.
This study aimed to analyse geographic and socio-demographic disparities in the uptake of the SS2 study and compare the results with those from SS1.
Methods
The SS2 study design has previously been published. 15 Briefly, half of all inhabitants in the Stockholm region born 1940 and 1941 were identified using their personal identification number by Statistics Sweden. A stratified, gender- and age-based 1:1 randomisation provided an intervention group to be invited to participate in an AF screening study, while the other half served as a control group. No information or intervention was provided to the control group. The intervention group was invited to screening via mail with a maximum of two reminders for non-responders. The only inclusion criteria were birth year and residence in the Stockholm region for those in the intervention group; there were no exclusion criteria. The intention-to-screen arm comprised 14,112 persons, and data were collected between April 2016 and February 2018. Participants received oral and written information, and signed informed consent documents. Participants reported their medical history, and those without previous AF had NT-proBNP analysed from venous blood samples and recorded a 30 s, handheld single-lead-ECG using the Zenicor II device (Zenicor Medical Systems, Stockholm, Sweden). Depending on the NT-proBNP results, participants were stratified to either prolonged ECG screening, consisting of two-week intermittent ambulatory handheld ECG recordings using the Zenicor II device, or to no further ECG screening. The results from the AF screening have been published. 16 This study addressed participation among those who were invited; data from the control group were not relevant. The study flow chart is shown in Figure 1.
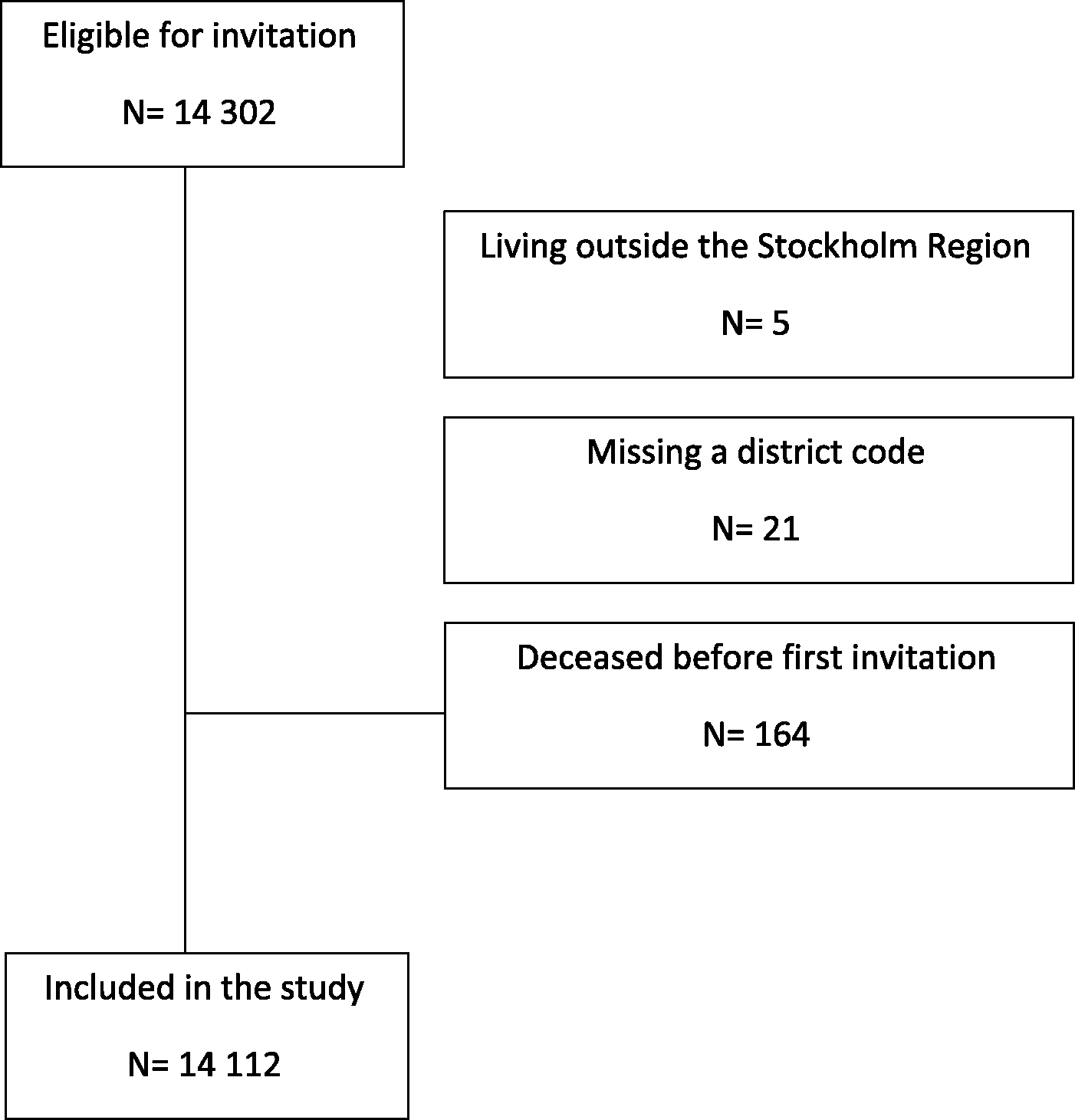
Study inclusion flow chart.
To improve screening uptake, a website (www.strokestop2.se) was launched providing general information on AF, the study procedure and the study team. Patient information was translated to the nine most common languages in Sweden. Three different screening sites were used to shorten the travel distance for participants. The Sabbatsberg Hospital site was the same as used in SS1. The two new sites in SS2 were Södertälje Hospital and Karolinska University Hospital.
The SS2 database comprises information on each invited person’s residential parish (99 parishes in Stockholm). Statistics Sweden provided both participants and non-participants with anonymised individual data for each of the following socioeconomic variables: educational level classified based on the number of school years completed (≤9 years, i.e. primary school; ≥10 years, i.e. secondary school/pre university/university), disposable income (<15,000 Euro/year, referred to as “low”; 15,000–30,000 Euro/year, “medium”; >30,000 Euro/year, “high”), immigrant (born in Sweden, born abroad) and marital status (unmarried, married, divorced, widow/widower). Invited persons who could not be classified based on the information in the national registers were grouped into an “other/unknown” category of the variable at issue. The same socio-demographic variables were considered in SS1, but we did not obtain individual-level data on the socio-demographic characteristics. The data used in SS1 were aggregated at parish level.
p-Values for the null hypothesis of equal participation in men and women and for each socioeconomic variable were obtained by chi-square test. All tests were two-sided, and a value of p < 0.05 was considered significant.
Geo-maps of Stockholm county displaying spatially smoothed participation ratios (PRs) were estimated by hierarchical Bayes methods. A parish-specific PR is based on the observed-to-expected numbers of participants, where the expected number was obtained from the sex-specific participation rates for the total study population of the county. Spatially smoothed PRs were obtained by running the hierarchical Bayesian mapping model (the Besag-York-Mollié model) implemented in the Rapid Inquiry Facility program. 17 This procedure allows parish-specific participation rates to be smoothed towards global and local mean participation rates across the county, yielding “shrinkage” of the conventional observed to expected ratios—in line with principles for multi-level modeling. 18 The corresponding statistical certainty geo-maps were obtained by calculating the posterior probabilities of a PR > 1 given the data, denoted Pr (PR > 1|data), using the Bayesian approach.
A parish with data yielding strong statistical evidence of elevated participation, more precisely Pr (PR >1|data)> 0.90, was coloured green in the certainty geo-map. By contrast, a parish with lowered participation rate, Pr (PR < 1|data) >0.90, was coloured red. The remaining parishes were coloured yellow. The choice of 0.90 for identifying an area with elevated/lowered participation rate has been shown to provide a cut-off with reasonable sensitivity and high specificity. 19
Binary logistic regression was used for the univariate and multivariable analyses of socio-demographic factors for the outcome reflecting participation or non-participation.
The statistical computations were performed by using IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp. For the spatial analyses, the Rapid Inquiry Facility free software (RIF 3.12). 17
The study complies with the Declaration of Helsinki, and the protocol was approved by the regional ethics committee (DNR 2015/2079–31/1). Informed consent was obtained from all participants in the screening program. ClinicalTrials.gov identifier: NCT02743416.
Results
Overall participation was 48.6%, a significant increase (p = 0.006) from the 46.9% uptake in SS1 in the Stockholm region. Figure 2 shows the statistical certainty geo-maps of PRs in the SS1 study and the SS2 study in Stockholm county displaying, for each of the 99 residential parishes, the spatially smoothed PRs which were evidently above or below 1. The addition of the two new southern Stockholm sites in SS2 increased the participation rates in those areas. In comparison, the northern region is depicted as red in SS2. This was due to increased uptake in the southern part, not because of lower actual uptake rates between the STROKESTOP trials.
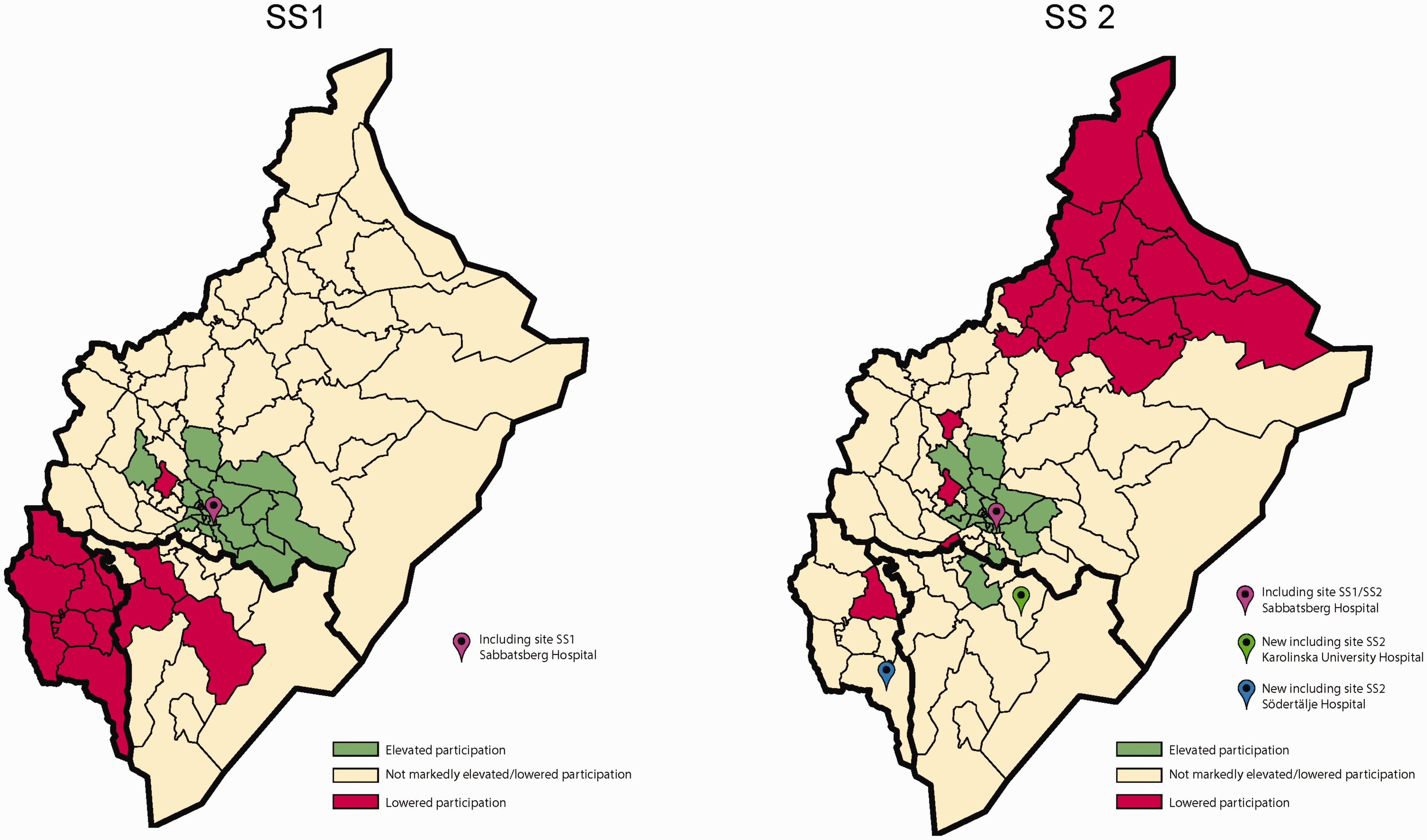
Statistical certainty geo-maps of participation in the SS1 study and the SS2 study in Stockholm county.
Compared with the same catchment areas and corresponding PRs from SS1, SS2 participation rates were significantly higher in the areas where a screening site had been added. In the area surrounding the Karolinska University Hospital site, uptake increased from 41% to 47% (p < 0.001), a 15% relative increase. In the vicinity of the Södertälje Hospital site, uptake increased from 28% to 43% (p < 0.001), a 54% relative increase. Uptake was not significantly changed (50% in SS1 vs. 49% in SS2, p = 0.17) in the catchment area of the Sabbatsberg Hospital site (the one site used in both studies, but with a smaller catchment area in SS2). In all three catchment areas, higher participation was observed among women, those with higher education, those with high income, among non-immigrants and among married individuals (see Table 1). Uptake was improved most markedly in the area around the Södertälje Hospital site, where a 1.5-fold increase was observed also in the socioeconomically weaker population groups (from 21% to 32% participants in the low education group, 22% to 32% participants in the low-income group and 31% to 47% participants in the immigrant group). The increases in uptake were pronounced (at least 10 percentage points) in socially deprived population groups with very low participation in SS1.
Participation rates in SS2 according to catchment area and socio-demographic characteristics, compared with corresponding rates in SS1.
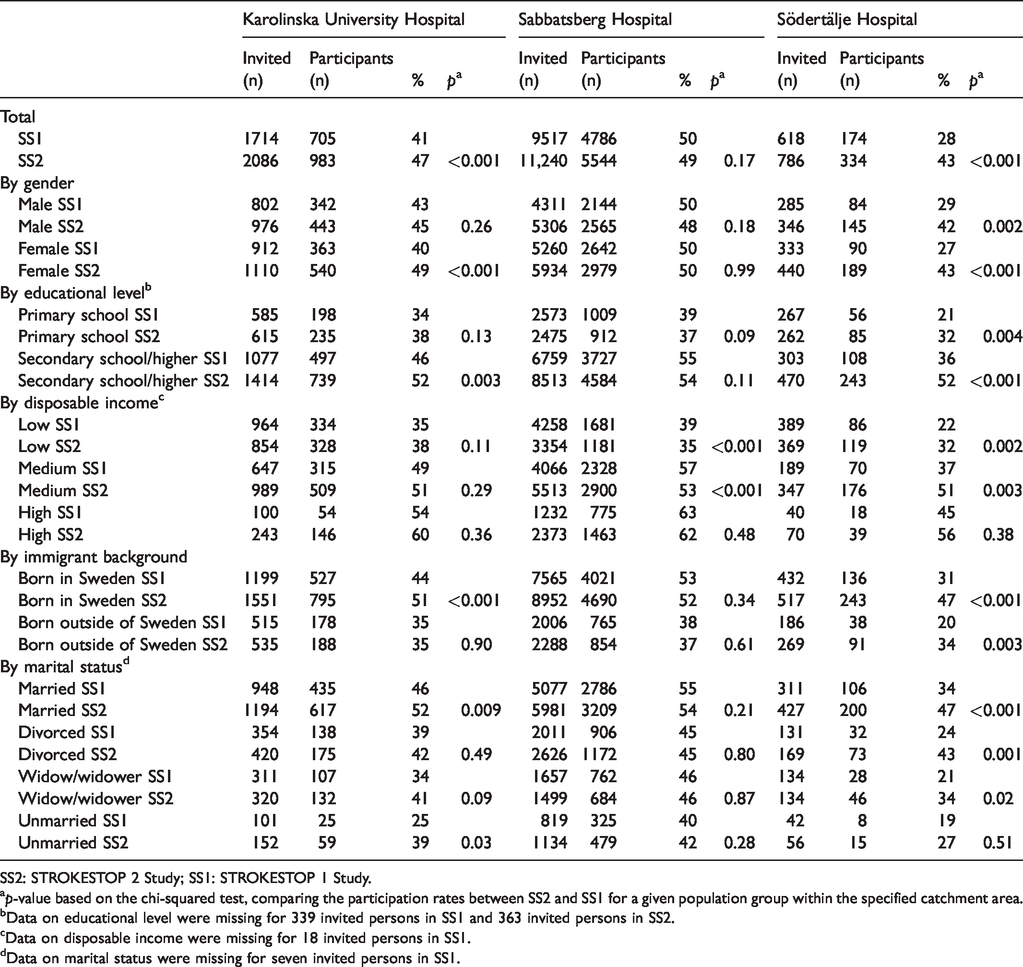
SS2: STROKESTOP 2 Study; SS1: STROKESTOP 1 Study.
ap-value based on the chi-squared test, comparing the participation rates between SS2 and SS1 for a given population group within the specified catchment area.
bData on educational level were missing for 339 invited persons in SS1 and 363 invited persons in SS2.
cData on disposable income were missing for 18 invited persons in SS1.
dData on marital status were missing for seven invited persons in SS1.
A univariate logistic regression analysis showed that the odds of participation in SS2 were highest among women, those with higher education, those with high incomes, non-immigrants, married people and those living in the catchment area belonging to the Sabbatsberg Hospital site. The difference in odds ratio in all categories compared with reference was significant. In the multivariable analysis, the odds of attendance were consistent with those in the univariate analysis, except in the catchment area where the difference became insignificant (see Table 2).
Results from logistic regression analyses based on data from SS2.
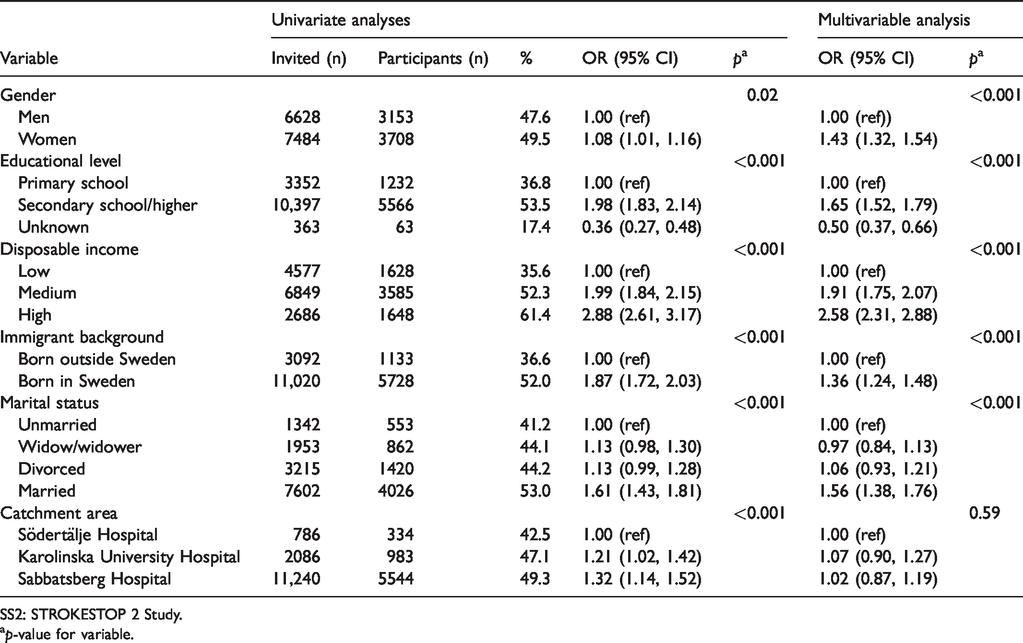
SS2: STROKESTOP 2 Study.
ap-value for variable.
Discussion
This study illustrates that geographic distance to the screening site is of high importance, and that increasing the number of sites has the potential to significantly increase uptake in screening studies. Socio-demographic factors have a significant impact on AF screening uptake. The increased uptake due to decentralised screening was particularly notable in attendees with socio-demographic factors which were previously associated with higher odds of attending. Notably, we also observed markedly increased participation in population groups with low socioeconomic status. The outcome of efforts to increase participation in socioeconomically weak groups was most pronounced in the catchment area of the Södertälje Hospital site, where the participation was very low in SS1. These results indicate that decentralised screening can substantially increase uptake in deprived areas. This site is further away from the site used in SS1 than the other new site, Karolinska Hospital, which could be one reason for the larger increase in uptake observed around the Södertälje site.
These results reinforce the importance of geographic proximity in screening. We found that screening uptake in those normally not attending screening (i.e. with the lowest educational level and income) might be affected by proximity of screening sites. Lower participation in this screening study goes hand in hand with increasing socio-demographic deprivation, which confirms the results from a previous study in which men aged 65 were invited to abdominal aortic aneurysm screening and those with lower socioeconomic status showed lower compliance. 11 A recent systematic review found inconsistent evidence for lower socioeconomic status and AF diagnosis, but those with lower socioeconomic status showed poorer outcomes when AF was present. 20 A study of four different strategies to reduce the socioeconomic gradient of uptake in the English NHS Bowel Cancer Screening Program found only an enhanced reminder letter to have an effect on the socioeconomic gradient. 21 These results stress the need for targeted actions to increase uptake in those with lower socioeconomic status, although a systematic review found that barriers and facilitators to participation in health checks for cardiometabolic disease were heterogenous, which makes it difficult to develop a “one size fits all” approach for increased uptake. 22
Travel distance to the screening site probably influences participation, as the increase in participation was markedly higher in the uptake areas of the two new sites compared with the area around the one site used in both STROKESTOP trials. The area with the lowest participation rates in SS2 was the one farthest from any screening site (Figure 2). In a Danish study on screening for vascular disease, specially trained nurses operated mobile clinics in hospitals, general practitioners’ offices and even in a town hall, resulting in an uptake of 74.7%. 23
All invitees in SS2 were aged 75–76, and there were no exclusion criteria. This could possibly mean that some invitees were not able to attend (i.e. in assisted living facilities, severe disabilities or dementia diagnosis), and thus the sampling frame should possibly be smaller than it is in this study.
As this is a study on AF screening, and not an established screening program, some non-responders may have been interested in participating in an established routine screening program, but not in a clinical trial. The European Society of Cardiology 2016 Guidelines for the management of AF gives a class Ib recommendation for opportunistic screening, and a IIb recommendation for systematic screening in individuals aged >75 or those at high stroke risk. This is based on studies showing increased detection of previously unknown AF in individuals with screening and the fact that the connection between AF and stroke in high-risk individuals is well established. 1 No study has shown that screening for AF reduces stroke incidence, although several are ongoing, including the STROKESTOP trials. Due to the lack of evidence, the US Preventive Services Task force recommendation statement on screening for AF from 2018 does not recommend population screening for AF and concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for AF. 24 Similarly, the 2019 UK National Screening Committee concluded that screening for AF is not recommended, based on a lack of trials that compare formal screening with routine clinical diagnosis, and that evaluate clinical health outcomes. 25
Our study has some limitations. The comparison of the two STROKESTOP trials is a comparison of two different study populations, as the studies and individual data collection are performed a few years apart. Therefore, the participants are not the same, and the demographics of the areas may have changed in these years, potentially introducing misclassification bias. Noticeably, there seems to have been a systematic change in the disposable income category, with a lower proportion of individuals in the lowest income category in SS2 compared with SS1, a shift that makes the comparison of the studies potentially biased. Such a bias would mean that we would detect a difference that reflects a change in demographics, rather than in participation. In addition, the effects of changes (website, more languages in the patient information, more sites) made to increase the screening uptake cannot be separated. This study cannot answer which changes had the strongest impact, and this may decrease the study’s external validity.
Conclusion
Decentralisation of screening sites in an AF screening program yielded a significantly positive impact on screening uptake. The addition of local screening sites in areas with low uptake had a beneficial impact on participation across a wide spectrum of socio-demographic groups. Importantly, decentralised screening increased substantially the screening uptake in deprived areas.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation. KG has received lecture fees from Pfizer. TF has received lecture fees from Pfizer and research grants from Boehringer-Ingelheim. ES has received lecture fees from Bayer, Bristol-Myers Squibb-Pfizer, Boehringer-Ingelheim, and Sanofi. JE has received lecture or consultant fees from Bristol Myers Squibb, Pfizer, Merck Sharp & Dome and Medtronic as well as research grants from Roche Diagnostics. AH and US have no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Roche diagnostics, The Swedish Heart and Lung Foundation, Carl Bennet AB. JE and ES are supported by the Stockholm County Council (clinical research appointment). ES has received grants from the Swedish Society of Medicine and the Swedish Heart and Lung Foundation for this work, US was financed by grants from the Swedish Research Council for Health, Working Life and Welfare (grant 2017–00414). TF has received unrestricted research grants from Boehringer-Ingelheim and Stiftelsen Hjärtat.