
Abstract
Background:
Obstetric ultrasound is a harmless, cheap, and noninvasive imaging modality that helps to scan a pregnant mother and delivers parents with a real-time image of the fetus. As the number of pregnancies rises globally, the demand for obstetric ultrasound becomes even more pressing.
Objectives:
To assess pregnant women’s knowledge, attitude, and associated factors toward obstetric ultrasound in public hospitals, Ethiopia.
Methods:
Institutional based cross-sectional study was employed. Systematic random technique was used to select 419 pregnant women from 10 April 2021 through 2 June 2021. A structured questionnaire was used to collect data during a face-to-face interview. Then the data were coded, cleaned, and entered into Epidemiological data version (EPIDATA) 3.1 and exported to the statistical package for Social Science version 23.0 for analyses. Bivariate and multivariable logistic regression model was used to identify statistically significant associations between dependent and independent variables. The odds ratio at 95% confidence interval with p-value 0.05% was considered statistically significant.
Result:
The majority of the study participants, 179 (42.8%), have ages ⩾ 25 years. Magnitude of having good knowledge and positive attitude of pregnant women toward obstetric ultrasound was 35.5% and 69.5%, respectively. Residence (adjusted odds ratio: 3.934; 95% confidence interval: 3.125–6.761), educational status (adjusted odds ratio: 3.614; 95% confidence interval: 1.986–5.964), and parity (adjusted odds ratio: 2.7621; 95% confidence interval: 1.68–3.275) were significantly associated with knowledge. Whereas exposure to obstetrical ultrasound in current pregnancy (adjusted odds ratio: 2.726; 95% confidence interval: 1.632–3.629), knowledge on obstetrical ultrasound (adjusted odds ratio: 3.92; 95% confidence interval: 1.324–3.120), and educational status (adjusted odds ratio: 2.84; 95% confidence interval: 1.337–3.381) were significantly associated with attitude.
Conclusion:
The level of good knowledge and positive attitude toward obstetric ultrasound was 35.5% and 69.5%, respectively, and it can be improved with appropriate interventions like ensuring the practice of obstetric ultrasound scan to all antenatal women. Obstetric care providers at the antenatal care units should advice pregnant women for obstetric ultrasound scan as per World Health Organization recommendations of one obstetric ultrasound scan before 24 weeks of gestation.
Introduction
Obstetric ultrasound is a harmless, cheap, and noninvasive imaging modality that helps to scan a pregnant mother’s abdominal and pelvic cavity with high-frequency sound waves and delivers parents with a real-time image of the fetus.1,2
The use of ultrasound in obstetrics is critical because it allows us to explore and detect various disorders even in the early stages of pregnancy, improve the quality of antenatal care (ANC) and pregnancy outcomes and treatment of disease in the current era of evidence-based medicine and as the number of pregnancies rises globally, the demand for obstetric ultrasound becomes even more pressing.3–12
World Health Organization (WHO) 2 recommends that all pregnant women have one ultrasound scan before 24 weeks of pregnancy to estimate gestational age (GA), assess placental placement, determine single or multiple pregnancies, increase fetal abnormality detection, and improve pregnancy outcomes in addition to ultrasound scans when indicated. Furthermore it can improve the accuracy and precision of GA measurement, making it easier to treat suspected preterm delivery and post-term pregnancies, particularly in low-income settings.13,14
Pregnant women in developing countries are more likely to have complications during pregnancy and die, and their newborns are more likely to have complications during birth or shortly after delivery; however, many of the problems may be avoided with adequate prenatal care involving ultrasound scan, which is one of the most significant components of prenatal care.2,15,16
Sub-Saharan Africa (SSA) has one of the highest levels of perinatal mortality globally, where the estimated perinatal mortality was 34.7 per 1000 births. 17 Intrauterine growth retardation (IUGR) is a major cause of perinatal mortality and morbidity, and ultrasound may be useful in identifying expectant mothers who are at early risk. For example, research in Africa (Egypt, Cairo) discovered a rate of infant growth retardation of 11.8%. Approximately 89.7% of these were detected via an obstetric ultrasound scan. 18
It has been demonstrated that women’s understanding and attitude about antenatal ultrasonography are critical, and that it has an impact on their mental health. This is especially true in cases where ultrasonography is being used newly. Despite this, several studies show that women have little awareness of prenatal sonography and have unreasonable expectations and demands.1,19
In Nigeria, majority of participants (96.4%) had good knowledge toward ultrasound scan and nearly one-third (31.3%) believed that too many ultrasonography procedures were harmful to the baby, while the remaining 13.8% believed it could lead to cancer. 20 According to previous studies conducted in Uganda, educational level and source of information about obstetric ultrasound were some of the major factors associated with knowledge of obstetric ultrasound. 9
Knowledge, attitudes and factors related to obstetric ultrasound among women in Africa, particularly in SSA, have not been fully addressed. In addition to this, previous researches were largely relied on a single-center strategy. This study, on the contrary, took advantage of multicenter research by allowing individuals from various contexts, including women from rural communities, to participate. 21
Since the level of knowledge and status of attitude of women about prenatal procedures affects their decision to undergo an obstetric ultrasound test, and the limited understanding of some women may result in rejection of prenatal screening and diagnoses, assessing their knowledge and attitude toward obstetric ultrasound is vital. 22 There were no studies conducted related to pregnant women’s knowledge and attitude toward obstetric ultrasound in Ethiopia. Therefore, this study aimed to assess pregnant women’s knowledge, attitude, and associated factors toward obstetric ultrasound in public hospitals in Ethiopia.
Methods
Study area, design, and period
Institution-based cross-sectional study was conducted from 10 April 2021 through 2 June 2021 at all four public hospitals in Gedeo Zone, Ethiopia. Gedeo zone is located 360 km south of Addis Ababa, Ethiopia’s capital city, with the administrative center in Dilla town. There are six districts and two town cities, 164 kebeles (31 urban and 133 rural), one referral hospital, three district hospitals, and 38 health centers.
Source population
All pregnant women who were attending ANC in Gedeo Zone public hospitals.
Study population
All selected pregnant women who were attending ANC in Gedeo Zone public hospitals during data collection.
Inclusion criteria
All pregnant women who were attending ANC and who have been living for at least 6 months in Gedeo zone were included in our study.
Exclusion criteria
Pregnant women who are critically ill and unable to communicate at the time of data collection.
Sample size determination
The sample size was determined by using a single population proportion formula, n = (z (α/2)) 2 p (1−p)/d 2 , taking 0.05 margin of error at 95% confidence level. Since no study was conducted yet in Ethiopia, considering the fact that the proportion was closer to 50%, the largest sample size was used. For a possible nonresponse rate, 10% of the total sample size was considered and made a final sample size of 422 (Re-revised).
Sampling technique
The sample was allocated proportionally to four hospitals—one referral hospital and three primary hospitals—and collected with a systematic random sampling technique. The previous month’s performance report of the health institutions before the study period was taken as a reference to estimate the client load (ANC load) in each hospital. Accordingly, there were 875 pregnant women in Dilla referral hospital, 560 pregnant women in Yirgachefe hospital, 540 pregnant women in Gedeb hospital, and 500 pregnant women in Bule hospital. There were a total of 2475 pregnant women in those public health facilities. Based on the information, a proportion of the sample for each institution under study was allocated. Therefore, 149 of the sample size was allocated to Dilla referral hospital, 96 allocated to Yirgachefe primary hospital, 92 allocated to Gedeb primary hospital, and 85 allocated to Bule primary hospital. A systematic random sampling technique was used, and every sixth pregnant mother was selected for an exit interview. The first study participant was determined randomly.
Study variables
Dependent variable
Knowledge and attitude of pregnant women toward obstetric ultrasound.
Independent variables
Socio demographics: age, marital status, religion, educational background, occupation, ethnicity, residence, family income, and household size.
Obstetrical and maternal characteristics: gravidity, parity, current obstetric scan exposure, bad obstetric history, number of ANC visits, time of initiation of ANC, source of information regarding ultrasound scan, distance from health facilities.
Operational definitions
Knowledge toward obstetric ultrasound: twelve knowledge-determining statements or items were administered to participants and the mean was calculated. The overall knowledge status was categorized as having good knowledge when the participant scored above or equal to the mean (6.4) and having poor knowledge when the participant scored below the mean (6.4) of the knowledge determining items.
Attitude toward obstetric ultrasound: The attitude score (AS) was also a summative score derived from Likert-type scale responses. Participants’ responses to each of the attitude questions could range from “strongly agree,” “agree,” “neither agree nor disagree,” “disagree,” or “strongly disagree.” Finally, they dichotomized into positive and negative attitudes by merging neutral, disagree, and strongly disagree into a negative attitude and agree and strongly agree into a positive attitude. The overall attitude was determined by the mean of all 11 attitude-related questions. Participants who scored above or equal to the mean value of 7.8 were determined to have a positive attitude, while those who scored below the mean (7.8) were determined to have a negative attitude toward obstetric ultrasound.
Data collection methods
Data collection tool was adopted from a previous study conducted in Jeddah 6 and contextualized to the study setting that was prepared in English, translated to Amharic and Gedeo offa languages, then back-translated to English by an independent translator for its consistency. The questionaries have four main items (socio-demographic characteristics), obstetrical and maternal health service characteristics, knowledge, and attitude assessment questions. Pre-test was done on 5% of the total participants (42 pregnant women) in Yirgachefe hospital near to the study area. During the pretest, the questionnaire was assessed for its clarity, readability, comprehensiveness, accuracy, and optimal time for completing the interview. Modifications and corrections were performed based on the results of the pretest.
The data were collected by using face-to-face interview with a pretested structured questionnaire among pregnant women at ANC clinics and it was lasted within 20 to 30 min. Data were collected by eight data collectors and four supervisors who had BSc in midwifery. Three days training was given for data collectors and supervisors on the overall procedure of the study.
Internal consistency/reliability of the item was checked by computing Cronbach’s alpha. The value of Cronbach’s alpha for knowledge assessment was 0.86 and attitude was 0.84.
Data analysis
Data were checked for completeness, edited, and coded. The data were entered by using Epidemiological data version (EPIDATA) 3.1 software and then exported to Statistical Package for Social Science (SPSS) version 23.0 statistical software for analysis. Descriptive statistics such as mean, median, frequency, and percentage were used. Binary logistic regression analysis was used to identify candidate variables for multivariable logistic regression. And variables with p-value less than 0.25 was regressed to multivariable logistic regression analysis. Multivariable analysis was employed to identify an independent determinant factor among explanatory variables. Adjusted odds ratio (AOR), 95% confidence interval (CI), and p-value less than or equal to 0.05 was used to decide a statistically significant association with the outcome variable. Model fitness test was checked by Hosmer and Lemeshow test. Multicollinearity was checked by using variance inflation factor (VIF) and tolerance test. Finally, the results were presented in the form of texts, tables, and graphs.
Data quality
Pre-test was done in Yirgachefe Hospital, which is outside of the study area with 5% of the total sample size. Based on the results of pretest, the necessary amendment was done on data collection tools. Three days training was given for the data collectors and supervisors on the general aims of the research, content of the questionnaire, and how to conduct the interview to increase their performance in the activities. The interviews were conducted at ANC services after they received all services. The collected data were checked every day by the supervisor and principal investigators for its completeness and consistency. All questionnaires were kept under lock and key for security and confidentiality of the obtained information.
Results
Socio-demographic characteristics of respondents
A total of 419 pregnant women took part in the study for a response rate of 99.3%. The majority, 179 (42.8%), of the study participants were under the age of 25 or less. The majority of mothers, 180 (43.0%), were protestant in religion. The majority (325 or 77.6%) were married, and 178 (42.2%) had completed secondary school. The details of the sociodemographic characteristics of the respondents were presented in Table 1.
Socio-demographic characteristics of pregnant women mothers in Gedeo Zone public hospitals, Ethiopia, 2021.

Obstetrics and maternal health service characteristics
From a total of 419 pregnant women, 173 (41.3%) were gravida 3–5. Majority (302, or 60.6%) of the respondents were multiparous, while the remaining 117 (27.9%) were primiparous. Majority, 192 (45.8%), of pregnant women had at least one bad obstetrical history in their lifetime. The details of obstetrics and maternal health service characteristics were presented in Table 2.
Obstetrical and maternal health service characteristics among pregnant women and mothers in Gedeo Zone public hospitals, Ethiopia, 2021.
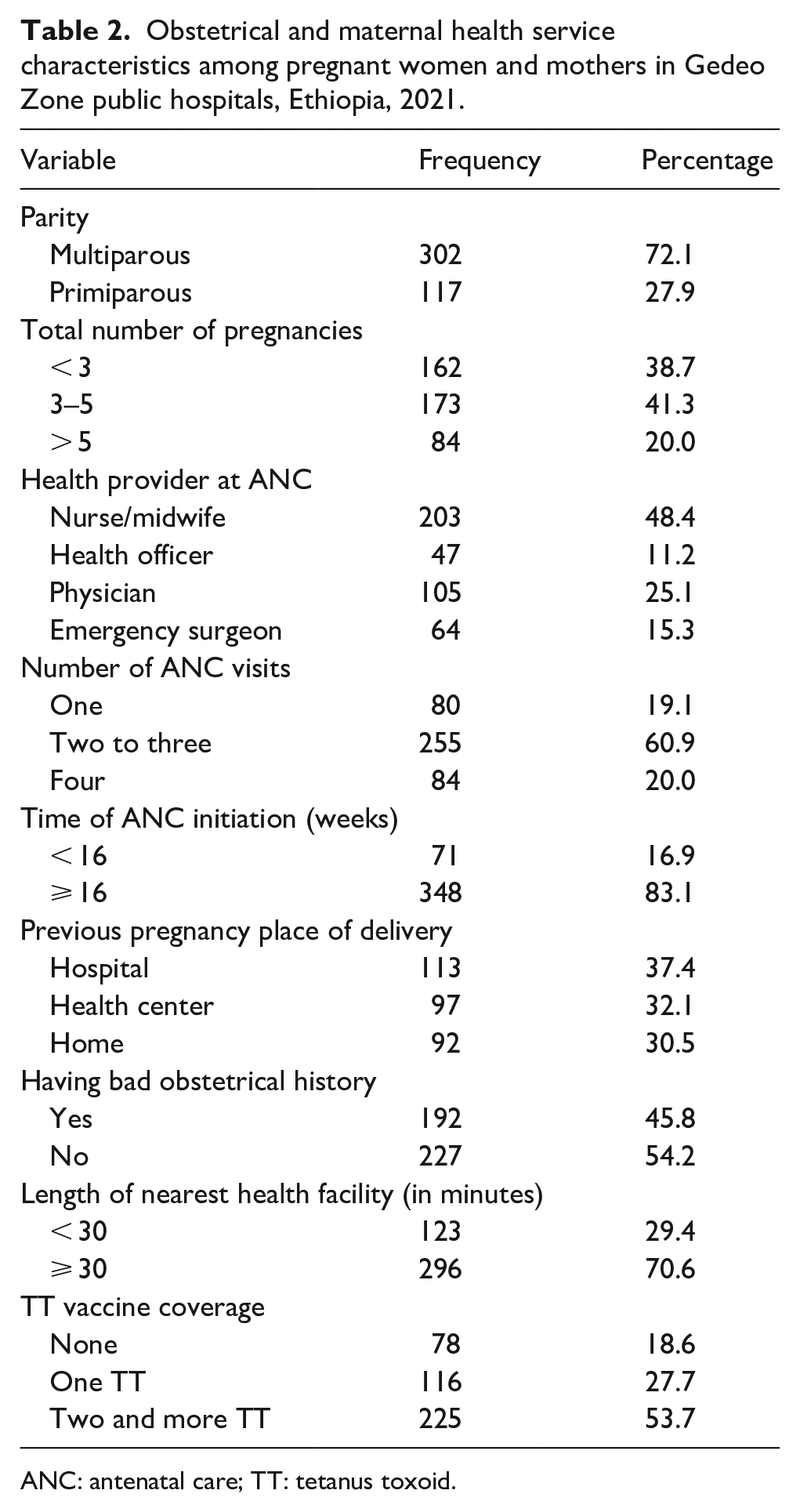
ANC: antenatal care; TT: tetanus toxoid.
Information and exposure of pregnant women toward obstetrical ultrasound
Out of 419 pregnant women, all (100%) of the women have heard about obstetrical ultrasound. From this, the majority, 194 (46.3%) pregnant women were mentioned by their relatives as primary sources of information about obstetrical ultrasound, followed by 124 (29.6%) who were heard at their ANC follow-up from healthcare providers, 58 (13.8%) were heard from social media, and the rest 43 (10.3%) pregnant women were heard from health extension workers. In terms of having been exposed to obstetrical ultrasound scanning during pregnancy, approximately 347 (82.8%) pregnant women had at least one exposure to obstetrical ultrasound scanning during their pregnancy. However, only 266 (63.5%) pregnant women had an obstetrical ultrasound scan during their current pregnancy. Among those, the majority (108 or 40.6%) were going to scan at the request of healthcare providers, followed by 101 (38%) at their own request, and the remaining 57 (21.4%) women were going to scan at the request of their husbands and families.
Moreover, from the total of 347 (82.2%) pregnant women who had exposure to obstetrical ultrasound scan at least once throughout their pregnancy, majority (219 or 63.1%) mentioned determination of fetus sex as a reason to go for ultrasound scan, followed by 62 (17.9%) to check the presentation of the fetus, 43 (12.4%) to assess the well-being of the fetus, and the rest 23 (6.6%) could not remember the exact reason to go for ultrasound scan.
Knowledge of pregnant women on obstetrical ultrasound
The most reported component of knowledge by participants was to determine the sex of the baby, with about 376 (89.7%) mothers reporting it. To confirm pregnancy was the second most reported importance of ultrasound, in which 332 (79.2%) women stated it. Detecting any defect or congenital abnormalities during pregnancy was the least reported component of knowledge regarding obstetric ultrasound, with only 73 (17.4%) women reporting having had it (as seen in Table 3).
Knowledge component on obstetrical ultrasound of pregnant women at Governmental Health Facilities in Gedeo Zone, Ethiopia, 2021.

In this study, out of 419 pregnant women, only 148 (35.3%) respondents had good knowledge of obstetrical ultrasound, while the rest (271, 64.7%) had poor knowledge of obstetrical ultrasound. This indicates the majority of women were not knowledgeable about the actual importance and effect of obstetric ultrasound. This, in turn, may lead to low utilization of obstetric ultrasound or hinder a woman from being examined by obstetric ultrasound even in an emergency, despite the fact that obstetric ultrasound scans improve pregnancy outcome (as seen in Figure 1).
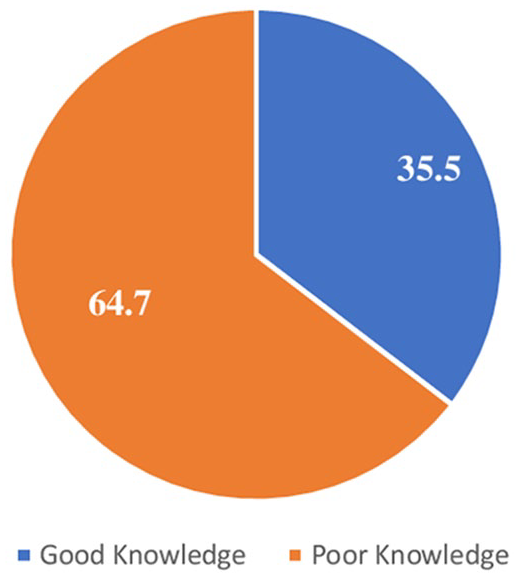
Overall knowledge of pregnant women on obstetrical ultrasound at public hospitals in Gedeo Zone, Ethiopia, 2021.
Attitude of pregnant women to obstetrical ultrasound
The most frequently mentioned component of attitude regarding obstetric ultrasound was “prefer to know the sex of your child,” where 354 (84.5%) women prefer ultrasound to determine the sex of the fetus. The second most stated component of attitude toward obstetric ultrasound was “safety of ultrasound for mothers,” where 345 (82.24%) women believed that obstetric ultrasound was safe for women. The vast majority (320 or 76.4%) of women reported feeling at ease during the obstetric ultrasound scan as seen in Table 4.
Attitude of pregnant women to obstetrical ultrasound at public hospitals in Gedeo Zone, Ethiopia, 2021.

Out of 419 pregnant women, majority (69.5%) had a positive attitude toward obstetrical ultrasound, while the remaining 128 (30.5%) respondents had a negative attitude toward obstetrical ultrasound. This indicates nearly one-third of women had a negative attitude toward obstetric ultrasound scans. And then, a negative attitude toward an ultrasound may mean that she will not be willing to be scanned by obstetric ultrasound, which may have a negative impact on the outcome of pregnancy both for the baby and the mother (as seen in Figure 2).

Attitude of pregnant women to obstetrical ultrasound at public hospitals in Gedeo Zone, Ethiopia, 2021.
Factors associated with knowledge of pregnant women on obstetrical ultrasound
In the bivariate logistic regression analysis, age of pregnant women, educational status, parity, exposure to obstetrical ultrasound, bad obstetrical history, occupational status, number of ANC visits, time of ANC initiation, residence, and monthly income were eligible variables for multivariable analyses. However, in multivariable logistic regression analysis, residence (AOR: 3.9; 95% CI: 3.125–6.761), educational status (AOR: 3.61; 95% CI: 1.986–5.964), and parity (AOR: 2.76; 95% CI: 1.68–3.275) were significantly associated with knowledge of pregnant women on obstetrical ultrasound (as shown in Table 5).
Bivariate and multivariable analysis on factors associated with knowledge of pregnant women on obstetrical ultrasound in Gedeo Zone public hospitals, Ethiopia, 2021.

COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
p < 0.01.
p < 0.05.
p > 0.05.
Factors associated with the attitude of pregnant women to obstetrical ultrasound
In bivariate logistic regression analysis, age of pregnant women, educational status, parity, exposure of obstetrical ultrasound in current pregnancy, having bad obstetrical history, number of ANC visits, time of ANC initiation, residence, and monthly income were eligible variables for multivariable analyses. However, in multivariable logistic regression analysis, exposure to obstetrical ultrasound in current pregnancy (AOR: 2.726; 95% CI: 1.632–3.629), knowledge on obstetrical ultrasound (AOR: 3.92; 95% CI: 1.324–3.120), and educational status (AOR: 2.84; 95% CI: 1.337–3.381) were significantly associated with attitude of pregnant women to obstetrical ultrasound as shown in Table 6.
Bivariate and multivariable analysis on factors associated with attitude of pregnant women to obstetrical ultrasound in Gedeo Zone public hospitals, Ethiopia, 2021.

COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
p < 0.01.
p < 0.05.
p > 0.05.
Discussion
In this study, only 148 (35.3%) of the respondents had good knowledge on obstetrical ultrasound. Residence, educational status, and parity were significantly associated with knowledge of pregnant women on obstetrical ultrasound. Majority, 291 (69.5%), of the participants in this study had a positive attitude toward obstetrical ultrasound. Exposure to obstetrical ultrasound, knowledge on obstetrical ultrasound, and educational status were significantly associated with attitude of pregnant women to obstetrical ultrasound.
Strengths and limitations of the study
Strength of the study
This research addressed women in different settings in urban and rural areas by incorporating all hospitals in the study area; and being the first national research, this is the strength of this research.
Limitations of the study
The literature related to pregnant women’s knowledge and attitude toward obstetric ultrasound is limited to discuss and hence is the limitation of the study.
Magnitude of knowledge
Only 35.5% women had good knowledge regarding ultrasonography scanning in this study. This may lead to reduced seek of ultrasound scan or utilization (helps in early identification and management of obstetric problems) in case of danger during pregnancy as knowledge toward ultrasound is one of the common factors that affect the utilization of obstetric scans. 23 This is lower than the previous study conducted in India and Jeddah.6,24 This may be due to the fact that in this study, most of the hospitals are primary and located in a district and most of the pregnant women have had no previous obstetric scan, so they become new to the experience. In addition to this, in our findings, most of the pregnant women perceive the use of obstetric ultrasound for sex determination only, which results in low scan experiences that help them know about other uses of obstetric ultrasound despite the fact that obstetric ultrasound is helpful in routine clinical management supported by the result part of our research. This study is also lower than the study done in Nigeria, Africa 20 in which the mean knowledge score was 86.3%. This might be due to the socioeconomic and cultural background of the pregnant women toward obstetric ultrasound use and educational background of the participants. Our finding is also lower than the study conducted in Sudan in which the majority of participants have fairly good knowledge. 25 It might be due to the sample size, tool discrepancy( parameters used), and the setting of the study; in the study of Sudan, a teaching hospital that is located in a capital city serves mainly for urban women who have more source of information regarding obstetric ultrasound than rural women and where much better obstetric care and advanced sonographic examinations are being performed than ours where advanced obstetric scans are relatively low and serve for rural population with little source of information about obstetric ultrasound scan. This study is slightly lower than the finding in Turkey where more than half of pregnant women had a moderately sufficient level of knowledge. 14
The current finding is in line with the study conducted in southern India, Bengaluru, where only 30%–40% pregnant women had knowledge toward some of the ultrasound scanning importance. 1
Majority of the women in this study, stated importance of obstetric ultrasound is about fetal sex determination where more than 76.1% of pregnant women knew about it. Similar findings in Mumbai, India, where 73.5% knew about sex determination by obstetric ultrasound. 26 The finding is also supported by a previous study in Uganda, in which more than 65% of pregnant women stated that the importance of obstetric ultrasound is to determine the sex of the baby. 27
The least identified obstetric ultrasound knowledge in this study is knowledge regarding the determination of a congenital anomaly, in which only 17.4% of pregnant women stated that an ultrasound scan is helpful in identifying congenital abnormalities. The finding is much lower than the study conducted in Uganda 27 and Jeddah. 6 This might be due to most of our participants’ having no previous obstetric ultrasound scan experience and the low incidence of bad obstetric history among pregnant women, who might miss the wider importance of the ultrasound scan. Majority of our participants lacked higher education, and the difficulty of understanding congenital abnormalities and uterine abnormalities may also contribute to this problem. The setting of the study may also explain the discrepancy.
In this study, more than 30% of women believe that ultrasound should be done routinely for all women. The finding is lower than the study conducted in Nigeria, where about 73.1% of pregnant women believe that an ultrasound scan should be done routinely for every pregnant woman. 28 The discrepancy may be explained by the study setting and sociodemographic characteristics of the study participants. It may also be due to the previous study limiting the setting to only tertiary institutions where mostly urban women were served, as opposed to our study participants, recruited from different hospitals, including districts and hospitals serving both urban and rural women.
Magnitude of attitude
This study revealed that 69.5% of pregnant women have a positive attitude toward the use of obstetric ultrasound. This finding is in line with the study conducted in Nigeria in which 73.1% of antenatal women believed that the ultrasound should be done for every pregnant woman. 28
This study is higher than the study conducted in Iran where the majority of pregnant women had a negative attitude. 29
This study is lower than the findings in Jeddah and India, where 78.9% and 88%, respectively, believed in the safety of obstetric ultrasonography during pregnancy. This may be explained by methodological variations (parameters measured), time of study, and socioeconomic differences. The finding is also lower than the study done among pregnant women in Kano, Nigeria, where majority (93.8%) of participants understood the necessity of obstetric ultrasound for pregnant women.6,19,30
In this study, majority of women believed that obstetric ultrasound is safe for women. Similar findings from Tanzania and India supported the present finding.19,31
This study revealed that 16.6% of pregnant women believe that obstetric ultrasonography can lead to congenital anomalies, which is higher than the finding in Jeddah 6 where only 5.5% of mothers believe that obstetric ultrasound leads to congenital anomalies. The difference may be due to the sociocultural background and the educational status of the respondents. Lower than the finding in Iran and Uganda where 53.3% and 78% of pregnant women, respectively, believed that ultrasound scanning is harmful for the baby.27,32 This might be due to the time of research conducted and the sociocultural background of the study participants.
Regarding the sex determination of the unborn child, 83.5% of women stated that they would prefer to know the sex of their fetus, which is in line with the study done in Nigeria where more than 79% of participants wanted to know the sex of their fetus. 33 This finding is higher than the study conducted in Bikaner, India and Mumbai, India, in which 62% and 59.4% of pregnant women stated “NO” for gender preference, respectively. This variation might be due to the time, setting of the study, and sociocultural background of the participants.26,34
In our findings, more than 83% of pregnant women felt comfortable during obstetric ultrasound examination. This indicates that majority of pregnant women received friendly care and their privacy was not violated during the procedure as it is one of the elements of respectful maternity care. This is in line with the study conducted in India where only 24% of pregnant women were uncomfortable during the obstetric ultrasound procedures. 19 It is higher than the study in Uganda where only 48% of pregnant women felt comfortable during obstetric ultrasound examination. 27 The variation may be due to the previous repeated exposure status for ultrasound and the normalization of the discomfort as part of the scan.
Factors associated with knowledge toward obstetric ultrasound
Pregnant women’s educational status is significantly associated with good knowledge where women with above secondary education are more likely to have good knowledge than below secondary level of education. Similar findings were obtained with the study conducted in Turkey, Jeddah, and Iran.6,14,35 This may be explained by the fact that as the educational status of the pregnant women increases, exposure to information may also increase. And discussing about this issue is also more common among above secondary school pregnant women as they are more empowered to ask and decide than below secondary school pregnant women.
Being multiparous women is positively associated with good knowledge about obstetric ultrasound. Multiparous women are more likely to have good knowledge than primigravida women. The study in Turkey and Jeddah has the same finding where multiparous women were more knowledgeable about obstetric ultrasound than nulliparous women.6,14 This may be explained by the experience of women having more children in which as a woman gets more children, the obstetric ultrasound exposure scan also increases and they do have more awareness regarding the knowledge of the ultrasound scan. It may also be due to the frequency of contact of multiparous women with medical personnel. The study conducted among pregnant women in India, Mumbai, had a finding similar to ours. 26
Place of residency is associated with good knowledge toward obstetric ultrasound where urban pregnant women have good knowledge toward obstetric ultrasound than rural pregnant women. This indicates rural women are more vulnerable to the violation of reproductive rights as they do have less decision-making ability on obstetric procedures (obstetric ultrasound scan) than urban pregnant women. This is probably due to multiple sources of information about obstetric ultrasound such as TV programs, private clinics, and so on for urban women than rural pregnant women; similar findings with the study conducted in Turkey. 14
Factors associated with attitude
In our study, the level of education influences the attitude of pregnant women toward obstetric ultrasound scan. The finding is similar with the study conducted in Nigeria. 28 This may be due to the fact that as the level of education increases, it helps them to analyze or obtain information regarding understanding about obstetric ultrasound.
Pregnant women having good obstetric ultrasound knowledge have a positive attitude to obstetric ultrasound scans. This indicates that as the knowledge of pregnant women toward obstetric ultrasound increases, more women are going to use obstetric ultrasound and that results in early prevention and management of obstetric problems and the long-term effect will be reduction of prenatal mortality. This might be explained as knowledge toward ultrasound increases, belief regarding the ability of obstetric ultrasound to estimate the outcome of pregnancy and help divert the negative outcomes also increases.
In this study, pregnant women with a current obstetric ultrasound scan are more likely to have a positive attitude than women with no previous experience of ultrasound scan. This might be because they already understand the facts about the procedures either from the healthcare providers or from the result of ultrasound examinations and this might help them to believe the positive impact of obstetric ultrasound.
Having poor knowledge about obstetric ultrasound and a negative attitude toward the procedure affects their decision to undergo an obstetric ultrasound test and may result in rejection of prenatal screening and diagnosis. This, in turn, may lead to low utilization of obstetric ultrasound. Obstetric ultrasound has come to play a significant role in obstetrics since its introduction in clinical care and there is no doubt that the advantages of obstetric ultrasound technique have led to improvements in pregnancy outcomes.22,36
Therefore, ensuring that all antenatal women receive obstetric ultrasound scans will be helpful to prevent and manage obstetric complications and have a better pregnancy outcome, as recommended by WHO. Obstetric care providers should provide proper obstetric care, which includes regular obstetric ultrasound scans, and raise awareness about the positive effect of ultrasound scans on pregnancy outcomes for all antenatal women by giving special attention to rural women and pregnant mothers without ultrasound scans to address their poor knowledge and attitude toward ultrasound scans. Furthermore, a periodic campaign targeting rural pregnant women with a full package of maternity care focusing on the positive outcome of obstetric ultrasound for every pregnancy should be implemented.
Conclusion
In this study, pregnant women’s knowledge of obstetrical ultrasound scanning was (35.3%). The importance of ultrasound for sex determination is commonly reported by respondents, which is 76.1%. Knowledge of obstetric ultrasound is significantly associated with educational status of the pregnant women, parity, and residency.
Majority (69.5%) of pregnant women had a positive attitude toward the use of obstetric ultrasound. Whereas Pregnant women’s attitudes toward obstetric ultrasound are significantly associated to their educational status, knowledge of obstetric ultrasound, and current exposure to obstetric ultrasound.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221091357 – Supplemental material for Pregnant women’s knowledge, attitude, and associated factors toward obstetric ultrasound in public hospitals, Ethiopia, 2021: Multi-centered cross-sectional study
Supplemental material, sj-docx-1-whe-10.1177_17455057221091357 for Pregnant women’s knowledge, attitude, and associated factors toward obstetric ultrasound in public hospitals, Ethiopia, 2021: Multi-centered cross-sectional study by Wondwosen Molla, Nebiyu Mengistu and Aregahegn Wudneh in Women’s Health
Footnotes
Acknowledgements
We are thankful to the study participants for giving their fruitful time to participate in this study and for their unlimited support throughout the data collection process.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent
Ethical approval and clearance were obtained from Dilla University, College of Medicine & Health Science Institutional Review Board with the unique ethical approval number of DU/IRB/0921. Permission was also obtained from the concerned bodies of Gedeo Zone public hospital. Prior to data collection, written informed consent was obtained from each study participant. Confidentiality of the information was assured and privacy of the respondents were maintained.
Availability of data and materials
All data included in this manuscript can be accessed from the corresponding author upon request through the email address.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.