
Abstract
Objectives
Describe patient characteristics, healthcare utilization, and Post-COVID-associated conditions among primary care patients with an ICD-10-CM diagnosis code for Post COVID-19 Condition (U09.9).
Methods
Using electronic health record (EHR) data from the American Family Cohort, a U.S. national primary care dataset, we identified patients with a U09.9 diagnosis documented October 1, 2021-June 1, 2023. Patient data were categorized into three periods: pre-pandemic (2016-2019), pandemic pre-index (2020 to the first U09.9 diagnosis, or ‘index’ date), and post-index (index date to the last observation). Post-COVID-associated conditions were aggregated a priori into 12 body systems.
Results
We identified 10,265 patients with a U09.9 diagnosis code; 81.9% were ≥40 years, 63.3% female, 74.4% White, and 70.5% resided in metropolitan counties. Patients averaged 12.7 primary care encounters in the year before the index U09.9 diagnosis, compared to 9.2 encounters annually in the post-index period. Over 68% of patients who had ≥1 pre-pandemic encounters had ≥1 underlying medical conditions. The prevalence of conditions across 9 out of 12 body systems increased from the pre-pandemic to the pandemic pre-index period for patients who had ≥1 conditions. Prevalence of respiratory and musculoskeletal conditions had the largest decrease from the pandemic pre-index to the post-index period.
Conclusions
Compared to adults who self-report Long COVID in nationally representative population-based surveys, patient characteristics in this cohort highlight a potential diagnosis gap - particularly for patients with rural residence or high county-level socioeconomic deprivation. Given frequent healthcare utilization and clinical complexity, primary care may require additional resources to meet patient needs.
3-question summary box
What is the current understanding of this subject?
Characteristics of patients with a diagnosis code for Post-COVID Conditions (PCC, U09.9) in primary care settings are unknown.
What does this report add to the literature?
Using a U.S. national primary care electronic health record dataset (American Family Cohort), this report details sociodemographic characteristics of patients with a U09.9 code and examines primary care utilization and the prevalence of documented PCC-associated conditions across 3 time periods.
What are the implications for public health practice?
This study identifies a potential diagnosis gap-i.e., lower likelihood of receiving a PCC diagnosis code-among patients with rural residence or high socioeconomic deprivation compared to sociodemographic patterns in national population-based surveys. High utilization and clinical complexity of patients with PCC may require additional resources to support primary care.
Introduction
Long COVID is characterized by new, returning, or ongoing health problems lasting three months or longer after SARS-CoV-2 infection 1 and may affect multiple body systems. 2 On October 1, 2021, the Centers for Disease Control and Prevention (CDC) approved the release of the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) diagnosis code U09.9, Post-COVID Condition (PCC). 3
Understanding of the use of U09.9 in clinical practice is limited. One study found that concordance between PCC diagnosis and recorded clinical criteria varied across health care systems and by clinical case definition. 4 Inconsistent use of the U09.9 code may be reflective of the challenges in diagnosing PCC. For example, the duration and nature of symptoms, which can be persistent or relapsing and remitting, or progressive, affecting one or more organ systems, adds complexity to the diagnosis process. 1 Currently, no diagnostic test can definitively confirm symptoms or conditions are related to SARS-CoV-2 infection. 5 Patient-level factors (e.g., frequency of primary-care visits and symptom-specific care-seeking) and provider-level factors (e.g., familiarity with PCC case definitions and the U09.9 code) may influence both the likelihood that a PCC diagnosis code is entered in the EHR and the timing of that documentation, independent of the patient’s underlying illness.
Many EHR studies focus on cohorts of individuals with documented, medically attended acute COVID-19 illness who are tracked over time for post-acute sequelae. Our approach instead centers on patients who received a PCC diagnosis code in primary care - irrespective of care seeking for their acute COVID-19 illness. These populations only partially overlap because selection into this study is not conditional on seeking care for acute COVID-19 or receiving a documented COVID-19 diagnosis. Because primary care practices often manage patients with PCC, electronic health record (EHR) data may elucidate how PCC is documented by frontline primary care practices, the clinical profile and sociodemographic characteristics of these patients, and their patterns of healthcare use in primary care settings.6–9
The current study has the following research aims: (1) to describe the sociodemographic characteristics of primary care patients who received a U09.9 diagnosis code; (2) to characterize primary care utilization patterns among these patients; and (3) to quantify changes in the prevalence of PCC-associated conditions relative to the pandemic’s onset and the first U09.9 diagnosis code.
Methods
Study design
The EHR data for this study come from the American Family Cohort, a research dataset derived from the Qualified Clinical Data Registry: PRIME. The American Family Cohort or AFC was launched in 2016 and contains EHR data for more than 7 million patients of all ages from 1,320 primary care clinical practices between 2016-2023. AFC clinical practices are spread across 47 U.S. states and Washington D.C., with patients residing in all 50 states.10–12 We created a cohort of all primary care patients who had a diagnosis code of U09.9 documented between October 1, 2021, and June 1, 2023 (henceforth referred to as the PCC cohort, n = 10,265).
Sociodemographic characteristics
Sociodemographic characteristics of primary care patients with a U09.9 diagnosis code (n = 10,265): American family cohort, October 1, 2021, to June 1, 2023.
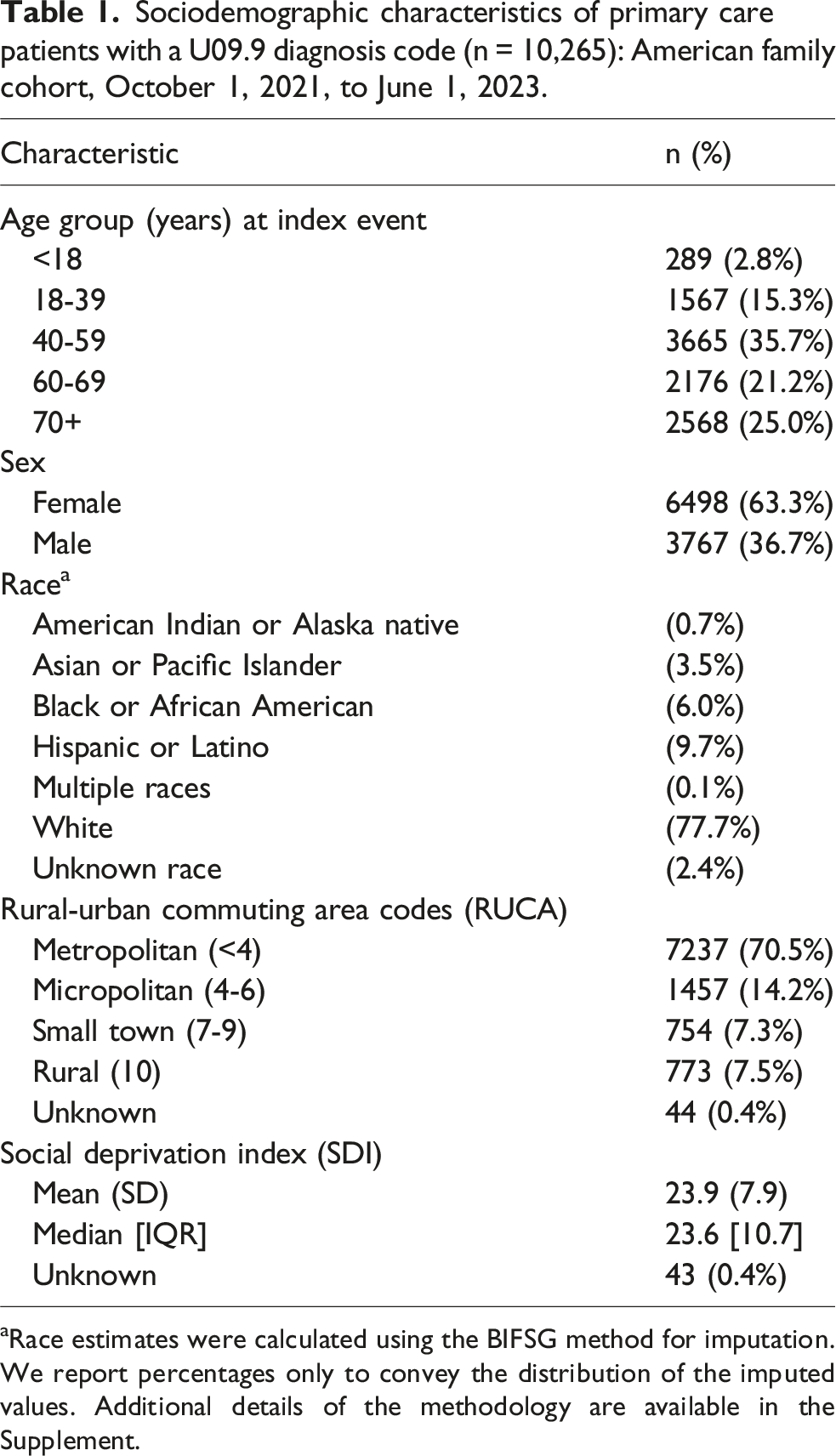
aRace estimates were calculated using the BIFSG method for imputation. We report percentages only to convey the distribution of the imputed values. Additional details of the methodology are available in the Supplement.
Observation time
The index date was the earliest date of a documented U09.9 diagnosis code. The observation period was standardized to control the pre-pandemic observation time. Using healthcare encounters (including visits and documented conditions), total observation time was calculated from January 1, 2016, or the patient’s first primary care encounter (whichever occurred first) to their most recent primary care encounter through June 28, 2023 - allowing for four or more weeks of possible post-index observation time). We delineated three distinct periods: pre-pandemic (2016-2019), pandemic pre-index (January 1, 2020, to the index date), and post-index (the day after the index date to the last observation day).
Healthcare utilization
To examine the secular trends in primary care utilization, we measured the number of primary care encounters compared to the length of observation days for each patient for each period.
PCC-associated conditions
There are more than 200 documented symptoms and conditions associated with PCC. 22 Using symptoms and conditions documented in previous publications,23–26 CDC curated a list of PCC-associated conditions, including 2,051 ICD-10-CM diagnosis codes, used for PCC surveillance (Supplemental Table 1). 27 This approach aligns with findings from extant literature that identify possible sequelae of SARS-CoV-2 infection, such as diabetes.28–30 PCC-associated conditions were categorized into 12 body systems: cardiovascular, dermatologic, endocrine, gastrointestinal, hematologic, musculoskeletal, neuropsychiatric, renal, liver diseases, respiratory, sensory, and systemic. Conditions documented prior to the index date were considered pre-existing medical conditions. Those documented on or after the index date were considered PCC-associated conditions.
Statistical analysis
To describe the primary care patients with a U09.9 diagnosis code, we characterized the analytic population based on key sociodemographic and health characteristics. To characterize primary care use patterns and explore variability in follow-up time and healthcare use, we created a scatter plot of primary care encounters by observation days and encounter counts - depicting average primary care use trend across the three observation periods (pre-pandemic, 12 months pre-index, and post-index) and modeled trends in primary care use across observation periods using negative binomial regression.
To examine prevalence of PCC-associated conditions, we calculated the prevalence of having one or more diagnoses within each body system among all patients in the pre-pandemic, pandemic pre-index, and post-index periods. Not all patients were observed during all three periods; thus, the denominators for each period vary. Data in the liver disease body system did not meet AFC data reporting guidelines and were suppressed.
To examine changes in prevalence of PCC-associated conditions, we created a restricted cohort of primary care patients with both a U09.9 diagnosis code and at least one primary care encounter during the pre-pandemic period. We calculated the prevalence of PCC-associated conditions by body system during the pre-pandemic and pandemic pre-index periods. To assess changes across these periods, we then calculated prevalence ratios (PR) and 95% Confidence Intervals (CI) assuming normal distribution of the log-transformed ratios and prevalence differences (95% CI) calculated based on binomially distributed prevalences.
We examined the prevalence of recurrent and new diagnoses relative to the pandemic’s onset and the first U09.9 diagnosis code in the restricted cohort. “Recurrent diagnosis” refers to any condition documented during the pre-pandemic period that was documented again during the pandemic pre-index period and “new diagnosis” refers to any condition not documented during the pre-pandemic period and first documented during the pandemic pre-index period. Prevalence estimates were based on the documented diagnosis for each period. For example, a chronic condition documented in the pre-pandemic period did not contribute to the numerator in the pandemic pre-index period unless the diagnosis was documented again during this subsequent period.
All statistical analyses were performed using R software (version 4.4.1) within the Redivis data platform. This activity was reviewed by CDC, deemed not human subjects research, and was conducted consistent with applicable federal law and CDC policy (45 C.F.R. part 46.102(l)(2), 21 C.F.R. part 56; 42 U.S.C. Sect. 241(d); 5 U.S.C. Sect. 552a; 44 U.S.C. Sect. 3501 et seq.). This study was also reviewed and approved by the Stanford University Institutional Review Board (Protocol ID: 61956).
Results
Sociodemographic characteristics
The number of primary care patients per week with an index event ranged from 13 to 372, with one peak in January 2022 (372 cases per week) and another in August 2022 (214 cases per week) (Supplemental Figure 1). Most patients were aged 40 years or older at first U09.9 diagnosis code (81.9%; median age at diagnosis=58.0 years, IQR = 25.0 years), female (63.3%), and White (77.7%) (Table 1). Nearly 30% resided outside of metropolitan areas. On average, primary care patients with a U09.9 diagnosis code resided in counties characterized by lower socioeconomic deprivation compared to the national average (Social Deprivation Index,
Primary care utilization
During the pre-pandemic period (2016-2019), 7,586 patients (73.9%) had at least one primary care encounter; of these, more than 80% (n = 6,150) of patients had at least two years of pre-pandemic observation (Figure 1). Patients with at least one primary care encounter during the pre-pandemic period averaged nine primary care encounters per year during 2016-2019; over the full 2016–2019 pre-pandemic period, this corresponded to a mean of 36.2 encounters (SD 48), median 21 (IQR 38). For the 12 months preceding the index date, 12.8% (n = 1,319) of patients had at least one primary care encounter, with an annualized mean of 12.7 primary care encounters (SD=11.8; median = 9; IQR=9). During the post-index period, 88.4% (n = 9,077) of patients had at least one primary care encounter, with an annualized mean of 9.2 primary care encounters during the post-index period (SD=10.1; median = 6; IQR=8). Primary healthcare utilization by length of observation days and encounter counts modeled using negative binomial regression among primary care patients with a U09.9 diagnosis, American family cohort, January 1, 2016 - June 28, 2023*. *The panels depict healthcare utilization average trends across different observation periods relative to the patients’ index dates (pre-pandemic, 12 months pre-index, and post-index). The x-axis represents the total observation days per person during each period, and the y-axis represents the total encounter counts. The smooth lines illustrate the modeled trends using negative binomial regression, stratified by the index year (indicated by color).
The length of patient observation varied across the three study periods (Supplemental Table 2). During the pre-pandemic period (2016-2019), longer observation time was significantly associated with higher encounter count (estimate = 0.002, p < 0.001), indicating that patients observed over longer durations had greater utilization of primary care. This pattern was also observed during the 12-month pre-index period (estimate = 0.002, p < 0.001) and after a PCC diagnosis (post-index period) (estimate = 0.004, p < 0.001). However, there was some variation across time periods by year of initial U09.9 diagnosis. Compared to patients diagnosed with PCC in 2021, encounter counts during the 12-month pre-index period decreased for patients diagnosed with PCC in 2022 (estimate = −0.210, p < 0.001) and 2023 (estimate = −0.680, p < 0.001). However, the finding was reversed for the post-index period such that patients who received their first U09.9 diagnosis code in 2022 or 2023 had significantly higher encounter rates compared to those diagnosed in 2021 (estimates = 0.191 for 2022, 0.201 for 2023; both p < 0.001), reflecting greater post-diagnosis healthcare utilization in later years.
PCC-associated conditions
Prevalence by body system
Among the PCC cohort, 9,373 (91.3%) had one or more pre-existing conditions or PCC-associated conditions documented during the study. The denominators for the prevalences differed by study period (pre-pandemic, n = 7,273; pandemic pre-index, n = 10,265; post-index, n = 8,867). There were increases in the prevalence of documented pre-existing conditions from the pre-pandemic to pandemic pre-index period for all body systems except for musculoskeletal and gastrointestinal. The largest absolute increases (percentage points, pp) were observed for respiratory (+14.0 pp; 95% CI 12.6, 15.5), systemic (+6.8 pp; 95% CI 5.5, 8.1), neuropsychiatric (+2.7 pp; 95% CI 1.2, 4.2), and renal (+2.2 pp; 95% CI 1.5, 3.0) conditions (Figure 2 and Supplemental Table 3). In contrast, musculoskeletal (−6.3 pp; 95% CI −7.8, −4.8) and gastrointestinal (−1.3 pp; 95% CI −2.6, 0.0) decreased over the same interval. The prevalence of diagnoses for all documented conditions during post-index period was lower than the pandemic pre-index period, and, for most body systems, the post-index period was lower than the pre-pandemic prevalence. Prevalences of documented respiratory and musculoskeletal conditions had the largest decreases, by -20.0 pp (95% CI −21.4, −18.6) and -14.4 pp (95% CI −15.7, −13.1) respectively, from the pandemic pre-index to the post-index periods. Prevalences of documented endocrine and dermatologic conditions had the smallest decreases, less than 1 pp each. Prevalence of documented conditions category by body system among patients with U09.9 in different time periods, American family cohort, January 1, 2016 - June 28, 2023*. *Denominators for prevalence vary across different time periods: n = 7,273 for 2016-2019; n = 10,265 for January 1, 2020, to the index date; and n = 8,867 after the index date.
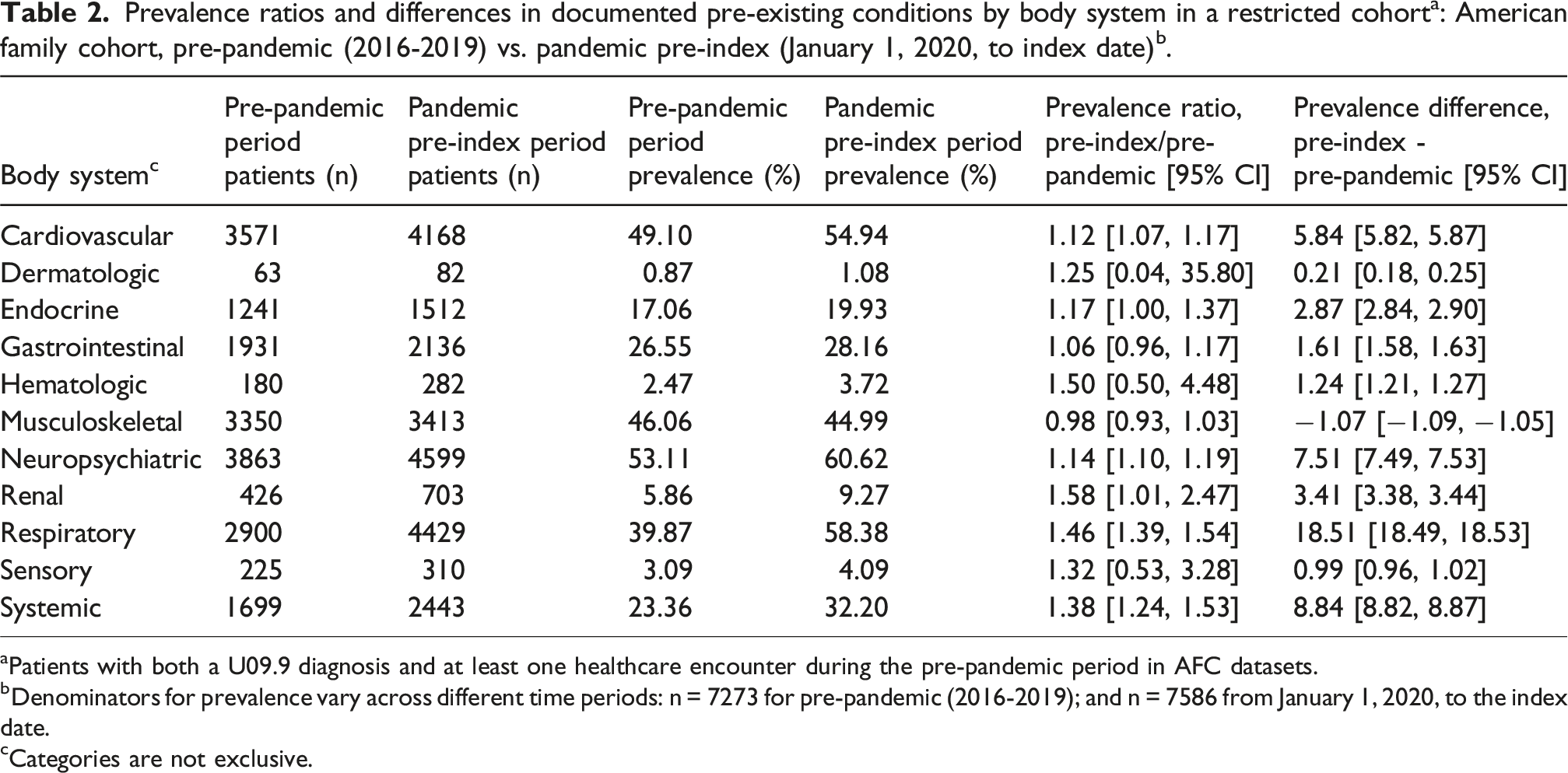
aPatients with both a U09.9 diagnosis and at least one healthcare encounter during the pre-pandemic period in AFC datasets.
bDenominators for prevalence vary across different time periods: n = 7273 for pre-pandemic (2016-2019); and n = 7586 from January 1, 2020, to the index date.
cCategories are not exclusive.
Recurrent vs new diagnoses in the restricted cohort
For the restricted cohort, the comparison of recurrent and new diagnoses between the pre-pandemic period and the pandemic pre-index period is presented in Figure 3. More than 50% of the diagnoses in the following body systems were recurrent: neuropsychiatric (66.3%, ± 1.4%), cardiovascular (72.9%, ± 1.3%), musculoskeletal (59.7%, ± 1.6%), gastrointestinal (54.6%, ± 2.1%), and endocrine (74.3%, ± 2.2%). In contrast, more than 50% of the diagnoses in the following body systems were new: respiratory (51.8%, ± 1.5%), systemic (63.3%, ± 1.9%), renal (56.2%, ± 3.7%), sensory (82.9%, ± 4.2%), hematologic (68.1%, ± 5.4%), and dermatologic (82.9%, ± 8.1%). Distribution of recurrent vs. new diagnoses by body system during the pandemic pre-index period (Jan 1, 2020-index date) vs. the pre-pandemic period (2016-2019) among patients with a U09.9 code in the restricted cohort (n = 7,586)*, American family cohort. *Patients with both a U09.9 diagnosis and ≥1 pre-pandemic primary care encounter in AFC datasets. Body-system categories are not mutually exclusive; a patient can contribute to multiple categories. “Recurrent” indicates a condition documented in 2016-2019 and again in the pandemic pre-index period; “New” indicates first documentation in the pandemic pre-index period.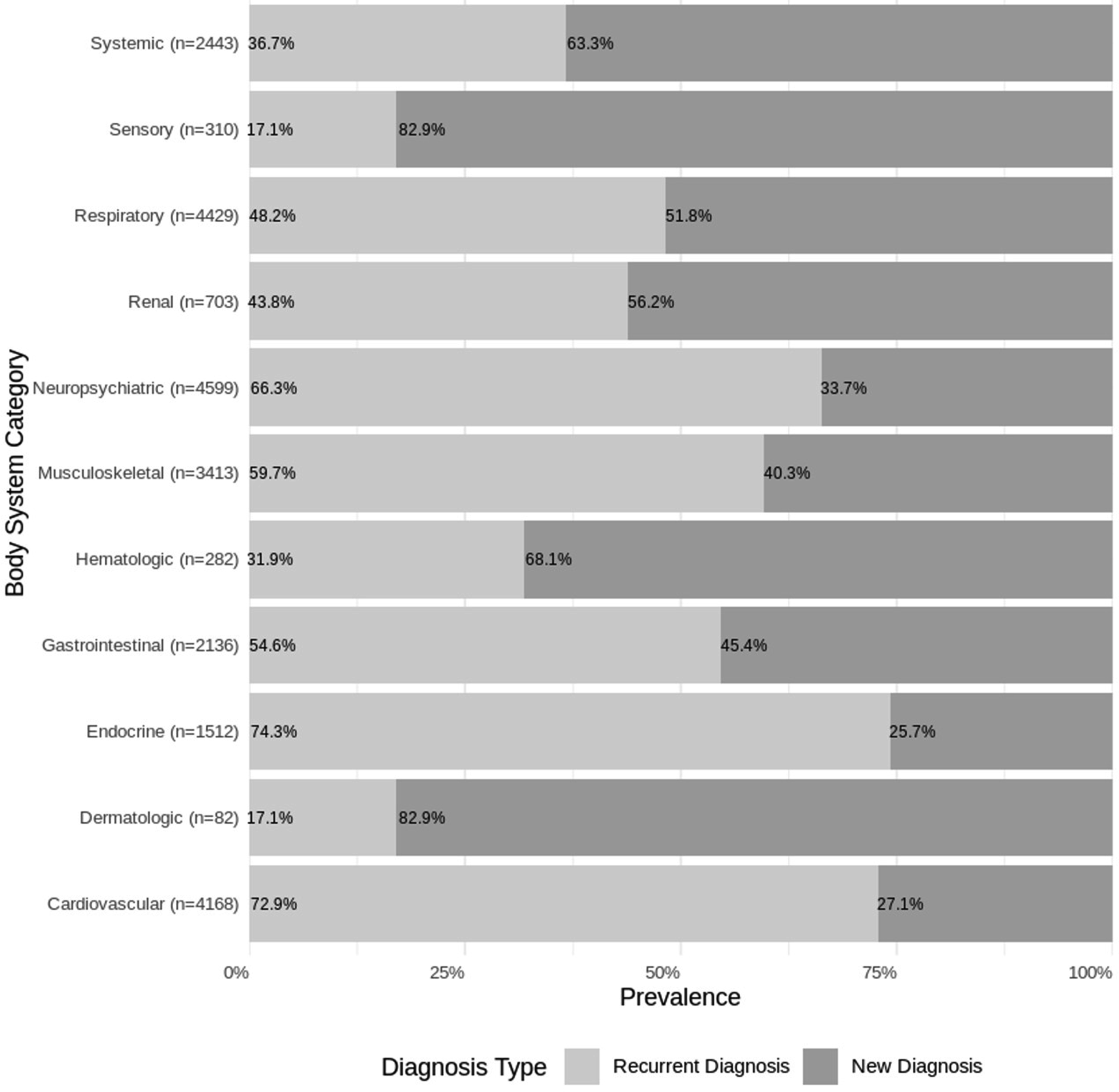
Discussion
This study of primary care patients with a U09.9 diagnosis code found that PCC was documented most frequently among patients who were female, White, non-Hispanic, residing in metropolitan areas and in counties with lower socioeconomic deprivation. Some demographic characteristics of this PCC cohort align with findings from a nationally representative population-based survey - the National Health Interview Survey (NHIS) - wherein self-reported Long COVID predominantly affected adults who were female, aged 35-49 years, non-Hispanic, and White. 31 While PCC likely affects demographic groups differently depending on factors including vaccination rates, underlying conditions, and age, our primary care data indicated a higher prevalence of PCC among individuals residing in metropolitan areas and counties characterized by lower socioeconomic deprivation. This finding contrasts those from NHIS which found higher prevalence of self-reported Long COVID among those residing in non-metropolitan counties compared to those residing in metropolitan counties. 32 Our study captured PCC identified in a clinical setting whereas the NHIS captured self-reported symptoms consistent with Long COVID, irrespective of clinical diagnosis; these findings highlight a potential gap between those experiencing and those getting Long COVID documented in their primary care medical record.
The demographic profile of patients in our study may partially reflect differences in healthcare access and utilization, with metropolitan and less socially vulnerable populations more likely to receive timely and documented diagnoses. Prior work shows that patients in rural or socially vulnerable areas face significant barriers to access healthcare, potentially leading to delayed, missed, or undocumented diagnoses. 33 Taken together, these patterns are consistent with the inverse care law 34 - populations with greater need for care (e.g., rural or socially vulnerable groups) often have less access and lower capture in diagnosis-based data. In our setting, higher documentation of PCC in metropolitan or less deprived areas alongside known access barriers in rural or more deprived areas suggests that true PCC burden may be higher in under-resourced communities than documented in EHR. One study found that non-clinical factors possibly influence the likelihood of a documented PCC diagnosis. 35 The demographic profile of the primary care U09.9 cohort suggests that access to healthcare, continuity at a clinical practice, and socioeconomic status may influence who receives a diagnosis code for PCC.
For patients with documented PCC, our findings highlight the shifting primary care utilization during 2016-2023. In 2020, healthcare utilization in general decreased due to fears of contracting COVID-19, healthcare system overloads, and stay-at-home orders.36,37 Changes in health insurance coverage during the early part of the pandemic may have also influenced access to care. 38 Evidence from a 2021 systematic review of data from 20 countries found a 42% reduction in healthcare visits from February-May 2020 compared to pre-pandemic. 36 Among patients with a PCC diagnosis code, however, healthcare engagement had distinct features. In a primary care cohort in England, patients diagnosed with Long COVID had high pre-pandemic healthcare utilization, averaging 30 visits per year (vs. 16 in patients without Long COVID), and healthcare utilization increased by 49% from pre-pandemic levels, indicating that utilization was highest following diagnosis. 39 We observed high-levels of healthcare utilization across all three study periods; however, the annualized mean encounters during the pandemic pre-index period was greater than the pre-pandemic and post-index periods. These findings suggest that patients may have had an increase in healthcare use because of symptoms prior to receiving a PCC diagnosis code, and that those with greater continuity of care may be more likely to receive a diagnosis code for PCC.
Patients with a PCC diagnosis code had high prevalence of both pre-existing medical conditions and PCC-associated conditions. We found that many of the prevalent pre-existing medical conditions continued to be documented in the post-index period, notably neuropsychiatric, cardiovascular, musculoskeletal, and other conditions. During the pandemic pre-index period, we observed an increase in the prevalence of certain medical conditions, including respiratory, systemic, renal, and neuropsychiatric conditions, compared to the pre-pandemic period. While we were unable to attribute specific factors to our findings, some possibilities include direct causes from SARS-CoV-2 infection, societal conditions of the pandemic more broadly, or secular changes in disease prevalence.
Our findings also indicate a general decrease in the documentation of new medical conditions following use of the U09.9 code, which is expected based on guidance that it be used in conjunction with specific codes for symptoms or conditions. 3 It is also possible that documentation practices shifted (e.g., problem lists consolidated, or symptoms attributed to existing diagnoses), which could contribute to under-documentation of ‘new’ conditions in EHRs.40,41 In tandem, early respiratory and musculoskeletal manifestations may improve or be recoded under established chronic diagnoses (e.g., asthma/COPD, chronic pain/arthritis), yielding the largest apparent post-index declines for these systems (−20.0 and −14.4 pp, respectively; Figure 2; Supplemental Table 3). Given the prevalence of both pre-existing and PCC-associated conditions, our findings highlight the complex clinical profile of patients with a PCC diagnosis. This information can be helpful for healthcare planning so that primary care is equipped to address the evolving needs of these patients. 35 Taken together, these patterns suggest that our absolute period-to-period prevalence estimates are conservative, while the observed directional changes (e.g., larger post-index declines in respiratory and musculoskeletal systems) may reflect a combination of symptom resolution and documentation shifts rather than coding artifacts alone.
The main strength of this study is that it uses longitudinal primary care practice data from across the U.S., including pre-pandemic encounters. Several limitations should be considered when interpreting our findings. This study is limited to patients who both accessed primary care and received a U09.9 code, so these findings are not generalizable to patients with U09.9 documented in other settings (e.g., specialists, emergency care) or those experiencing PCC more broadly. Heterogeneous adoption of U09.9 and organ-system coding may produce under-ascertainment of PCC in EHR. Additionally, a substantial share of U.S. adults does not attend primary care annually, 42 meaning individuals with PCC who do not engage with primary care were less likely to be captured, further biasing prevalence downward. Non-clinical factors - including continuity and access to primary care, clinician recognition of PCC, variation in coding workflows, insurance status, and geographic barriers - may influence the likelihood PCC diagnosis and lead to under-identification or misclassification of patients. 35 Because PCC encompasses both new and worsening manifestations of pre-existing conditions, our reliance on ICD-10-CM diagnosis codes allowed us to identify new diagnoses but not to systematically assess worsening of previously documented conditions, limiting our ability to describe the full clinical spectrum of PCC. Future work may examine the magnitude of a potential diagnostic gap. Given the observational nature of the data and the study design, the variability in observation periods and healthcare access across different regions may also influence the results, such as, differences in follow-up time (e.g., shorter post-index windows for patients receiving a U09.9 code in 2023) and regional access patterns (e.g., fewer visits during pandemic surges or in underserved areas) could lower detection of new conditions post-index and shift observed prevalence between periods. Despite these limitations, our study provides a valuable perspective on patients with a diagnosis code for PCC documented in primary care settings, which may help inform healthcare planning at the primary care-level for patients with PCC.
Conclusions
Differences in some sociodemographic characteristics between primary care patients with a U09.9 diagnosis code and those who self-report PCC in nationally representative population-based surveys, which capture self-reported symptoms consistent with Long COVID irrespective of clinical diagnosis, highlight a potential diagnosis gap - particularly for patients residing in rural areas and those with higher socioeconomic deprivation. Given the prevalence of pre-existing conditions and PCC-associated conditions combined with high healthcare use, patients with a U09.9 diagnosis code in this cohort were clinically complex. Future work focusing on primary care practices and identifying any needed support may help meet patient needs for PCC management.
Supplemental material
Supplemental Material - Post-COVID-19 conditions identified by ICD-10-CM code in a cohort of U.S. primary care patients, 2021 – 2023
Supplemental Material for Post-COVID-19 conditions identified by ICD-10-CM code in a cohort of U.S. primary care patients, 2021 – 2023 by Xiaoyu Wang, Esther Velásquez, Sharon Saydah, Emilia H. Koumans, Ilia Rochlin, Sebastian Romano, David H. Rehkopf, Nicole D. Ford in Journal of Multimorbidity and Comorbidity.
Supplemental material
Supplemental Material - Post-COVID-19 conditions identified by ICD-10-CM code in a cohort of U.S. primary care patients, 2021 – 2023
Supplemental Material for Post-COVID-19 conditions identified by ICD-10-CM code in a cohort of U.S. primary care patients, 2021 – 2023 by Xiaoyu Wang, Esther Velásquez, Sharon Saydah, Emilia H. Koumans, Ilia Rochlin, Sebastian Romano, David H. Rehkopf, Nicole D. Ford in Journal of Multimorbidity and Comorbidity.
Footnotes
Ethical considerations
This study was reviewed and approved by the Stanford University Research Compliance Office (Protocol Approval #61956).
Consent to participate
This IRB protocol approved by the Stanford University Research Compliance Office was granted Waiver of Consent because the research was conducted on retrospective administrative data, and there were approved study protocol procedures in place to protect confidentiality and privacy.
Consent for publication
All authors consent to publication of this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by funding from the Centers for Disease Control and Prevention, (75D30122P12974). This activity was reviewed by CDC, deemed not research, and was conducted consistent with applicable federal law and CDC policy (45 C.F.R. part 46.102(l)(2), 21 C.F.R. part 56; 42 U.S.C. Sect. 241(d); 5 U.S.C. Sect. 552a; 44 U.S.C. Sect. 3501 et seq.).
Declaration of conflicting interests
No authors have any disclosures to report.
Data Availability Statement
Complete data are available from the American Family Cohort for approved research projects. See up-to-date access requirements at https://www.AmericanFamilyCohort.org. The current analysis used AFC OMOP RIF version 5.0 (![]() ). Users of the data do not have access to patients or practices that contribute data to the registry and are prohibited from making contact; neither patients nor the public were involved in the current study.
). Users of the data do not have access to patients or practices that contribute data to the registry and are prohibited from making contact; neither patients nor the public were involved in the current study.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention (CDC).
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.