
Abstract
Background:
Anaemia disproportionately affects women of reproductive age in sub-Saharan Africa including Nigeria. Yet, community-based studies on the prevalence and determinants of anaemia among women of reproductive age are scarce in Nigeria.
Design:
A cross-sectional community-based survey using a nationally representative sample.
Objectives:
This study described anaemia prevalence and its associated factors among women of reproductive age, pregnant women, and non-pregnant women in Nigeria.
Methods:
We analysed data from the 2018 Nigeria Demographic and Health Survey. Pregnant women with a haemoglobin level less than 11 g/dL and non-pregnant women with a haemoglobin level less than 12 g/dL were considered anaemic. Anaemia was also categorized as mild, moderate, and severe. Pearson’s chi-square test was used to evaluate the association between anaemia status and independent variables. All variables with ρ ⩽ 0.25 in bivariate analyses were further analysed using complex sample logistic regression.
Results:
Anaemia prevalence was 57.8%, 57.4%, and 61.1% for women of reproductive age, non-pregnant women, and pregnant women, respectively. The prevalence of severe anaemia was 1.6%, 1.5%, and 2.3% for overall women of reproductive age, non-pregnant women, and pregnant women, correspondingly. The southern regions, rural residence, low education, unemployment, low wealth index, and non-use of modern contraceptives significantly increased the likelihood of anaemia and severe anaemia among women of reproductive age and non-pregnant women. The likelihood of being anaemic was significantly increased by large family size among women of reproductive age and by being underweight among non-pregnant women. The South-East region, rural residence, low education, and unemployment were significantly associated with anaemia among pregnant women. The South-South region and unemployment increased the likelihood of severe anaemia among pregnant women. Short stature significantly reduced the odds of being anaemic and severely anaemic among pregnant women.
Conclusions:
Anaemia prevalence among all categories of women of reproductive age is high in Nigeria. Predictors of anaemia prevalence and severity should be considered in policies intended to reduce anaemia among women of reproductive age in Nigeria.
Keywords
Introduction
Anaemia is a condition in which the number of healthy red blood cells is decreased, and haemoglobin (Hb), the primary oxygen-carrying molecule in red blood cells, is insufficient to meet the body’s physiological needs for oxygen delivery to vital tissues. 1 Anaemia is highly prevalent in low- and middle-income countries (LMICs) and disproportionately affects women of reproductive age (WRA), especially in sub-Saharan Africa.2,3 In Nigeria, anaemia prevalence among pregnant and non-pregnant women is high.4,5 Nigeria has also a high prevalence of micronutrient deficiencies. 6 Despite policies and programmes to reduce the anaemia burden among WRA in LMICs, the decrease in anaemia prevalence has been marginal. 2 Only three LMICs, excluding Nigeria, have a high probability of achieving the global nutritional target of a 50% reduction of anaemia prevalence by 2030. 3
The health and socio-economic impacts of anaemia are huge. Anaemia in pregnant WRA increases the risk of preterm birth, stillbirth, perinatal morbidity, low birth weight, and susceptibility to infection. 2 The risk of maternal death is twice as high in pregnant women with severe anaemia compared with those without severe anaemia. 7 Anaemia is a major direct and indirect cause of maternal mortality and is associated with high foetal wastage in Nigeria. 8 Anaemia among pregnant and non-pregnant WRA results in impaired cognitive functioning, academic and workplace underperformance, and loss of productivity from reduced work capacity.9,10 Loss of productivity from anaemia, in turn, results in personal income and substantial national economic losses. 9
Previous community-based studies from sub-Saharan Africa, which included pregnant and non-pregnant women, found three classes of risk factors for being anaemic. The first category, individual maternal risk factors, included current pregnancy status,11–16 increasing age,11,13 younger age,12,14 marital status,14,17,18 large household size, 17 female-headed households,14,19 underweight,11,17,18 high parity,12–14,19,20 ever had a terminated pregnancy, 14 non-use of modern contraceptives,12,14,17,18 currently breastfeeding,13,15 being HIV positive,13,15,16 and tobacco use. 17 Household and socio-economic risk factors are the second set of factors and included region or province of residence,4,17,18,20 rural residence,4,11,13,15,21 urban residence, 14 low education,4,12–14,16,19 low literacy, 17 being poor,4,11–14,16–19,21,22 unemployment,11,14,20 unimproved toilet facilities,13,14,17 unimproved water source,4,14,17 and non-use of mosquito bed nets.17,18 The third group of factors are health service–related factors comprising perceiving distance as a big problem, 14 low intake of iron-folic acid,15,19 home deliveries, 19 and malaria infection.16,22 Furthermore, non-use of modern contraceptive,23,24 rural residence, 24 being married, 24 increasing parity, 24 being poor, 24 unemployment, 24 poor malaria knowledge, 4 malaria infection, and living camp 22 were specific factors associated with being anaemic among non-pregnant women.
Few community-based studies in Africa specifically examined the risk factors among pregnant WRA.22,25–32 Among pregnant women, the individual risk factors were being unmarried, 33 monogamous families, and high parity.25,26 The household and socio-economic risk factors comprised being poor,25,26,31 low education,19,31 low dietary diversity, 26 unemployment, 27 rural residence,28,31,32 region of residence,30,31 and non-use of mosquito bed nets.28,29 The health service–related risk factors for being anaemic included low intake of iron-folic acid,19,25–27 pregnancy trimester,25,26,30 number of antenatal care,27,30 malaria infection,22,28,29 and worm infestation.26,28
Community-based, Nigerian studies investigating the determinants of anaemia among WRA are scarce. Three existing studies have methodological limitations. One study with a subnational pregnant women sample from one district in Northern Nigeria lacked a predictive model. 27 The two studies, using nationally representative data, did not account for the different risk factors for pregnant women and non-pregnant women.4,31 These studies also included a narrow set of risk factors for anaemia among the two categories of WRA.4,31 This article aims to update the evidence about the prevalence and determinants of anaemia and its severity among WRA, and pregnant and non-pregnant women in Nigeria using a logistic predictive model that includes a wider range of individual, household/socio-economic, and health service–related factors.
Methods
Study setting
Nigeria had an estimated population of 195,874,683
Study design
This study used a quantitative, cross-sectional design by analysing data from the Nigeria Demographic and Health Survey (NDHS) 2018.
Sampling strategy
The sampling frame consisted of households listed in Nigeria’s 2006 Population and Housing Census (NPHC). The primary sampling unit (PSU) consisted of a distinct group of enumeration areas (EAs) from the sampling frame referred to as a cluster. An EA is usually a clearly defined geographic area which groups several households together for population and housing census. A two-stage stratified sampling technique was used to select the households. Each of the 36 states and the Federal Capital Territory was stratified into urban and rural areas, creating 74 sampling strata. In the first stage, 1400 (580 urban and 820 rural) EAs were selected from the sampling strata with probability proportional to EA size. In the second stage selection, 30 households were selected from every cluster through equal probability systematic sampling, resulting in a total sample size of about 42,000 households (Figure 1). One-third of the total sample size of households (14,000) were selected for anaemia testing. Using an estimated proportion of WRA that are anaemic (P = 0.578), design effect (Deft = 1.434), relative standard error (α = 0.01), individual response rate (Ri = 97%), household gross response rate (Rh = 95%), and the number of eligible individuals per household (d = 1.032), 35 the sample size in terms of the number of households (n) was calculated using the formula 36


Flowchart for the sampling procedure.
Data collection
The survey was successfully carried out in 1389 clusters in 36 states and Federal Capital Territory comprising 747 LGAs from August to December 2018. Eleven clusters, with deteriorating law-and-order situations, were dropped during the fieldwork. To prevent bias, no replacements and no changes to the pre-selected households were allowed in the implementing stages. Anaemia testing was conducted for WRA in one-third of sampled households selected through equal probability systematic sampling from the total sample size of 42,000 households. The inclusion criteria were all WRA, either permanent residents or visitors who stayed in the sampled household the night before the survey. Women who did not agree to provide consent and women outside the age of 15–49 years were excluded. A blood sample from a finger prick site was drawn into a microcuvette, and a haemoglobin analysis was carried out on-site with a battery-operated portable HemoCue analyser (HemoCue Hb 301 system, Sweden).
Variables
Dependent variable
Anaemia status at the time of the survey is the dependent variable. Pregnant women with a haemoglobin level less than 11 g/dL and non-pregnant women with a haemoglobin level less than 12 g/dL were considered anaemic.35,37 Anaemia was categorized as mild (haemoglobin (Hb) of 10.0–10.9 g/dL for pregnant women and 11.0–11.9 g/dL for non-pregnant women), moderate (Hb of 7.0–9.9 g/dL for pregnant women and 8.0–10.9 g/dL for non-pregnant women), and severe (Hb < 7.0 g/dL for pregnant women and <8.0 g/dL for non-pregnant women). The anaemia status of respondents was also recoded into a binary variable as anaemia (mild, moderate, and severe) and no anaemia.
Haemoglobin levels were adjusted for cigarette smoking and for the altitude in EAs that are above 1000 metres. 38 The adjustment was made with the following formula: ‘adjust = –0.032 × alt + 0.022 × alt 2 ’ and ‘adjHb = Hb – adjust (for adjust > 0)’ where ‘adjust’ is the amount of the adjustment, ‘alt’ is the altitude in 1000 feet (converted from metres by dividing by 1000 and multiplying by 3.3), ‘adjHb’ is the adjusted haemoglobin level, and ‘Hb’ is the measured haemoglobin level in grammes per decilitre. Regarding smoking adjustment, no adjustment for women who smoked less than 10 sticks per day, while the haemoglobin of women who smoked 10–19, 20–39, and 40 or more sticks of cigarette per day were adjusted by –0.3, –0.5, and –0.7 g/dL, correspondingly.
Independent variables
The variables were grouped into individual maternal characteristics, socio-economic and household characteristics, and health service–related factors based on the conceptual framework for maternal anaemia determinants. 2 The individual characteristics included the age of the respondent, marital status (never in a union, married/living with a partner, and divorced/separated/widowed), family size (<5 and ⩾5), sex of household head (female and male), ever had a termination of pregnancy (yes and no), breastfeeding status (yes and no), body mass index (BMI) (underweight, normal, overweight, and obese), and modern contraceptive use (yes and no). The total children ever born (0, 1, 2–4, and ⩾5) were regrouped into four categories of parity (nulliparity, primiparity, multiparity, and grand multiparity), correspondingly. 39 BMI was converted from a numeric to a categorical variable based on the World Health Organization (WHO) BMI. 35 As BMI is not appropriate for pregnant women, we used stature (height) for all categories of WRA categorized as short stature (<145 cm) and normal (⩾145 cm). 35 The socio-economic and household characteristics included region (North-Central, North-East, North-West, South-East, South-South, and South-West), type of residence (urban and rural), highest education (no education, primary, secondary, and higher), employment (unemployed and employed), wealth index (poorest, poor, moderate, rich, richest), access to sanitation (unimproved and improved), the main source of drinking water (unimproved and improved), ownership of a mosquito bed net for sleeping (yes and no), respondent having slept under a mosquito bed net the night before the survey (yes and no), and media exposure (none and any form). Based on the consumption of 10 food groups in the 24 h preceding the survey, women were categorized into low (<5) and high diversity (⩾5) groups. 35 The health service–related factor is the extent to which respondents considered the distance to a health facility as a problem (not a problem, not a big problem).
Statistical analysis
Data were analysed using SPSS 20 (IBM Corp., Armonk, NY). We adjusted the data for sampling weights, stratification, and multistage sampling before analysis to account for the non-proportional allocation of the sample to the different states and provide representative population estimates. The basic characteristics of the respondents were presented using frequencies, population estimates, and percentages (weighted). Pearson’s chi-square test was used to evaluate the association between anaemia prevalence and independent variables. Multicollinearity was assessed using the variable inflation factor (VIF). The independent variables showed no multicollinearity (minimum VIF = 1.00, maximum VIF = 3.80). All variables with a p value ⩽ 0.25 in bivariate analyses were further analysed using multivariable complex samples logistic regression. In addition, we included age, stature, and parity in the model for pregnant women based on clinical significance. The results of regression analysis were presented by crude/unadjusted odds ratio (COR) and adjusted odds ratio (AOR) with 95% confidence intervals (CIs), F statistics, and p values. The McFadden test statistic for overall WRA, non-pregnant women, and pregnant women ranged from 0.02 to 0.04. Since values ranging from 0.2 to 0.4 indicate good model fit and values beyond 0.4 indicate excellent fit, our models might not be the best fit. 40 However, McFadden test, a log-likelihood-based pseudo-R 2 that represents the improvement in model likelihood over a null model, is influenced by sample size (the smaller the sample size, the higher the value), number of predictor variables, and number of categories of the dependent variable and its distribution asymmetry. 40 Statistical significance for the multivariable complex sample logistic regression analyses was set at p < 0.05.
Ethical consideration
The 2018 NDHS protocol was reviewed and approved by the National Health Research Ethics Committee of Nigeria (NHREC) and the ICF Institutional Review Board. Informed consent was obtained from participants before interviews or biomarker tests were conducted. Consequently, our study, being a secondary analysis, did not require further ethical approval.
Results
Characteristics of respondents
The proportion of non-pregnant women (NPW) and pregnant women (PW) included in the study were 89.4% and 10.6%, respectively. The basic characteristics of the respondents are shown in Table 1. About 53%, 52%, and 61% of WRA, NPW, and PW were from rural areas, respectively. Most WRA, NPW, and PW were married/living with a partner (72%, 69%, and 97%), and had a male head of household (83%, 82%, and 90%), correspondingly. About 66% of WRA and NPW each and 63% of PW were employed. Almost 11% of WRA and NPW each, and 8% of PW received higher education. Approximately 44% of WRA, 45% of NPW, and 38% of PW were rich. About 88% of WRA and 87% of NPW did not use modern contraceptives, while approximately 11% of WRA and 12% of NPW were underweight.
Basic characteristics of WRA in Nigeria, 2018.

WRA: women of reproductive age.
Prevalence of anaemia
Overall, about 57.8% (95% CI: 56.7–59.0) of WRA, 57.4% (95% CI: 56.7–58.7) of non-pregnant women, and 61.1% (95% CI: 57.9–64.2) of pregnant women were anaemic. Anaemia prevalence significantly differed with family size, sex of household head, parity, and current use of modern contraceptives among WRA. Among non-pregnant women, anaemia prevalence significantly varied with age, family size, sex of household head, parity, use of modern contraceptives, breastfeeding, and BMI (Table 2). Of all individual women characteristics, anaemia prevalence among pregnant women significantly differed with marital status only (Table 2).
Prevalence of anaemia among WRA in Nigeria disaggregated by maternal characteristics, 2018.
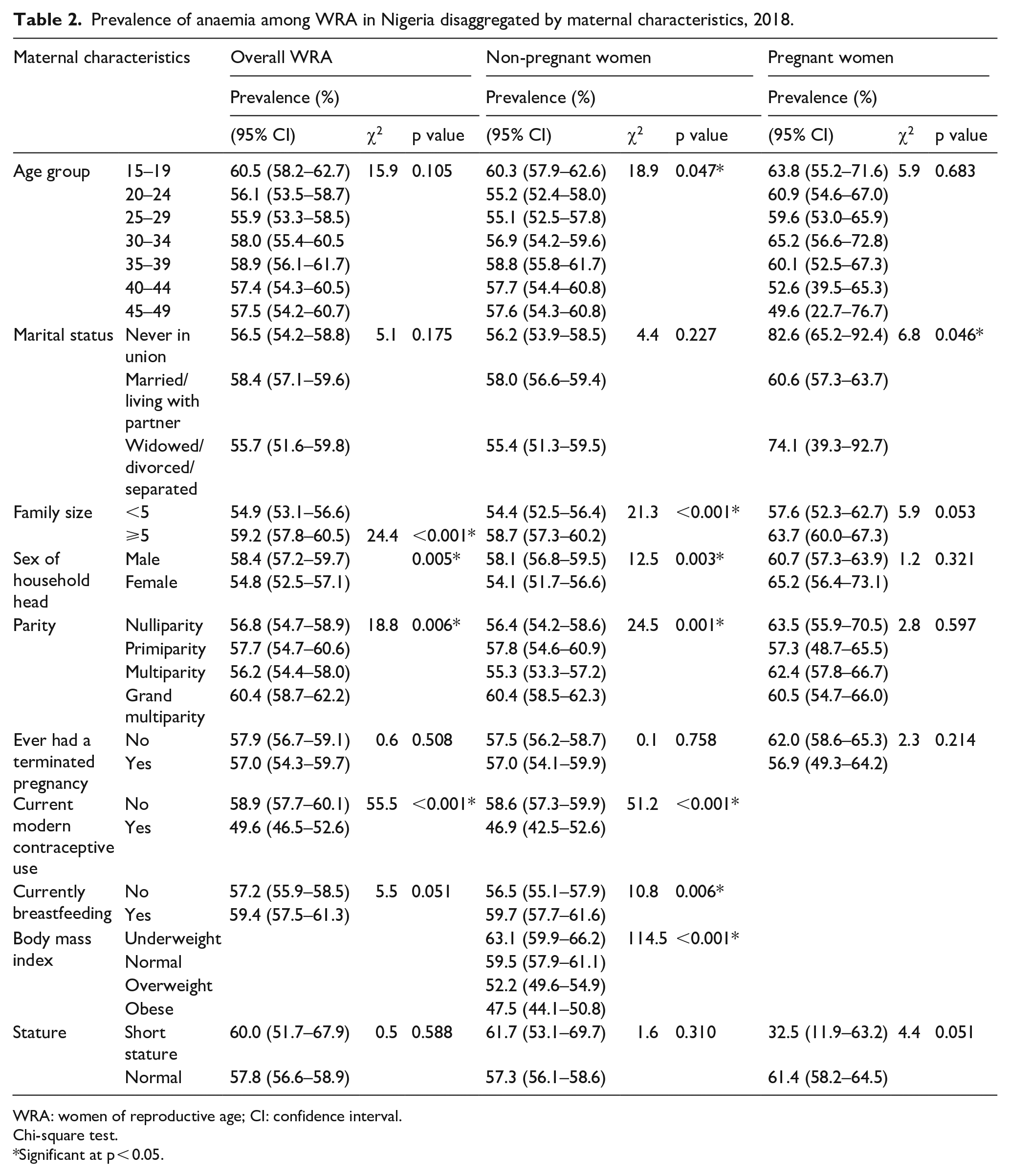
WRA: women of reproductive age; CI: confidence interval.
Chi-square test.
Significant at p < 0.05.
Apart from the type of water source, ownership of a mosquito bed net, and sleeping under a mosquito bed net, anaemia prevalence among overall WRA and NPW significantly differed by other socio-economic and household factors (Table 3). In addition, anaemia prevalence was significantly associated with the region, type of place of residence, education, and access to sanitation among pregnant women (Table 3). Whereas distance to health facility showed no significant association with anaemia prevalence among pregnant women, anaemia prevalence significantly differed by ‘distance to health facility’ among overall WRA and non-pregnant women (Table 3).
Prevalence of anaemia among WRA in Nigeria disaggregated by women’s socio-economic, household environmental, and health service factors, 2018.

WRA: women of reproductive age; CI: confidence interval.
Chi-square test.
Significant at p < 0.05.
Prevalence of severity of anaemia
The prevalence of mild, moderate, and severe anaemia among all WRA, non-pregnant women, and pregnant women are shown in Table 4. About 1.6%, 1.5%, and 2.3% WRA, NPW, and PW were severely anaemic, correspondingly. Apart from age, sex of household head, ever had a termination of pregnancy, stature, having bed net, slept under bed net, and water, all other variables were significantly associated with severity of anaemia among overall WRA. Similarly, ever had a terminated pregnancy, having bed net, slept under bed net, and water were not significantly associated with severity of anaemia among non-pregnant WRA. Regarding pregnant women, only marital status, region, place of residence, education, and employment showed significant association with anaemia severity.
Prevalence of severity of anaemia among women of reproductive age in Nigeria, 2018.

Chi-square test.
Significant at p < 0.05.
Determinants of anaemia among WRA
Family size (AOR = 1.13, 95% CI: 1.03–1.23, ρ = 0.007), non-use of modern contraceptive (AOR = 1.27, 95% CI: 1.11–1.44, ρ = 0.001), residing in the South-East (AOR = 1.67, 95% CI: 1.42–1.97, ρ < 0.001) or South-South region (AOR = 1.30, 95% CI: 1.09–1.55, ρ = 0.004), rural residence (AOR = 1.35, 95% CI: 1.21–1.50, ρ < 0.001), no education (AOR = 1.67, 95% CI: 1.39–2.13, ρ < 0.001), primary education (AOR = 1.31, 95% CI: 1.10–1.57, ρ = 0.003), secondary education (AOR = 1.18, 95% CI: 1.00–1.38, ρ = 0.044), unemployment (AOR = 1.20, 95% CI: 1.09–1.31, ρ = 0.002), poorest quintile (AOR = 1.55, 95% CI: 1.32–1.82, ρ < 0.001), poorer quintile (AOR = 1.23, 95% CI: 1.06–1.44, ρ = 0.007), middle quintile (AOR = 1.23, 95% CI: 1.06–1.42, ρ = 0.006) significantly increased the odds of being anaemic among overall WRA. In contrast, residing in North-Central (AOR = 0.85, 95% CI: 0.72–0.99, ρ = 0.037), North-East (AOR = 0.76, 95% CI: 0.64–0.90, ρ = 0.002), and North-West (AOR = 0.77, 95% CI: 0.65–0.91, ρ = 0.002) regions significantly reduced the likelihood of being anaemic among WRA (Table 5).
Risk factors for being anaemic among WRA in Nigeria, 2018.

WRA: women of reproductive age; OR: odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
Significance at p < 0.05.
Determinants of anaemia among non-pregnant women
Non-use of modern contraceptive (AOR = 1.20, 95% CI: 1.05–1.37, ρ = 0.006), underweight (AOR = 1.15, 95% CI: 0.99–1.34, ρ < 0.001), residing in the South-East (AOR = 1.76, 95% CI: 1.48–2.08, ρ < 0.001) or South-South region (AOR = 1.38, 95% CI: 1.15–1.66, ρ = 0.001), rural residence (AOR = 1.26, 95% CI: 1.13–1.41, ρ < 0.001), no education (AOR = 1.67, 95% CI: 1.37–2.03, ρ < 0.001), primary education (AOR = 1.25, 95% CI: 1.03–1.51, ρ = 0.023), unemployment (AOR = 1.14, 95% CI: 1.03–1.26, ρ = 0.013), poorest quintile (AOR = 1.43, 95% CI: 1.20–1.70, ρ < 0.001), middle quintile (AOR = 1.18, 95% CI: 1.01–1.37, ρ = 0.033), and richer quintile (AOR = 1.04, 95% CI: 0.91–1.20, ρ = 0.001) significantly increased the odds of being anaemic among overall WRA. In contrast, residing in North-Central (AOR = 0.82, 95% CI: 0.70–0.97, ρ = 0.019), North-East (AOR = 0.79, 95% CI: 0.66–0.95, ρ = 0.013), North-West (AOR = 0.78, 95% CI: 0.65–0.95, ρ = 0.011) regions and being overweight (AOR = 0.79, 95% CI: 0.70–0.90, ρ < 0.001) significantly reduced the likelihood of being anaemic among WRA (Table 5).
Determinants of anaemia among pregnant women
Short stature (AOR = 0.24, 95% CI: 0.07–0.88, ρ = 0.032) significantly reduced the likelihood of being anaemic among pregnant women (Table 5). Conversely, living in the South-East (AOR = 1.95, 95% CI: 1.03–3.68, ρ = 0.039) regions, rural residence (AOR = 1.43, 95% CI: 1.07–1.91, ρ = 0.015), no education (AOR = 2.97, 95% CI: 1.79–4.92, ρ < 0.001), primary education (AOR = 3.46, 95% CI: 1.97–6.07, ρ < 0.001), and secondary education (AOR = 1.81, 95% CI: 1.13–2.90, ρ = 0.014), and no employment (AOR = 1.38, 95% CI: 1.03–1.86, ρ = 0.031) increased the odds of being anaemic among pregnant women (Table 5).
Determinants of anaemia severity among WRA
As shown in Table 6, the likelihood of severe anaemia among overall WRA increased with contraceptive use (AOR = 2.19, 95% CI: 1.10–4.33, ρ = 0.025); residing in North-West (AOR = 2.13, 95% CI: 1.06–4.28, ρ = 0.033), South-East (AOR = 4.51, 95% CI: 2.33–8.74, ρ < 0.001), and South-South (AOR = 4.07, 95% CI: 1.97–8.38, ρ < 0.001); no education (AOR = 5.12, 95% CI: 2.26–11.59, ρ < 0.001); primary education (AOR = 3.13, 95% CI: 1.46–6.73, ρ = 0.003); and unemployment (AOR = 1.43, 95% CI: 1.01–2.04, ρ = 0.046). Rural residence (AOR = 1.39, 95% CI: 1.22–1.59, ρ < 0.001); poorest (AOR = 1.63, 95% CI: 0.35–0.97, ρ < 0.001), poorer (AOR = 1.29, 95% CI: 1.08–1.54, ρ = 0.005), and richer quintile (AOR = 1.31, 95% CI: 1.10–1.55, ρ = 0.002); and lack of access to media (AOR = 1.18, 95% CI: 1.06–1.30, ρ = 0.002) increased the likelihood of being moderately anaemic.
Risk factors for severity of anaemia among overall women of reproductive age in Nigeria, 2018.

Significance at p < 0.05.
Determinants of anaemia severity among non-pregnant women
As shown in Table 7, the likelihood of severe anaemia among non-pregnant increased with non-contraceptive use (AOR = 2.16, 95% CI: 1.08–4.34, ρ = 0.030); underweight (AOR = 2.38, 95% CI: 1.58–3.58, ρ < 0.001); residing in North-West (AOR = 2.51 95% CI: 1.16–5.41, ρ = 0.019); South-East (AOR = 5.10, 95% CI: 2.55–10.23, ρ < 0.001); South-South (AOR = 4.01, 95% CI: 1.87–8.59, ρ < 0.001); no education (AOR = 4.70, 95% CI: 1.88–11.72, ρ = 0.001); and primary education (AOR = 2.79, 95% CI: 1.18–6.61, ρ = 0.020). In contrast, the likelihood of severe anaemia among NPW is reduced by age 15–19 years (AOR = 0.42, 95% CI: 0.20–0.86, ρ = 0.018) and overweight (AOR = 0.50, 95% CI: 0.29–0.86, ρ = 0.006). Furthermore, the likelihood of moderate anaemia among non-pregnant women increased with age 35–39 years (AOR = 1.28, 95% CI: 1.03–1.60, ρ = 0.029); rural residence (AOR = 1.30, 95% CI: 1.12–1.50, ρ < 0.001); poorest (AOR = 1.47, 95% CI: 1.20–1.81, ρ < 0.001); middle quintile (AOR = 1.24, 95% CI: 1.04–1.48, ρ = 0.016), and lack of access to media (AOR = 1.20, 95% CI: 1.08–1.34, ρ = 0.001).
Risk factors for severity of anaemia among non-pregnant women in Nigeria, 2018.

Significance at p < 0.05.
Determinants of anaemia severity among pregnant women
Residing in South-South (AOR = 9.27, 95% CI: 1.24–69.25, ρ < 0.030) and unemployment (AOR = 3.92, 95% CI: 1.51–10.15, ρ = 0.005) increased the odds of being severely anaemic among pregnant women as shown in Table 8. In contrast, short stature (AOR = 0.00, 95% CI: 0.00–0.00, ρ < 0.001) reduced the likelihood of severe anaemia among pregnant women (Table 8). Whereas residing in the North-East region reduces the likelihood of moderate anaemia, residing in the South-East region increases the risk of being moderately anaemic. Also, rural residence (AOR = 1.44, 95% CI: 1.04–1.98, ρ = 0.027), no education (AOR = 4.97, 95% CI: 2.68–9.19, ρ < 0.001), primary education (AOR = 4.82, 95% CI: 2.54–9.16, ρ < 0.001), and secondary education (AOR = 2.40, 95% CI: 1.35–4.28, ρ = 0.003) increased the likelihood of developing moderate anaemia.
Risk factors for severity of anaemia among pregnant women in Nigeria, 2018.

Significance at p < 0.05.
Discussion
The high anaemia prevalence among pregnant women in our study is consistent with evidence from some community-based studies in sub-Saharan Africa,25,28 but contrasts with the lower anaemia prevalence in other prior studies in Sudan and Ethiopia due to differences in dietary practices, iron supplementation, and malaria endemicity.22,26,29 Similarly, the high anaemia prevalence among WRA and non-pregnant women in the current study compares to evidence of high prevalence from previous African studies.11,12,16,31 In contrast, other African studies found low anaemia prevalence among WRA.12,13,15,17–19 Since anaemia prevalence greater than 40% constitute a severe public health problem, 41 our findings indicate that anaemia among WRA is a grave public health problem in Nigeria. Consequently, increased maternal mortality, poor birth outcomes, and reduced productivity due to anaemia among reproductive-age women might persist in Nigeria.9,10 To reduce anaemia prevalence, the Government of Nigeria introduced the national guidelines on micronutrient deficiency control in 2013. 42 The Government of Nigeria has implemented measures to reduce anaemia including universal iron and folate supplementation for adolescent girls and during pregnancy, deworming of pregnant women and adolescents, food fortification, promotion of dietary diversification, focused antenatal care, intermittent preventive treatment of malaria during pregnancy, health education, and promotion of personal hygiene.6,42,43 Therefore, there is a need not only to sustain these interventions but also to address the risk factors identified in this study in strategies to reduce anaemia prevalence in Nigeria.
Our findings of significant regional differences in anaemia prevalence and severity among WRA, pregnant women, and non-pregnant women are consistent with evidence that residing in specific regions or provinces increased the odds of being anaemic in other LMICs.15,17,18,20,44 Our finding that the northern regions were largely protective is surprising given that households in South-East and South-South zones consumed more diverse diets than in other regions in Nigeria. 45 Contrary to our finding, anaemia prevalence among WRA was higher in the Northern regions than in Southern regions in a previous Nigerian study. 4 The reduction in anaemia in the Northern regions in the current study might stem from the use of different datasets and the timing of the studies. Our study used the 2018 NDHS dataset, but the prior study used the 2015 NDHS dataset. 4 It could be that variations in geographical and dietary-related factors could have a role in regional differences in anaemia prevalence as found in an earlier study. 14 The high consumption of meat and milk, which are rich in iron, may be one reason for the low prevalence of anaemia in the North. Between 2013 and 2017, there was improved access to a micronutrient, use of health facilities, nutritional counselling, and dietary diversity in Northern Nigeria resulting from increased donor-supported community-based maternal and child nutrition and food security interventions in Northern Nigeria. 46 Future qualitative studies to understand the geographical disparities in anaemia prevalence in Nigeria are warranted.
Our finding that rural residence predicted increased risk of anaemia and its severity is consistent with increased odds of being anaemic among pregnant women,28,31,32 non-pregnant women, 24 and all WRA4,11,13,15,21,44 in prior studies but differs from other studies where a rural residence is protective 14 or urban residence is a risk factor. 16 Low access to mass media in rural areas resulting in inequitable access to health information might contribute to the risk of being anaemic even though media exposure was only significant for moderate anaemia among all WRA and NPW in our model. 47 Second, Nigerian women residing in urban areas are more likely to be overweight/obese, while rural women are more likely to be either underweight or overweight. 48 Third, rural women are less likely to use modern contraceptives compared to urban women. 49 In our study, being underweight and non-use of contraceptives increased the odds of being anaemic among all WRA and NPW. To reduce the anaemia burden in rural areas, strategies addressing these rural disparities are needed.
Our findings that low education increased the odds of being anaemic and anaemia severity among all WRA, pregnant women, and non-pregnant WRA agreed with evidence from prior studies among pregnant women,19,31 and all WRA,4,13,16 whereas educational attainment was protective of being anaemic.2,12,14 As stated elsewhere,4,13 high education helps women to improve their nutrition and sanitary practices, hence reduce the risk of anaemia. Also, the more educated pregnant women complied with the uptake of iron-folate supplements to prevent anaemia during pregnancy. 31 Evidence shows that women who did not consume iron supplements during pregnancy had consistently higher odds of anaemia compared to women who did. 15
Equally, this study’s findings that being unemployed increased the odds of being anaemic among all WRA, pregnant women, and non-pregnant women are consistent with evidence from earlier studies.11,14,20,27 Furthermore, unemployment increased the risk of severe anaemia among pregnant women and overall WRA in the current study. First, employment could enhance women’s participation in household decision-making for their health care, hence improving health-seeking behaviours. 50 Second, employment increases women’s economic empowerment, which means that women can effectively improve their food consumption preferences and hygienic practices. 50 Third, enhanced women’s decision autonomy and economic empowerment increase the use of modern contraceptives, which in turn, decreases the likelihood of being anaemic. 23
Our findings that household socio-economic status predicted anaemia prevalence and severity among all WRA and non-pregnant women highlight the protective role of wealth and predisposing role of poverty in being anaemic. These findings agreed with existing evidence that the rich quintile reduced the likelihood of being anaemic among non-pregnant women 24 and in all WRA,2,11,12,14,18,44 while being poor increased the likelihood of anaemia among all WRA.4,13,16,17,21,22,31 High socio-economic status improves women’s access to improved sanitation, adequate dietary diversity, enhanced access to health care facilities as well as better media exposure, which contribute to the prevention of anaemia among WRA. 51
The use of modern contraceptives reduced the risk of being anaemic and anaemia severity as was reported in several prior studies among non-pregnant women,23,24 and all WRA.2,14,17,18 Conversely, contraceptive use increased the likelihood of being anaemic. 12 Evidence from the literature indicates that the prevalence of anaemia declines with increasing duration of use of modern contraceptives in one of three ways. 23 First, spacing births reduces nutritional stress associated with successive pregnancies, preventing maternal iron depletion. 23 Second, some contraceptives modify the iron status, which lowers the risk of being anaemic. 23 Third, iron-containing contraceptives provide iron supplementation to prevent iron deficiency anaemia. 23 Further studies are needed to determine which of these factors play a greater role in predisposing to anaemia among WRA in Nigeria.
Similar to findings in Ethiopia, normal body weight reduced the likelihood of being anaemic among non-pregnant women in our study. 24 Our findings also agreed with evidence that normal weight11,17 and being overweight or obese 18 reduced the chances of anaemia, but underweight increased the risk of anaemia among all WRA.11,16–18 Nevertheless, short stature was found to be a protective factor for being anaemic and developing severe anaemia among pregnant women in the current study. The protective influence of short stature might be because women with short stature were prioritized in micronutrient supplementation and food fortification interventions in Nigeria. 43 Anaemia, due to being underweight, might result from undernourishment, but poor dietary diversity was not predictive of being anaemic in this study. Further studies are required to determine the relationship between micronutrient-rich diets and BMI and anaemia among WRA and non-pregnant women in Nigeria.
Our finding that large household size increased the likelihood of developing anaemia is congruent with evidence from Ethiopia and Rwanda.14,17 Low per capita income, commonly seen in large-sized households, results in food insecurity, reducing access to a diversity of sustainable healthy diets, and predisposing women to nutritional deficiency anaemia. On the contrary, our finding that lack of media exposure increased the likelihood of being moderately anaemic among non-pregnant and overall WRA is consistent with evidence from a preceding study. 52 Access to media is associated with awareness of the value and availability of health services,47,53 information on diets and nutrition, 54 and increased likelihood of contraceptive use.55,56 Furthermore, our finding that age 30 to 39 increased the odds of developing moderate anaemia among non-pregnant women contrasts evidence of reduced odds of anaemia among this age group in Ethiopia. 13 A possible explanation for the increased odds among women aged 30–39 years in Nigeria could be their high fertility rates.13,35
Our study provides generalizable evidence of determinants of anaemia among WRA in Nigeria. Second, we included both pregnant and non-pregnant WRA. Nevertheless, a cause-and-effect relationship cannot be established in a cross-sectional study such as ours. Also, pregnancy status relied on women’s verbal responses and was not validated by any clinical test, which could bias the results. Moreover, this study did not account for chronic diseases such as blood disorders and metabolic diseases, which might affect anaemia status.
Conclusion
Anaemia prevalence among WRA, pregnant women, and non-pregnant women constituted a severe public health problem. The region, rural residence, low education, unemployment, low wealth index, and non-use of modern contraceptives increased the likelihood of being anaemic among all WRA and non-pregnant women. Lack of media exposure significantly increased the odds of developing severe anaemia among overall WRA and non-pregnant women. In addition, large family size significantly increased the likelihood of being anaemic among overall WRA. Among pregnant women, specific regions, unemployment, and low education also increased the likelihood of being anaemic and developing severe anaemia. Whereas underweight increased the likelihood of being anaemic in non-pregnant women, short stature reduced the odds of both anaemia and severe anaemia among pregnant women. Considering these factors in health and nutrition interventions and programmes would reduce anaemia prevalence and severity among WRA in Nigeria.