
Abstract
Purpose:
To investigate the effectiveness of perturbation-based training (PBT) on balance and balance confidence in patients with stroke.
Methods:
Systematic searching was performed from inception to November 2021. The inclusion criteria were RCTs assessed the effectiveness of PBT in patients with stroke. Data regarding participants, intervention parameters, outcome measures, follow-up, and main results were extracted. The outcomes were balance and balance confidence. Methodological quality and quality of evidence were assessed using the Physiotherapy Evidence Database (PEDro) scale and the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system; respectively.
Data analysis:
A total of 7 articles )271 patients) were included. A meta-analysis using a random-effect model was performed on 6 studies. Standardized mean difference (SMD) with a 95% confidence interval was calculated for balance and balance confidence.
Results:
PEDro scale revealed 5 good-quality and 2 fair-quality studies. The currently available evidence showed significant effect of PBT in improving balance (SMD 0.60 [95% CI 0.15-1.06]; P = .01; very low-quality evidence) and non-significant in improving balance confidence (SMD 0.11 [95% CI −0.24 to 0.45]; P = .55; low-quality evidence).
Conclusion:
PBT may improve balance in patients with stroke, however its effect on balance confidence was limited. The quality of the evidence was low or very low with little confidence in the effect estimate, which suggests further high-quality trials are required.
Registration:
PROSPERO registration number (CRD42021291474).
Introduction
Stroke is a prevalent cerebrovascular disease, which leads to high morbidity, mortality, and disability rates that imposes a significant financial load on society and families.1,2 Diminished balance control, low balance confidence, and high number of falls are common consequences of stroke, which influence patients’ quality of life and reduce their physical activity as a strategy to avoid falls, thus causing further function and health status disorders.3-5
Patients with stroke are at high risk of falls during the acute and chronic phase, even when they achieve independent ambulation. 6 Falling happens when an individual is unable to recover from a postural perturbation or loss of balance.7,8 The capability to regain balance and avoid falling is determined by the efficacy of balance reactions. These reactions are divided into 2 types, fixed support reactions such as swaying around the ankles or hips to maintain balance against minor postural perturbations.9,10 On the other hand, change-in-support reactions involve fast stepping and grasping actions to defend against major postural perturbations. 11
There are many and varied balance exercise programs that are usually intended to improve balance control in static such as standing with a small base of support, or during dynamic movement like sit-to-stand exercise.12-15 These types may decrease the probability of losing balance in daily life and prevent falls. Nonetheless, accidental loss of balance is an unavoidable consequence of ambulation, so the capability to react rapidly after losing balance (ie, reactive balance control) is crucial for preserving balance and preventing falls. 9 Therefore, it is possible that more specific exercises focused on the mechanism of occurrence of falls that enhance control of rapid reactive movements might be more effective for falls prevention, such as perturbation training.16-18
Perturbation-based training (PBT) is a novel balance training in which individuals are repetitively subjected to postural perturbations to induce rapid balance reactions, enabling the subject to improve control of these reactions with practice. 18 It differs from other balance exercise programs as it is particularly to improve reactive balance control to avoid a fall following a balance failure in real life. 19 Studies have shown a beneficial effect of PBT as it can improve voluntary movements’ speed and control, 17 enhance rapid balance reactions,20,21 and decrease fall occurrence.20-22
Many trials are evaluating the effectiveness of PBT in the treatment of patients with stroke. However, the effect of PBT on balance and balance confidence has not been conclusively determined. In addition, prior reviews focused mainly on the effects of PBT in young and older healthy adults and individuals with Parkinson’s disease,18,23-25 there is no review focused on PBT in the treatment of patients with stroke. Therefore, the purpose of this systematic review and meta-analysis was to investigate the effectiveness of perturbation-based training (PBT) on balance and balance confidence in patients with stroke.
Methods
Study design
This study involved systematic review and meta-analysis conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 26 The review’s protocol was registered in the International prospective register of systematic reviews (PROSPERO) with a registration number (CRD42021291474).
Search strategy
A systematic search for original journal articles was performed from inception to November 2021 via following databases and registers: MEDLINE, PubMed, Web of Science, Scopus, EBSCO, Science direct, Physiotherapy Evidence Database (PEDro), REHABDATA, the Cochrane Central Register of Controlled Trials (CENTRAL), and RCT registration website (http://www.ClinicalTrials.gov). Moreover, searching was done via other methods including 2 grey literature databases (Grey Literature Report and Open Grey), website (Research Gate), and reference lists of all eligible studies.
In literature, the terminology used to describe PBT is varied and inconsistent. Some researchers used perturbation-based training, while others used terms such as reactive balance training, gait-slip, or gait-trip training. Moreover, there are no related Medical Subject Headings (MeSH) within MEDLINE database to precisely involve the PBT content. Therefore, searching via methods other than database and registry was performed to find all possible eligible studies. The search was performed in all databases according to their specific Boolean criteria and included the following terms: (perturbation OR slip OR trip OR reactive balance) AND (training OR practice OR rehab OR exercise) AND (stroke OR cerebrovascular accident OR CVA) (Table 1).
Search terms and methods (PubMed).

Eligibility criteria
Studies were included if they met the following criteria: (1) The study design was RCT; (2) involved PBT either the perturbation applied through equipment (eg, moving platform) or manually (eg, therapist push); (3) included participants with stroke (>18 years old), no restriction on sex and race; (4) must have measured the primary outcome which is balance, while balance confidence considered as a secondary outcome; (5) written in English with available full text.
Studies were excluded if they (1) were non RCT (case reports, case series, observational, cross-sectional) and trials without a control group; (2) involved a control group that received any type of perturbation training; (3) assessed the PBT effectiveness with healthy subjects or other neurological diseases; (4) did not measure balance.
Study selection
Two reviewers (NA&AE) independently completed the initial review including the title and abstract review to assess their eligibility against the defined inclusion and exclusion criteria. Duplications in the search results were removed by using EndNote 20 software for windows. If the abstract did not include sufficient information, full text was screened. Then, all studies that matched the inclusion criteria were carefully assessed for final decision and any discrepancies were resolved by another reviewer (MA) in a consensus meeting. Moreover, reference lists of the included articles were screened to find additional studies that might be eligible for inclusion in the review. These articles were also screened.
Data extraction
A standardized form was used to extract the data from each included study. The following data were extracted: authors’ names, publication year, participants characteristics (sample size, sex, age, stage of the disease), outcome measures used, experimental and control interventions (type of training, frequency, and duration of sessions, duration of the training program), follow-up, and main results. The content of the extracted data is presented via tables.
In order to conduct the meta-analysis, sample size, mean, and standard deviation of the experimental and control groups were extracted. If any study results were not reported in form of mean and standard deviation, the study’s authors were contacted to obtain those data.
Evaluation of methodological quality
Studies were rated for methodological quality using the PEDro scale which is commonly used in systematic reviews as a reliable tool to assess the risk of bias of randomized controlled trials, 27 it was developed by the Physiotherapy Evidence Database (PEDro). 28 This scale is dichotomous (yes/no) and involves 11 items. The total score is 10 as criteria one uncounted in the overall score. 28 Included studies were rated according to the following criteria: excellent quality (9-10), good quality (6-8), fair quality (4-5), or poor quality (⩽3). 29 The evaluation of the methodological quality was performed by 2 independent reviewers (AE & TS). A third reviewer (MA) was needed for reviewing the discrepancy in the score by the 2 reviewers if present.
Quality of evidence
To assess the quality of evidence, Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system was used. GRADE is not only a rating system; it offers a clear and organized process for developing and presenting evidence summaries. Grading quality of evidence was performed according to GRADE rating standards as following “High quality,” “Moderate quality,” “Low quality” or “Very low quality,” each of these 4 levels have a description which concentrate on the implications of the degrees of evidence for future research (the less the quality, the more probability that further research would change the estimates of the effect and the confidence in these estimates).30-32
Decision for downgrading the quality of evidence was based on the following criteria: (1) Study limitations (risk of bias): evidence is downgraded by one level (serious limitation) if there is one study rated as fair quality, while downgraded by 2 levels (very serious limitation) if there is more than one study rated as fair quality, or one study rated as poor quality in PEDro scale. (2) Inconsistency: evidence is downgraded if there were an unexplainable high heterogeneity (I 2 ⩾ 75%). 33 (3) Indirectness: evidence is downgraded if there were considerable discrepancies between the population, intervention, or outcomes measured in the included studies. 34 (4) Imprecision: evidence is downgraded if the sample size was small (<400 participants) and/or wide CI that overlaps no-effect line. 35 (5) Publication bias: evidence is downgraded if the included studies involved only statistically significant results with absence of negative results. 36
Data analysis
Data analysis was performed based on PRISMA guidelines in qualitative and quantitative methods. 26 Tables were used to represent the qualitative (descriptive) data, while quantitative synthesis was performed through meta-analysis using Review Manager (version 5.4) software for windows. The 2 outcomes of interest were balance (primary outcome) and balance confidence (secondary outcome).
The random-effects model was used in the meta-analysis. Moreover, the overall effect size with a 95% confidence interval was calculated based on the standardized mean difference (SMD) of the individual studies. Effect size can be categorized as follow: small (0.2), medium (0.5) and large (0.8). 37 Additionally, statistical heterogeneity across trials was assessed with the I 2 statistics, and it is graded as : low (I 2 ⩽ 25%), medium (I 2 26%-50%) and high(I 2 ⩾ 75%). 38 Furthermore, subgroup analysis was conducted to investigate the effectiveness of PBT alone or combined with other exercises versus control interventions. Also, another subgroup analysis was performed to test whether stage of stroke impacts the effect of PBT in patients with stroke or not.
Result
Study selection
The systematic search identified 623 records via databases (n = 523) and registers (n = 100). After deletion of duplicated records (n = 269), 354 records’ titles and abstracts were screened. A total of 23 articles were initially eligible and after the full-text screening, only 4 of them met the inclusion criteria,39-42 while 19 articles were excluded because they were not randomized controlled trials (n = 17), did not measure balance (n = 1) and both groups underwent PBT (n = 1). A total of 104 records were identified via other methods. After the exclusion of 100 records, 4 studies were screened and only 3 studies met the inclusion criteria,20,43,44 while one study was excluded because it was pre-printed and not peer-reviewed yet. Consequently, 7 articles were included in the review, and only 6 of them were included in the meta-analysis.20,39-43 The steps of searching and selection procedure using the PRISMA flow diagram were represented in Figure 1.

Flow diagram of the study selection process.
Study characteristics
Seven studies with a total of 271 participants were included in this review, 134 participants were in experimental groups and 137 in control groups. All these studies were published during the period from 2005 to 2020 and included both genders,20,39-43 only one study did not mention sample’s gender. 44 Two studies investigated the effect of PBT in patients with subacute stroke40,43 4 studies in patients with chronic stroke,20,39,41,42 however Kumar et al 44 did not report the participants’ stage of stoke. According to definition of stroke’s stages by Bernhardt et al 45 the subacute stage includes 7 days to 6 months and chronic stage > 6 months from stroke onset.
All included studies evaluated balance either functional,20,39-41,43,44 dynamic,39,41,42 or reactive. 40 Other measures were performed such as standing postural reflexes 20 and step reaction time. 20 Moreover, one study performed a robot-based evaluation for static, dynamic, and reactive balance, proprioceptive control, and sit-to-stand tests. 41 In addition, balance confidence was assessed in 4 studies.20,39,40,42 Monitoring and follow-up periods ranged from 1 to 12 months in 5 studies,20,39-42 while the other 2 studies did not follow-up the patients.43,44
The intervention in 3 studies focused only on PBT,39,40,42 while in other studies, PBT was involved as part of an exercise program.20,41,43,44 The control groups’ intervention was conventional/traditional physiotherapy treatment,39,41,43,44 stretching and weight-shifting, 20 weight shifting and/or gait training, 40 walking 42 as shown in Table 2.
Characteristics of included studies.
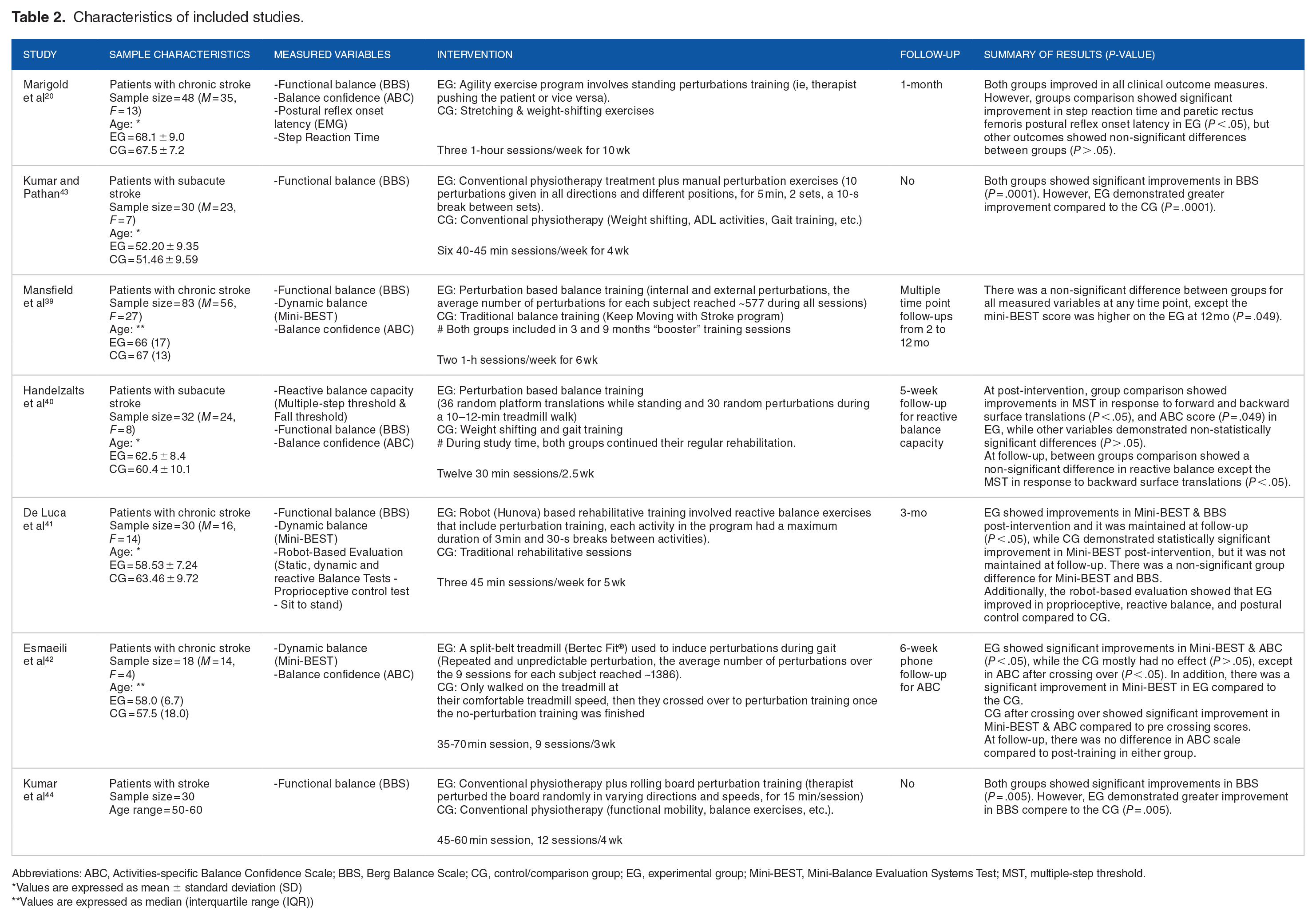
Abbreviations: ABC, Activities-specific Balance Confidence Scale; BBS, Berg Balance Scale; CG, control/comparison group; EG, experimental group; Mini-BEST, Mini-Balance Evaluation Systems Test; MST, multiple-step threshold.
Values are expressed as mean ± standard deviation (SD)
Values are expressed as median (interquartile range (IQR))
Risk of bias assessment
PEDro scale was used to assess the methodological quality of the included studies; scores ranged from 5 to 8 out of a maximum of 10. Five studies were rated as good quality,20,39-42 and 2 studies were rated as fair quality.43,44 All included studies did not perform subjects’ and therapists’ blinding. Additionally, the least met criteria were the allocation concealment in 5 studies (71%),40-44 and intention to treat analysis in 4 studies (57%).20,41-43 Thus, the highest risk of bias for these studies was selection bias and performance bias. Details of the methodological quality appraising of the included studies are shown in Table 3.
Methodological quality assessment of included studies (PEDro scale).

Not included in the final score
Data synthesis
A descriptive synthesis was performed for all included studies and each study’s findings are presented in Table 2. Different types of balance were assessed in the included studies. Functional balance was assessed by berg balance scale (BBS) in 6 studies,20,39-41,43,44 2 studies43,44 found that there was a significant improvement in PBT compared to control (P < .05), while the other 4 studies20,39-41 found a non-significant difference (P > .05). Moreover, dynamic balance was evaluated by mini-balance evaluation systems test (Mini-BEST) in 3 studies,39,41,42 2 studies reported better outcomes in favors of the PBT (P < .05),39,42 but a study by De Luca et al 41 found a non-significant group difference. Additionally, De Luca et al used a robot-based evaluation which showed that PBT improved in reactive balance and postural control compared to control (P < .05), indicating an increased trunk control with decreased compensatory strategies at the end of the training.
Assessment of balance confidence was done in 4 studies using the Activities-specific Balance Confidence Scale (ABC),20,39,40,42 only one of them reported that there was a significant group difference. 40
Meta-analysis
Six studies were included in the meta-analysis, and subgroup analysis was performed according to addition of other exercises to PBT (Figures 2 and 4) and stage of stroke (Figures 3 and 5). A Study by Kumar et al 44 was excluded because standard deviation was missing. Furthermore, 6 themes were identified to assess the quality of evidence (GRADE) and presented with the pooled analysis in Table 4.

Forest plot for the effect of PBT alone or combined with exercise on balance.

Forest plot for the effect of PBT on balance in subacute and chronic stroke.
Quality of evidence (GRADE).
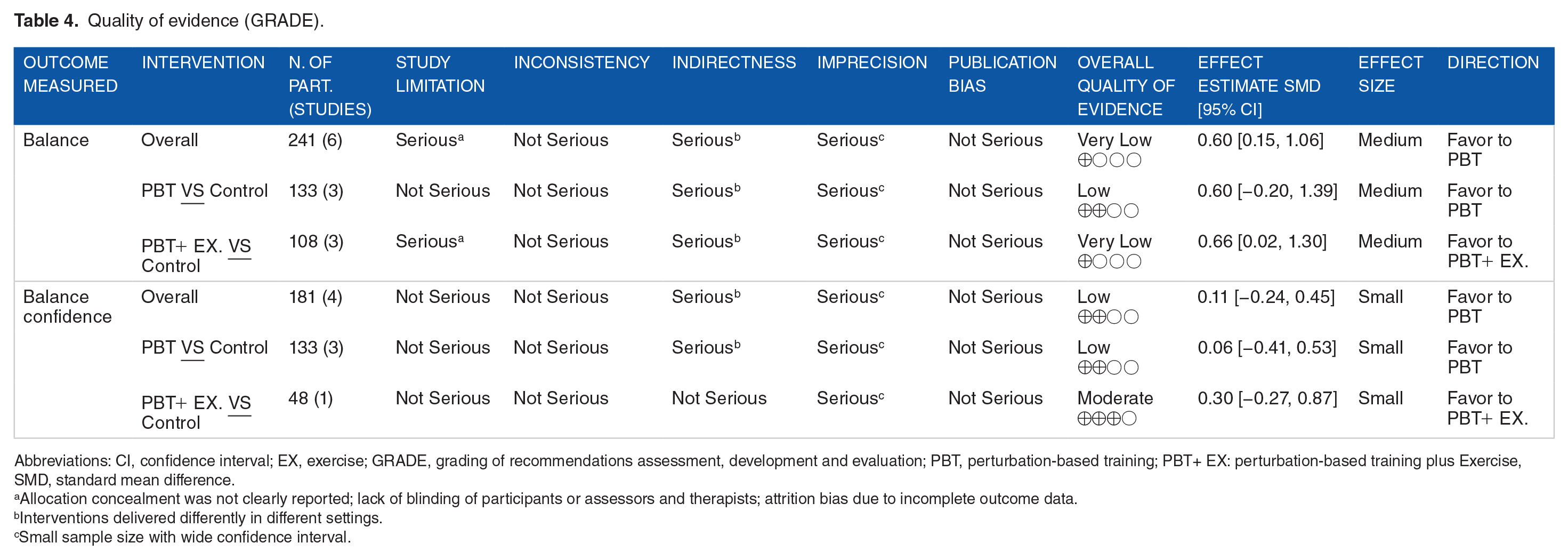
Abbreviations: CI, confidence interval; EX, exercise; GRADE, grading of recommendations assessment, development and evaluation; PBT, perturbation-based training; PBT+ EX: perturbation-based training plus Exercise, SMD, standard mean difference.
Allocation concealment was not clearly reported; lack of blinding of participants or assessors and therapists; attrition bias due to incomplete outcome data.
Interventions delivered differently in different settings.
Small sample size with wide confidence interval.
Effects of perturbation-based training on balance
Six studies with 241 participants were eligible to be included in this analysis, 3 trials were PBT VS Control39,40,42 3 trials were PBT+EX. VS Control.20,41,43 The overall effect was favor to PBT in terms of improving balance in patients with stroke with significant difference and medium effect size (SMD 0.60 [95% CI 0.15-1.06]; P = .01) (Figure 2).
Subgroup analysis according to addition of other exercises to PBT indicated that patients with stroke who underwent PBT with other exercises were improved significantly more than control (SMD 0.66 [95% CI 0.02-1.30]; P = .04). However, PBT alone did not improve balance significantly compared to control, despite the presence of medium effect size (SMD 0.60 [95% CI −0.20 to 1.39]; P = .14) (Figure 2).
In addition, Subgroup analysis according to stage of stroke revealed that the effect size was greater for patients with subacute stroke (SMD 0.83 [95% CI −0.06 to 1.72]; P = .07) more than those with chronic stroke (SMD 0.50 [95% CI −0.05 to 1.05]; P = .08) (Figure 3).
The variability between the 6 studies was evaluated with I 2 and it showed presence of medium heterogeneity (I 2 = 63%). Furthermore, subgroup analysis demonstrating existence of heterogeneity approximately similar to that found across the whole 6 studies indicated that addition of other exercises to perturbation training and stage of stroke did not explain the heterogeneity in the overall effect estimate (Figures 2 and 3).
The quality of evidence (GRADE) was rated as “Very low” quality for overall effect on balance due to serious risk of bias, indirectness, and imprecision. Additionally, PBT versus control was rated as “Low” quality due to serious indirectness and imprecision, while PBT+EX. versus control was rated as “Very low” quality due to serious risk of bias, indirectness, and imprecision (Table 4).
Effects of perturbation-based training on balance confidence
Four studies with 181 participants were eligible to be included in this analysis, 3 trials were PBT VS Control,39,40,42 one trial was PBT+EX. VS Control. 20 The forest plot showed non-significant favor to PBT in terms of improving balance confidence with small effect size (SMD 0.11 [95% CI −0.24 to 0.45]; P = .55).
Subgroup analysis according to addition of other exercises to PBT showed that the effect size was greater for patients who underwent PBT with other exercises (SMD 0.30 [95% CI −0.27 to 0.87]; P = .31) more than PBT alone (SMD 0.06 [95% CI −0.41 to 0.53]; P = .81) (Figure 4).

Forest plot for the effect of PBT alone or combined with exercise on balance confidence.
In addition, Subgroup analysis according to stage of stroke showed medium effect size of PBT in patients with subacute stroke (SMD 0.54 [95% CI −0.17 to 1.25]; P = .14), while in chronic stroke there was a small effect size of control interventions, thus because study by Mansfield et al. has the largest weight on the results and showed favor to control (SMD −0.02 [95% CI −0.34 to 0.30]; P = .91) (Figure 5).

Forest plot for the effect of PBT on balance confidence in subacute and chronic stroke.
The variability between studies evaluation showed presence of low heterogeneity( I 2 = 23%). However, subgroup analysis according to stage of stroke demonstrating absence of heterogeneity in chronic subgroup (I 2 = 0%) which indicated that differences in the stage of stroke may explain the heterogeneity in the overall effect estimate (Figure 5).
The quality of evidence (GRADE) was rated as “Low” quality for overall effect on balance confidence due to serious indirectness and imprecision. Additionally, PBT versus control was rated as “Low” quality due to serious indirectness and imprecision, while PBT+EX. versus control was rated as “Moderate” quality due to serious imprecision (Table 4).
Discussion
The results of this systemic review and meta-analysis suggests that PBT may be associated with a significant moderate improvement in balance in patients with stroke based on meta-analysis results which evaluated the short-term effects of PBT (SMD = 0.60; very low-quality evidence). However, effects of PBT on improving balance confidence was not statistically significant compared to control and demonstrated small effect size (SMD = 0.11; low-quality evidence).
Lack of significant results in balance confidence can be explained by presence of limited number of studies and small sample size which probably leads to failure in reaching sufficient statistical power that detects between-group differences. Additionally, study by Mansfield et al. has the largest weight on the results and showed favor to control.
Outcome measures used in the analyses are Berg Balance Scale (BBS) and Mini-Balance Evaluation Systems Test (Mini-BEST) as balance measures. While Activities-specific Balance Confidence scale (ABC) was used as a balance confidence measure. All these scales are reliable and valid tools to be used in patients with stroke.46-49
Significant improvement of balance may translate to increased ability to respond to an unpredicted loss of balance in real-life situations, thereby reducing falls.21,50 This finding was consistent with previous reviews that demonstrated beneficial effects of PBT in fall reduction among young and older healthy adults and individuals with Parkinson’s disease,18,23,25 and contrary to the systematic review’s result by Hulzinga et al which found a non-significant improvement in balance when comparing gait perturbation training with non-perturbation training in Parkinson’s disease and healthy older adult. 24 Although PBT showed a favorable effect in balance, 2 included studies showed a non-significant reduction in falling rates over 1-year post-training.20,39 This discrepancy may result from the small sample size that leads to inability to reach sufficient statistical power.
The ABC scale measures fear of falling by evaluating individual’s confidence to maintain balance and remain steady while performing various functional tasks.51,52 Therefore, improvement in balance confidence measured by ABC Scale indicated less fear of falling which is a major psychological barrier that may limits an individual’s contribution in everyday activities, limits functioning, and increases the risk of falls. 40 A previous study reported that balance confidence was a significant contributing factor of falls in chronic patients with stroke. 53
However, there was no additional favorable effect of PBT over other control interventions in improving balance confidence. As the PBT may be insufficient to produce considerable effect, addition of some psychological interventions such as cognitive behavior therapy (CBT) to PBT could produce significant effect in improving balance confidence. Previous study stated that CBT appears to be a feasible adjuvant therapy to increase the therapeutic effects of physiotherapy intervention on fear of falling reduction. 54 Consequently, it is necessary to investigate the effect of addition of psychological interventions to PBT in future studies.
Possible explanations for the mechanism underlying patients’ improvement after perturbation training can be clarified at functional level as experiencing various balance perturbations can improve the usage of sensory feedback, which sends information about the direction and magnitude of body imbalance to select and scale appropriate reactive movements which help in balance recovery from random perturbations. 55 In addition, the improvement can be explained at neural level. Patel et al found increased prefrontal and parietal cortices activation following repeated slip-like perturbations training during walking, perturbation training can reinforce those cortical areas connectivity which leads to rapid selection and scaling of proper compensatory movements to cope with a particular balance perturbation. 56
Additionally, the effect of PBT was greater in patients with subacute stroke more than chronic, this because patients improved significantly in the first few weeks after a stroke and reach a relative plateau around 3 months and less meaningful recovery thereafter,57,58 and after 6 months recovery is usually limited. 59 Consequently, researchers and clinicians who are using PBT in patients’ rehabilitation should begin as early as possible.
One of the included studies performed booster training sessions; which is a short session after months of the training program ends, to repeat the important training components, this study found that these sessions may help to retain the benefits obtained from training by providing opportunity to practice reactive balance skills. 39 In addition, van Duijnhoven et al 60 reported patients with stroke were interested in performing booster sessions, which can serve as a refresher and enhance memory consolidation to be more stable and permanent, also to maintain the consolidated memory within the motor memory areas that can be recalled as subjects could have motor memory disappearing as unused memory going to store in subconscious areas. 50 Hence, it is important to assess booster training sessions’ effectiveness in future studies.
Although it is effective, there was no definite protocol existing for the PBT in patients with stroke as well as the way of training was inconsistent between the included studies as some studies used PBT alone,39,40,42 while other studies used PBT combined with other exercises.20,41,43,44 Moreover, perturbation was done manually in 4 studies,20,39,43,44 and device-based perturbation was used in 3 studies.40-42 Also, Sessions’ frequency and program duration were various between studies, ranging from 2 to 6-sessions per week, for 2.5 to 10 weeks. Only 4 studies reported the number of perturbations per session/ per whole training program.39,40,42,43 Thus, the optimal type and dosage of training for causing improvement and lasting effects must be determined.
There were some methodological quality issues such as inadequate allocation concealment, lack of blinding of participants or assessors and therapists, attrition bias, and small sample size. Also, the variations in type and dosage of training and outcome measures used for balance evaluation. All these factors may have an impact on the quality of evidence and may explain the heterogeneity in the meta-analyses.
This study was the first systematic review that assessed the effectiveness of PBT on balance and balance confidence in patients with stroke. The study focused on the short-term effect of PBT as follow-up interval was not consistent between studies, so lasting improvement was not evaluated. The original protocol was amended, the additional/secondary outcome was changed from functional mobility to balance confidence which is a major psychological barrier that may limits an individual’s contribution in everyday activities and functioning. 40 Moreover, presence of inconsistency in the terminology regarding PBT in literature causing difficulties in detecting all eligible studies while searching in online databases. However, we are relatively certain that the searching strategy that has been used, enabled us to find all possible eligible studies.
There were some limitations that may affect the generalizability of the results. The number of studies is limited, the included studies had some methodological issues, and most of the existing evidence showed very low or low quality. Also, nearly all studies had a small number of patients, the type and dosage of training were inconsistent between studies. In addition, non-English language studies were excluded. So, the accuracy of finding may be impacted due to these issues. Also, it is difficult to draw clinical recommendation based on the current evidence, further high-quality trials are needed.
Conclusion
The current evidence regarding PBT showed that it may improve balance in patients with stroke, however its effect on balance confidence was limited. Generally, the quality of the evidence was low or very low with little confidence in the effect estimate, which suggests further high-quality trials are required.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Significance Statement
Diminished balance control, low balance confidence, and high number of falls are common consequences of stroke which influence patients’ quality of life and reduce their physical activity as a strategy to avoid falls. Multiple rehabilitation therapies have been reported to be effective for post-stroke balance impairment. Perturbation-based training (PBT) is a novel balance training aimed to improve reactive balance control to avoid a fall following a balance failure in real life.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by [