
Abstract
Background:
The American Foregut Society (AFS) is dedicated to advancing patient care and digestive health within the realm of foregut disease. One of the most common and debilitating esophageal conditions is gastroesophageal reflux disease (GERD). The Hill grade is an endoscopic classification of the esophagogastric junction (EGJ) based on the appearance of the gastroesophageal flap valve from a retroflexed view of the hiatus. This endoscopic classification provides insight into the anatomic disruption of the EGJ which has been shown to correlate with GERD. However, clinical utilization of this classification by endoscopists has been limited due to the perceived relevance and subjectivity of the classification. With the advent of endoscopic treatment options for GERD, there is renewed enthusiasm to develop a grading system of the EGJ that can objectively define anatomical impairment and reduce interobserver grading variability.
Methods:
The AFS convened a 13-member working group tasked with reviewing the Hill grade classification and formulating a proposal for its revision utilizing a modified Delphi method. This white paper summarizes the output from this working group.
Results:
The working group concluded that all components of the antireflux barrier—the lower esophageal sphincter and its sling fibers, the crural diaphragm, and the gastroesophageal flap valve—contribute to EGJ integrity. Using defined objective parameters of extent of hiatal axial herniation and crural disruption and presence or absence of a flap valve, the new AFS classification stratifies EGJ integrity from normal (grade 1) to increasing degrees of EGJ disruption (grade 2-4) beginning with loss of the flap valve and progressing to increasing degrees of crural disruption and hiatus hernia. This AFS classification also stipulates appropriate endoscopic methodology to utilize in making the assessment and provides a basic nomenclature for communication among endoscopists.
Conclusions:
The AFS endoscopic classification of the EGJ expands on the Hill classification by including assessment of axial hiatal hernia length (L), hiatal aperture diameter (D), and presence or absence of the flap valve (F) making it more comprehensive - LDF components. Future directions include validation studies correlating the ability of the AFS classification in predicting the presence and severity of GERD.
Keywords
Introduction
Gastroesophageal Reflux Disease (GERD) is the most common chronic esophageal disorder.1,2 An important mechanism for the development of GERD is the deterioration of the antireflux barrier (ARB).2 -5 The Hill grade is an endoscopic classification of the ARB specifically focused on the flap valve that was developed by Hill et al and reported to correlate with the severity of GERD.5,6 However, utilization of this classification by endoscopists has been limited, partly due to skepticism as to its relevance and the perceived subjectivity in its application. Nonetheless, with the advent of endoscopic treatment options for GERD, there is increasing enthusiasm to develop an improved endoscopic grading system of the esophagogastric junction (EGJ) that can accurately define anatomical impairment using objective, relevant endoscopic findings with minimal interobserver variability. Toward that goal, the American Foregut Society (AFS) convened a working group tasked to critically review the Hill grade classification and formulate a proposal for its revision utilizing a modified Delphi method. This white paper summarizes the discussion from the working group including an in-depth review of the mechanisms of the antireflux barrier, the Hill grade along with its original supporting data, the pitfalls of the Hill grading system, the issue of interobserver variability, and a proposal for a new AFS endoscopic classification of EGJ integrity.
Understanding the Hill Grade Classification
In 1996, Hill et al reported on an in vitro cadaver model wherein they found that there was a pressure gradient between the esophagus and the stomach across the EGJ. 5 Since there is no LES function in a cadaver model, the gradient was attributed to a competent “flap valve,” an anatomic musculomucosal fold locate between the distal esophagus as it enters the stomach at the angle of His and the gastric fundus. This flap valve can be readily seen from the retroflexed endoscopic view. Hill and colleague proposed that the endoscopic view of the flap valve correlated with the degree of reflux. 5 They then conducted a small in vivo study of control patients without reflux (n = 12) and a cohort of patients with reflux (n = 12) reporting a distinct difference in appearance of the flap valve. 5 They concluded that the appearance of the valve was a better predictor for the presence of reflux than measurement of the LES pressure. 5 Based on these findings, Hill et al proposed a 4-point grading scale of the retroflexed endoscopic visualization of the EGJ. 5 With a Hill grade I flap valve, there was tight approximation of the ridge of the gastroesophageal fold against the endoscope. With a Hill grade II flap valve, there was a loose grip of the gastroesophageal valve around the endoscope that intermittently opens. As evident in the schematic drawing of Hill and Kozarek grade I & II (Figure 1), both have a long segment of intraabdominal esophagus without a hiatal hernia and both are considered normal.5,7 With Hill grade III flap valve, there was a vertical length of hiatal hernia as judged by the distance between the squamocolumnar junction and the diaphragmatic crura impression, lack of intraabdominal esophagus, and an open hiatus on retroflexion. Finally, a Hill grade IV was similar to Hill grade III but with a larger, and wider diaphragmatic opening with herniation of the stomach into the mediastinum with insufflation. Hill grades III and IV were considered abnormal and observed in patients with reflux.6,7 Subsequent studies have demonstrated that Hill grade III and IV are associated with symptomatic and pathologic GERD and erosive esophagitis.8,9
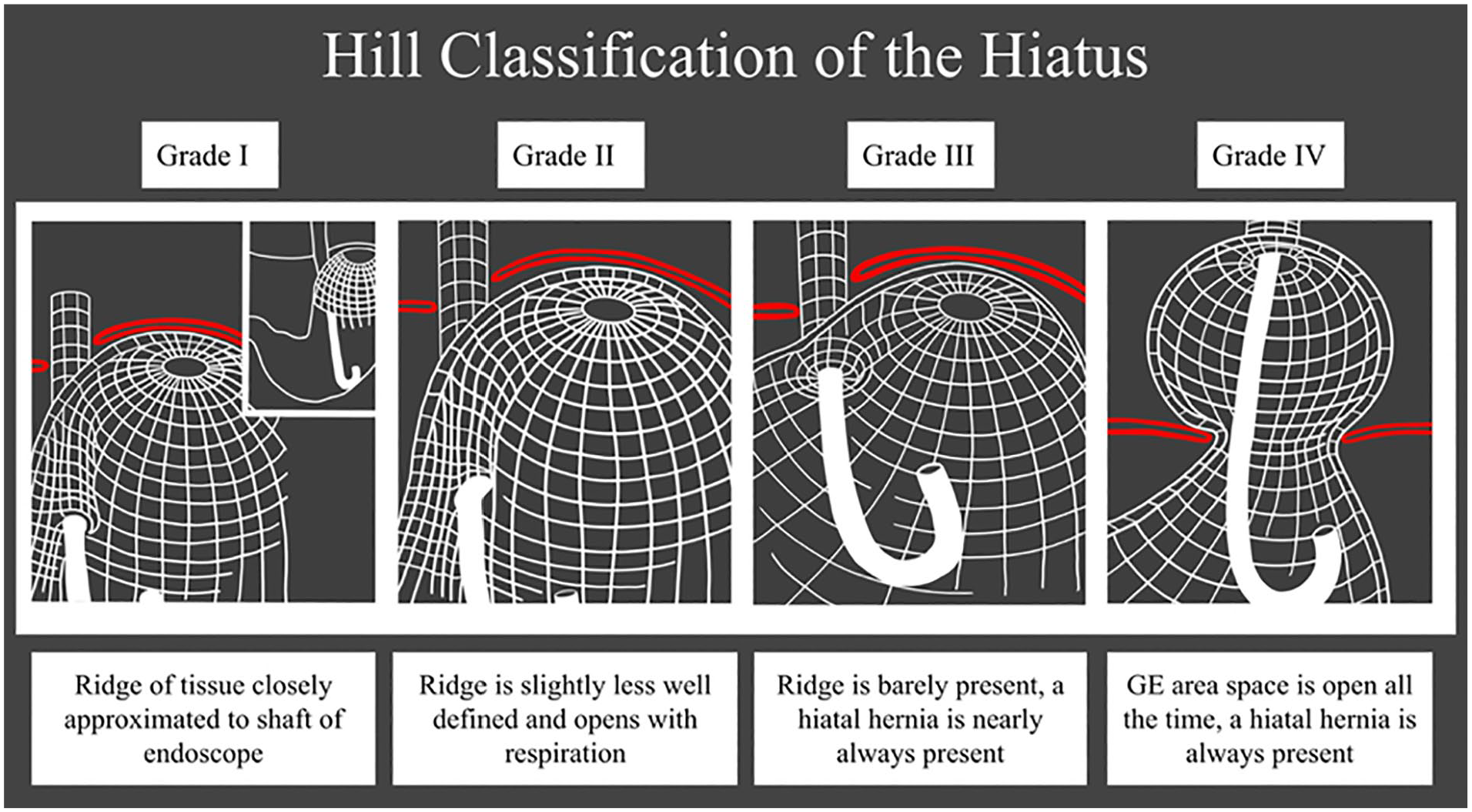
The original schematic description of the Hill classification of the hiatus with grade I and II being a normal flap valve while grade III and IV represent valves associated with reflux.
Limitations of the Hill Grade Classification
There are several limitations of the Hill grading scheme limiting its acceptance and routine utilization by endoscopists. For starters, the Hill grade is a classification focused on the flap valve which was a novel concept at the time. 5 Although the presence of a hiatal hernia is mentioned in the grading system, its parameters are vague and subjective. For example, grade III was described as nearly always associated with a hiatal hernia while grade IV was always associated with a hiatal hernia. Measurements of the hiatal hernia was not a factor used in differentiating among the grades. Second, the classification is vague regarding what characteristics define a competent flap valve. The defining characteristic for a Hill grade I flap valve was described as a ridge of tissue closely approximated to the shaft of the endoscope but this description is subject to interpretation. Third, schematically both grades I and II are considered normal with no explanation of why the distinction is important; essentially, both grades are subtle variations of a normal flap valve. Fourth, the grading system does not describe the optimal endoscopic technique to minimize interobserver variability in scoring the Hill grade. Variables such as time of insufflation and the use of provocative maneuvers to promote optimal grading of the flap valve were not described. Variability in endoscopic methodology is a major contributor to the variability in scoring among endoscopists. Additionally, endoscopic nomenclature and terminology for communication in the description of the anatomic EGJ have not been well developed. This is critically important as it provides a basis for standardized communication among endoscopists. Finally, the classification was developed by a thoracic surgeon, albeit a world renowned esophagologist, and was not widely adopted by medical or surgical societies and thereby limiting its use in routine upper endoscopy practices. Understanding these limitations is critical in devising an improved anatomic classification of the EGJ.
The AFS Hill Grade Revision Working Group
The AFS working group was comprised of 13 members tasked with developing an improved classification scheme for endoscopically gauging the endoscopic integrity of the EGJ. The group was composed of experts in foregut disease from gastroenterology (n = 7) and gastrointestinal surgery (n = 6). The expert consensus discussion was based on a modified Delphi method. A series of surveys that critiqued the Hill classification were circulated among the group and suggested improvements were solicited. The first group meeting discussed the following topics:
Current understanding on the components of the antireflux barrier and the Hill grade definition
Difficulties in obtaining a reproducible Hill grade
The strength of data supporting the Hill classifi-cation
Interobserver variability in applying the Hill grade in clinical practice
Understanding endoscopic nomenclature of EGJ
Pitfalls of the Hill grade classification
Proposals for revision of the Hill classification, standardization of endoscopic methodology, and standard endoscopic nomenclature for describing the EGJ
Based on survey results and the working group’s discussion, a proposal for a revised anatomic classification of the EGJ was developed. Following the initial virtual meeting, additional smaller group meetings were convened to further refine the preliminary proposal. Based on these discussions, a new classification was proposed and named the AFS endoscopic classification of EGJ integrity. This new classification is comprehensive in nature and seeking to improve the physiological relevance of the grading classification, to standardize the endoscopic methodology in applying it, and proposing nomenclature for endoscopic grading. A key difference of the new classification is that it focuses not only on the flap valve but also anatomic disruption of the diaphragmatic hiatus (crural separation) and the axial extent of hiatal herniation with an understanding that all 3 variables are integrally related and impact the ARB. The AFS classification stratifies EGJ integrity from normal (grade 1) to increasing degrees of anatomic disruption (grade 2-4) beginning with loss of the flap valve and progressing to increasing degrees of hiatal disruption and hiatus hernia.
AFS Position on Components of the Antirefux Barrier
In preparation for a discussion on the endoscopic assessment of EGJ integrity, it was important for the expert working group to have a common understanding of important factors contributing to the ARB. This was an important exercise to ensure a consistent understanding of factors contributing to the ARB both within this group, but also among the entire AFS membership. The literature on this topic varies widely with some investigators describing the ARB as being composed of 2 sphincters with the crural diaphragm representing the “external sphincter” and the lower esophageal sphincter (LES) representing the “internal sphincter.” On the other hand, Hill and Kozarek championed the anatomic flap valve an important component of the ARB.5 -7 The 2010 SAGES guidelines for surgical treatment of GERD states that although the exact nature of the ARB is poorly understood, the current view is that the ARB includes the LES, the diaphragmatic crura, and the phrenoesophageal ligament. 10 The phrenoesophageal ligament is a fascial extension from the crural diaphragm to the distal esophagus so it is commonly considered an extension of the crural diaphragm rather than an independent anatomic structure contributing to the ARB. Based on the survey of the AFS working group, there were 6 factors contributing to the ARB, albeit with some being interrelated: (1) the LES and its sling fibers, (2) the crural diaphragm, (3) the phrenoesophageal ligament, (4) the gastroesophageal flap valve, (5) the presence of intraabdominal esophageal length, and (6) the acute angle of His. The survey additionally asked which of these were the main factors contributing to the ARB and 3 rose to the top: the crural diaphragm, the LES and its sling fibers, and the gastroesophageal flap valve (Figure 2). The discussion noted that the intraabdominal esophageal length and an acute angle of His are both components of having an intact GEFV and therefore both belong under the main heading of the flap valve. This trilogy of mechanisms contributing to the ARB has long been recognized, even if frequently forgotten. Atkinson elegantly described them in a 1962 review appearing in Gut wherein he summarized the data supporting the contributions of the LES, the pinchcock action of the crural diaphragm, and “a flap of mucous membrane situated on the greater curvature aspect of the cardia” which “intragastric pressure would thrust this flap against the lesser curvature. . ..” 11 In contemplating the mechanism by which each of the trilogy functions, the working group consensus was that the gastroesophageal flap valve was a mechanical barrier to reflux, the LES was a physiologic barrier to reflux, and the crural diaphragm contribute both to the physiologic and mechanical barrier to reflux. The working group also noted that any process that mechanically disrupt the ARB can potentially induce GERD.12 -14
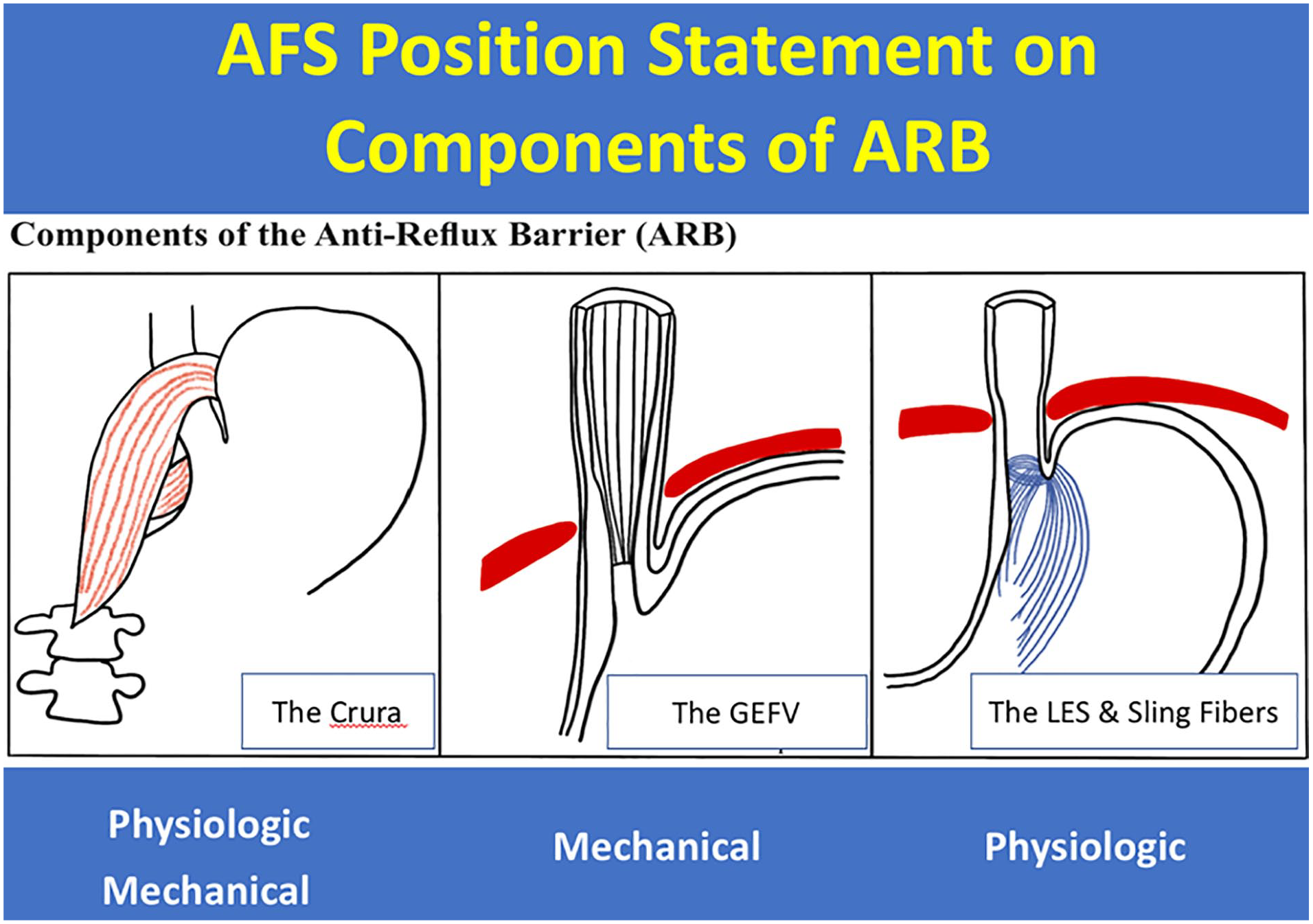
The AFS position on components of antireflux barrier: the crura of the diaphragm, the gastroesophageal flap valve (GEFV), and lower esophageal sphincter and its sling fibers. These 3 factors contribute to the mechanical and physiologic barriers to reflux.
Overview of Differences Between the Hill Grade and the AFS Endoscopic Classification of Esophagogastric Junction Integrity
An overview of the differences between the Hill grade and the new AFS classification is shown in Table 1. The emphasis of the Hill grade is the flap valve while the AFS classification considers the flap valve and degree of disruption of the hiatus as measured by the hiatal aperture and axial length of gastric herniation. This is a critical difference as any anatomic disruption of the EGJ will involve the disruption of both the flap valve and the diaphragmatic hiatus as these structures are integrally related. The development of a sliding hiatal hernia necessarily implies loss of esophageal intra-abdominal length and loss of a functioning flap valve. The Hill grade describes visual characteristics of the flap valve while the AFS classification utilizes visual characteristics to describe the presence or absence of a flap valve along with objective parameters to describe the integrity of the hiatus. The degree of axial hiatal length is measured in centimeters and dilatation of the hiatus and crural separation is also measured centimeters based on comparison with the diameter of the endoscope which is approximately 1 cm when utilizing a standard scope. With Hill grading, both grade 1 and 2 are considered normal.5 After extensive discussion, the working group concluded that 2 variations of a normal valve were not necessary. Consequently, the AFS classification described a competent flap valve with AFS hiatus grade 1 leaving 3 grades (AFS hiatus grades 2-4) to describe the degrees of anatomic hiatal disruption, all with loss of a functioning flap valve. Another key emphasis of the AFS classification not discussed in the Hill classification is the accuracy of grading is predicated upon using endoscopic maneuvers to induce the optimal image showing the extent of hiatal anatomic disruption; and the accuracy of any visual classification begins with a systematic methodology to image the hiatus.
Overview Comparison of the AFS Versus Hill Classification of the Esophagogastric Junction (EGJ).
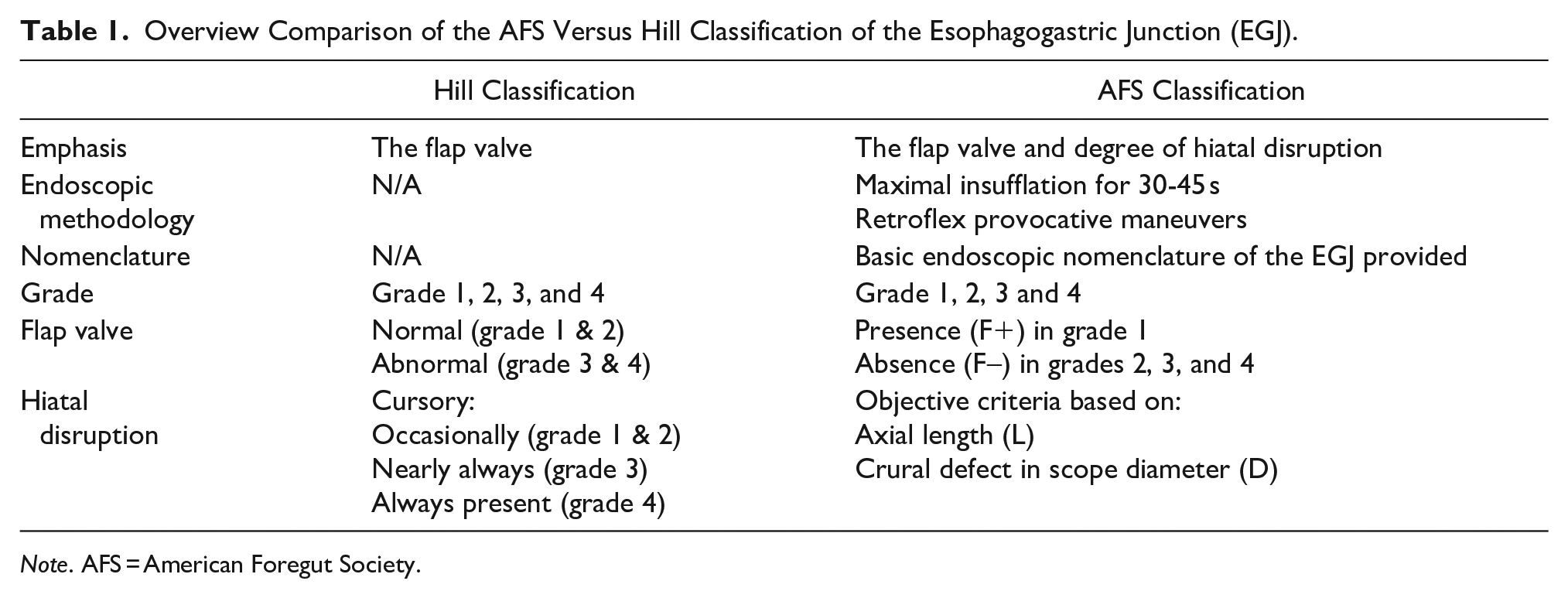
Note. AFS = American Foregut Society.
Optimal Endoscopic Methodology for Endoscopic Grading of EGJ Integrity
A key in obtaining optimal EGJ visualization is adequate insufflation. Suggested methods include endoscopic insufflation for approximately 30 to 45 seconds or insufflation until there is flattening of the gastric fundus rugal folds. Additionally, endoscopic rotational maneuvers in the retroflex position to induce potential sliding hiatal herniation should be performed. This is initiated by gently pulling the tip of the endoscope in the retroflex position along the lesser curvature to induce potential sliding hiatal herniation and widening of the hiatus aperture (Figure 3). This maneuver will provide an accurate assessment of the hiatal opening defect as measured in centimeters, along with assessment of the extent of hiatal herniation as demonstrated by real-time involution of the Z line. Upon completion of the provocative maneuver, the endoscopist can revert back to the forward view to measure the axial length of herniation, the distance between the Z line and diaphragmatic indentation. Without these suggested maneuvers, the EGJ can often be “under-graded” and contribute to interobserver variability.
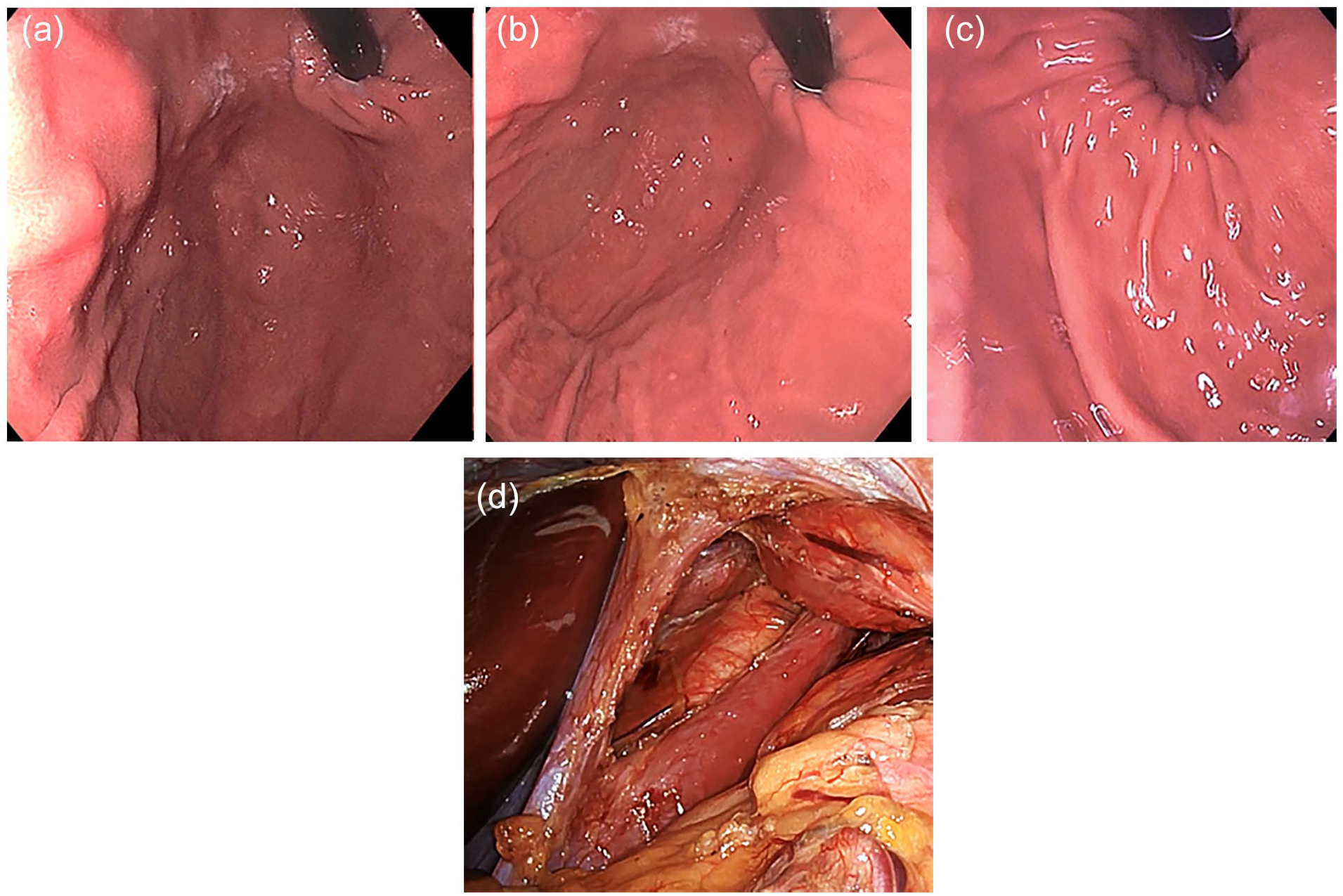
Endoscopic evaluation of the esophagogastric junction demonstrating (a) the initial appearance of the EGJ upon entry into the stomach, (b) progressive involution of the gastric folds and Z line with further insufflation, (c) further involution showing a large diaphragmatic aperture observed after full insufflation with provocative maneuvers, and (d) large diaphragmatic crural separation observed at the time of laparoscopy.
Basic Endoscopic Nomenclature of the EGJ
Establishing common nomenclature in describing EGJ anatomic characteristics is critically important as emphasized by Jobe et al in patients who underwent antireflux surgery. 15 Important characteristics include the orientation of the greater and lesser curvature in the retroflexed view along with the corresponding positioning of the anterior and posterior gastric walls (Figure 4). Understanding the orientation and nomenclature is important in standardizing reporting and communication among endoscopists. Also important is description of the gastroesophageal flap valve composing the lip and body of the valve. The length of the valve is the distance between the diaphragmatic impression in the distal esophagus and the Z line on the forward endoscopic view or can also be measured in the retroflexed view. This is clearly observed on endoscopic examination immediately after laparoscopic repair of the diaphragmatic hiatus.
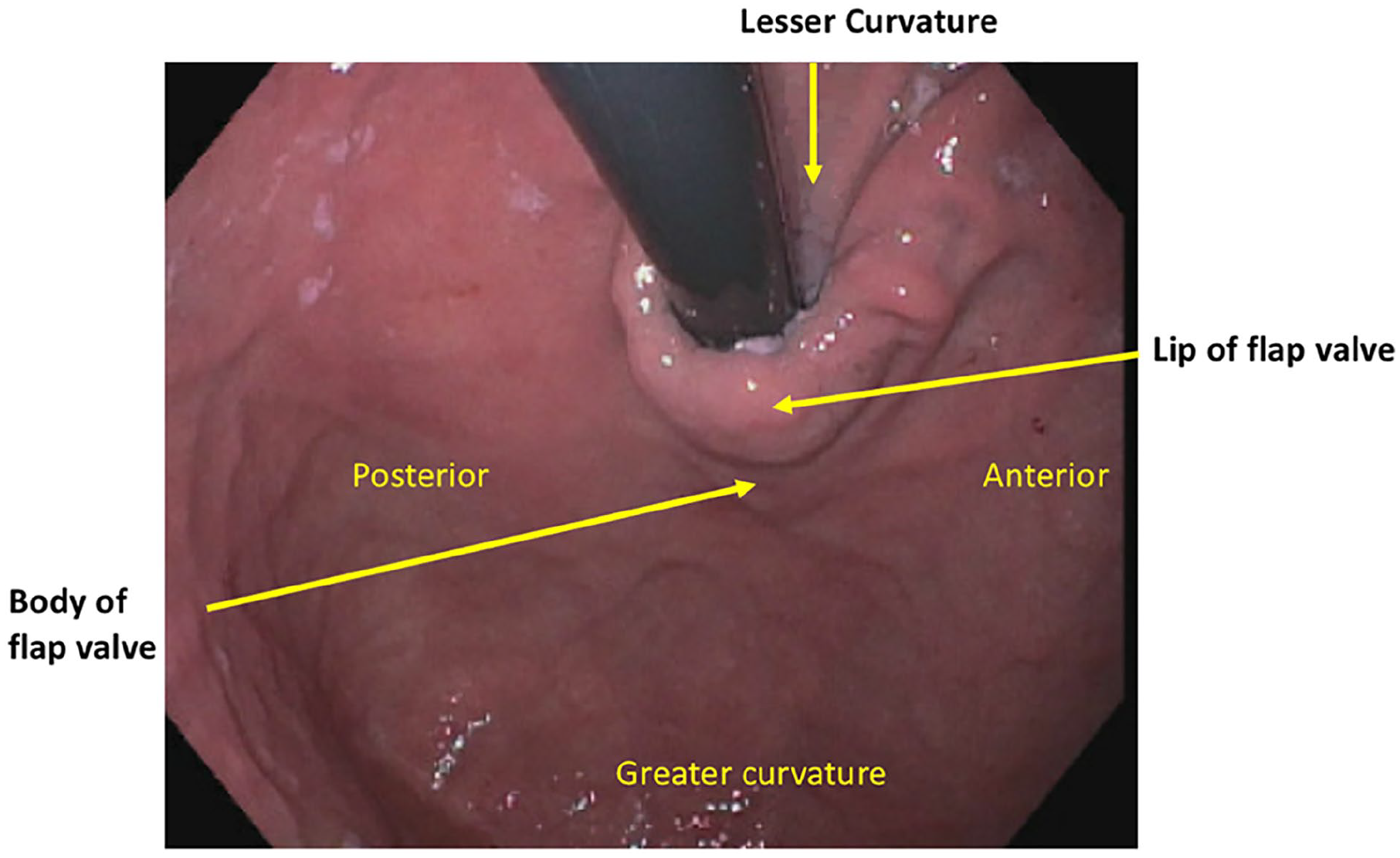
Endoscopic anatomic orientation of the esophagogastric junction and basic flap valve nomenclature.
The AFS Endoscopic Classification of Esophagogastric Junction Integrity
The new AFS classification of the EGJ is based on objective measurement on the degree of hiatal disruption and the presence or absence of a flap valve as characterized by the LDF components (Figure 5). Unlike the Hill grade which is a classification of the flap valve only, the AFS classification encompasses both the flap valve and the degree of hiatal disruption with an understanding that the hiatus and the flap valve are integrally connected and disruption of one component will affect the other. It is important to note that there are 2 components within hiatal disruption to include (1) hiatal defect or diaphragmatic aperture as seen in the retroflexed view which represents the degree of crural defect or separation and (2) the vertical length that represents the extent of axial gastric herniation. The L within the LDF components represents the hiatal hernia axial length measured in centimeters between the Z line and the diaphragmatic imprints; the D represents the largest aperture of the hiatus measured in centimeters with 1 conventional scope diameter being approximately 1 centimeter; and the F represents the present (F+) or absent (F−) of the gastroesophageal flap valve. Since the hiatal aperture measurement is based on centimeters, it is important to know your scope diameter to make an accurate measurement. For each AFS grade, the LDF components are indicated to minimize ambiguity and inter-observer variability.
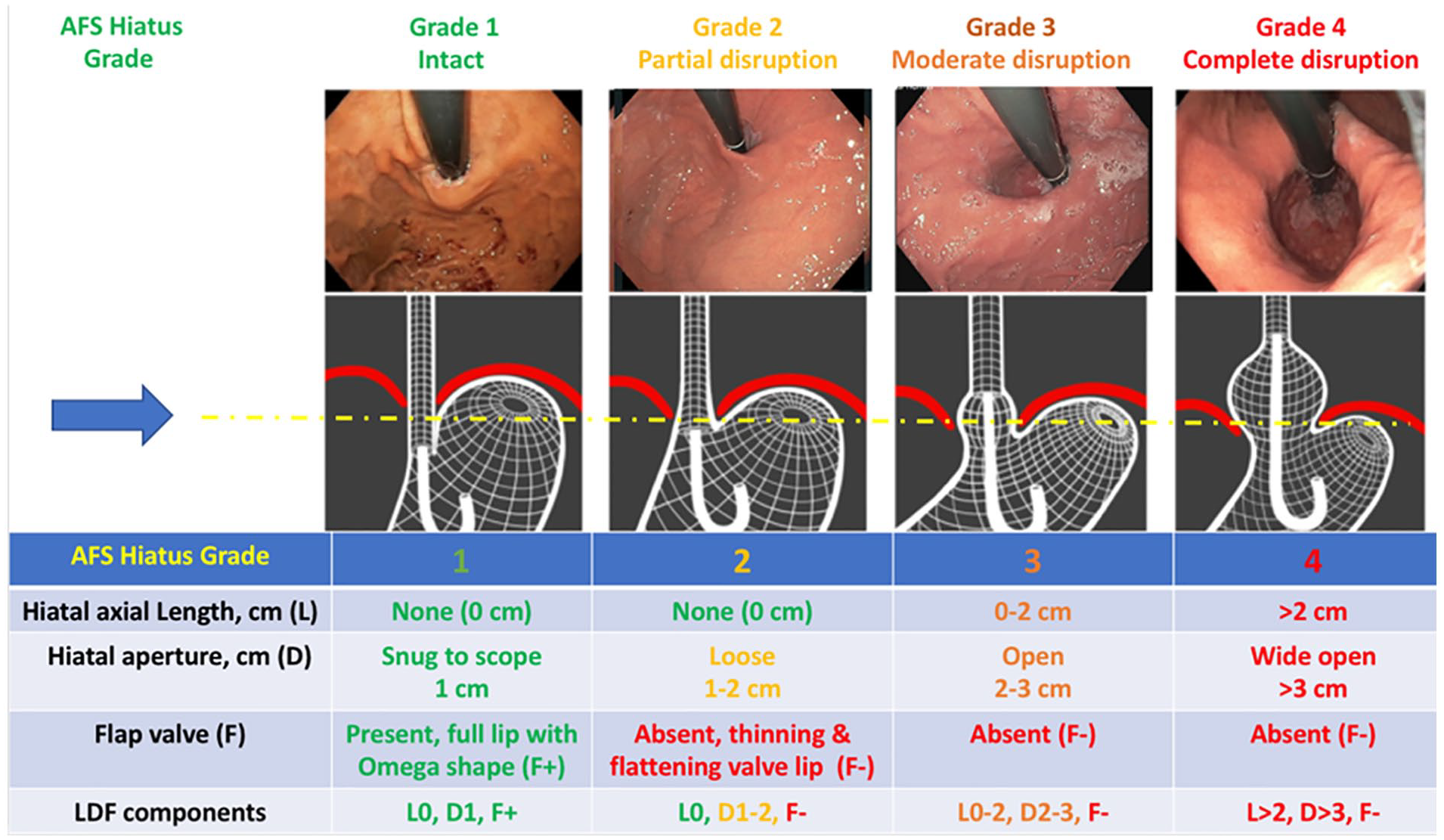
The AFS Endoscopic Classification of the Esophagogastric Junction Integrity as depicted by the LDF components (Length/Diameter/Flap valve). The arrow represents the relative level of the diaphragmatic hiatus starting with normal anatomy with a good segment of intraabdominal esophagus and an intact hiatus and progressing to increasing degree of hiatal disruption (hiatal axial length and widening of the crural defect) and loss of the flap valve.
The complete AFS endoscopic classification of EGJ integrity is summarized in Figure 5. The AFS grading system starts with an intact anatomy of the EGJ (grade 1) with a hiatal diameter of approximately 1 cm and a functioning flap valve (L0, D1, F+). There is no axial hiatal hernia length in an AFS grade 1 EGJ and the hiatus is snug against the endoscope. The Hill grade 2 is a variation of a “normal” flap valve is now encompassed within the AFS hiatus grade 1. The key aspect of AFS hiatus grade 1 is a flap valve that is judged to be normal based on the endoscopic visual characteristics of a full or thick valve lip that takes the shape of an omega configuration (approximately 270°). As depicted in the schematic diagram, an AFS grade 1 has adequate intraabdominal esophageal length with an acute angle of His that is requisite to preserve the flap valve. The AFS classification is different than that of Hill classification in that the Hill grade description is solely based on visual characteristics of the flap valve without a consideration for the hiatus anatomy. For example, in clinical practice some endoscopists document the presence of axial length of hiatal herniation but also document a Hill grade I flap valve based on endoscopic visual characteristics. In the AFS classification this scenario is not possible as the presence of any axial length of hiatal hernia immediately moves the AFS hiatus grade to at least moderate disruption (AFS hiatus grade 3).
The AFS grades 2 to 4 represent progressive degrees of EGJ disruption. Again, hiatal disruption has 2 components to include the hiatal aperture diameter (D) which represents the extent of crural separation and the extent of gastric herniation as measured by vertical axial length (L). AFS grade 2 represents partial disruption and loss of intraabdominal esophageal length; a gap or loose hiatus with 1 to 2 cm aperture diameter; and loss of the gastroesophageal flap valve characterized by thinning and flattening of the valve lip with loss of the omega shape (L0, D1-2, F-). The AFS grade 2 has no equivalent within the Hill grade classification making it one of the key differences between Hill versus AFS classification. The most distinctive difference between the AFS hiatus grade 1 versus AFS grade 2 is the loss of the flap valve as it represents the beginning of hiatal disruption and crural separation leading to the development of a gap in the hiatus (1-2 cm in diameter), progressive mediastinal migration of the intraabdominal esophagus, and widening of the acute angle of His. The next level of disruption is AFS grade 3, which represents moderate disruption with the presence of a hiatal axial length of up to 2 cm or an enlarged hiatal aperture of 2 - 3 cm along with loss of the flap valve (L0-2, D 2-3, F-). The AFS hiatus grade 3 is similar to that of Hill grade 3 but with objective measures of the degree of hiatal disruption based on the degree of crural separation and the degree of axial length of hiatal herniation. This is an important point in that using the AFS classification, upon recognition of a hiatal hernia as demonstrated by the presence of axial length, the lowest grade would be an AFS grade 3. The AFS grade 4 represents complete disruption of the EGJ with a hiatal axial length of >2 cm or wide open hiatal aperture of >3 cm, and loss of the flap valve (L > 2, D > 3, F-). With regard to the recommended parameters set forth by the expert panel for hiatal disruption, the grade is dependent on the parameters that represent the greatest level of disruption. As an example, an endoscopy demonstrating a hiatal axial length of 1.5 cm (AFS hiatus grade 3) but a hiatal aperture of 4 cm in diameter (AFS hiatus grade 4), then the final grade would be categorized as an hiatus grade 4. The final AFS hiatus grade should reflect the grade that represents the greatest degree of EGJ disruption. It is also important to not only document the hiatal aperture diameter (cm) and axial length (cm) but also to capture endoscopic images with the highest degree of endoscopic EGJ disruption as a way to communicate the information between endoscopists. Lastly, as a way to ensure uniform adoption of the AFS classification, a color scheme was used to differentiate between a normal EGJ anatomy for AFS hiatus grade 1 (green) with progression toward degree of hiatal disruption in grade 2 (yellow), grade 3 (orange), and grade 4 (red). Additionally, the color coding scheme was assigned to specific LDF components of the classification to demonstrate which of the component contributes to the extent of EGJ disruption (Figure 5). The AFS classification depicts a gradation of EGJ anatomic disruption as shown by the degree of dilation of the hiatus aperture diameter and extent of hiatal axial length. In contrast, the color scheme reinforces that once there is sufficient gap in the hiatus with development of a sliding hiatal hernia, there is loss of the intraabdominal esophagus leading to the loss of the flap valve. Therefore, the flap valve component is either intact (green) or disrupted (red) without a gradation.
Summary
The Hill grade is an endoscopic classification of the retroflexed view of the hiatus focused solely on the visual characteristics of the gastroesophageal flap valve. Although the Hill grade provides important clinical information and insight into an anatomic mechanism of GERD, its routine utilization in endoscopic practice has been limited due to skepticism as to its relevance and the perceived subjectivity in its application. With a broader understanding of the anatomic mechanisms of the antireflux barrier including the crura of the diaphragm, the LES and its sling fibers, and the flap valve and the integral relationship between them, the new AFS classification expands on the grading classification by including assessment of the hiatus aperture, objective extent of hiatal axial length and the presence or absence of the flap valve, making it much more comprehensive. The AFS endoscopic classification of the EGJ also stipulates methodology for acquiring an accurate assessment and provides a basic nomenclature for communication among endoscopists. Future directions include: 1) validation studies to determine the accuracy of this new classification in its ability to accurately predict the presence and severity of gastroesophageal reflux, and 2) extending the work to encompass grading of the hiatal appearance in patients who have undergone antireflux interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nguyen receives honoraria as a speaker for Endogastric Solutions and Olympus. Chang receives honoraria from Apollo, Boston Scientific, C2 Therapeutics, Cook Medical, Covidien, Endogastric Solutions, Erbe, Mederi, Medtronic, Mauna Kea, Olympus, Ovsco, Nine Point, Pentax, and Torax. Kahrilas receives honoraria for consulting from AstraZeneca, Ironwood, Reckitt, and Johnson & Johnson. He also shared patent on FLIP technology with John E Pandolfino and Zhiyue Lin. Muthusamy receives honoraria for consulting for Medtronic, Medivators, Interpace Diagnostics and Boston Scientific; research support for Boston Scientific; Advisory Board honoraria for Endogastric Solutions, Motus GI; Honoraria from Torax Medical; Equity position from Capsovision. Canto receives research support from Pentax Medical Corporation and Endogastric Solutions, royalties from UpToDate, advisory board honoraria from BlueStar Genomics and Castle Biosciences. Swanstrom receives honoraria from Boston Scientific, Auris, Fractyl, Human Extensions, and provides regulatory consultation for Medtronic, USGI, Boston Scientific, EndoGenix, Taurus Medical, Quelon. Dr. Abu Dayyeh is a consultant for Endogenex, Endo-TAGSS, Metamodix, and BFKW; consultant and grant/research support from USGI, Spatz Medical, Endogastric Solutions, Boston Scientific, Medtronic; grant/research support from Apollo Endosurgery, Cairn Diagnostics, Aspire Bariatrics; speaker roles with Olympus, Johnson and Johnson.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Peter J. Kahrilas is supported by P01 DK092217 (John E. Pandolfino) from the US Public Health Service.