
Abstract
Background:
The increasing prevalence of patients with multimorbidity in the general population affects the health-care system. There is a lack of knowledge of the proportion of patients attending multiple hospital outpatient specialty clinics simultaneously.
Objective:
This study describes the development in the proportion of patients managed simultaneously in multiple hospital outpatient specialty clinics.
Design:
We obtained three cross-sectional samples from all of the hospitals in Denmark. The data set consists of adults (age 18+) in long-term outpatient care on January 1 in 2004, 2009, and 2014 with one or more of 50 consensus-selected chronic diseases. Descriptive statistics were used to examine and compare the proportion of patients treated simultaneously in multiple outpatient specialty clinics. We also investigated the most common combinations of outpatient specialty clinics.
Results:
In 2004, 176,786 patients with chronic diseases were registered as receiving outpatient care in Denmark. This figure increased to 246,542 patients in 2009 and 341,015 in 2014. The proportion of patients managed simultaneously in multiple outpatient specialty clinics was 4.0% in 2004, 5.5% in 2009, and 7.7% in 2014. The most common specialty clinic combination was endocrinology and cardiology, accounting for 12.1% in 2004, 11.5% in 2009, and 9.6% in 2014.
Conclusions:
The proportion of patients in multiple clinics nearly doubled over a 10-year period. While there were some common specialty clinic combinations in which patients were treated most often, there was also considerable variation. Further studies are needed to identify generic and disease-specific initiatives.
Background
As the prevalence of patients with multimorbidity (MM) increases in the population, the secondary health sector can expect an increase in the management of these patients. However, knowledge about how this MM patient population is managed in the hospital outpatient clinics is sparse.
MM is commonly defined as the presence of two or more chronic medical diseases in an individual. 1,2 A Danish population study has reported that around 50% of the adult population has one chronic disease and approximately half of these patients live with MM. 3 MM increases with age, as shown in a Scottish national primary care survey in which 11% of people aged 25–44 years, 65% of those over age 65, and 82% over age 85 suffered from MM. 4 The prevalence of MM increases with time, as shown in studies from the Netherlands, where it rose by 3.2% over a 10-year period (from 14.3% in 2001 to 17.5% in 2011) 5 and is expected to increase further in the future as a result of aging populations together with health-care advances. 5 –7
The increasing prevalence of MM patients in the population affects all health-care sectors. While studies on the prevalence and patterns among MM patients have been conducted in the primary health-care sector in different countries, 1 no studies have been performed at hospital-level outpatient clinics.
In contrast to the primary health-care level, the hospital sector is built on single-disease management, 8 and care for each disease is provided from disease-specialized outpatient clinics. MM patients must therefore often go to multiple clinics. To optimize clinical organization and patient trajectories, it is important to know the extent of this development among patients simultaneously managed in different outpatient specialty clinics and which combinations of specialty clinics are most common.
On that background, this study describes the population of patients managed simultaneously in multiple outpatient specialty clinics among patients in long-term outpatient treatment for chronic diseases. More specifically, we address the following two research questions: Firstly, what was the development in the proportion of patients managed simultaneously in multiple outpatient specialty clinics among outpatients between 2004, 2009, and 2014? And secondly, what were the most common specialty clinic combinations?
Material and methods
This study was designed as a historic, register-based, cross-sectional study of a national data set from Danish hospitals, extracting data for 2004, 2009, and 2014.
The Danish health-care system
The Danish Health Authority provides access to tax-financed health care for all 5.8 million persons residing in Denmark. 9 General practitioners (GPs) provide most of the care for patients with chronic diseases. 10,11 If the chronic disease reaches a certain level of severity or complexity, however, patients are referred to specialists in hospital outpatient specialty clinics. In the hospital outpatient clinics, patients are enrolled in a course of treatment within a specific disease-group clinic for each disease for which they are referred to hospital treatment. A course of treatment consists of all the contacts in connection with diagnosing or diagnosing and treatment aspects in a hospital outpatient clinic. The duration of a treatment course is from the patient’s first contact to the clinic until the last contact, which is when treatment courses are completed or of other reasons terminated.
Data sources
All Danish hospitals, both public and privately owned, automatically report all inpatient and outpatient contacts to The National Patient Register (NPR). The NPR possesses longitudinal data derived from patient medical records on inpatient contacts in Danish hospitals since 1977 and outpatient contacts since 1995, as well as discharge diagnosis codes according to the International Classification of Diseases, Revision 8 (ICD8) for 1977–1993 and the International Classification of Diseases, Revision 10 (ICD10) from 1994 onward. Since 2000, it has also served as the basis for payment via the Diagnostic Related Group system. 12,13 The NPR was used to extract the study population and to obtain information on the patients’ age, sex, and diagnoses.
Study population
We included patients aged 18 and older who were in an ongoing course of treatment in hospital outpatient specialty clinics for one or multiple chronic diseases on January 1, 2004; January 1, 2009; or January 1, 2014. There is no standard approach for defining which diseases should be included in MM patient studies. 2,14,15 The included morbidities in such studies are therefore inevitably partly subjective and dependent on the available data. As others, we included diseases with a high prevalence in our setting. 14
Information on diseases based on activity (outpatient visits) in hospital outpatient settings is available from The Danish National Board of Health statistics. 16 We extracted information from 2014 from all Danish hospitals (not including psychiatric hospitals), all age groups, and based on four-character ICD-codes (e.g. DJ44).
Four specialists (two in internal medicine, one in family medicine, and one in public health) reviewed all of the diagnoses and extracted 50 chronic, frequent, and clinically relevant diagnoses. Disagreement was resolved by discussion and consensus. The 50 most frequent diagnoses constituted 31% of the outpatient group and 33% of the outpatient activity based on 2014 data.
We included patients with 1 of the 50 selected chronic diseases if they had been enrolled in a course of hospital outpatient treatment for at least 6 months from the inclusion date in 2004, 2009, or 2014. The 6-month criterion was chosen to avoid acute or subacute forms of certain diseases and transitory hospital-outpatient treated diseases. Six months duration is the definition for chronic disease used by the Danish Health Authority. 17 We then categorized these 50 diagnoses into 16 organizational groups according to how Danish hospitals generally group the different specialist clinics based on information from four typical Danish hospital organizations and Danish Health Statistics. 18 For instance, diabetes and thyrotoxicosis are both treated in an outpatient specialty clinic for endocrine diseases. Diagnoses and categorization are shown in Appendix 1.
Statistics
Patients in 2004, 2009, and 2014 were described in absolute numbers and percentages using 2004 as reference. The χ 2 test was used to investigate significant differences in sex, age groups, and number of specialty clinics between 2014, 2009, and 2004.
To determine the most prevalent combination patterns of hospital outpatient specialy clinics, we calculated all of the possible combinations of specialty clinics and their frequencies when patients were in multiple clinics, presented as absolute numbers and percentages. The five most common specialty clinic combinations were ranged for patients treated in two clinics. Two-sided statistical tests were used, and p < 0.05 was considered statistically significant. All data analyses were performed using Stata software, version 15.0 (StataCorp LP, College Station, Texas, USA).
Ethics
The study did not involve any direct contact with patients or access to patient files, for which reason neither informed consent nor ethical approval were required. 19 The study was registered with the Danish Data Protection Agency (J.nr. 18/35695). We applied STROBE criteria to ensure adequate reporting and transparency. 20
Results
In 2004, 176,786 patients (3.3% of the Danish population) with one or more of the 50 selected diseases were managed in a hospital outpatient setting, 246,542 patients (4.5%) in 2009, and 341,015 patients (6.1%) in 2014 (Table 1). There was an increase for almost all diagnoses. In 2014, four diagnoses (type 2 diabetes, breast cancer, type 1 diabetes, and sleeping disorders) covered 25% of the diagnoses. The changes from 2004 to 2009 and 2014 within each diagnosis group are presented in Appendix 2.
Study population and Danish population in 2004, 2009, and 2014.

a2004 was used as the reference from which the percentage in 2009 and 2014 was calculated.
The patient characteristics for all three populations are described in Table 2. In 2004, the median age was 57 years (interquartile range (IQR) 44–69) and 34% of the patients were 65 years or older; in 2009, the median was 60 years (IQR 47–70), 38% of patients were 65+; in 2014, the median was 62 years (IQR 48–72; p < 0.001, reference 2004), 44% of patients were 65+. The proportion of patients treated in multiple outpatient specialty clinics was 4.0% in 2004, 5.5% in 2009, and 7.7% in 2014. The patients treated in one hospital specialty clinic nearly doubled over 10 years (169,678 patients in 2004 vs. 314,762 patients in 2014), while the number of patients treated in two or more specialty clinics increased nearly fourfold (7108 patients in 2004 vs. 26,253 patients in 2014).
Number of patients distributed by sex, age groups, and number of outpatient specialty clinics in 2004, 2009, and 2014.

a χ 2 test for group differences between 2004 and 2009 as well as between 2009 and 2014.
The distribution of specialty clinics among patients managed in multiple clinics is shown in Table 3. The patients were most often treated at an endocrine clinic in combination with another clinic. Among patients treated in two specialty clinics, the five most common combinations of specialties are shown in Table 4. The top five pairs accounted for 31% of all combinations in 2004, 29% in 2009, and 28% in 2014. The most common combination was endocrinology and cardiology, accounting for 12.1% in 2004, 11.5% in 2009, and 9.6% in 2014.
Frequency distribution of specialty clinics among patients in multiple outpatient treatment in 2004, 2009, and 2014.
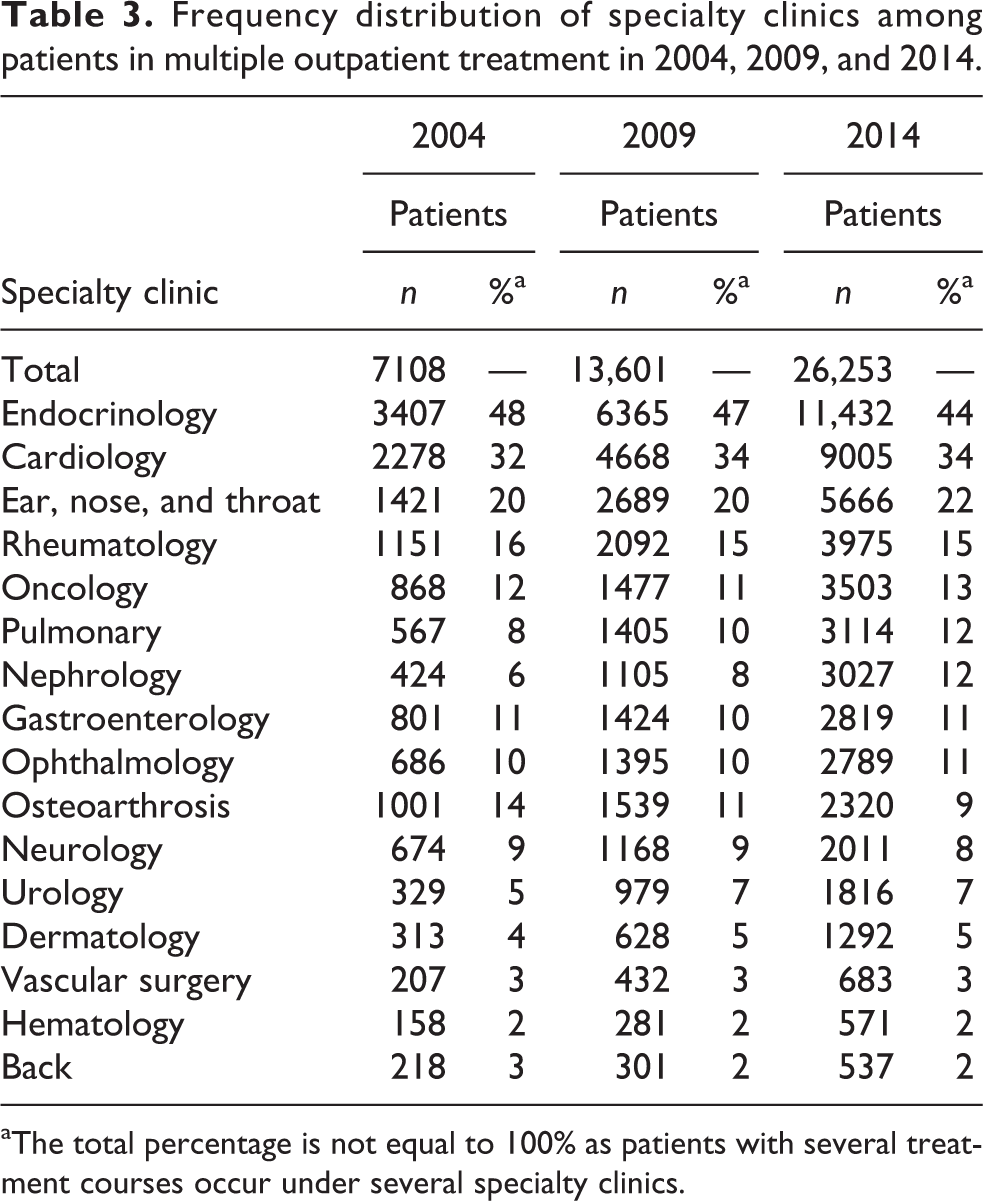
aThe total percentage is not equal to 100% as patients with several treatment courses occur under several specialty clinics.
Top 5 most common pairs of specialty clinics among patients with two hospital outpatient treatment courses in 2004, 2009, and 2014.

ENT: ear, nose, and throat.
Discussion
This study has shown that patients managed simultaneously in multiple hospital outpatient specialty clinics accounted for 7.7% in 2014, nearly double as many as in 2004. The most common specialty clinic combination was endocrinology and cardiology, but there was great diversity in the combinations of specialty clinics, and the top 5 specialty pairs accounted only for about one-fourth of all combinations.
Our main and novel finding is that the proportion of patients in multiple clinics nearly doubled over the last 10 years. In the existing literature, a time trend in this setting of hospital outpatient specialty clinics has not been studied before. This is probably because research in hospitals has traditionally had a single-disease or narrow-comorbidity focus, and MM in hospital outpatient settings is a relatively new research area. We found two studies from the primary health-care sector examining a time trend. 5,21 First, GPs in the Netherlands reported that the proportion of patients with MM increased by 67% over a 20-year period (from 12.3% in 1985 to 20.5% in 2005). 21 Another Dutch study showed a 28% increase over 7 years (from 12.7% in 2004 to 16.2% in 2011). 5 The deviation from the Dutch studies can be explained by target population differences between hospital and primary settings, where proportion estimates from the primary health-care sector were among patients with and without chronic diseases.
The large increase in the number of patients undergoing treatment in multiple clinics in our study could be explained by several factors. First, the fact that patients with chronic diseases presumably live longer in 2014 than 2004 due to treatment advances, thereby they have more opportunity to acquire more diseases. Since the severity of the diseases might increase over time or the additional diseases render treatment more complex, the GP refers more often to specialized hospital outpatient care. Second, the Danish health-care system recognized more diseases as a hospital specialty in 2014 than in 2004 (e.g. sleep disorders). Third, the Danish health-care system offered hospital treatment at an earlier stage of the disease in 2014 than in 2004 (e.g. insulin treatment for patients with type 2 diabetes).
Our second finding, the most common pair of specialty clinic combinations, has not previously been studied at the hospital level. A systematic review from primary care reported that hypertension and osteoarthritis were the most frequent combination, followed by different combinations of cardiovascular diseases. 22 This shows that MM may consist of many disease combinations in different patterns and are health-care specific, which must be considered when using our research for clinical practice.
Implications
The notable increase over the past 10 years in the number of patients who are treated in multiple hospital outpatient specialty clinics simultaneously gives rise to a number of considerations. While a 7.7% total may seem small, this is probably an underestimation since we did not include all diseases or hospital clinics. Furthermore, we presume that the proportion of the appointments consumed by these patients is at least twice as high. A Danish study on patients from the primary health-care sector showed an additive rise in outpatient appointments with number of diseases; that is, for example, patients with three chronic diseases had nearly three times as many annual outpatient appointments as patients with one chronic disease. 23 As the number of patients with MM is expected to increase, we expect a future increase of patients in multiple hospital outpatient care.
This encourages a focus on treatment regimens that take multiple diseases into account. One way is to identify common disease combinations and address which clinics should benefit from close corporation. For example, we found that patients often attend an endocrine clinic in combination with another type of clinic. Clinical pathways or disease management programs already exist for some combinations of diseases (e.g. diabetes, cardiovascular disease). 24 However, this study also found that it is the low-frequency combinations that account for most of the combinations. Future strategies for MM patient management should therefore be generic and non-disease specific. Approaches to multidisciplinary care for people with MM have already been initiated in Denmark and countries with similar health-care systems. 25
Strengths and limitations
Our study has some strengths. First, we had a large study sample, covering 100% of all Danish hospitals; second, because of the Danish health-care structure, all of the examined patient groups with specialized needs are referred to hospital outpatient specialty care, meaning that the development reflects a true increase; third, we sampled at three periods; and fourth, we included 50 diagnoses. This latter “strength” could also be seen as a limitation, however, as we did not include all patient groups in hospital treatment for chronic diseases and cannot calculate the total proportion of patients in hospital outpatient treatment for chronic diseases. Our study therefore probably shows an underestimation of the true figure.
Another limitation is that the process of how we chose diagnoses was based on frequent diagnoses at a total hospital level and then categorizing them into organizational outpatient specialty clinics. In that sense, we have not included all hospital specialty clinics in this study; only if the clinic cared for a diagnosis which was within the 50 most frequent hospital diagnoses.
This study did not include psychiatric hospitals, as they are separate from somatic hospitals in the Danish system. While information pertaining to patients treated in both somatic and psychiatric hospitals is important, it is not the focus in this study. Additionally, our study did not show if patients had other, less severe diseases than those investigated in our study. Patients may have one or even several courses of treatment for chronic diseases for which they are receiving treatment from their GP.
The decision about which diseases to include in the study was based on expert opinions. Other experts might consider otherwise. The diagnoses we included are from the NPR and generally of high validation, but not all diagnoses are validated. 13 We used primary diagnoses set by a specialized doctor in a hospital outpatient specialized clinic and had a 6-month criterion for inclusion, which strengthens the correctness of the diagnoses.
Further limitations include the categorization of diagnoses. We categorized diagnoses into clinical organizational groups using information from typical Danish hospital organizations. However, some hospitals may have organized their outpatient clinics differently.
Our results reflect a health-care system in which the specialist services for MM patients are almost completely covered by the hospital sector. In other countries, some specialists are operating outside the hospitals and our conclusions might not be applicable to such systems.
We did not include factors such as socioeconomic status, which has been shown in other studies to have a strong association with MM4 and would have been relevant to adjust for in the time-trend investigation and an analysis of different characteristics between patients in one or several hospital outpatient treatments.
Conclusions
This study has described the development of patients managed simultaneously in multiple hospital outpatient specialty clinics. We found that the proportion has increased nearly 100% over 10 years. Further, we found great diversity in the combination of specialty clinics in which patients with two diseases are treated. Our findings urge hospital outpatient managers to prepare for a future where increasing numbers of MM patients require more complex care. Research is needed on effective and cost-efficient initiatives using integrated care regimens for patients treated simultaneously in multiple outpatient specialty clinics.
Footnotes
Authors’ note
Due to Danish laws on personal data, data cannot be shared publicly. To request these data, please contact the corresponding author for more information.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a Grant from, Knud og Edith Eriksens Mindefond. The funding source played no role in the study design, the collection, analysis, or in the interpretation of data.
Appendix 1
Organizational diagnosis-group, ICD-10 code, and diagnosis.

| Specialty clinic | ICD-10 code | Diagnosis |
|---|---|---|
| Oncology | DC18 | Malignant neoplasm of colon |
| DC20 | Malignant neoplasm of rectum | |
| DC34 | Malignant neoplasm of bronchus and lung | |
| DC50 | Malignant neoplasm of breast | |
| Dermatology | DC44 | Other malignant neoplasms of skin |
| DL40 | Psoriasis | |
| Urology | DC61 | Malignant neoplasm of prostate |
| Hematology | DC91 | Lymphoid leukemia |
| Endocrinology | DE05 | Thyrotoxicosis (hyperthyroidism) |
| DE10 | Type 1 diabetes mellitus | |
| DE11 | Type 2 diabetes mellitus | |
| DE66 | Obesity | |
| DM81 | Osteoporosis without pathological fracture | |
| Neurology | DG35 | Multiple sclerosis |
| DG40 | Epilepsy | |
| Ophthalmology | DH02 | Other disorders of eyelid |
| DH25 | Senile cataract | |
| DH35 | Other retinal disorders | |
| DH40 | Glaucoma | |
| Ear, nose, and throat | DH90 | Conductive and sensorineural hearing loss |
| DH91 | Other hearing loss | |
| DH93 | Other disorders of ear, not elsewhere classified | |
| DG47 | Sleep disorders | |
| Cardiology | DI10 | Essential (primary) hypertension |
| DI20 | Angina pectoris | |
| DI25 | Chronic ischemic heart disease | |
| DI35 | Nonrheumatic aortic valve disorders | |
| DI48 | Atrial fibrillation and flutter | |
| DI50 | Heart failure | |
| Pulmonary | DJ30 | Vasomotor and allergic rhinitis |
| DJ44 | Other chronic obstructive pulmonary disease | |
| DJ45 | Asthma | |
| Gastroentrology | DK50 | Crohn disease (regional enteritis) |
| DK51 | Ulcerative colitis | |
| DK58 | Irritable bowel syndrome | |
| DB18 | Chronic viral hepatitis | |
| Rheumatology | DM05 | Seropositive rheumatoid arthritis |
| DM06 | Other rheumatoid arthritis | |
| DM07 | Psoriatric and enteropathic arthropathies | |
| DM45 | Spondylitis ankylopoietica | |
| Osteoarthrosis | DM16 | Coxarthrosis (arthrosis of hip) |
| DM17 | Gonarthrosis (arthrosis of knee) | |
| DM23 | Internal derangement of knee | |
| DM48 | Other spondylopathies | |
| DM75 | Shoulder lesions | |
| DM79 | Other soft tissue disorders, not elsewhere classified | |
| Back | DM51 | Other intervertebral disc disorders |
| DM54 | Dorsalgia | |
| Nephrology | DN18 | Chronic kidney disease |
| Vascular surgery | DI73 | Other peripheral vascular diseases |
Appendix 2
Number and relative distribution of treatment courses by diagnosis in 2004, 2009, and 2014.

| Specialty clinic | ICD | Diagnosis | 2004 | 2009 | 2014 | |||
|---|---|---|---|---|---|---|---|---|
| Treatment courses | Treatment courses | Treatment courses | ||||||
| n | % | n | % | n | % | |||
| Total | 185,143a | 100 | 262,520a | 100 | 372,976a | 100 | ||
| Oncology | DC18 | Malignant neoplasm of colon | 902 | 0.5 | 1759 | 0.7 | 3028 | 0.8 |
| DC20 | Malignant neoplasm of rectum | 660 | 0.4 | 932 | 0.4 | 1533 | 0.4 | |
| DC34 | Malignant neoplasm of bronchus and lung | 981 | 0.5 | 1561 | 0.6 | 2942 | 0.8 | |
| DC50 | Malignant neoplasm of breast | 12,654 | 6.8 | 16,382 | 6.2 | 25,903 | 6.9 | |
| Group total | 15,197 | 8.2 | 20,634 | 7.9 | 33,406 | 9.0 | ||
| Dermatology | DC44 | Other malignant neoplasms of skin | 1331 | 0.7 | 2169 | 0.8 | 3014 | 0.8 |
| DL40 | Psoriasis | 1201 | 0.6 | 1901 | 0.7 | 3660 | 1.0 | |
| Group total | 2532 | 1.4 | 4070 | 1.6 | 6674 | 1.8 | ||
| Urology | DC61 | Malignant neoplasm of prostate | 3826 | 2.1 | 8950 | 3.4 | 12974 | 3.5 |
| Group total | 3826 | 2.1 | 8950 | 3.4 | 12,974 | 3.5 | ||
| Hematology | DC91 | Lymphoid leukemia | 1785 | 1.0 | 2336 | 0.9 | 3333 | 0.9 |
| Group total | 1785 | 1.0 | 2336 | 0.9 | 3333 | 0.9 | ||
| Endocrinology | DE05 | Thyrotoxicosis (hyperthyroidism) | 6944 | 3.8 | 6916 | 2.6 | 7416 | 2.0 |
| DE10 | Type 1 diabetes mellitus | 16,859 | 9.1 | 18,462 | 7.0 | 20,308 | 5.4 | |
| DE11 | Type 2 diabetes mellitus | 17,030 | 9.2 | 24,870 | 9.5 | 28,666 | 7.7 | |
| DE66 | Obesity | 962 | 0.5 | 2867 | 1.1 | 3392 | 0.9 | |
| DM81 | Osteoporosis without pathological fracture | 2850 | 1.5 | 6788 | 2.6 | 12,926 | 3.5 | |
| Group total | 44,645 | 24.1 | 59,903 | 22.8 | 72,708 | 19.5 | ||
| Neurology | DG35 | Multiple sclerosis | 5169 | 2.8 | 7675 | 2.9 | 9657 | 2.6 |
| DG40 | Epilepsy | 11412 | 6.2 | 13037 | 5.0 | 15165 | 4.1 | |
| Group total | 16,581 | 9.0 | 20,712 | 7.9 | 24,822 | 6.7 | ||
| Ophthalmology | DH02 | Other disorders of eyelid | 477 | 0.3 | 1075 | 0.4 | 1854 | 0.5 |
| DH25 | Senile cataract | 1406 | 0.8 | 2317 | 0.9 | 3472 | 0.9 | |
| DH35 | Other retinal disorders | 1220 | 0.7 | 4394 | 1.7 | 8734 | 2.3 | |
| DH40 | Glaucoma | 828 | 0.4 | 1111 | 0.4 | 1583 | 0.4 | |
| Group total | 3931 | 2.1 | 8897 | 3.4 | 15,643 | 4.2 | ||
| Ear, nose, and throat | DH90 | Conductive and sensorineural hearing loss | 1783 | 1.0 | 2231 | 0.8 | 3554 | 1.0 |
| DH91 | Other hearing loss | 8877 | 4.8 | 10931 | 4.2 | 13519 | 3.6 | |
| DH93 | Other disorders of ear, not elsewhere classified | 1632 | 0.9 | 2366 | 0.9 | 3198 | 0.9 | |
| DG47 | Sleep disorders | 4493 | 2.4 | 9431 | 3.6 | 18946 | 5.1 | |
| Group total | 16,785 | 9.1 | 24,959 | 9.5 | 39,217 | 10.5 | ||
| Cardiology | DI10 | Essential (primary) hypertension | 4842 | 2.6 | 5600 | 2.1 | 7060 | 1.9 |
| DI20 | Angina pectoris | 3190 | 1.7 | 3730 | 1.4 | 4281 | 1.1 | |
| DI25 | Chronic ischemic heart disease | 3628 | 2.0 | 4835 | 1.8 | 6770 | 1.8 | |
| DI35 | Nonrheumatic aortic valve disorders | 3449 | 1.9 | 7248 | 2.8 | 12,986 | 3.5 | |
| DI48 | Atrial fibrillation and flutter | 5900 | 3.2 | 8839 | 3.4 | 14,562 | 3.9 | |
| DI50 | Heart failure | 2524 | 1.4 | 4740 | 1.8 | 7183 | 1.9 | |
| Group total | 23,533 | 12.7 | 34,992 | 13.3 | 52,842 | 14.2 | ||
| Pulmonary | DJ30 | Vasomotor and allergic rhinitis | 990 | 0.5 | 900 | 0.3 | 1308 | 0.4 |
| DJ44 | Other chronic obstructive pulmonary disease | 3686 | 2.0 | 6745 | 2.6 | 9814 | 2.6 | |
| DJ45 | Asthma | 3744 | 2.0 | 4785 | 1.8 | 7858 | 2.1 | |
| Group total | 8,420 | 4.5 | 12,430 | 4.7 | 18,980 | 5.1 | ||
| Gastroenterology | DK50 | Crohn disease (regional enteritis) | 5036 | 2.7 | 6355 | 2.4 | 8636 | 2.3 |
| DK51 | Ulcerative colitis | 8600 | 4.6 | 11039 | 4.2 | 14,999 | 4.0 | |
| DK58 | Irritable bowel syndrome | 614 | 0.3 | 926 | 0.4 | 1466 | 0.4 | |
| DB18 | Chronic viral hepatitis | 1857 | 1.0 | 3011 | 1.1 | 5103 | 1.4 | |
| Group total | 16,107 | 8.7 | 21,331 | 8.1 | 30,204 | 8.1 | ||
| Rheumatology | DM05 | Seropositive rheumatoid arthritis | 7143 | 3.9 | 9655 | 3.7 | 12,832 | 3.4 |
| DM06 | Other rheumatoid arthritis | 3391 | 1.8 | 4741 | 1.8 | 6468 | 1.7 | |
| DM07 | Psoriatric and enteropathic arthropathies | 1602 | 0.9 | 3283 | 1.3 | 5317 | 1.4 | |
| DM45 | Spondylitis ankylopoietica | 936 | 0.5 | 1818 | 0.7 | 2653 | 0.7 | |
| Group total | 13,072 | 7.1 | 19,497 | 7.4 | 27,270 | 7.3 | ||
| Osteoarthrosis | DM16 | Coxarthrosis (arthrosis of hip) | 4173 | 2.3 | 4267 | 1.6 | 3294 | 0.9 |
| DM17 | Gonarthrosis (arthrosis of knee) | 3046 | 1.6 | 4065 | 1.5 | 4749 | 1.3 | |
| DM23 | Internal derangement of knee | 1393 | 0.8 | 1334 | 0.5 | 3044 | 0.8 | |
| DM48 | Other spondylopathies | 956 | 0.5 | 1044 | 0.4 | 1539 | 0.4 | |
| DM75 | Shoulder lesions | 1400 | 0.8 | 2213 | 0.8 | 3584 | 1.0 | |
| DM79 | Other soft tissue disorders, not elsewhere classified | 653 | 0.4 | 789 | 0.3 | 1538 | 0.4 | |
| Group total | 11,621 | 6.3 | 13,712 | 5.2 | 17,748 | 4.8 | ||
| Back | DM51 | Other intervertebral disc disorders | 1960 | 1.1 | 1916 | 0.7 | 2226 | 0.6 |
| DM54 | Dorsalgia | 1410 | 0.8 | 1465 | 0.6 | 2052 | 0.6 | |
| Group total | 3370 | 1.8 | 3381 | 1.3 | 4278 | 1.1 | ||
| Nephrology | DN18 | Chronic kidney disease | 2523 | 1.4 | 4523 | 1.7 | 9882 | 2.6 |
| Group total | 2523 | 1.4 | 4523 | 1.7 | 9882 | 2.6 | ||
| Vascular surgery | DI73 | Other peripheral vascular diseases | 1215 | 0.7 | 2193 | 0.8 | 2995 | 0.8 |
| Group total | 1215 | 0.7 | 2193 | 0.8 | 2995 | 0.8 | ||
aThe total number of treatment courses is higher than the total number of patients, as shown in Table 1, as patients with several treatment courses occur under more than one diagnosis. Furthermore, patients can be enrolled with more than one diagnoses within each specialty clinic.