
Abstract
Background:
Women’s multidimensional expectations of pregnancy and childbirth can involve many emotions, from joy to fear. It is estimated that most women in Africa suffer from childbirth fear (20%–61.2%). However, to our knowledge, no study has been conducted on fear of childbirth (FOC) in women who had a prior cesarean section, particularly in the study area. This study aimed to fill this gap by assessing the level of childbirth fear and identifying its contributing factors.
Methods:
Institusional based cross-sectional study was conducted among 314 pregnant women with previous cesarean sections from selected public and private health facilities in Dire Dawa. FOC was assessed using the Wilma Delivery Expectancy Questionnaire (W-DEQ-A), which comprises 33 items rated on a 6-point Likert scale, ranging from low to severe FOC, and data were analyzed using multivariable ordinal regression.
Results:
A total of 314 pregnant women participated in this study, with a response rate of 99.3%. Sixty-seven (21.3%, 95% confidence interval (CI): 17%–26%) moderate, 81 (25.8%, 95% CI: 21%–31%) high and severe 30 (9.6%, 95% CI: 6%–13%). The mean W-DEQ score was 54.35 ± 23.6. The mean score for FOC was 54.35 ± 23.6. Being unemployed (adjusted odds ratio (AOR) = 0.442; 95% CI: 0.225, 0.870), having previous pregnancy/labor-related indication for cesarean section (maternal/fetal; AOR = 0.085; 95% CI: 0.020, 0.360, AOR = 0.067; 95% CI: 0.015, 0.297), unplanned pregnancy (AOR = 0.137; 95% CI: 0.057, 0.326), current pregnancy complications (AOR = 4.581; 95% CI: 2.144, 9.788), recurrent cesarean section delivery (AOR = 0.393; 95% CI: 0.175, 0.880) and low and moderated social support of the women (AOR = 109.666; 95% CI: 33.230, 361.926) and (AOR = 5.252; 95% CI: 2.438, 11.314) were factors associated with severe FOC.
Conclusion:
In this study, a quarter of the women with previous cesarean section records suffer from a high degree of FOC. Thus, accommodating counseling during antenatal care visits is needed to address those women who are at a high risk of considerable childbirth fear and its health consequences.
Plain language summary
•
•
•
•
•
Introduction
Fear of childbirth (FOC), also known as tokophobia or maieusiophobia, is a psychological condition characterized by anxiety and fear specifically related to the childbirth process, ranging from mild apprehension to extreme phobic reactions. Tokophobia can manifest in two distinct forms: primary tokophobia, which is an intense FOC without a prior traumatic experience, and secondary tokophobia, which develops following a traumatic birth experience. 1 It is a component of broader pregnancy-related anxiety, which encompasses a range of concerns and fears associated with pregnancy and childbirth. While FOC primarily focuses on the delivery process, pregnancy-related anxiety can include additional worries about the health of the child, pregnancy complications, and postpartum experiences.2 –4
It is a significant challenge many women face during pregnancy, causing emotional distress and increasing the risk of obstetric complications. 5 Globally, FOC rates range from 3.7% to 43%. of women experience FOC, with higher rates observed in industrialized nations. 6 Over the past 30 years, the prevalence of FOC has increased, from 6% in 1980 to 14% in 2017. 7 In Africa, the prevalence of high FOC varies, with figures ranging from 10% to over 60%, as seen in countries like Malawi (20%), 8 Egypt (11.3%), 9 Kenya (58.6%), 10 and Ethiopia (23%). 11 In East Africa, the pooled prevalence of the FOC among pregnant women in East Africa was 27.86%. 12 In Ethiopia, studies have shown that FOC is a significant concern. For example, a study in Arba Minch town reported that 25.3% of women experienced a high degree of fear, while 24.5% had a severe degree of fear. 5 Another study in Eastern Ethiopia found that about a quarter of pregnant women experienced FOC. 11
FOC is linked to various negative health outcomes for both mothers and infants. Maternal complications include infections, bleeding, ruptures, dystocia, preterm delivery, and reluctance to have future pregnancies.13 –16 Fetal risks include distress, low birth weight, preterm, and intrauterine fetal demise.17,18 Furthermore, FOC often drives women to request unnecessary cesarean sections (CS), increasing the risks of complications, medical costs, and social burdens.18,19 The childbirth experience can significantly impact women’s mental health, with traumatic experiences leading to long-term psychological issues such as anxiety and depression. 20 Anxiety during pregnancy, which can be exacerbated by FOC, may also lead to adverse outcomes, such as neonatal abnormalities.20 –22 These psychological issues, in turn, can affect the relationship between the baby and the mother, contributing to a vicious cycle of negative expectations surrounding childbirth. 23
Women with a history of cesarean sections are especially vulnerable to FOC. Their past experiences, which may have been traumatic or complicated, heighten their anxiety about potential complications in future pregnancies. 24 Specifically, they worry about risks such as uterine rupture, placental issues, and broader reproductive health problems associated with repeated cesarean procedures. These concerns extend to the potential impact on both their own health and their child’s well-being.25,26 Despite the rising rates of cesarean sections and associated complications, FOC remains understudied in Ethiopia, especially in Dire Dawa. A meta-analysis of East African studies reveals a regional cesarean prevalence of 24%, with Ethiopia having the highest pooled prevalence at 28.3%. 27 Furthermore, a national study found that the cesarean rate in Dire Dawa was 25.8%. 28 While maternal mortality and morbidity are often highlighted, mental health issues such as FOC remain under-researched. Women with prior CS deliveries are a distinct group with additional fears, so addressing their specific needs is crucial.
Ethiopia’s pregnant population is diverse, with varying delivery histories, cultural practices, and economic backgrounds. These factors influence the degree of FOC.29,30 This highlights the need for localized research and interventions tailored to these women’s unique experiences. By understanding the burden and factors associated with FOC, especially among those with a previous CS, targeted mental health support and care strategies can be developed to improve maternal health outcomes and reduce unnecessary medical interventions. Addressing mental health concerns among pregnant women, particularly those with a history of CS, is vital for enhancing overall maternal and fetal health in Ethiopia. This study aims to fill the gap in knowledge regarding the prevalence and factors influencing FOC in pregnant women with a previous CS in Dire Dawa, thereby contributing to the development of better mental health interventions and policies.
Materials and methods
Study area and period
The study was conducted in Dire Dawa City, Ethiopia, which has an estimated population of 465,000, 50.2% of whom are females. Data collection was carried out from July 20 to August 20, 2023. Dire Dawa provides a range of healthcare services by public and private health institutions. Dil Chora Hospital, which is the biggest public hospital in the city, serves approximately 1.5 million patients. Sabian Hospital, being another public hospital, delivers services to a significant number of individuals. Out of the private institutions, Bilal Hospital is relatively small, with approximately 507 antenatal care (ANC) mothers annually. In addition, Dr. Merid Mersha and Bereket Clinics, which are private organizations, collectively deliver ANC services to more than 2950 mothers annually. This study was conducted within these selected public and private health institutions.
Study design and population
A facility-based cross-sectional study was conducted among pregnant women with a previous history of CS attending ANC services in health facilities within the Dire Dawa city administration. The study population included all pregnant women with a history of CS, excluding those who attended ANC due to medical complications or illness during their pregnancy.
Sample size determination and sampling method
The sample size for this study was determined using the single population proportion formula, considering a 0.05 margin of error, a 95% confidence interval (CI), and an estimated prevalence of 43.76% for FOC based on a study in China. 31 The initial sample size was calculated to be 378. However, since the study population was 1207, which is less than 10,000, a correction formula was applied, resulting in a revised sample size of 287. Adding a 10% nonresponse rate, the final sample size was 316. A systematic random sampling technique was used to select a representative sample. The sample size for each health facility was determined based on the average ANC attendance from the past 6 months. The sampling interval was calculated by dividing the number of ANC attendees by the required sample size for each facility. The first participant was selected randomly, and subsequent participants were chosen at regular intervals (every fourth mother). Data were collected at the end of the service, ensuring the comfort of the pregnant women. The participants were selected proportionally from each selected health facilities.
Data collection methods
Data collection tools and procedures
Data collection was conducted through face-to-face interviews, supplemented by record reviews, using a structured, interviewer-administered questionnaire. Some obstetric factors, such as chronic illness, indication of CS, and current complications, were taken from the chart record. The process was carried out by three diploma-level midwives, with one BSc midwife serving as a supervisor. The questionnaire included four main sections: sociodemographic characteristics and obstetric factors (adapted from related studies).5,13,31,32 And the Wilma Delivery Expectancy Questionnaire (W-DEQ-A) FOC scale. The W-DEQ-A consists of 33 items, with a 6-point Likert scale (ranging from 0 to 5), yielding a total score between 0 and 165. 33 In addition, the Multidimensional Scale of Perceived Social Support was used. This 12-item tool assesses the adequacy of social support from three sources: family, friends, and health professionals, using a 5-point Likert scale (0 = strongly disagree, 5 = strongly agree). 34 The questionnaire was initially prepared in English and later translated into Amharic, Afan Oromo, and Somali. Both data collectors and supervisors received comprehensive training, which was conducted by BSc midwives fluent in Amharic, Afan Oromo, and Somali. These supervisors were trained in the English version of the questionnaire by the principal investigator.
Operational definitions
Low level of FOC: a score of ⩽37 with W-DEQ-A FOC assessing questionnaire. 2
Moderate level of FOC: a score of 38–65 with W-DEQ-A FOC assessing questionnaire. 2
High level of FOC: a score of 66–84 with W-DEQ-A FOC assessing questionnaire. 2
Severe level of FOC: a score of ⩾85 with W-DEQ-A FOC assessing questionnaire. 2
Low social support: mean scale score ranging from 1 to 2.9 with the multidimensional scale of perceived social support questionnaire. 34
Moderate social support: a score of 3 to 5 on the multidimensional scale of the perceived social support questionnaire. 34
High social support: a score from 5.1 to 7 with the multidimensional scale of the perceived social support questionnaire. 34
Data quality control
The questionnaire was initially prepared in English and then translated into Amharic, Afan Oromo, and Somali. To ensure consistency, it was later translated back into English by an independent translator. Data collectors and supervisors received 2 days of training on the data collection tools and procedures. Prior to the actual data collection, the questionnaire was pretested on 5% of the sample size at Delt Hospital, which was outside the study area, to assess its consistency and validity. Based on the pretest results, necessary corrections were made to the questionnaire. Data collectors were closely supervised by the supervisors and the principal investigator. The completeness of each questionnaire was reviewed daily by the principal investigator and supervisors. Double data entry was performed by two data clerks, and the consistency of the entered data was cross-checked by comparing the two separately entered datasets in EpiData.
Data analysis and interpretation
After data collection, the questionnaire was checked for completeness, coded, entered, and cleaned using Epi-Data, and then finally exported to SPSS 24 for analysis. Descriptive statistics and ordinal logistic regression analysis were used to identify associated factors of FOC. Descriptive statistics was used to provide an overall summary and presented using texts, graphs, and tables. Bivariate ordinal regression analysis was done, and variables with p ⩽ 0.25 in the bivariate analysis were included in the final model of multivariable ordinal regression analysis to control for all confounding variables. The direction and strength of statistical association were measured by adjusted odds ratio (AOR) with 95% CI. Finally, in multivariable regression, variables with a p-value less than 0.05 were considered statistically significant. To assess model fitness and multicollinearity of variables, the model fitness, goodness of fit test, and variance-inflated factor were used, respectively. The data was normally distributed, and no multicollinearity was diagnosed; the model fitness and goodness of fit test were well-fitted. The Cronbach’s alphas were 0.86, 0.70, and 0.81 for W-DEQ, obstetrics-related questionnaire, and social support questionnaire, respectively, and the data were reliable with a Cronbach’s alpha score of good internal consistency.
Results
Sociodemographic characteristics of the respondents
The participants’ ages ranged from 20 to 43 years, with a mean age of 29.4 years (SD ±5.5). The majority (51%) of the pregnant women were in the 25–29 age group. All of the women were married. More than half of the study participants (58.3%) were unemployed, and only 15.6% had a college diploma or higher (Table 1).
Sociodemographic status of pregnant women with previous CS delivery attending ANC at selected public and private health institutions of Dire Dawa city administration, 2024 (n = 314).

CS: cesarean section; ANC: antenatal care.
Obstetrics characteristics of the participants
While all patients experienced a prior CS, in their additional previous pregnancies, 78 (24.8%) had also experienced a vaginal delivery, and 124 (39.5%) had a history of abortion. The majority of the women, 269 (85.7%), had undergone an emergency CS, and 119 (37.9%) had more than one CS delivery. Regarding the current pregnancy, 204 (65%) participants confirmed that their pregnancy was planned. Most of the women were Para 1 (47.1%) or Para 2 (34.1%). A total of 208 (66.2%) women were in their third trimester. The majority, 263 (83.8%), had not experienced any complications during their pregnancy, while 51 (16.2%) reported current pregnancy complications. When asked about their preferred mode of delivery, 136 (43.3%) expressed a desire for vaginal delivery. Concerning chronic health conditions, 59 (18.8%) participants reported having chronic diseases, including chronic hypertension (6.7%), diabetes mellitus (5.4%), heart disease (1.9%), and asthma (4.8%). In terms of physical activity, 205 (65.3%) women claimed to engage in regular physical exercise (Tables 2 and 3). Regarding CS indications, for over half of the women (54.1%), the indication for a previous CS was maternal-related, while fetal-related indications accounted for 130 (41.4%) cases. Among the fetal-related complications, fetal distress was the most common (15.6%), followed by a large baby (13.4%) and mal-presentation (15.9%). Among maternal indications, prolonged labor (15%) was the most common indication, followed by hypertensive disorders (14.30%; Figure 1).
Obstetrics characteristics of pregnant women with previous CS delivery attending ANC at selected public and private health institutions of Dire Dawa city administration, 2024 (n = 314).

CS: cesarean section; ANC: antenatal care.
Bivariable and multivariable ordinal logistic analysis for factors associated with severe FOC among pregnant women with previous CS delivery attending ANC at selected public and private health institutions of Dire Dawa city administration, 2024 (n = 314).

AOR: adjusted odds ratio; COR: crude odds ratio; CI: confidence interval; 1: references category; CS: cesarean section; FOC: fear of childbirth; ANC: antenatal care.
indicates significant.

Maternal-related indications for previous CS delivery among the participants attending ANC visits.
Magnitude of fear of childbirth
In this study, 136 (43.3%, 95% CI: 38%–49%) had low FOC, 67 (21.3%, 95% CI: 17%–26%) moderate, 81 (25.8%, 95% CI: 21%–31%) high and severe 30 (9.6%, 95% CI: 6%–13%). The mean W-DEQ score was 54.35 ± 23.6 (Figure 2).
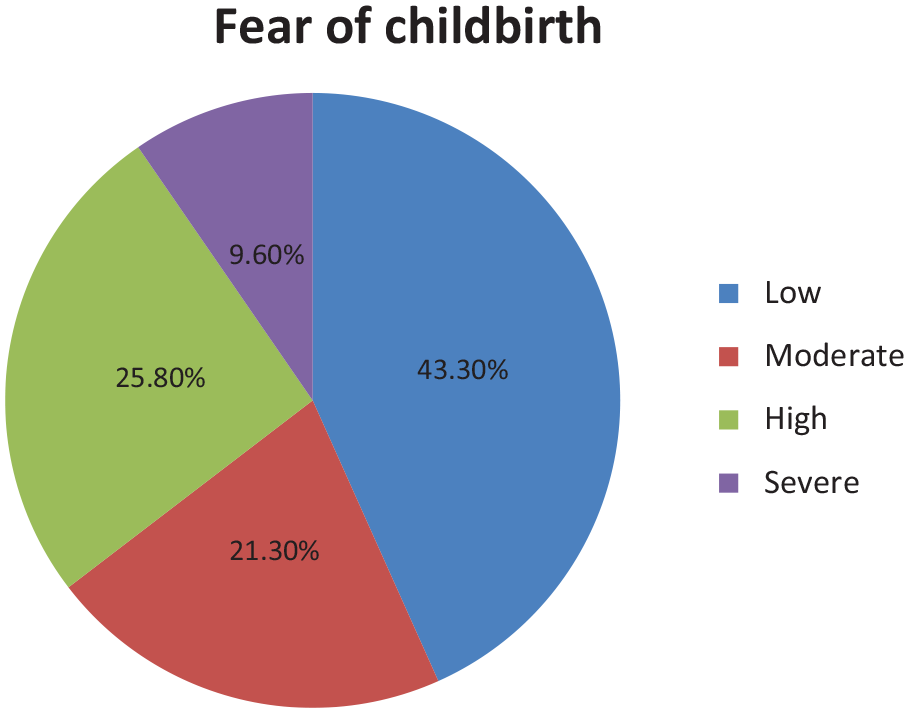
Prevalence of FOC of pregnant women with previous CS delivery attending ANC at selected public and private health institutions of Dire Dawa city administration, 2024 (n = 314).
Social support
In this study, the combined average score of social support received by participants from their family, husband, friends, and healthcare professionals was categorized as follows: low support (95, 30.3%), moderate support (104, 33.1%), and high support (115, 36.6%). When examining support from each source separately, only 6 (1.9%) participants reported receiving high support from healthcare professionals. In contrast, half of the study participants, 157 (50%), indicated receiving high support from their spouses. In addition, 198 (63.1%) women reported receiving high support from their family, and 106 (33.8%) reported high support from their friends (Figure 3).

Social support of pregnant women with previous CS delivery attending ANC at selected public and private health institutions of Dire Dawa city administration, 2024 (n = 314).
Factors associated with fear of childbirth
In the bivariate ordinary logistic regression, several variables, including occupational status, planned pregnancy, maternal chronic disease, regular physical exercise, current pregnancy-related complications, preferred mode of delivery, number of previous CS deliveries, and social support, had p-values less than 0.2, making them candidates for multivariable logistic regression analysis.
The results from the multivariable logistic regression analysis showed that certain factors were associated with a reduced likelihood of higher FOC. Specifically, being employed (AOR = 0.442; 95% CI: 0.225, 0.870), having a planned pregnancy (AOR = 0.137; 95% CI: 0.057, 0.326), and having only one previous CS delivery (AOR = 0.393; 95% CI: 0.175, 0.880) all reduced the chances of developing moderate to moderate-to-severe fear.
On the other hand, several factors were associated with an increased likelihood of moderate-to-severe fear. Women with pregnancy-related complications had nearly five times higher odds of experiencing higher fear (AOR = 4.581; 95% CI: 2.144, 9.788). In addition, women with low social support were significantly more likely to experience higher FOC (AOR = 109.666; 95% CI: 33.230, 361.926), and those with moderate social support also had a higher chance of FOC (AOR = 5.252; 95% CI: 2.438, 11.314). These findings suggest that employment, planned pregnancies, fewer previous CS deliveries, pregnancy complications, and social support are key factors influencing the likelihood of moderate-to-severe fear.
Discussion
This study aimed to assess the FOC and its associated factors among pregnant women with previous CS delivery at selected health facilities in Dire Dawa, Ethiopia. The prevalence of high levels of FOC in this study was found to be 25.8%, which aligns with the prevalence rates of the eastern part of Ethiopia and south Ethiopia. A study from Eastern Ethiopia reported a 19.3% prevalence of FOC, while findings from Southern Ethiopia showed a prevalence of 25%, aligning with our results.5,11 However, the prevalence of severe FOC was notably higher in these studies, at 23.3% and 24.5%, respectively, compared to only 9.6% in our study. This variation may be due to differences in study populations, as severe FOC often focuses on labor pain, whereas these studies included all women regardless of their childbirth history or mode of delivery. Conversely, our results align with a study from Egypt, which reported an 11.3% prevalence of severe FOC. 9 The average mean score for FOC in our study was 54.35 (SD ±23.6), consistent with studies conducted in China, which reported the average of FOC as 43.76 (SD ±5.27). 31 This consistency suggests that the level of childbirth fear among women in low-income countries is similar to that in high-income countries, despite differences in birth rates, medical.
This study suggests that employed women are less likely to experience higher levels of fear compared to unemployed women. Specifically, they have approximately 56% lower odds of reporting moderate-to-severe FOC than their unemployed counterparts. This finding aligns with studies from northern Ethiopia and Malawi, where being unemployed was determined to be responsible for women to the development of FOC.35,36 Unemployment often brings financial insecurity and uncertainty about the future, leading to increased stress and anxiety. Unemployment can also have negative health consequences. Those who are unemployed report feelings of depression, anxiety, low self-esteem, demoralization, worry, and physical pain. Unemployed individuals tend to suffer more from stress-related illnesses, such as high blood pressure, stroke, heart attack, heart disease, and arthritis. 37 On the contrary, other studies reported that employed women were more likely to experience childbirth fear and seek treatment for psychological well-being. 38 Harmful workplace conditions, including psychosocial stress, workplace injuries, exposure to harmful chemicals, interpersonal conflicts, and long working hours, can increase the risk for negative health outcomes. 37
Furthermore, women who have had one previous cesarean section are less likely to experience higher levels of fear compared to those who have had more than one cesarean delivery. The odds of moderate-to-severe FOC are reduced by approximately 61% in those who have had only one CS. This finding is supported by the study conducted in China, where the number of CS and experience with previous CS were significantly associated with FOC. First, a CS is a traumatic surgical procedure, and women thus bear potential risks. 31 Experience with a previous CS affects women’s future reproductive ability and increases their risk of ectopic pregnancy and placental implantation. Second, repeated CSs (⩾2) may cause uterine rupture in the perinatal period because of a scarred uterus and pose a threat to the child. 31 Cesarean deliveries are expected to carry higher risks for mothers’ mental health compared to natural deliveries. Indeed, women who have a cesarean delivery are more likely to suffer from physical pain after childbirth and have longer and more difficult postnatal recovery, both conditions that also affect their psychological well-being. 39
Women experiencing current pregnancy-related complications are significantly more likely to report higher levels of fear regarding childbirth. Specifically, they have over four times the odds of experiencing moderate-to-severe fear compared to those without complications. As pregnancy-related complications have adverse outcomes and are related to maternal and neonatal morbidity as well as mortality, women who had pregnancy-related complications during the interview were more likely to have a FOC than those who had not. This finding is supported by the study findings from the research conducted in Arba Minch and Turkey.5,40
Unplanned pregnancy was also one factor associated with FOC. In the current study, unplanned pregnancy was strongly associated with FOC, which is supported by findings from a study conducted in Arba Minch, Eastern Ethiopia, Thailand, Turkey, Bangkok, and a study from six European countries.5,6,40,41 The reason behind this may be due to an increase in stress among women with an unplanned pregnancy, in addition to pregnancy physiological maladaptation. Consistent with other studies from Ethiopia,5,11,32 this study showed that having low and moderate social support was strongly associated with FOC. Women with low social support are extremely more likely (over 100 times) to experience high levels of fear compared to those with high social support. Similarly, Women with moderate social support also have significantly increased odds (over five times) of experiencing moderate-to-severe levels of fear compared to those with high social support. Social support during pregnancy can alleviate emotional and physical pressures, improving the well-being of the mother and child. 42 Perceived support can prevent a psychological or physiological stress reaction from arising when a potentially stressful event occurs. 42 Consequently, perceived support may increase the perception that individuals can cope with negative events. 42 Perceived social support can intervene between the event of a stress reaction and the onset of a pathological process by reducing the stress reaction. Pregnant women should experience a valued and wide variety of emotional support from different sources, including their husbands, families, friends, and healthcare professionals. 42
Strength and limitation
This study addresses both public and private health institutions, making the findings representative of all women who have had a previous CS. In addition, the study explores previously untouched areas of obstetric-related problems, providing baseline data for interventions proven to improve maternal outcomes and reduce FOC, particularly among women with a previous CS history. However, a limitation of the study is that its results are compared with studies conducted among all women, which may not fully capture the specific dynamics of FOC in this targeted population.
Conclusion
A quarter of women with a history of CS in Dire Dawa City Administration experience a high degree of FOC, which is strongly linked to unemployment, current pregnancy complications, multiple prior CS deliveries, unplanned pregnancies, and insufficient social support from family, partners, friends, and healthcare providers. Addressing these factors through enhanced social support networks, accessible psychological care, and economic empowerment initiatives can significantly reduce FOC levels. Comprehensive interventions must involve healthcare systems (e.g., integrating prenatal education that incorporates local CS statistics to clarify risks and benefits), community programs to bolster emotional and practical assistance, and policies to alleviate financial stressors. In addition, postpartum care should prioritize structured discussions on physical recovery, mental health support, and future pregnancy planning, including contraceptive counseling and vaginal birth after cesarean options. Together, these strategies can improve maternal mental health outcomes and mitigate childbirth-related anxiety in the study area.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251349628 – Supplemental material for Rates of fear of childbirth after previous cesarean section in Dire Dawa City, Ethiopia
Supplemental material, sj-docx-1-whe-10.1177_17455057251349628 for Rates of fear of childbirth after previous cesarean section in Dire Dawa City, Ethiopia by Ayantu Kedir, Habtamu Bekele and Maleda Tefera in Women’s Health
Footnotes
Acknowledgements
We would like to express our deepest gratitude to Haramaya University for providing funding for conducting this research. We are also indebted to both public and private health facilities for the cooperation and assistance they provided us throughout this study.
Author’s Note
Maleda Tefera is now affiliated to Department of Midwifery, College of Health and Medical Sciences, Dire Dawa University, Ethiopia.
Ethical considerations
Before starting the data collection process, ethical clearance was secured by Haramaya University Institutional Health Research Ethics Review Committee (IHRERC) with No. IHRERC131/2023.
Consent to participate
An official letter was written to each selected health facility of Dire Dawa City and the Dire Dawa health bureau by Haramaya University College of Health and Medical Sciences and delivered to each health facility director to get permission. Participants were informed about the purpose of the study and the privacy of the information. Informed, voluntary, written, and signed consent from participants in the study was obtained before conducting the interview. For illiterate participants, the consent form was read aloud to them, and their consent was documented using a fingerprint signature. For this, a page of the participants’ information sheet and a page of the consent letter form were attached to each questionnaire. The name of the respondents was not addressed for the sake of confidentiality.
Consent for publication
Not applicable.
Author contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data can be made available upon a reasonable request directed to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.