
Abstract
Background:
Preterm premature rupture of membranes (PPROM) is a significant risk factor for perinatal morbidity and mortality. It is the main cause of preterm birth and affects approximately 10% of all pregnancies. The occurrence of PPROM has recently increased significantly. However, there is limited data on the determinants of PROM in the study area.
Objective:
To assess the determinants of PPROM, among pregnant women admitted to maternity wards of public hospitals in the Sidama Region.
Design:
An institution-based, unmatched case–control study
Methods:
The study was conducted in public hospitals in the Sidama Region from March 1st to May 15th, 2023. The consecutive cases were recruited until the required sample size was reached, and controls were randomly selected. Face-to-face interviews were used to collect data from 69 cases and 207 controls. Binary logistic regression analysis was used to identify determinants of PPROM. An adjusted odds ratio (AOR) with a 95% confidence interval (CI) was reported to show the strength of the association. The significance of the association was declared at a p value <0.05. The goodness-of-fit model was checked by the Hosmer–Lemeshow test.
Results:
A total of 69 cases and 207 controls were included in the study. Pregnancy-induced hypertension (AOR: 2.65; 95% CI: 1.12–6.27), a history of abortion (AOR: 3.1; 95% CI: 1.41–7.08), a history of abortion (AOR: 3.78; 95% CI: 1.75–8.15), a history of cesarean section (AOR: 2.57, 95% CI: 1.10–5.99), a mid-upper arm circumference <23 cm (AOR: 2.1; 95% CI: 1.02–4.54), a history of urinary tract infection (AOR: 2.42; 95% CI: 1.10–5.32), and a hemoglobin level <11 mg/dl (AOR: 2.68; 95% CI: 1.15–6.23) were determinants of PPROM.
Conclusion:
Past obstetric history, nutritional status, and risks in the index pregnancy have an association with PPROM. Therefore, strategies to reduce the occurrence of PPROM should target women in rural areas and emphasize the early identification and treatment of urinary tract infections, anemia, and pregnancy-induced hypertension.
Introduction
Premature rupture of membranes (PROM) occurs in 2%–18% of pregnancies before labor onset. 1 Preterm PROM (PPROM) accounts for 20%–40% of premature membrane rupture and occurs before 37 weeks of gestation. 1 It increases the risk of intraamniotic infection, postpartum infection, and endometritis in pregnant women, leading to high maternal and neonatal morbidity and mortality. 1 It also has serious effects on pregnancy and increases the risk of premature labor by 2.58 times. 2 PPROM is a condition characterized by abnormalities in the uterus, cervix, or vagina, often linked to excessive amniotic sac stretching, sexually transmitted infections, and low socioeconomic status.3,4 While it cannot be avoided, however; women with a history of PROM can reduce risk by taking vitamin C supplements after the 14th week. 5
The occurrence of PPROM varies from country to country; 1.94% in rural Nigeria, 6 3.08% in India, 7 4.91% in Cameroon, 8 8.2% in Bangladesh, 9 and 13.8% in rural Uganda. 10 The prevalence of PPROM in Ethiopia varies, with Wolkite Comprehensive Specialized Hospital reporting 6.6% 11 to 13.7% in Debre Tabor General Hospital. 12 Several factors, such as gestational diabetes, anemia, history of PROM, abnormal vaginal discharge, history of cesarean section (CS), urinary tract infection (UTI), malnutrition, cigarette smoking, and history of abortion were determines of PPROM.11 –15
A PPROM is closely linked with unfavorable pregnancy outcomes, including prematurity, stillbirth, neonatal jaundice, and neonatal intensive care unit (NICU) admission.16,17 The Sustainable Development Goal (SDG) 3 aims to improve maternal and child health by reducing poverty, improving maternal nutrition, and providing quality primary healthcare. 18 However, a systematic review and meta-analysis reported that over a quarter of pregnant women in Ethiopia are anemic. 19 Furthermore, previous studies have produced inconsistent findings regarding the association between anemia and PPROM. Some studies have indicated that anemia is significantly associated with PPROM, 14 while others have found no such significant association.11,12 This discrepancy underscores the need for further studies. There is limited data on the determinants of PPROM in the study area. Therefore, this study aimed to assess the determinants of PPROM at public hospitals in the Sidama Region.
Methods
Study area and period
The study was conducted in public hospitals located in the Sidama Region. Hawassa is the capital city of the Sidama Region and is located 273 km south of Addis Ababa, Ethiopia’s capital city. There are 22 public hospitals in this region (1 comprehensive specialized hospital, 5 general hospitals, and 16 primary hospitals). The aforementioned health facilities offer various maternal and child health services, including antenatal care (ANC), labor, delivery, family planning, safe abortion, comprehensive abortion care, visual inspection with acetic acid, sexual assault, prevention of mother-to-child transmission, immunization, NICU, and gynecologic problem diagnosis and treatment. The study was conducted from March 1st to May 15th, 2023.
Study design
A hospital-based, unmatched case–control study was conducted among pregnant women in maternity wards of public hospitals in the Sidama Region.
Population
All mothers with a gestational age of more than 28 weeks were admitted to the labor, maternity, and high-risk wards of public hospitals in the Sidama Region, as were the source population. The study population for controls was those selected pregnant mothers with a gestation age between 28 and 36+6 weeks who were admitted to labor, maternity, or high-risk wards of specific hospitals and who experienced a painless flow of fluid from the vagina along with a change in the color or size of the uterus. The study population for controls was those selected pregnant mothers with a gestational age of more than 28 weeks and admitted to the same wards of the selected hospitals without any of the aforementioned signs during the study period. Mothers who were initially in the control group but later shifted to the case group were excluded from the study. Participants who had a gestational age of less than 28 weeks and those who were very ill during the duration of data collection were not included.
Sample size and sampling technique
Sample size calculation
We used Centers for Disease Control and Prevention (CDC) Epi Info version 7 statistical software to determine the sample size for an unmatched case–control study, with assumptions including a 95% confidence level, 80% power, a 1:3 case-to-control ratio, and a percentage of exposure among controls and cases (proportion of cesarean section among women without PPROM). The percent of cases exposed to cesarean section (25.8%) and the percent of controls exposed to CS (10.2%) were taken from a study conducted in public Hospitals of Guraghe Zone. 20 The sample size was 264 (66 cases and 198 controls) based on the aforementioned assumptions. The study’s final sample size was 290 (72 cases and 218 controls) after accounting for a 10% nonresponse rate.
Sampling technique
Six out of 22 public hospitals in the region were selected based on obstetric case management reports over the past 3 months before data collection. The sample size was proportionally allocated for the selected hospitals based on caseload. The cases were from Hawassa University Comprehensive Specialized Hospital (20 cases and 60 controls), Adare General Hospital (26 cases and 78 controls), Motitte Furra Primary Hospital (5 cases and 15 controls), Tula General Hospital (5 cases and 15 controls), Leku General Hospital (3 cases and 9 controls), and Yirga Alem General Hospital (10 cases and 60 controls). Three controls were chosen at random, and the cases were enlisted until the necessary sample size was reached.
Study variables
Dependent variable: PPROM (yes/no).
Independent variables: Socioeconomic and demographic factors included the mother’s age, marital status, employment, level of education, location of residence, and monthly income. Obstetric factors included the following: previous history of PROM, history of abortion, gravida, parity, history of cesarean section, and history of trauma to the abdomen during the index pregnancy. The medical and other factors included a history of genitourinary tract infection, history of abnormal vaginal discharge during the current pregnancy, hypertension during the current pregnancy, Diabetes Mellitus, anemia, alcohol consumption, and the mid-upper circumference of the mother.
Operational definition
PROM: A spontaneous rupture of membranes after 28 weeks but before 37 weeks of gestational age. 1 The physician confirmed PPROM through diagnostic examinations, including speculum examinations, categorizing mothers as “mothers with PPROM” and “mothers without PPROM.”
Mid-upper arm circumference (MUAC): A MUAC of less than 23 cm was considered inadequate nutritional status in the present study. 21
Data collection tool and methods
A structured questionnaire and checklist were developed after reviewing different kinds of literature.11,12,22 –24 The data were collected through a chart review and an interview. The data were collected by two trained midwives. The questionnaire was prepared in English and translated into Amharic. The checklist consists of demographic, obstetric-related characteristics, and medical and behavioral-related variables. Nonelastic MUAC tapes were used to measure each woman’s MUAC at the midpoint of her left arm’s elbow and shoulder tips.
Data quality
A pretest was conducted on 5% of the study sample of women (4 cases and 12 controls). The supervisors and data collectors had a day of training before data collection, and onsite supervision was provided to address any concerns regarding the methods and instruments used. The collected information was checked for consistency and completeness on the same day by the principal investigator. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) for case–control studies was used to report the findings of the study (Supplemental Material). 25
Data processing and analysis
An Open Data Kit was used for data collection, and IBM Statistical Package for the Social Sciences (SPSS) version 25 was used for analysis. A summary of descriptive statistics is provided by the frequency, percentage, and mean, along with the standard deviation. Bivariable and multivariable logistic regression analyses were utilized to identify the factors associated with PPROM. Variables with a p value ⩽0.2 in the bivariable analysis were included in the final multivariable analysis. Multi-collinearity was assessed using the variance inflation factor, which yielded a mean Variance Inflation Factor (VIF) of 1.63, suggesting that there is no collinearity present. An adjusted odds ratio (AOR) with a 95% confidence interval (CI) was reported to show the strength of the association. The significance of the association was declared at a p value <0.05. The Hosmer–Lemeshow test was used to evaluate the goodness of fit (p value = 0.810).
Results
Sociodemographic characteristics
In all, 276 mothers (69 for cases and 207 for controls) participated in the study, yielding a 95.1% response rate. The median age of the study participants in both the case and control groups was 27.5 (Interquartile rang = 12). Approximately 43.48% of the patients and 54.59% of the controls were housewives. Over a quarter of the cases and more than one-third of the controls had completed secondary education. Approximately half of the cases and two-thirds of the controls lived in urban areas. The proportion of participants earning less than 5000 Ethiopian Birrs was greater in the cases than in the controls (Table 1).
Sociodemographic and economic characteristics of mothers admitted to public hospitals in the Sidama Region, Ethiopia, 2023.
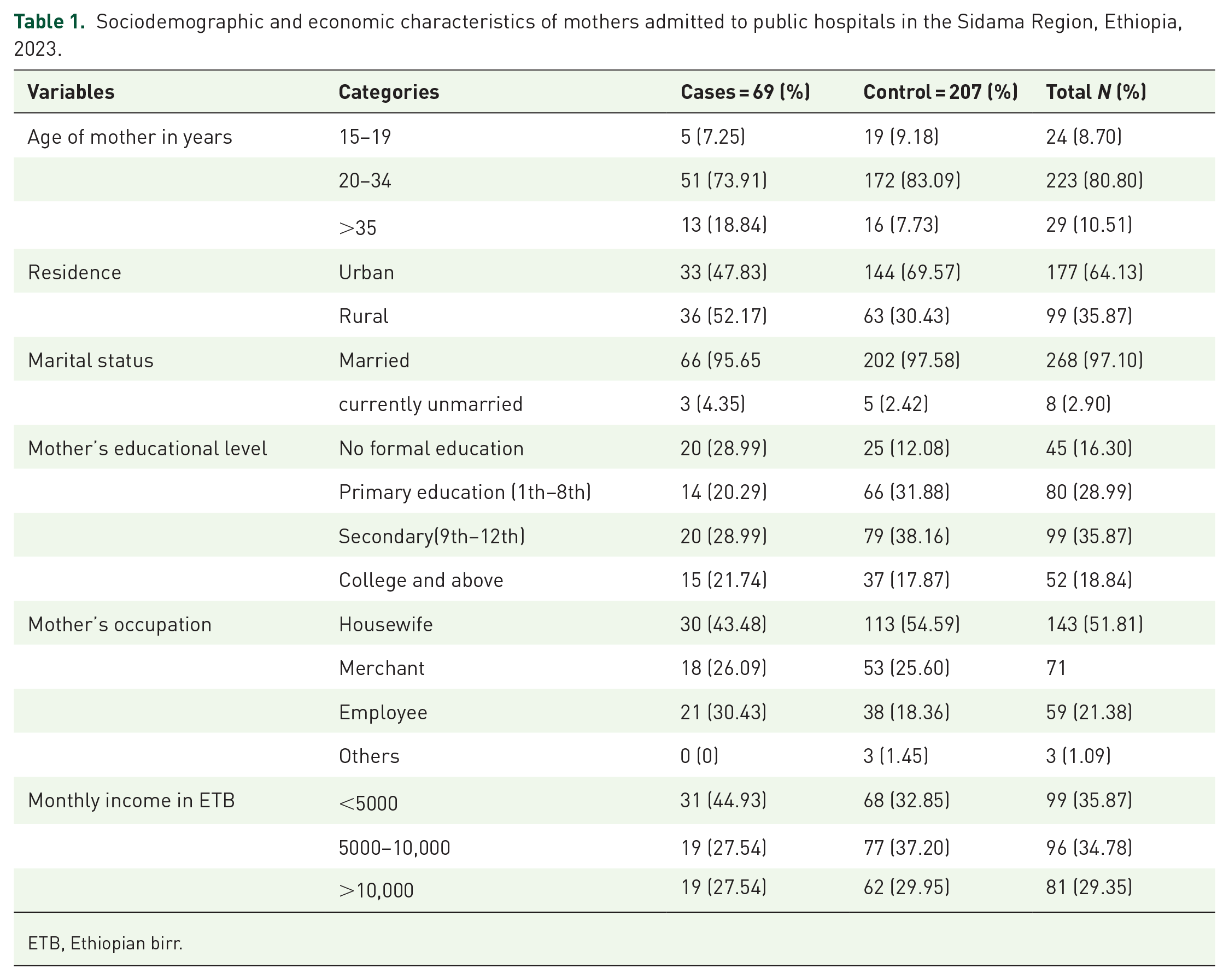
ETB, Ethiopian birr.
Obstetric characteristics
The majority of cases (43 (62.32%)) and controls (154 (74.40%)) were multigravida. Twenty-five (36.25%) cases and 41.55% of controls had visited less than four ANC facilities. A total of 28 (40.54%) cases and 36.23% of the control participants started ANC before 16 weeks of gestational age. Thirty-one (44.93%) cases and 24.64% of the controls had an abortion. A history of cesarean section was observed in 18.36% of the controls and 33.3% of the cases. About 11.1% of control women and 25% of cases had a history of PROM. One-third of the cases and 20.77% of the controls had pregnancy-induced hypertension (PIH; Table 2).
Obstetric characteristics of women admitted to public hospitals in the Sidama Region, 2023.

ANC, antenatal care; APH, Antepartum hemorrhage; PIH, pregnancy-induced hypertension; PPROM, premature rupture of membranes.
Twenty-six (36.68%) cases and 19.32% of the women in the control group experienced UTIs. More than one-third of the cases and 23.67% of the controls had a history of abnormal vaginal discharge. Approximately half (47.83%) of the cases and 30.43% of the controls had been diagnosed with anemia. Thirty-one (44.93%) cases and 29.95% of the controls had an upper arm circumference less than 23 cm. Twenty-six (30.43%) and 23.67% of the cases and controls, respectively, had a history of abdominal injury (Table 3).
Medical and other related characteristics of women admitted to public hospitals in the Sidama Region, 2023.

MUAC, mid-upper arm circumference: UTI, urinary tract infection.
Determinants of PPROM
In bivariable logistic regression analysis, age, educational status, residency, gravida, history of abortion, abnormal vaginal discharge, history of CS, UTI, PIH, anemia, alcohol intake, danger signs of pregnancy, and previous history of PROM and MAUC less than 23 cm were found a p value <0.2. According to the multivariable logistic regression, a previous history of abortion, a previous history of cesarean section, UTI, PIH, rural residency, anemia, and an MAUC of less than 23 cm were significantly associated with PPROM.
Pregnant women who resided in rural areas were three (AOR: 3.1; 95% CI: 1.41–7.08) times more likely to develop PPROM than women in urban areas. Pregnant women with a history of UTI had 2.4-fold greater odds (AOR: 2.42; 95% CI: 1.10–5.32) of having PPROM than pregnant women without a history of UTI. Pregnant women with MUACs <23 cm were 2.1 times (AOR: 2.1; 95% CI: 1.02–4.54) more likely to develop PROM than were those with MUACs greater than or equal to 23 cm. Compared to pregnant women without a history of abortion, those with a history of abortion had a 3.78-fold (AOR: 3.78; 95% CI: 1.75–8.15) increased risk of having PPROM.
Women who had a history of a cesarean section had 2.6 times (AOR: 2.57; 95% CI: 1.10–5.99) greater odds of developing PPROM than their counterparts. Women with hemoglobin levels below 11 mg/dl had 2.7-fold (AOR: 2.68, 95% CI: 1.15–6.23) higher odds of having PPROM than women with hemoglobin levels above 11 mg/dl. Moreover, the odds of developing PPROM were 2.65 times greater (AOR: 2.65; 95% CI: 1.12–6.27) in women who had PIH than their counterparts (Table 4).
Determinants of preterm PROM among pregnant women admitted to public hospitals in the Sidama Region, Ethiopia, 2023.

Significant at a p value <0.05 and ** significant at a p value <0.001 level.
AOR, adjusted odds ratio; COR, crude odds ratio; C/S, cesarean section; PROM, premature rupture of membranes.
Discussion
This study aimed to identify the determinants of PPROM. Thus, among pregnant women admitted to maternity wards of public hospitals in the Sidama Region, PPROM was significantly influenced by UTI, history of abortion, history of CS, MAUC <23 cm, rural resident women, hemoglobin 11 mg/dl, and PIH.
This study found that UTI was linked to PPROM. Pregnant women who had UTIs in pregnancy had 2.4 times higher odds of PPROM than pregnant women without a history of UTI. The finding was similar to a study conducted at Debre Tabor General Hospital 12 and the San José Hospital in Callao, Peru. 13 This is explained by the fact that microbes cause the production of inflammatory mediators such as prostaglandins and cytokines, which are responsible for disrupting the integrity of the fetal membrane and inducing uterine contractions. 4 UTI affects 2%–15% of pregnant women and is the main cause of preterm birth26,27; this highlights the importance of screening for UTIs.
The odds of PPROM were higher among undernourished women. Pregnant women with MUAC less than 23 cm were 2.1 times more likely to develop PPROM than those with MUACs greater than or equal to 23 cm. This finding is supported by a study conducted in the public hospitals of Guraghe Zone and Debre Tabor General Hospital.12,20 This could be explained by the deficiency of important micronutrients like vitamins and minerals, which can increase the risk of infection and lead to easy breakage of the membrane. 28 Besides, evidence suggests that vitamin C supplementation after the 14th week of gestation may help prevent PPROM in women who have a history of PPROM. 5 Similarly, women in rural areas have an increased risk of developing PPROM. Those living in rural areas had a threefold greater risk of developing PPROM than those living in urban areas. This phenomenon can be linked to rural women experiencing shorter intervals between pregnancies, with multiple (more than five) pregnancies associated with an increased risk of PPROM.29,30 In addition, poor healthcare access, poor sanitation, higher infection rates, nutritional deficiencies, heavy agricultural work, higher rates of poverty, and limited education can contribute to an increased risk of PPROM.
According to the present study, women who had previously experienced an abortion were also more likely to develop PPROM. Compared to women without a history of abortion, pregnant women with a history of abortion had a 3.78-fold higher probability of experiencing PPROM. These findings are similar to those of a study conducted in the Gedeo Zone 24 and Mekelle City, Tigray, Ethiopia. 23 This is because abortion techniques, including dilatation and curettage, reduce the flexibility of the cervical and uterine tissues, which can lead to premature membrane rupture, cervical insufficiency, and uterine scarring. 31
A history of cesarean section is a significant risk factor for PPROM, with women who had cesarean sections having 2.6 times greater odds of developing this condition than women without cesarean section. This finding was consistent with previous studies conducted at public hospitals in the public hospitals of the Guraghe Zone 20 and Nekemte Town. 32 This is because uterine scarring from previous pregnancies increases the risk of uterine rupture and can increase the likelihood of preterm premature membrane rupture. 33
The study revealed a significant association between PPROM and anemia during pregnancy. Anemic women had a 2.7 times greater risk of having PPROM than their counterparts. The findings align with a Peruvian study that revealed anemia roughly fivefold increased odds of PROM. 13 This may be because anemia reduces the amount of oxygen delivered to tissues and increases the production of the hormone corticotropin-releasing hormone, which increases the risk of premature membrane rupture triggered by hypoxia in tissues. 34 Furthermore, pregnancy-related hypertension is a significant contributor to PPROM, with women with PIH having a 2.65-fold greater risk of developing this condition. The finding is corroborated by a study conducted in the Gedeo Zone 24 and southern Ethiopia. 21 This is because PIH decreases uteroplacental perfusion due to aberrant cytotrophoblast invasion of spiral arterioles, resulting in placental ischemia and maternal vascular endothelial dysfunction with secondary increased endothelin and thromboxane production, increased angiotensin II sensitivity, and decreased vasodilator production.35,36
Limitations of the study
The diagnoses of cases were made by different senior doctors; there may be a misclassification bias. Another drawback of this study may be recall bias; participants in this study may not recall and describe past events. In addition, the socially unacceptable nature of drinking alcohol may lead to more inaccurate responses, underestimating the relationship between PPROM and smoking. The third drawback is selection bias, as some women may not be aware of gestational age, and the small sample size may affect generalization. Furthermore, controlling for all potential confounders was difficult as cases and controls were not matched with relevant variables due to the unmatched case–control design.
Conclusion
The study discovered that a history of UTI, maternal anemia, a previous history of abortion, a previous history of CS, MAUC <23 cm, a rural residence, and PIH were the determinants of PPROM. Therefore, strategies to reduce the occurrence of PPROM should target women in rural areas and aid in the early identification and treatment of UTIs, anemia, and PIH.
Supplemental Material
sj-doc-1-reh-10.1177_26334941251349378 – Supplemental material for Determinants of preterm premature rupture of membranes among pregnant women at public hospitals in the Sidama Region, Ethiopia
Supplemental material, sj-doc-1-reh-10.1177_26334941251349378 for Determinants of preterm premature rupture of membranes among pregnant women at public hospitals in the Sidama Region, Ethiopia by Kidist Gebre, Desalegn Dawit Assele, Ephrem Lejore and Wondwosen Teklesilasie in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
We are thankful that Hawassa University, College of Medicine and Health Sciences, has given us the ethical clearance to conduct this research. We extend our heartfelt thanks to the data collectors and supervisors for their commitment to the successful accomplishment of this research work.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.