
Abstract
Background:
Maternal and child mortality rates remain a serious public health challenge in Ethiopia. Short interpregnancy intervals are known to negatively impact perinatal and child health; therefore, improving this practice is a key strategy to reduce mortality and adverse outcomes.
Objective:
This study aimed to evaluate the extent of short intervals between pregnancies and the factors associated with them among women who gave birth at public hospitals in the North Wollo Zone of northeastern Ethiopia in 2023.
Design:
A facility-based cross-sectional study was conducted in the North Wollo Zone of northeastern Ethiopia in 2023.
Methods:
This study was conducted on mothers who delivered at public hospitals in the North Wollo Zone of northeastern Ethiopia. The study participants were selected using a systematic random sampling technique between February 1, 2023, and April 1, 2023. Data were collected through an interviewer-administered questionnaire using the Kobo Collect tool and analyzed using SPSS version 27.0. Bivariable and multivariable analyses were performed to determine the relationship between the outcome and predictor variables. A p value of less than 0.05 was considered significant in the multivariable analysis.
Results:
The study found that 51.5% of participants had short interpregnancy intervals. Several independent factors were associated with a short birth interval, including the status of the last pregnancy (adjusted odds ratio (AOR): 9.51; 95% CI: 3.932–23.0028), educational status of the woman (AOR: 4.545; 95% CI: 1.208–17.108), and use of modern contraceptives in previous pregnancies (AOR: 6.460, 95% CI: 3.882–23.008).
Conclusion:
Despite the efforts made through public health interventions in Ethiopia, the prevalence of short interpregnancy intervals in this study was high. Therefore, increasing the utilization of modern contraceptives and promoting health education at both health facilities and community levels could contribute to addressing this issue.
Plain language summary
Why was the study done? This study was conducted to evaluate the prevalence of short intervals between pregnancies and identify the factors associated with them among women who gave birth at public hospitals in the North Wollo Zone of northeastern Ethiopia in 2023. This research aimed to understand the extent of the issue and its determinants to inform strategies and interventions aimed at reducing maternal and child mortality and improving health outcomes in the region.
What did the researchers do? This cross-sectional study was conducted in 2023 in the North Wollo Zone of northeastern Ethiopia. They selected mothers who had given birth at public hospitals between February and April 2023 using systematic random sampling. Data were collected through interviews and analyzed to identify factors associated with short birth intervals.
What did the researchers find? The researchers found that over half (51.5%) of the participants had short intervals between pregnancies. They discovered significant associations between short birth intervals and factors such as the outcome of the last pregnancy, educational status of the women, and use of modern contraceptives in previous pregnancies. These findings highlight the importance of addressing these factors to improve the maternal and child health outcomes in the region.
What do the findings mean? These findings suggest that a considerable proportion of women in the North Wollo Zone of northeastern Ethiopia experienced short intervals between pregnancies. Factors such as the outcome of previous pregnancies, educational status, and use of modern contraceptives play crucial roles in determining the length of birth intervals. Addressing these factors through improved access to modern contraceptives and enhanced health education could potentially reduce the maternal and child health risks associated with short birth intervals in the region.
Background
The World Health Organization (WHO) defines birth interval as the time between a live birth and subsequent pregnancy and recommends a minimum interval of 24 months. 1 Short birth intervals of less than 2 years have a negative impact on the health of both mothers and their children. 2 However, adequate birth intervals allow women to recover from nutritional depletion that occurs during pregnancy and breastfeeding, leading to improved health outcomes for children and subsequent pregnancies. 2
Maternal and newborn mortality is a significant global public health issue, with low-income countries disproportionately affected.2–5 Sub-Saharan Africa (SSA) and South Asia account for 87% of the estimated 358,000 maternal deaths per year and more than 75% of the 3.6 million newborn deaths worldwide according to a 2017 WHO study. SSA has the highest maternal mortality rate, with 533 maternal deaths per 100,000 live births or 200,000 deaths annually. Two-thirds (68%) of all maternal deaths worldwide occur in this region.3,5
Short birth intervals have been linked to negative health outcomes for both mothers and newborns, including preterm birth, low birth weight, perinatal death, stillbirth, intellectual disability, and developmental delays.6,7 Maternal health is also affected, with consequences such as nutrient depletion, anemia, cervical insufficiency, antepartum hemorrhage, preterm membrane rupture, and eclampsia.7,8 In addition, closely spaced birth intervals contribute to rapid population growth, which hinders development efforts and limits women’s ability to participate in workforce and economic development. 9 Limited resources within a family are often disproportionately allocated to newborn care, potentially neglecting the needs of other children.10,11
Studies conducted in African countries, including Rwanda, Uganda, Cameroon, and Ethiopia, have reported the prevalence rates of short birth intervals ranging from 20% to 55%.5,12–14 Ethiopia has faced a significant number of infant and neonatal deaths compared to the average rates in Africa. 15 However, optimal birth spacing offers the greatest benefits in terms of health, social, and economic outcomes for families. 16 However, in developing countries, over 200 million women desire to space or limit pregnancies and lack access to family planning options. 17 Research from Demographic Health Surveys has consistently shown that factors such as maternal education, maternal age, early marriage, inability to breastfeed, and inadequate knowledge, attitude, and practice regarding modern contraceptive use are determinants of short birth intervals. 9
Despite some progress, Ethiopia still lags behind the global targets for family planning and fertility. The country’s fertility and population growth rates of 2.5% remain high, positioning Ethiopia among countries with elevated fertility rates in Africa. 19 In addition, 22% of women in Ethiopia have an unmet need for family planning, and the contraceptive discontinuation rate is 35%. 17 In addition, 22% of women in Ethiopia have an unmet need for family planning, with a contraceptive discontinuation rate of 35%. 18 Moreover, the reduction in under-5 mortality in Ethiopia has been stagnant compared to the reduction in neonatal mortality. 17 Optimal child spacing is recognized as a crucial factor in the health of women and their children. 17 Therefore, it is essential to identify the factors that influence the birth interval of women in countries with high fertility and maternal mortality rates, such as Ethiopia. Few studies have been conducted on short birth intervals in Ethiopia, particularly in the study area.
Therefore, it is important for Ethiopia to study birth spacing and its factors to improve programs that can boost the health of both mothers and children. This study aims to fill this gap by examining how long women wait between giving birth and what influences this among pregnant women in the North Wollo Zone of the Amhara Region, Ethiopia.
Method
Study area and period
This study was conducted in the North Wollo Zone, located in the Amhara Region of northern Ethiopia. The study employed a facility-based cross-sectional design and was conducted from February 1, 2023, to April 1, 2023. According to the 2017 population estimation conducted by the Central Statistical Agency of Ethiopia, the North Wollo Zone has a total population of 1,500,303, with 752,895 men. The zone is served by six public hospitals: Woldia Comprehensive Specialized Hospital, Kobo Primary Hospital, Mersa Primary Hospital, Shediho Mekete Primary Hospital, Wadila Primary Hospital, and Lalibela General Hospital. In addition, 69 health centers in the zone are expected to provide emergency obstetrics and newborn care services to the community.
Study design
This was a facility-based, cross-sectional study.
Population
Source population
The source population consisted of all pregnant women who delivered at the North Wollo Zone public hospitals.
Study population
The study population consisted of all women who gave birth at public hospitals in the North Wollo Zone during the study period and who had at least two previous births.
Eligibility criteria
Inclusion and exclusion criteria
The study included women who had to have given birth twice or could have given birth once and were currently pregnant, while those with fewer than two births or who were medically ill or unable to provide information due to their illness were excluded. In addition, women who had experienced a recent miscarriage or abortion before the current pregnancy were also excluded, as they were more likely to conceive again sooner due to pregnancy loss, and it is recommended that women have a minimum interval of 6 months.
Sample size determination and sampling technique
Sample size determination
The sample size was determined using the formula for a single population proportion. We considered the p value from a study in Tselemti, northern Ethiopia, which is 23.3% prevalence of short birth interval, 19 95% level of confidence, 5% margin of error to be tolerated, and 10% non-response rates.
When a 10% non-response rate is added n = 27.2 + 272N = 299.
where
Z = standard score corresponding to 95% confidence interval (CI); P = assumed proportion of fertility desire; and D = the margin of error (precision) 5%.
Therefore, the final sample size needed for the study considering a 10% non-response rate is 299.
Sampling technique and procedure
A systematic sampling technique is used in this study. The average number of mothers attending antenatal care in the last 2 months was reported to be 720, according to monthly hospital reports. To determine the sample population, proportional allocation was used to distribute the sample size across each hospital, based on their monthly reports. The sampling interval, denoted as “k,” was calculated by dividing the source population by the total sample size. In this case, k = 720/299, resulting in k being approximately equal to 2. An interval of two was then utilized to select the study participants. To start the sampling process, the first participant was chosen through simple random sampling, specifically using the lottery method, from among the first two maternity care users. Subsequently, data were collected from each participant based on the designated sampling interval.
Variables
Dependent variables
Short interpregnancy intervals
Independent variables
The independent variables examined in this study included the mother’s age, occupation, education level, husband’s education level and occupation, sex and survival status of the index child, parity, breastfeeding duration, pregnancy-related complications, knowledge of birth intervals, and modern contraceptive use.
Data collection procedure and quality management
The study employed a structured interviewer-administered questionnaire developed after a thorough review of the pertinent literature. The methodology section of the study strictly adhered to the guidelines outlined in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for observational studies (Supplemental Material). This adherence ensures that the research aligns with established best practices for meticulous data collection and rigorous analytical procedures.4,19,20 Initially prepared in English, the questionnaire was translated into the local language Amharic. To ensure its effectiveness, the questionnaire was checked and pretested in 5% of the study population outside the selected area. The data collection process involved training eight BSc midwives over two consecutive days. These trained midwives were responsible for data collection. On each day of the data collection, the collected data were carefully reviewed for completeness and consistency. Supervision and monitoring were conducted daily by the assigned supervisors and principal investigator to ensure data quality.
Measurement of the outcome variable
The interpregnancy interval refers to the time interval between the self-reported last normal menstrual period and the reported date of the last child’s live birth. In this study, the majority of participants were aware of the due date for their current pregnancy as well as the date of their child’s birth. However, for participants who did not have exact information on the date of conception for the current pregnancy or the birth date of the previous child, an approximation was made by considering the middle of the month. To calculate the interpregnancy interval, the date of birth of the previous child was subtracted from the date of conception of the current pregnancy using the formula: IPI = date of conception (LMP) − date of birth of the previous child. A short interpregnancy interval was defined as an interval of less than 24 months.
Data processing and analysis
Data were collected through face-to-face interviews using a pretested, semi-structured questionnaire. The questionnaire was initially prepared in English and then translated into the local language (Amharic), followed by back translation into English. Eight midwifery students with BSc degrees were involved in the data collection under the supervision of two MSc midwives in each cluster. Regular meetings were held between the data collectors, supervisors, and lead investigators throughout the data collection process.
Prior to entry, the collected data were reviewed and checked for completeness. Incomplete data were excluded. The data were entered, cleaned, and analyzed using Epi-data version 3.1 software, EpiData Association. The final dataset was exported to SPSS version 25, IBM (International Business Machines Corporation) for further analysis. Descriptive statistics such as frequencies, proportions, and summary data were used to describe the study population. A binary logistic regression model was used to assess the association between the outcome and explanatory variables. In the multivariate analysis, variables with a p value less than 0.2 in the bivariate analysis were included to minimize confounding effects. The strength of the associations is presented using adjusted odds ratios and 95% CIs. Statistical significance was set at 5%. Model fitness was assessed using the Hosmer–Lemeshow test, while multicollinearity was examined using the variance inflation factor.
Operational definitions and definition of terms
Optimal interpregnancy intervals are defined as birth intervals between the child under study and the immediately preceding live and surviving birth of the mother, ranging from 24 to 36 months, which includes 3 to 5 years. 21
Short interpregnancy intervals are characterized by birth intervals of less than 24 months between the child under study and the immediately preceding live and surviving births of the mother. 22
Long interpregnancy intervals refer to birth intervals greater than 36 months between the child under study and the immediately preceding live and surviving births of the mother. 22
Postpartum complications occur during the first 6–12 weeks following the delivery of an infant. These complications can arise from normal physiological changes that the body undergoes to return to its pre-pregnancy state, or as a result of complications during the labor and delivery process. 22
Unplanned pregnancy: Occurs without active planning, and may be a surprise or inconvenience, but the individual/couple is open to the idea of having a child. 23
Unwanted pregnancy: Pregnancy not desired by the individual/couple, actively not wanted, may lead to considering options like abortion or adoption. 23
Result
Sociodemographic characteristic
A total of 299 mothers participated in this study, with a response rate of 100%. The majority (80.4%) of the study participants were married, 81 (27.1%) were in the age group of 25–29, and 163 (53.8%) lived in urban areas (Table 1).
Sociodemographic characteristics of women who delivered in North Wollo Zone public hospital, Ethiopia 2023.

Maternal/obstetric characteristics
Of the 299 total respondents, 166 (55.5%) had gravidities of three or more, but 133 (44.5%) had low parity. Of the 199 (66.6%) current pregnancies, 100 (33.4%) were unplanned. Out of a total of 100 respondents, unplanned pregnancies were due to not using family planning; failure of family planning and having unplanned sex were the major reasons. Of the 299 total respondents, 72 (22.4%) had abortions; however, about 50 (16.7%) mothers reported that their children died soon after birth (Tables 2 and 3).
Maternal obstetric characteristics of the prevalence of short interpregnancy intervals among mothers delivered in North Wollo Zone public hospital, Ethiopia, 2023.

CS, Cesarean section.
Pregnancy-related complications of the prevalence of short interpregnancy intervals among mothers delivered in North Wollo Zone public hospital, Ethiopia, 2023.
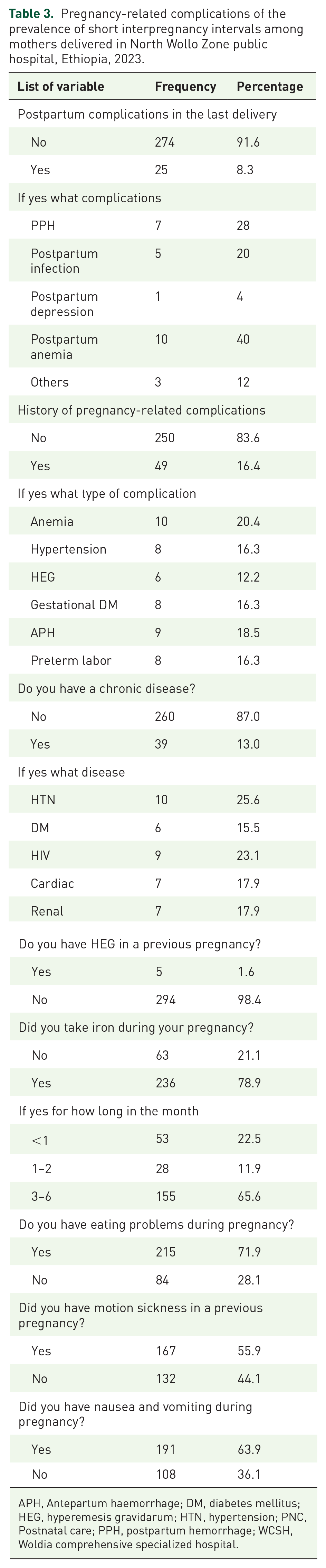
APH, Antepartum haemorrhage; DM, diabetes mellitus; HEG, hyperemesis gravidarum; HTN, hypertension; PNC, Postnatal care; PPH, postpartum hemorrhage; WCSH, Woldia comprehensive specialized hospital.
Knowledge of birth interval
Many of the respondents (149, 49.8%) had heard of birth spacing; however, out of the total, 150 (50.2%) had not. Respondents considered a varied number of months as the appropriate length of time between two births. From the whole group, 53 (17.7%) said below 2 years, 110 (36.7%) said 2–5 years, 62 (20.7%) said above 5 years, and 74 (24.7%) explained that they did not know about it. The majority of 242 (80.9%) of the study respondents agreed that an optimal birth interval has health advantages for the mother and child, while the remaining 57 (19.1%) did not agree (Table 4).
Knowledge of the birth interval of the prevalence of short interpregnancy intervals among women delivered in North Wollo Zone public hospital, Ethiopia, 2023.

Biological and behavioral factors
Ages at first marriage: The majority of respondents were above 18 years old, and out of the total 141 (63.5%), 267 (89.2%) of mothers at PNC in WCSH had breastfed their last child, but about 32 (10.7%) of them had not breastfed their last child (Tables 5 and 6).
Biological and behavioral prevalence of short interpregnancy intervals among women delivered in North Wollo Zone public hospital, Ethiopia, 2023.

Family planning knowledge prevalence of short birth interval among women Delivered in North Wollo Zone public hospital, Ethiopia.

Prevalence of short interpregnancy interval
In this study, the prevalence of short interpregnancy intervals (<24 months) was 154 (55.5%), with a 95% CI of 43–56. The median interpregnancy interval of the study subjects was 30 (17–49) months. Among the short interpregnancy intervals, 29 (9.6%) experienced a very short interpregnancy interval (less than 12 months).
Factors associated with short interpregnancy intervals
The analysis began with binary logistic regression, where variables with a p value of less than 0.25 were selected for further analysis using multiple logistic regressions. 10 In the bivariate logistic regression analysis, several variables showed a statistically significant association with the outcome variable, which was a short birth interval. These variables included the educational status of the mother, status of the last pregnancy (unplanned), sex of the index child, use of modern contraceptives, fetal outcome of the last pregnancy, and ANC follow-up in the last pregnancy. Subsequently, multiple logistic regression analyses were performed using the selected variables. Three independent variables were identified as significant predictors of short birth intervals. These variables were the education of the mother, non-contraceptive use, and the status of the previous pregnancy (Table 7).
Bivariable and multivariable binary logistic regression analysis results of factors associated with short interpregnancy interval among women who delivered in North Wollo Zone public hospital, Ethiopia, 2023.

ANC, antenatal care; AOR, adjusted odds ratio; COR, crude odds ratio.
Discussion
The study conducted at the North Wollo Zone public hospital in Ethiopia aimed to identify factors influencing short birth intervals among mothers who delivered in 2013. Adequate interpregnancy intervals are important for women to recover from the physical and nutritional effects of pregnancy and to ensure optimal health before conceiving again, particularly in regions with high perinatal mortality and fertility rates, such as SSA.
The findings of this study indicated that mothers with no formal education were more likely to have shorter interpregnancy intervals than those who had received formal education. This finding aligns with those of previous research conducted in Saudi Arabia, Nepal, Jordan, and Pakistan.24–27 The higher likelihood of shorter birth intervals among women with no formal education can be partly attributed to the fact that educated women often have greater decision-making autonomy and access to information about healthcare options. Conversely, women with limited education may lack awareness of the potential negative consequences of having multiple children in quick succession. These findings highlight the significance of education in empowering women to make informed decisions regarding family planning and reproductive health. Improving women’s access to education can help increase their knowledge and awareness of the importance of spacing pregnancies adequately, ultimately contributing to better maternal and child health outcomes.
The findings of this study align with previous research conducted in various regions such as Manipur, Ethiopia, Jordan, Ahvaz (Iran), and Egypt, which has shown that women who did not use modern methods of contraception before becoming pregnant with their last child were more likely to have shorter birth intervals than those who used contraception.24,28–30 This can be attributed to the effectiveness of modern contraception in preventing and delaying pregnancy. The non-use and failure of contraception are significant contributors to unintended pregnancies, which may lead to shorter interpregnancy intervals.
The sex of the previous child was also found to be strongly correlated with the birth interval in this study. Mothers with female pregnancies were more likely to have shorter birth intervals than those with male pregnancies. Similar findings have been reported in studies conducted in Manipur, Saudi Arabia, Babol, Jordan, and Tanzania.24,25,28 This can be explained by cultural and economic factors that influence reproductive decision-making. In some societies, having children, especially male children, is considered an economic asset for families. As a result, mothers may be less inclined to practice long-term breastfeeding or use modern contraceptives until they achieve their desired number of children.
Furthermore, this study found that mothers who had an unexpected pregnancy were at higher risk of having a short birth interval. Similar effects were observed in studies conducted in Mississippi, Tennessee, and New Guinea.31,32 Unplanned pregnancies may disrupt the intended birth spacing and lead to shorter intervals between pregnancies.
Despite the WHO and the government of Ethiopia’s optimal birth interval recommendations, this study found that a higher proportion of women (51.5%) became pregnant before the recommended time, which hinders the health of women, children, and the community at large, similar to adverse maternal and infant health outcomes. It is known to affect perinatal, neonatal, and child health outcomes, including preterm birth, low birth weight, perinatal death, stillbirth, intellectual disability, and developmental delays. It also has adverse maternal health outcomes such as nutritional depletion, anemia, cervical insufficiency, and antepartum hemorrhage.
Limitations of the study
Descriptive cross-sectional studies were used in this research, which may not have established causal relationships between different factors and short birth intervals. The limitations of the cross-sectional design prevented causal inferences from being demonstrated. In addition, there is a possibility of recall bias, since women were asked to provide information about past events, although various techniques were employed to aid memory recall. Furthermore, the exclusion of women who had experienced a miscarriage or abortion just prior to their current pregnancy may have underestimated the prevalence of short interpregnancy intervals.
Recommendation
The study found that a significant proportion of mothers (51.5%) in the sample were still practicing short birth intervals, despite the importance of optimal spacing to reduce fertility and improve maternal and child mortality rates. To address this issue, it is recommended that healthcare providers, including health workers and health extension workers, deliver informative and comprehensive counseling on birth spacing at both the healthcare facilities and community levels. The North Wollo Health Bureau should prioritize programs that emphasize the use of modern contraceptives for birth spacing and promote overall maternal and child health. Information about birth spacing should be disseminated through various channels, including healthcare institutions, the mass media, and community platforms. In addition, Zonal and District health officials, along with health extension workers, should raise awareness of the significance of antenatal care follow-up and ensure easy access to cost-free family planning services and contraceptive methods in the region.
Conclusion
The educational level of the mother, status of previous pregnancy, and use of modern contraceptives were found to have a statistically significant association with the occurrence of a short birth interval. A significant percentage of mothers in the study had no formal education, which resulted in low utilization of family planning methods despite having knowledge about them.
Supplemental Material
sj-docx-1-reh-10.1177_26334941241301392 – Supplemental material for The magnitude of short interpregnancy intervals and associated factors among women who delivered in North Wollo Zone public hospitals, northeastern Ethiopia, 2023: A facility-based cross-sectional study
Supplemental material, sj-docx-1-reh-10.1177_26334941241301392 for The magnitude of short interpregnancy intervals and associated factors among women who delivered in North Wollo Zone public hospitals, northeastern Ethiopia, 2023: A facility-based cross-sectional study by Mulugeta Wodaje Arage, Samrawit Shimels, Abebe Tarekegn Kassaw and Gizachew Yilak in Therapeutic Advances in Reproductive Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.