
Abstract
Background:
Birth preparedness and complication readiness (BPCR) is a strategy that promotes the timely use of skilled maternal and neonatal care among pregnant women. Positive pregnancy outcomes can be achieved by appropriate birth preparedness and emergency complication readiness planning.
Objective:
To explore the perceptions, benefits, awareness, and barriers of BPCR among pregnant women and health professionals at the antenatal care (ANC) clinic in the Oromia Region, Ethiopia.
Design:
An exploratory, phenomenological descriptive qualitative study conducted from March 20 to April 24, 2022.
Methods:
Three focus group discussion (FGD) sessions were conducted with 36 purposefully selected pregnant women attending ANC clinics. Key informant in-depth interviews (KIIs) were held with nine health professionals in Arsi Zone, Oromia, Ethiopia, using an interview guide. The data were analyzed using an inductive thematic analysis approach.
Results:
Among the FGD participants, 19 reside in urban areas and 17 in rural areas. The KII participants comprised six midwives, two health officers, and a nurse. The participants mentioned their perception of BPCR during pregnancy, childbirth, the postpartum period, obstetric danger signs, and barriers to BPCR. Different sources of information on BPCR were mentioned, including friends, neighbors, health professionals, and family. The study showed that the participants were unfamiliar with the major BPCR components. The health professionals planned to educate pregnant women during ANC visits to enhance the adequacy of their BPCR plans. Facilitating husband support, increasing health facility accessibility, economic empowerment, and transport access will enable pregnant women to develop adequate BPCR plans.
Conclusion:
This study’s findings indicated that most participants did not focus strongly on BPCR plans because of low awareness, lack of support from husbands, family, and the community, poor infrastructure, and improper handling by health professionals. To increase service utilization, husbands, families, and the community should be informed about the benefits of the BPCR plan for pregnant women.
Keywords
Introduction
According to the World Health Organization (WHO), birth preparedness and complication readiness (BPCR) is an essential element of the antenatal care (ANC) package. This strategic program often addresses efforts to increase awareness of BPCR among pregnant women, their families, and the community as part of the ANC service. 1 The components of BPCR include awareness of the danger signs and symptoms, and preparing for immediate action to prevent maternal and neonatal mortality. Appropriate birth preparedness and emergency complication readiness planning can promote positive pregnancy outcomes. 2
The Ethiopian Ministry of Health launched the community-based healthcare system in 2003. 3 One of its approaches involves assigning female health extension workers to each established health post at the grassroots level to provide maternal healthcare services. 4 Despite significant progress in birth preparedness and other maternal healthcare services, pregnant women still encounter numerous challenges in accessing maternal healthcare services. 5
An assessment of pregnant women’s BPCR level can inform strategies to promote their timely use of trained health professionals during childbirth, booking at ANC centers at the early stage of pregnancy, saving money for unexpected obstetric complications, and identifying means of transportation during labor to the health care facility. 6 In the 2021–2025 Federal Ministry of Health, Ethiopia’s reproductive health strategic document, one of the strategies to decrease maternal and newborn mortality due to obstetric complications involves implementing a BPCR plan at each smallest unit of the district (Kebele) throughout the country. 7
The WHO revealed that many women still die from complications during pregnancy, childbirth, and postpartum. 8 Women in developing countries have the highest lifetime risk of death due to obstetric complications. There is a probability that 1 in 37 15-year-old women will die in sub-Saharan Africa, versus 1 in 6500 in Europe and 1 in 7800 in Australia and New Zealand because of obstetric complications. 8
In Thailand, the maternal mortality ratio has improved from 48 deaths per 100,000 live births in 2000 to 29 deaths per 100,000 live births in 2020. In addition, the infant mortality rate has reduced in recent years, from 7.1 deaths per 1000 live births in 2021 to 6.5 deaths per 1000 live births in 2024. This reflects improved maternal and newborn health care outcomes. 9
According to a study conducted in Thailand, among 672 pregnant women attending ANC, 144 (21.4%) were unfamiliar with BPCR, 47% were aware of some danger signs during labor, and 70.4% planned to attend four ANC visits with a skilled provider. 10 Bangladesh has made remarkable progress in reducing maternal and neonatal mortality by implementing BPCR practices for pregnant women. In Bangladesh, maternal mortality has reduced from 173 deaths per 1000 live births in 2017 to 123 in 2020. In addition, neonatal mortality reduced from 42 deaths per 1000 live births in 2017 to 17.4 in 2020. 11 A study in a rural area of Bangladesh on the practice of birth preparedness in relation to the different components of BPCR among pregnant women and couples indicated that 80% of women identified a place of birth and skilled birth attendants in advance. 12
Husbands’ involvement and knowledge of BPCR are vital. A study in Tanzania found that upon confirmation of pregnancy, husbands began saving money to prevent potential obstetric complications, highlighting the importance of their engagement. 13
In Ethiopia, due to a lack of awareness of BPCR, when a woman’s first birth is without complications, they assume birthing the next baby at a health facility is unnecessary. 14
Women should be counseled on BPCR to ensure they know what to do if complications arise. Another study in Ethiopia determined that 65.1% of respondents did not receive counseling on BPCR and danger signs during pregnancy. 15 Of the counseled participants, only a few pregnant women were informed of the following danger signs: vaginal bleeding (30%), severe headache (19.4%), offensive vaginal discharge (14.4%), blurring vision (7.4%), and leg and facial edema (6%). 16 Another study in Ethiopia exploring health professionals’ opinions on BPCR identified that women had a low perception of risks during pregnancy and did not seek maternal health services if they felt well during pregnancy. 17
To improve BPCR among pregnant women, the barriers should be identified. Some of the barriers to BPCR include a lack of access to transportation, a significant distance between the home and health facility, low decision-making power, poor access to information, a lack of husbands’ support, inconvenient times, poor socioeconomic status, disregarding health professionals’ behavior, and conceiving out of wedlock.18 –23
BPCR encourages the prompt seeking of professional care for mothers and newborns. It is important to know the signs of danger and obstetric complications, choose a birthplace and provider, obtain basic safe birth supplies, and identify a woman’s companion. Other requirements include transportation, money, and temporary family care in cases of emergency. 24 In this study, we aimed to explore pregnant women and health professionals’ perceptions toward BPCR at the ANC clinics in the Arsi Zone, Oromia Region, Ethiopia.
Methods
Study design and setting
An exploratory phenomenological descriptive qualitative research design was used to explore pregnant women’s perceptions of BPCR while attending ANC clinics in two health centers and one referral hospital in Arsi Zone, Ethiopia. These facilities were selected from the health facilities in 26 districts of the Arsi Zone using the lottery method. Health professionals’ beliefs about BPCR were also assessed via key informant in-depth interviews (KIIs). According to the 2020 annual plan of the Arsi Zone Health Office, the total population of the zone is estimated at 3,673,474 million, with 812,940 women of childbearing age and 127,470 pregnant women; 90% of the population resides in rural areas. 25
Study population and sampling
The study population included pregnant women attending an ANC clinic in the above-mentioned health facilities and health professionals who provided maternal and child healthcare (MCH) services in the Arsi Zone, Ethiopia. In addition, three focus group discussion (FGD) sessions with 12 participants each (a total of 36 purposefully selected pregnant women) were conducted, one at the hospital and two at the health centers. KIIs were conducted with nine purposively selected health professionals.
Inclusion and exclusion criteria
Inclusion criteria: Pregnant women who had attended at least two ANC visits for their current pregnancy before this study.
Exclusion criteria: Pregnant women who did not volunteer to participate in this study.
Data collection procedure
Semi-structured interviews and FGD guides were developed based on existing related literature on BPCR among pregnant women. 21 The interview guides were developed with open-ended questions to enable the researcher to explore participants’ perceptions and experiences on the research topic. The core aspects covered in the KII guide include challenges encountered in implementing BPCR and pregnant women’s suggested intervention strategies to improve BPCR. The prepared FGD and KII guides were translated into Afan Oromo and Amharic local languages. The FGD guide was pretested on eight pregnant women, and the KII on four health professionals in a facility where the actual study was not conducted (Sagure Health Center), to allow necessary modifications to the data collection tools before data collection. This study also used the consolidated criteria guidelines for reporting qualitative research. 26
Data collection spanned from March 20, 2022, to April 24, 2022. KIIs were conducted following the FGD sessions.
The FGDs were conducted at one hospital and two health centers using the Afan Oromo and Amharic local languages spoken in the study areas. Discussions were conducted face-to-face in a quiet place to prevent noise and other disturbances. After greeting the participants, the researcher introduced the objective of the FGD, and informed consent was obtained from them. The FGDs were audio-recorded with participants’ permission, and a research assistant simultaneously took field notes.
The KIIs were conducted in the Afan Oromo and Amharic languages. The objective of the KII was introduced to each participant before the interviews began. The KII sessions were held in participants’ offices at suitable times to give each individual sufficient time for in-depth interviews until the required data saturation was reached. Each FGD and KII lasted approximately 70 and 45 min, respectively.
Data analysis
The data collected were cross-checked, and the complete dataset was analyzed. The findings were coded, categorized, and summarized using an inductive thematic content reduction and analysis strategy to analyze the basic concepts of the data collected. All FGDs and KII data were independently coded by the principal researcher and the research assistants. The researcher listened carefully to the records and read the notes taken during each FGD and KII to determine whether further revision was necessary. The researcher translated the audio transcripts and notes from Amharic and Afan Oromo into English. A language expert fluent in English, Amharic, and Afan Oromo checked the consistency of the translated Amharic and Afan Oromo versions before further data analysis. The translated data were exported to the qualitative data analysis software ATLAS ti version 8 for further content analysis and integrated into the Johns Hopkins Program for International Education in Gynecology and Obstetrics model related to the BPCR perception of pregnant women. The main themes derived from the FGDs and KIIs are presented in the results section, with quotes to substantiate the findings.
Results
In total, 36 pregnant women participated in the FGDs. The minimum, maximum, and mean age of the participants were 16, 36, and 25 ± 5 years, respectively. Notably, 18 (50%) participants were between the ages of 26 and 30.
In addition, 34 pregnant women were married, and 2 were single. Nineteen participants lived in urban areas, and 17 lived in rural areas. Nineteen participants were Orthodox, 15 were Muslim, and 2 were Christian. Overall, 23 participants had primary education, 7 had secondary education, 5 had a college degree or higher, and 1 could not read or write. Thirty-five pregnant women were housewives, and one was a government employee. Fifteen women were pregnant for the first time, eight for the second time, seven for the fourth time, and one for the sixth time (Table 1).
Demographic characteristics of the FGD participants.

FGD, focus group discussion.
The minimum, maximum, and mean ages of the KII participants were 30, 45, and 37 ± 5 years. Of the nine KII participants, seven were females. The nine participants comprised six midwives, two health officers, and a nurse. Four participants were ANC care providers, three were MCH coordinators, and two were health facility directors. The participants’ minimum service duration was 9 years, and the maximum was 25 years (Table 2).
Demographic characteristics of the KII participants.
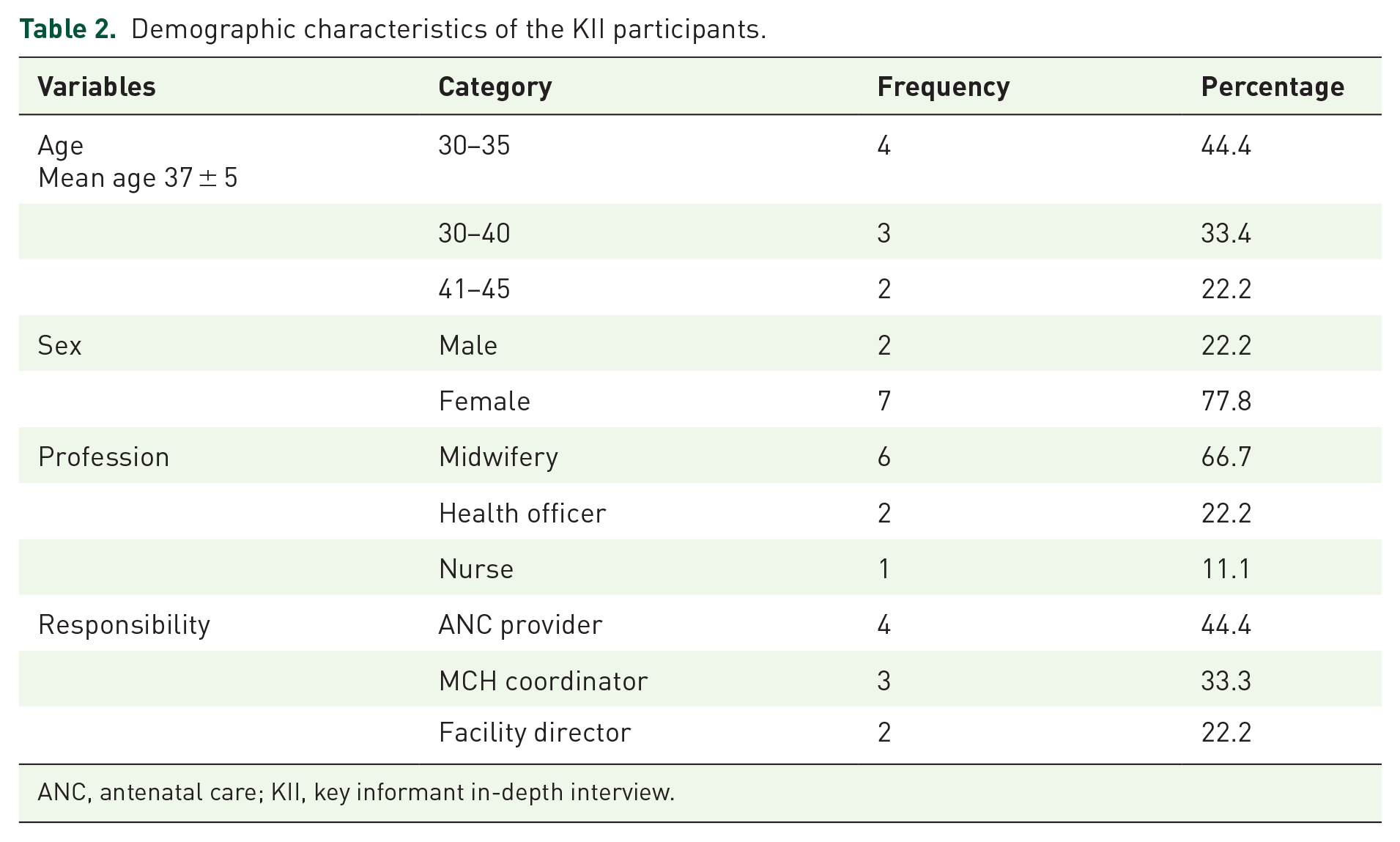
ANC, antenatal care; KII, key informant in-depth interview.
Themes
Four themes emerged from the FGDs and KIIs (Table 3).
Themes and subthemes of FGDs and KIIs in the Arsi Zone, Oromia, Ethiopia, 2022.

ANC, antenatal care; BPCR, birth preparedness and complication readiness; FGD, focus group discussion; KII, key informant in-depth interview.
Theme 1: Obstetric problems pregnant women encountered during pregnancy
This theme addressed the danger signs that could occur during pregnancy, childbirth, and the first 2 days postpartum.
Subtheme 1.1: Danger signs encountered during pregnancy
The findings reflected that some participants were unaware of key danger signs that may present during pregnancy. For instance, a pregnant woman from Eteya Health Center (EHC) was asked, “What are the obstetric danger signs that happen during pregnancy?”
Her response was
I am not familiar with the problem happening during pregnancy. I came to the health center to take the vaccine and for a pregnancy check-up, but nobody told me about any danger signs happening during pregnancy. (Pregnant woman aged 26 years).
Few participants could identify the danger signs:
The problems that arise during pregnancy can be vomiting, weakness of the body, and the fetal movement may stop. (Pregnant woman aged 25 years)
One of the pregnant women from Ogolcho Health Center (OHC) mentioned that the most common danger sign during pregnancy is vaginal bleeding, based on her experience in a previous pregnancy:
I was 6 months pregnant before this pregnancy, and the blood and fluid were leaking from my womb. I was afraid of the situation when I came to the health center. The female health professional wrote me a referral letter to the hospital, and then I was admitted for more than a month. After my problem was treated, I went back home and gave birth in the health center. (Pregnant woman aged 27 years)
Subtheme 1.2: Danger signs encountered during labor
Participants identified the following key danger signs during labor: prolonged labor, fetal malpresentation, vaginal bleeding, and pregnancy-induced hypertension, among others.
One participant from EHC indicated:
One of the participants from EHC indicated:
The problem during labor is being unable to give birth at home due to prolonged labor, which makes the mother weak. I remember last year when my brother’s wife was pregnant for the first time. Her labor started, but she did not tell anybody. After that, when the labor became strong, the husband took her to the health center; the health center confirmed that the fetus had become weak. When they arrived at the hospital, the fetus had died in the womb. (Pregnant woman aged 36 years).
Another participant from EHC mentioned that negligence by the family and community at the onset of labor might delay pregnant women from going to the health facility.
For my part, the problem during labor is a delay in giving birth in our area. The family, the community, and other members expect that the labor is always simple for them; they say again, and again, don’t take her anywhere she will give birth now; this saying worsens the labor to a complicated situation. (Pregnant woman aged 21 years)
Subtheme 1.3: Danger signs encountered during the first 2 days of the postpartum period
Most maternal and newborn deaths occur during the first 2 days of the postpartum period. This critical period requires urgent care for the mother and the newborn to save their lives.
A participant described some danger signs during the first 2 days of the postpartum period as follows:
Bleeding is one of the problems that happens after giving birth. Bleeding is dangerous for most pregnant women. I remembered my neighbor in the countryside; she was sick during her pregnancy, but nobody took her to the health facility. After some days, she gave birth at home, but she started to bleed. The bleeding did not stop, and the husband took her to the hospital. Finally, she died, leaving her 1-week-old neonate alone. (Pregnant woman aged 25 years)
Another participant from Asella Hospital (AH) mentioned that there are no danger signs for a pregnant woman and her newborn during the postpartum period:
Once you give birth, nothing will happen after birth, but in my perception, breast pain and the child not sucking the breast may be the problem unless I do not know another problem. (Pregnant woman aged 28 years)
Theme 2: Pregnant women’s utilization of obstetric services
This theme addresses the perception, experience, and level of ANC service utilization among pregnant women.
Subtheme 2.1: Pregnant women’s perception of ANC service
Assessing pregnant women’s perceptions of ANC services and sharing these experiences will enhance their early use of ANC and increase ANC visits.
One participant from EHC mentioned her perception as follows:
I was pregnant three times. I am starting ANC when the fetus moves in my womb. My reason for the ANC visit is to know my gestational age and to have a vaccine. More than this, I do not know. (Pregnant woman aged 28 years)
Another participant from OHC mentioned the benefits of ANC visits:
The benefit of ANC is not questionable. During antenatal care, it is possible to identify the status of the pregnancy and associated problems. Unless social and other issues require a follow-up visit to the ANC, as much as possible, I have planned two to three ANC visits throughout this pregnancy because it can prevent complications resulting from pregnancy and childbirth. (Pregnant woman aged 30 years).
Subtheme 2.2: Pregnant women’s experience of ANC services in the community
Identifying the experience of pregnant women who attended ANC services in the community helps to identify why some pregnant women do not attend ANC, and others report good ANC attendance.
One participant from AH mentioned the following in relation to her attendance at ANC services:
Due to a lack of awareness of the benefits of ANC, pregnant women start the ANC at the time of late pregnancy or when they face a problem related to the pregnancy. If the pregnancy is normal for her, she does not feel sick. She gives birth without attending ANC. Most of the pregnant women in our community do not start ANC visits in the early stages of pregnancy since being pregnant is usual and not expecting bad things related to pregnancy. (Pregnant woman aged 23 years)
Another participant from OHC explained her ANC trends: most pregnant women visit the health facility if they feel sick. This may indicate a lack of awareness of the purpose of ANC among pregnant women and the community.
I want to attend an ANC visit only when I feel sick; when I’m normal, I stay home without having an ANC visit. I am so busy with household activities throughout the day, if you go to the health facility frequently for an ANC visit, the community assumes that you are sick. (Pregnant woman aged 35 years)
Subtheme 2.3: Major barriers that hinder pregnant women’s use of ANC services
Notably, some barriers preventing pregnant women from attending ANC services included a lack of quick services, transportation difficulties, long waiting times, socioeconomic factors, and negative perceptions among husbands and the community toward ANC services, as mentioned by the participants.
I knew the benefit of ANC visits, but due to many constraints like transportation, lack of money, and busy household work, I did not follow the ANC service at an early stage of pregnancy and the full follow-up visit of the ANC. (Pregnant woman aged 35 years)
Another participant from EHC explained that a long waiting time at the health center was one of the constraints that influenced her not attending the ANC service:
Long waiting times at the health center disappoint me not to have frequent ANC visits. I have to get back to my home without delay because I have many responsibilities there, and sometimes I do not get a cart to travel home if it is too late. (Pregnant woman aged 25 years)
One participant from AH revealed that her husband was not in support of her visiting the hospital frequently.
When I go to the hospital frequently for ANC visit, my husband feels as if I have neglected the household work, and I’m not giving care to my children. Therefore, I only attend a maximum of two visits to the health center throughout my pregnancy. (Pregnant woman aged 26 years).
Subtheme 2.4: Pregnant women’s preferred place for giving birth
Identifying a place to give birth before the onset of labor is helpful for pregnant women to prevent birth-related obstetric complications.
A pregnant woman from EHC mentioned that she lived far from the health facility, which forced her to give birth at home.
My home is far away from the health center; if it were nearer to me, I would like to give birth in the health center, but it’s not. I had three of my children in my home, and even though I am suffering a lot, I finally gave birth to my third child at home. (Pregnant woman aged 31 years)
Another participant from AH explained that the home environment was more comfortable than the health facility.
I preferred home delivery to a health institution because everything is available in the home. For instance, if you want to get food, you will get it soon; the same thing is true if you want to drink coffee, you can get it at home. You are always a stranger to the health facility. I don’t feel free as my home; if the government-built a nearby health center, I may give birth there. (Pregnant woman aged 35 years)
Assessing pregnant women’s perceptions of and reasons for giving birth in a health facility promotes a better understanding of the advantages of giving birth in these facilities. Two participants from OHC and AH mentioned why they preferred giving birth at a health facility:
. . . it is advantageous to the woman when she gives birth at health facilities because everything is complete here. After the placenta is removed and the bleeding stops, she can go home without any problems. (Pregnant woman aged 30 years). . . . instead of giving birth at home, it is better to give birth at the health facility because if the labor starts at night, and you encounter a problem, it is very difficult to access transportation to reach the health facility. . . death can happen without getting treatment; therefore, I preferred giving birth at a health facility birth to giving birth at home. (Pregnant woman aged 27 years)
Theme 3: Pregnant women birth preparedness
This theme addresses pregnant women’s awareness of the benefits of BPCR.
Subtheme 3.1: Saving money to use during an emergency
Participants perceived saving money during pregnancy for obstetric emergencies as beneficial; one participant emphasized the benefit of saving money based on her previous pregnancy experience.
It is my second pregnancy; I have started saving money because I encountered a prolonged labor and birth complication during my first pregnancy. I have faced transportation and scarcity of money to buy drugs that I used when giving birth. Learning from my previous experience, it is better to prepare before the problem happens. (Pregnant woman aged 23 years)
Another participant from OHC mentioned that she did not save money; instead, she planned to prepare food to eat after giving birth and buy clothes for her newborn.
. . .since my birth date is not close, I do not prepare at this time. When the due date comes, I will prepare food for myself and clothes for my baby. (Pregnant women 22 years)
Subthemes 3.2: Identifying means of transportation
The participants stated that identifying an appropriate means of transportation before an obstetric emergency would enable them to reach the health facility without delay. Transportation options should be identified instead of pregnant women depending on the free ambulance service provided by the health center because one ambulance does not cover all areas.
The number of ambulances in the health facility is not enough to serve the laboring mothers. Only one ambulance serves all laboring mothers residing in the district. The makes pregnant women arrive late or unable to give birth in the health institutions due to the absence of an ambulance. My neighbor, who faced complicated labor at home, said that when she called the driver, he was taking other women to the hospital. Until the rental car search, she bled a lot. After she gave birth at Assela Hospital, she was admitted for more than a month for severe blood loss. (Pregnant woman aged 30 years). As much as possible, I try to catch the phone number of the health center Ambulance driver; if I have it, I will prepare the money for transportation, but money is scarce. I am not preparing more than what I have mentioned; since emphasis is not given to labor and delivery by my husband or family, they count it as a normal process. (Pregnant woman aged 24 years)
Subtheme 3.3: Planning for the place of birth
Free services promote pregnant women’s intentions to give birth at a public health facility. Most participants mentioned that they planned to give birth at the public health facility because some services were free. Two participants indicated the following:
. . . I have planned to give birth in this hospital because some of the services are given freely without payment. I also undergo ultrasound examinations without payment. I am satisfied with this free service. (Pregnant woman aged 28 years) If transportation services were facilitated, I would have planned to give birth in the hospital, but the hospital did not provide ambulance service for the pregnant woman during labor. I remember my neighbor, her labor started at night with no one in the house with her. The intensity of the labor increased without any assistance. She gave birth at home, but she bled a lot. Finally, when she went to the hospital, on arrival, she died.” (Pregnant woman aged 35 years)
Subtheme 3.4: Identifying skilled birth attendants
Most pregnant women were unfamiliar with the importance of identifying skilled birth attendants during pregnancy. One participant mentioned that labor is a normal process, and there is no need to identify a skilled birth attendant.
God solves all problems since we are in the hand of God; our preparation is nothing, I will not expect complications to happen, so there is no need for me to identify a skilled birth attendant. (Pregnant woman aged 25 years)
Subtheme 3.5: Benefits of early BPCR
Most participants mentioned the advantages of birth preparedness in the early stages of pregnancy. However, some were unfamiliar with BPCR, whereas others were reluctant to adopt BPCR.
. . . In my opinion, as I have understood it, early preparation at the early stage of pregnancy is advantageous because instead of searching for a solution when problems arise, it is better to plan and prepare early. (Pregnant woman aged 30 years)
Another participant mentioned that she was not aware of what she needed to prepare for birth because nobody told her.
. . . I am not aware of birth preparedness since this is my first pregnancy. During my ANC visit, the health worker did not tell me. I will plan it in the future. (Pregnant woman aged 25 years)
Subtheme 3.6: Support and care given to pregnant women during the obstetric period
Husbands’ support during the obstetric period is critical for a healthy pregnancy and safe labor. Lack of support from their husbands can discourage pregnant women from using obstetric care, as reported by the participants:
My husband helps me with the housework and looks after my children when I go to the health facility. Sometimes he cooks food for us. Since I have no money, he gives me money for transport, to buy drugs, and other expenses at the health facility, but he does not accompany me to the health facility. Most husbands feel pregnancy is a woman’s business. (Pregnant woman aged 28 years) My husband assists me with all household activities, including cooking food and looking after our children, and he shares all my challenges and my happiness; I am so happy with his conduct. He helps me more when I am pregnant. (Pregnant woman aged 26 years)
One pregnant woman from OHC did not receive any support from her family during the postpartum period. She mentioned that it was difficult to manage all the challenges related to childbirth.
. . .I was married far away from my family, and we are living away from my husband’s family. Therefore, no one helps me any time, especially since I suffered a lot during the postpartum period. Getting help from somebody is very necessary. For instance, I was sick for some days during my first childbirth, and I was in great difficulty handling my newborn because my husband lacks experience with newborn care. (Pregnant woman aged 21 years)
Subtheme 3.7: Challenges in planning BPCR for pregnant women
According to the participants, some obstacles to adopting BPCR include a lack of understanding of the benefits of BPCR, a poor perception of BPCR among husbands, and inadequate information from health professionals. Three participants stated the following:
. . . the obstacle preventing me from adopting BPCR is a lack of understanding of the benefits of early preparation. Another obstacle is my husband’s poor perception and lack of support for me; unless the husband does not support the woman, she does not do anything alone. (Pregnant woman aged 27 years). . . .due to the numerous activities of the health worker, I did not receive adequate information on birth preparedness and complication readiness from the health worker during my ANC visit. She only told me about the next ANC visit appointment. (Pregnant woman aged 28 years) The expectation of the husband, family, and community that pregnancy is always normal makes them negligent. They perceive it as a culture and did not give due attention to the complications raised. Therefore, they do not adopt BPCR before the complication happens. (Pregnant woman 24 years)
A key informant from EHC indicated a challenge of pregnancy outside of marriage, including a lack of engagement in BPCR, leading to neglect of the fetus, low socioeconomic status, and shying away from the social norm of pregnancy after marriage. When they experience complicated labor and are referred to a higher-level health facility, they often do not have the funds for transportation or other expenses.
. . . there are also pregnant mothers who became pregnant out of wedlock and did not have an ANC visit due to many social constraints. This problem complicated the referral system since they did not have money for transport or a person to accompany them to the referral area. Due to no budget allocated by the health center for this purpose, we begged for money from people and staff to covey her to the referral places. (Key informant interview, female aged 37 years)
Theme 4: Key informant health professional in-depth interview on BPCR
This theme addressed the challenges health professionals faced while implementing BPCR services for pregnant women.
Subtheme 4.1: Challenge faced by health professionals during BPCR implementation
The professional challenge to implementing BPCR in our hospital is due to the large daily flow of pregnant women, which does not enable us to address the benefit of BPCR to each client. This creates a shortage of time for the health professional. Another challenge is the narrowing of the room to give health education. (KI1 interview, female midwife aged 34 years)
The study identified the job burden of health professionals due to the inadequate assignment of health professionals to address BPCR of pregnant women during ANC visits, childbirth, and the postpartum period, and offer high-quality maternal services.
. . . The influx of laboring mothers increases more at night than in the daytime, so the health center only assigned one midwife for night duty. One midwife was serving the whole procedure conducted on the laboring mother, including filling out partographs, following the progress of labor, managing the delivery, and postnatal care. (KII, female midwife aged 41 years)
Subtheme 4.2: Institutional challenges the health professionals faced during BPCR implementation
A key informant asserted that the BPCR plan for pregnant women was not included in any standard operating procedures, and they had no data that indicated which pregnant women had planned for birth preparedness.
We do not have the exact number of pregnant women planning birth preparedness. The midwife informs them about birth preparedness during the ANC visits; furthermore, we do not have a registration book or the standard operating procedures to guide birth preparedness and complication readiness practices. (KII, female midwife aged 36 years)
Theme 5: Suggested intervention strategies to improve pregnant women BPCR
This theme addresses strategies to improve the birth preparedness practice among pregnant women to prevent obstetric complications during pregnancy, childbirth, and the first 2 days of the postpartum period.
Subtheme 5.1: Suggested strategies to improve pregnant women’s utilization of BPCR from FGD participants
Lack of income, poor awareness of obstetric services, lack of partner involvement in the BPCR plan, and mismanagement by health professionals were some of the problems participants mentioned that hindered planning for BPCR. The pregnant women suggested that they require great empowerment to generate their income, training for health professionals on good healthcare approaches, and enhanced partner involvement in the BPCR plan.
. . . empowerment of pregnant women to generate their income can enable the women to make their own decisions to plan for birth preparedness and use other obstetric services. (Pregnant woman aged 25 years)
The importance of partner involvement in BPCR was raised and discussed by the participants. They have mentioned that most maternal health services are not arranged for partners’ participation in BPCR; therefore, pregnancy seems to be only a woman’s problem.
. . . For my part, improving partner involvement in maternal health services is crucial. Most partners consider all reproductive issues to be female. The health institution needs to raise awareness about birth preparedness practices for partners at the community or village level. (Pregnant woman aged 28 years)
During the FGDs, the participants discussed health professionals’ negative behaviors. Some health professionals exhibited negative attitudes toward pregnant women during ANC visits and other maternal services.
‘. . .some of the health workers do not have respect for pregnant women during ANC visits. If they do not answer our question in a polite manner and with respect, it is better to give training on good conduct and how to approach pregnant women with a smile. (Pregnant woman aged 25 years).
This finding showed that a home-based postnatal service should be provided by a nearby health facility to prevent complications during the first two postnatal days. According to cultural norms, women are not allowed to leave their homes in the first few days after giving birth; therefore, it is difficult for pregnant women to plan the first 2 days of postnatal service at a health facility.
. . . according to our culture, a woman who gives birth early is not allowed to go outside the home because she may encounter a problem due to her body being weak. Most women are not permitted to go to a health facility within 2 days or 7 days postpartum. (Pregnant woman aged 25 years) To solve all obstacles, the health center should plan to provide a home-based early postnatal care service. Changing the perception of the community by giving sustainable information about the importance of early postnatal care is necessary; additionally, getting support from influential community members is important because I am not allowed to go out of my bed and under the sun for a minimum before 15 days of delivery, except when I am going to the toilet early in the morning before sunrise. (Pregnant woman aged 28 years)
Subtheme 5.2: Suggested intervention strategies to improve BPCR of pregnant women from KII participants
This theme addressed the strategies suggested by KII health professionals to improve pregnant women’s BPCR and minimize preventable obstetric complications during pregnancy, labor, and the first 2 days postpartum.
‘. . . rewarding the model pregnant women who attend all ANC visits, plan for birth preparedness, and benefit from birth preparedness can initiate the others. (KII, female aged 37) . . . Inviting the women to hear the trends of pregnant women who encountered or faced pregnancy complications and suffered from a shortage of money, transportation, delay to reach a health facility during pregnancy, labor, at birth, the postpartum period, and the action she took to resolve the problems. (KII, female aged 45 years)
The KII ANC provider from EHC mentioned that an intervention strategy to improve BPCR entails increasing awareness of birth preparedness by conducting women’s conferences at the family and community levels.
. . . the future strategies I suggest will be preparing women conference program to create an awareness of birth preparedness and complication readiness practice with their husbands including the community, and influential persons. (KII, female aged 40 years)
A KII participant from AH also indicated that the greatest challenge in improving BPCR among pregnant women is the lack of BPCR programs integrated into the ANC service, as well as the health facility’s annual and monthly reports. The Federal and Regional Ministry of Health should address this issue by including the program as an ANC component.
. . .helpful strategies to implement BPCR include addressing the hot issue of the program in the federal and regional health offices by including birth preparedness in the annual plan and monthly report of health facilities, which enables health professionals to report BPCR of pregnant women to regional and federal health offices. (Key informant interview, female aged 38 years)
Another KII from EHC emphasized the importance of providing a maternity waiting area for pregnant women who reside far from the health facility, where they can stay until they give birth.
. . . building a maternity waiting area for the pregnant women who are in the third trimester of pregnancy and coming from far away to stay here until they give birth. This action can prevent shortages in transportation and birth complications that can occur at home. (KII, female aged 46 years)
Discussion
This study explored the perceptions of pregnant women toward BPCR at ANC clinics in the Oromia Region, Ethiopia. Five major themes emerged from the data: (i) obstetric problems pregnant women encountered during their pregnancy; (ii) pregnant women’s utilization of obstetric services; (iii) pregnant women’s birth preparedness; and (iv) key informant health professional in-depth interviews; and (v) suggested intervention strategies to improve pregnant women’s BPCR.
This study’s findings showed that pregnant women’s BPCR was very low, and most pregnant women merely planned to prepare food for consumption after birth and during the postpartum period and buy clothes for the newborn. Only a few participants mentioned the major components of BPCR, such as saving money for emergencies and identifying a reliable means of transportation. This result aligns with a study from Ghana, where most participants never knew they had to arrange transport and save money to use during an obstetric emergency. 27 This study also identified a gap in addressing the importance of the BPCR plan with pregnant women during ANC visits. This finding was supported by a study conducted in Kenya, where <50% of pregnant women were informed about BPCR; no one taught them about birth plans, and they just waited for their delivery time. 28
Regarding the danger signs detected during pregnancy and childbirth, most participants reported vaginal bleeding. This finding is similar to those in Ethiopia and India, where participants mentioned vaginal bleeding as a frequently occurring obstetric sign of danger.29,30 The similarity in these studies might be attributed to the fact that pregnant women can easily observe bleeding, but complications such as obstructed labor, sepsis, and pregnancy-induced hypertension are among the life-threatening obstetric complications that participants cannot identify. Therefore, it is important to create awareness among pregnant women about the danger signs during ANC visits.
Identifying where to give birth before labor begins can prevent complications during labor and childbirth. The study showed that some pregnant women preferred home deliveries to a health facility because they found their homes more comfortable, with access to food and no additional expenses for transportation. A study in Gondor, Ethiopia, reported similar findings: participants did not worry about the risk and were very happy with home delivery. 22 However, a study in Ghana indicated that all participants decided to give birth in a health facility because they felt more secure and received greater medical attention at the health facility. 24 The variation between the two countries might be attributed to a higher awareness of the benefits of health facilities among participants in Ghana.
The barriers that prevented this study’s participants from planning for BPCR during pregnancy were poor awareness, distance from a health facility, lack of support from their husbands, waiting time to seek services, and lack of money. Similar studies revealed that transportation issues and a lack of knowledge about BPCR prevented women from planning for BPCR. 31 In addition, another study emphasized long waiting times as a barrier to BPCR. 32
The use of obstetric services and BPCR practices depends on the pregnant woman’s husband or family support throughout her pregnancy. Participants with spouse support were very pleased and had easy access to ANC and other maternal treatments without facing financial or other obstacles. 33 This is consistent with research conducted in Ethiopia, which concluded that husbands’ involvement in BPCR encouraged their spouses to use skilled birth attendants and plan for BPCR. 34
In this study, pregnant women who experienced obstetric issues in their previous pregnancies discussed the advantages of a BPCR plan to avoid potential obstetric complications during pregnancy, childbirth, and the postpartum period. Similarly, a study in northern Ethiopia found that obstetric health issues and complications during previous pregnancies compelled women to choose experienced delivery attendants during subsequent pregnancies. 35
Strengths and limitations of this study
The study provides precise insights since the qualitative method allowed an in-depth exploration of pregnant women’s views on BPCR. However, the study setting may not be generalized to other places in the country due to the small sample size and the possibility of interviewer bias in this qualitative research. Author bias might influence the researcher’s experience, belief, and value in the study process. This study suggests conducting more research at the community, policymaker, and program levels using different research approaches to identify the root causes of pregnant women’s lack of early action on the main components of BPCR.
Conclusion
Our findings indicated that most study participants did not focus strongly on BPCR plans because of low awareness, lack of support from husbands, family, and the community, poor infrastructure, and improper handling by health professionals. Conversely, BPCR was conceptualized by pregnant women who previously experienced obstetric complications and had learned from their and others’ experiences. To increase service utilization, husbands, families, and the community should be informed about the benefits of the BPCR plan for pregnant women.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251345951 – Supplemental material for Pregnant women and health professionals’ perceptions toward birth preparedness and complication readiness in Oromia, Ethiopia
Supplemental material, sj-docx-1-reh-10.1177_26334941251345951 for Pregnant women and health professionals’ perceptions toward birth preparedness and complication readiness in Oromia, Ethiopia by Mengesha Solomon Tejineh and Thanyani Lumadi in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
The authors express their deepest gratitude to the study participants and research assistants. We appreciate the Oromia Regional Health Office and Arsi Zone Health Office for providing the necessary information and support during data collection. We would like to thank Editage (![]() ) for English language editing.
) for English language editing.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.