
Abstract
The impact of aerobic exercise training (AET) on cerebral blood flow (CBF) regulation remains inconclusive. This study investigated the effects of one-year progressive, moderate-to-vigorous AET on CBF, central arterial stiffness, and cognitive performance in cognitively normal older adults. Seventy-three older adults were randomly assigned to AET or stretching-and-toning (SAT, active control) intervention. CBF was measured with 2D duplex ultrasonography. Central arterial stiffness, measured by carotid β-stiffness index, was assessed with the ultrasonography and applanation tonometry. Cerebrovascular resistance (CVR) was calculated as mean arterial pressure divided by CBF. A cognitive battery was administered with a focus on memory and executive function. Cardiorespiratory fitness was measured by peak oxygen consumption (
Keywords
Introduction
Cerebral hypoperfusion and central artery stiffening have been recognized as important risk factors for age-related cognitive decline and Alzheimer’s disease and related dementias (ADRD).1–3 Elevated central arterial stiffness exposes the cerebral small blood vessels to the augmented arterial pulsation (i.e., increases in arterial pressure and blood flow pulsatility) due to the reduction of its Windkessel effects4,5 which is referred to as the buffering effects of the large arterial wall to attenuate arterial pulsations generated from the heart. 6 Augmented arterial pulsation can lead to cerebral endothelial dysfunction and vasoconstriction;4,5 thereby, increasing cerebrovascular resistance (CVR) and decreasing cerebral blood flow (CBF) often observed in the aging brain.5,7,8 These changes in cerebral hemodynamics have been linked to brain atrophy, white matter hyperintensity (WMH, a measure of cerebral small blood vessel disease), and cognitive impairment in older adults.9–11 Conversely, pharmacological or non-pharmacological interventions to reduce central arterial stiffness may lead to improvement in cerebral perfusion which may prevent or slow the progression of age-related brain structural changes and cognitive decline and ADRD.4,8,12
Aerobic exercise training reduces central arterial stiffness in older adults. 13 However, at present, the effects of aerobic exercise training on CBF regulation and cognitive performance in older adults are inconclusive.14–18 Recently, we reported that one-year progressive moderate-to-vigorous aerobic exercise training reduces central arterial stiffness and increases global CBF in patients with mild cognitive impairment (MCI), a prodromal stage of ADRD. 19 Differences in the exercise protocol (intensity, frequency, and duration) and the study population (age, sex, pre-existing comorbidities, and cognitive status) may have led to inconsistent observations in previous studies.14,17,18
The purpose of this study was to investigate the effects of a one-year progressive, moderate-to-vigorous aerobic exercise training program on CBF and its associations with changes in central arterial stiffness and cognitive performance in cognitively normal older adults. We hypothesized that aerobic exercise training would increase CBF which is associated with reduction in central arterial stiffness and improvement in cognitive performance in older adults.
Materials and methods
Study design
The present study was a sub-study of a one-year, open-label, parallel randomized control trial (RCT) comparing the effects of progressive moderate-to-vigorous aerobic exercise training with stretching-and-toning (active control) on cognitive performance in cognitively normal older adults. 20 In the parent study, cognitive function and cardiorespiratory fitness were assessed at baseline, midpoint (6-month), and trial completion (12-month). Cardio- and cerebrovascular hemodynamic assessments and magnetic resonance imaging (MRI) were performed at baseline and trial completion (12-month). The detail of randomization procedures and trial design were reported previously. 20 Briefly, a stratified randomization by years of education and sex using a blocking factor of 4 was implemented after participants’ baseline measurements. The flowchart for the trial relevant to the present study is presented in Figure S1. All outcome measures (CBF, central arterial stiffness, and cognitive test scores) were blinded to the investigators who performed measurements and analyzed the data.
The sample size estimate for CBF measurement was not performed in the original parent study which focused on the effects of exercise on cognitive performance in older adults. 20 However, based on our pilot study which showed that aerobic exercise improved CBF in cognitively normal healthy older adults, 21 we anticipated that total CBF would increase by ∼27 ± 10 mL after one year of aerobic exercise compared with the stretching group. We analyzed total CBF using a repeated measures design with 1 between (Group: aerobic exercise vs. stretching) and 1 within effects (Time: baseline and 12 month). Twenty-one participants in 2 groups (42 total) achieves 5.8% power to detect an effect size of 0.041 for group, achieves 93.3% power to detect an effect size of 0.547 for Time, and achieves 97% power to detect an effect size of 0.610 for the interaction of group and time using a Geisser-Greenhouse Correct F test and a 5% significance level.
Participants
Nine-hundred ninety-one men and women aged between 60 and 80 years were recruited from the Dallas-Fort Worth metropolitan area using advertisements. Out of those individuals, 73 participants met the criteria for this study (Figure S1). Exclusion criteria were as follows: (1) clinical diagnosis of psychiatric or neurological disorders or taking medications that have major impacts on cognition, (2) mini-mental status examination (MMSE) score <26 to exclude dementia, (3) history of recurrent epilepsy, stroke, or traumatic brain injury with a loss of consciousness ≥30 minutes, (4) physically active (>90 minutes of moderate-to-vigorous physical activity per week), (5) uncontrolled hypertension (sitting systolic blood pressure (SBP) ≥140 mmHg or diastolic blood pressure (DBP) ≥90 mmHg), (6) diagnosed diabetes mellitus (fasting glucose >126 mg/dL or taking antidiabetic medications), (7) history of cigarette smoking over the past 5 years, and (8) body mass index (BMI) ≥35 kg/m2. Screening procedures included a detailed medication history and medication questionnaire, a comprehensive physical examination, 12-lead electrocardiogram (ECG), echocardiography, and carotid artery ultrasonography to exclude severe carotid stenosis (>50%) and overt cardiovascular disease.
This study was approved by the Institutional Review Board of University of Texas Southwestern Medical Center, Texas Health Presbyterian Hospital Dallas, and University of Texas at Dallas in accordance with the guidelines of the Declaration of Helsinki and Belmont Report. All participants gave written informed consent before participation.
Intervention
All participants were randomly assigned to either aerobic exercise training or stretching-and-toning programs. Each participant was closely supervised by an exercise physiologist during the first 4 to 6 weeks of their training programs. Once participants were familiarized with the required exercises and demonstrated understanding of the exercise protocol, they performed the exercises safely by themselves either at a fitness center or home. All participants were instructed to perform the assigned interventions on top of their regular physical activities and record their exercises in written logs. To ensure adherence to aerobic exercise training interventions, participants were required to utilize a heart rate (HR) monitoring during each of the exercise sessions and to meet with the exercise physiologist monthly or as needed to review and resolve training-related issues in addition to keeping a detailed training log. The compliance to exercise training in the aerobic exercise training group was calculated as a ratio of the completed exercise sessions in which participants achieved the target HR over the prescribed exercise sessions. The compliance to stretching-and-toning intervention was calculated as a ratio of the self-reported exercise sessions in exercise logs over the prescribed exercise sessions.
Aerobic exercise training program
The progressive moderate-to-vigorous exercise program was based on each individual’s fitness level evaluated with peak oxygen consumption (
Stretching-and-toning program
The stretching-and-toning program was used as an active control group to maintain participants’ attention to a similar level as the aerobic exercise training group. The frequency and duration of the stretching-and-toning program were the same as the aerobic exercise training program. This program focused on the upper and lower limb stretching exercises. During each session, participants were asked to keep their HR below 50% of maximal HR from cardiorespiratory fitness testing. At week 19, a more advanced set of whole-body stretching exercises was prescribed. At week 26, a set of low resistance exercises performed with exercise elastic bands focused on strengthening the upper and lower body was prescribed.
Procedures and measurements
All data were collected in a quiet, environmentally controlled laboratory with an ambient temperature of ∼22°C. All participants were instructed to abstain from caffeinated beverages, alcohol, and high-intensity exercise for at least 24 hours prior to the visit of hemodynamics assessment and MRI. The same study protocols were used for baseline and trial completion (12-month).
Cardiorespiratory fitness testing
The
Cardio- and cerebrovascular assessments
To ensure stable hemodynamics throughout cardio- and cerebrovascular assessments, HR using a 3-lead ECG (Hewlett-Packard, Palo Alto, CA, USA), and beat-to-beat arterial pressure were continuously recorded from the middle finger of the left hand using a Finapres (Finapres Medical Systems, Amsterdam, The Netherlands). CBF velocity was measured from the right middle cerebral artery (MCA) using a 2-MHz transcranial Doppler (TCD) probe (Multi-Dop X2, Compumedics/DWL, Singen, Germany) using standard procedures. 26 The probe was securely attached to the temporal bone acoustic window by using either an individually created mold to fit the facial bone structure or a probe holder (Spencer Technologies, Seattle, WA) to keep the position and angle of the probe unchanged. 27 The individually created probe mold ensured the same probe position and insonation angle during repeated CBF velocity measurements. 27 When a probe holder was used, the probe position where the optimal CBF velocity signal was obtained was measured carefully perpendicular to and from the eye and ear tragus line at baseline, and the same position was used for the repeated visit. End-tidal carbon dioxide (CO2) was monitored using capnography (Carpnograd, Novamatrix, Wallingford, CT). All physiological variables were continuously recorded with a sampling frequency of 1000 Hz using data acquisition software (Acknowledge, BIOPAC Systems, Goleta, CA, USA).
After participants were instrumented and rested in supine position for >15 minutes, 6-minutes of baseline hemodynamics was obtained. Then, brachial cuff blood pressure was measured intermittently at least three times using an ECG-gated electronic sphygmomanometer (Suntech, Morrisville, NC, USA) and averaged to obtain SBP and DBP. Beat-by-beat arterial pressure waveforms from the carotid, brachial, and femoral arteries were obtained for >13 seconds using applanation tonometry (SphygmoCor 8.0; AtCO2 Medical, West Ryde, NSW, Australia) at least twice. Mean arterial pressure (MAP) was calculated from the area under the curve of the brachial pressure waveform. The carotid pressure waveform was calibrated to the MAP and DBP to calculate carotid SBP.19,28 Carotid pulse pressure was calculated from the carotid SBP minus DBP. The carotid-femoral pulse wave velocity (cfPWV) was measured between the right carotid and the left femoral arteries at least twice and averaged according to a standard procedure.
29
The right common carotid artery (CCA) images were obtained at least 3 clips with a total of ≥15 complete cardiac cycles using a 3-to-12 MHz linear array transducer with duplex ultrasonography (CX50, Philips Ultrasound, Bothell, WA, USA). The systolic and diastolic CCA diameters were measured from a >10 mm segment of the near-wall media-adventitia layer to the far wall lumen-intima layer at 10–20 mm proximal to the carotid bifurcation using an edge-detection software (Vascular Tool 5; Medical Imaging Applications, Coralville, IA, USA).13,19,28 The carotid β-stiffness index, as a measure of the local carotid arterial stiffness adjusted for the distending pressure, was calculated by the following equation:
30
Cerebrovascular hemodynamics in both steady-state and pulsatile components were obtained by duplex ultrasonography (CX50, Philips Ultrasound, Bothell, WA, USA) and TCD (Multi-Dop X2: Compumedics/DWL, Singen, Germany). The former was used to obtain total CBF as a sum of volumetric blood flow measured from the bilateral internal carotid (ICA) and vertebral arteries (VA).19,28,32,33 At least 3 clips of bilateral ICA and VA images with a vessel length of >5 mm were obtained to measure the average arterial diameter over a timespan of >15 cardiac cycles; The diameter was measured using the same edge-detection software above. Further, time-averaged mean velocity (TAMV) of the total ≥15 completed and consecutive cardiac cycles were measured at the same location where the vessel diameters were measured. Volumetric blood flow in each artery was calculated by the following equation:19,28,32,33

Volumetric blood flow of the ICA and VA was summed from both the right and left sides. CVR was calculated as MAP divided by total CBF. To adjust for individual brain size differences, total CBF and CVR were normalized to brain tissue mass which was obtained based on MRI measurement of total brain tissue volume and an estimate of brain tissue density of 1.06 g/mL 34 and were represented as nCBF and nCVR, respectively. CBF velocity at the MCA using TCD was averaged for 6 minutes baseline and CVR index (CVRi) was calculated as MAP divided by CBF velocity. The pulsatility index (PI) was calculated to assess pulsatile components of CBF at the MCA. Briefly, continuous CBF velocity waveforms measured at the MCA by TCD, consisting of >15 cardiac cycles without artifact, were extracted. PI was calculated as systolic minus diastolic CFB velocity divided by mean CBF velocity.19,28
Brain tissue volume
All MRI data were collected by a 3-Tesla scanner (Philips Medical System, Best, The Netherlands) which uses a body coil for radiofrequency transmission and an 8-channel head coil with parallel imaging capability for signal reception. 3D magnetization-prepared rapid acquisition gradient echo (MPRAGE) pulse sequence was acquired to measure brain tissue volume using the following parameters: TE/TR = 3.7/8.1 ms, flip angle = 12°, FOV =256 × 256 mm, number of slices = 160 (no gap), resolution = 1 × 1 × 1 mm3, SENSE factor = 2, and scan duration = 4 min.
The FreeSurfer software (version 6.0, https://surfer.nmr.mgh.harvard.edu) was used for tissue segmentation to measure total gray matter (GM) and white matter (WM) volume. Total brain volume was calculated as a sum of measured cortical and subcortical GM and WM volumes, including brainstem and cerebellum19,28,33 and was used for normalization of CBF and CVR for individual differences in brain size.
Cognitive function assessment
A comprehensive battery of cognitive tests was administered to all participants. The cognitive test took ∼2 hours to complete. The domains of function tested included inductive reasoning, long-term episodic memory, working memory, processing speed, and verbal ability. Reasoning was assessed using the: Educational Testing Service (ETS) Letter Sets test, and the Raven’s Progressive Matrices test. Episodic memory was assessed using the Wechsler Memory Scale (WMS) Logical Memory Immediate and Delayed Recall subtests, and the Woodcock-Johnson (WJ) Memory for Names Immediate and Delayed Recall subtests. Processing speed was measured using the Digit Comparison test. Working memory was tested using the WMS Letter Number Sequencing test, and the Operation Span test. Verbal fluency was measured using the Controlled Oral Word Association – FAS test, and word knowledge was assessed using the ETS Vocabulary subtest. These tests were chosen for administration for credible validity, reliability, and sensitivity to cognitive decline in older adults based on our previous studies.35,36
Statistical analysis approach
The Chi-square test was used when comparing the ratio differences between groups in categorical variables. The Student’s t-test was used when comparing the means differences between groups at baseline and percentage changes from baseline to trial completion in continuous variables. Two-way repeated-measures analysis of variance (ANOVA) was performed on complete outcome data to examine the main effects of time and group as well as the interaction effect of time-by-group. Post-hoc multiple pairwise comparisons were corrected by the Bonferroni method in the case of a significant time-by-group interaction. Partial eta squared (ηp2) was calculated to represent effect sizes of significant terms. Pearson’s product-moment correlation analysis was performed to test linear associations between variables in aerobic exercise training and stretching-and-toning groups separately. Mediation analysis was performed to understand the relationship between aerobic exercise training-related changes in
Results
Participants’ demographics at study completion
Among 73 participants enrolled in the trial (37 in stretching-and-toning and 36 in aerobic training), 56 participants (28 in stretching-and-toning and 28 in aerobic training) completed the study intervention with complete CBF and central arterial stiffness measurements. Of those who completed the trial, one participant in the stretching-and-toning group was excluded from data analysis because of development of severe atherostenosis in the right ICA at the trial completion. CBF velocity measured in the MCA with TCD was available in 43 participants (22 in stretching-and-toning and 21 in aerobic training) (Figure S1). The demographic characteristics of the participants who completed the cerebral hemodynamic assessments did not significantly differ from those who participated in the parent study (data not shown; p’s > 0.05).
20
There were no significant differences in baseline participant characteristics between groups, including distributions of sex and race, age, years of education, baseline MMSE score, body mass, BMI, the usage rate of antihypertensive drug, systemic hemodynamics, and
Baseline participant demographics by groups.
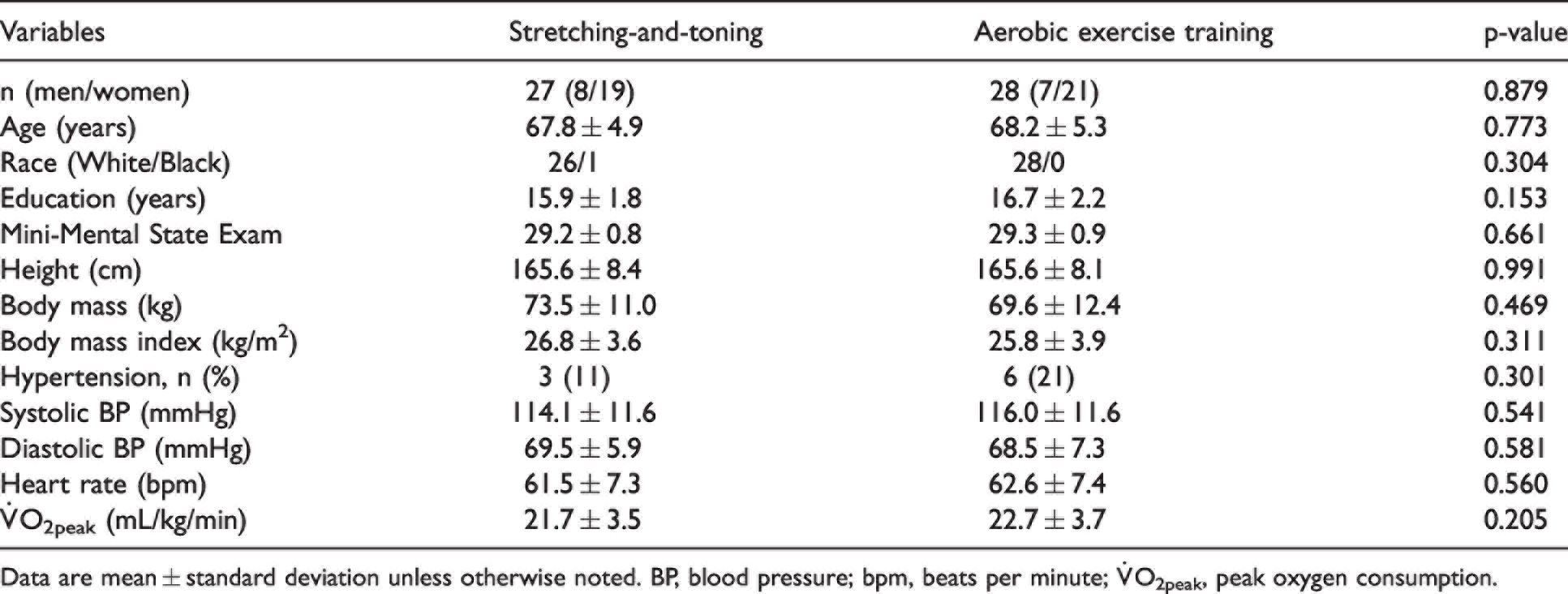
Data are mean ± standard deviation unless otherwise noted. BP, blood pressure; bpm, beats per minute;
Intervention effects: Group differences in cardiorespiratory fitness and systemic and carotid hemodynamic measurements
The average compliance to exercise training was 80 ± 14% in the aerobic training group and 77 ± 25% in the stretching-and-toning group, a nonsignificant difference. Repeated measures ANOVA with main effects of Time (baseline and follow-up), Group (aerobic training and stretching-and-toning), and a time-by-group interaction as independent variables predicting the dependent variables of interest were conducted. Specifically, main effect of Time on
Cardiorespiratory fitness and systemic and carotid hemodynamic measurements by groups.
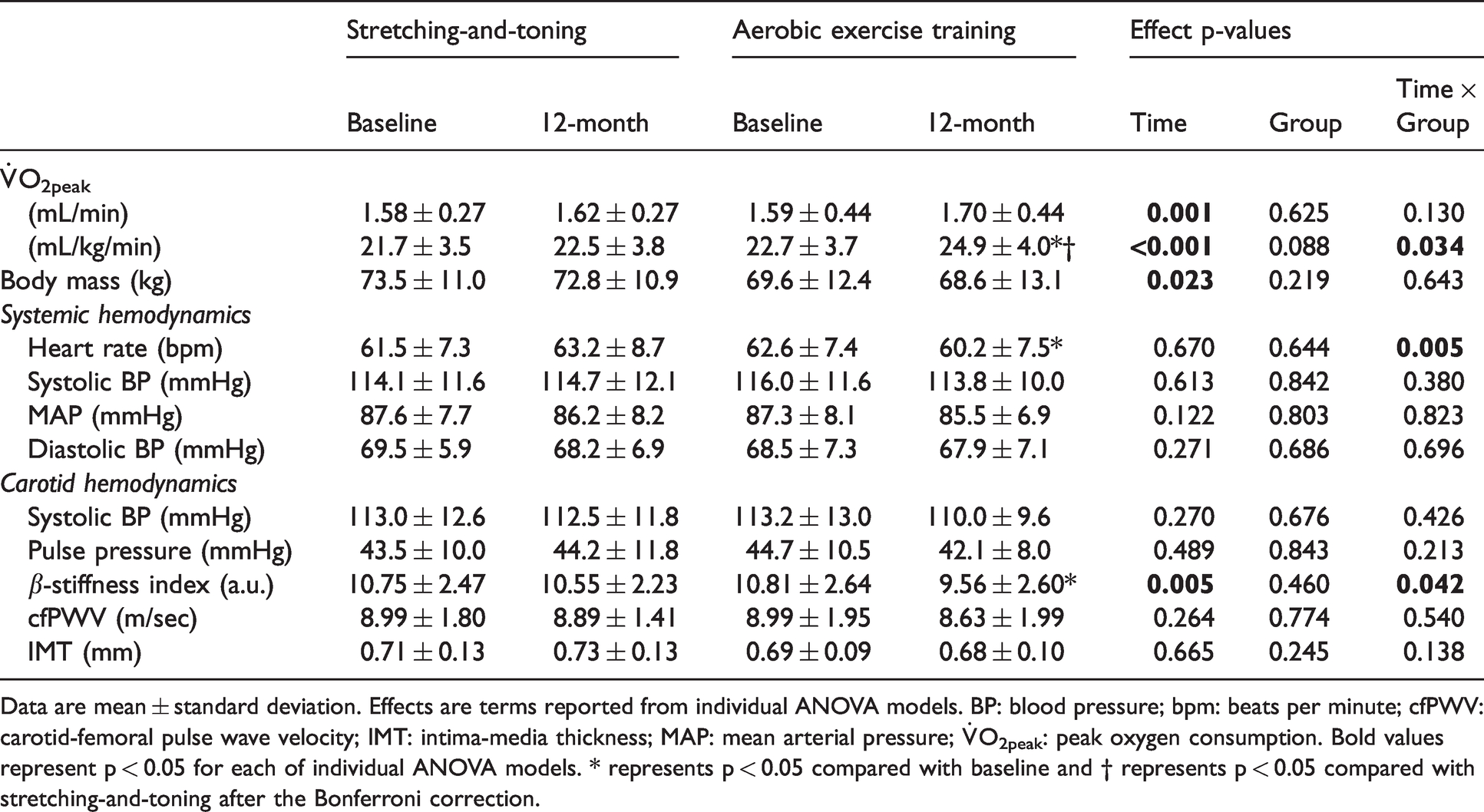
Data are mean ± standard deviation. Effects are terms reported from individual ANOVA models. BP: blood pressure; bpm: beats per minute; cfPWV: carotid-femoral pulse wave velocity; IMT: intima-media thickness; MAP: mean arterial pressure;
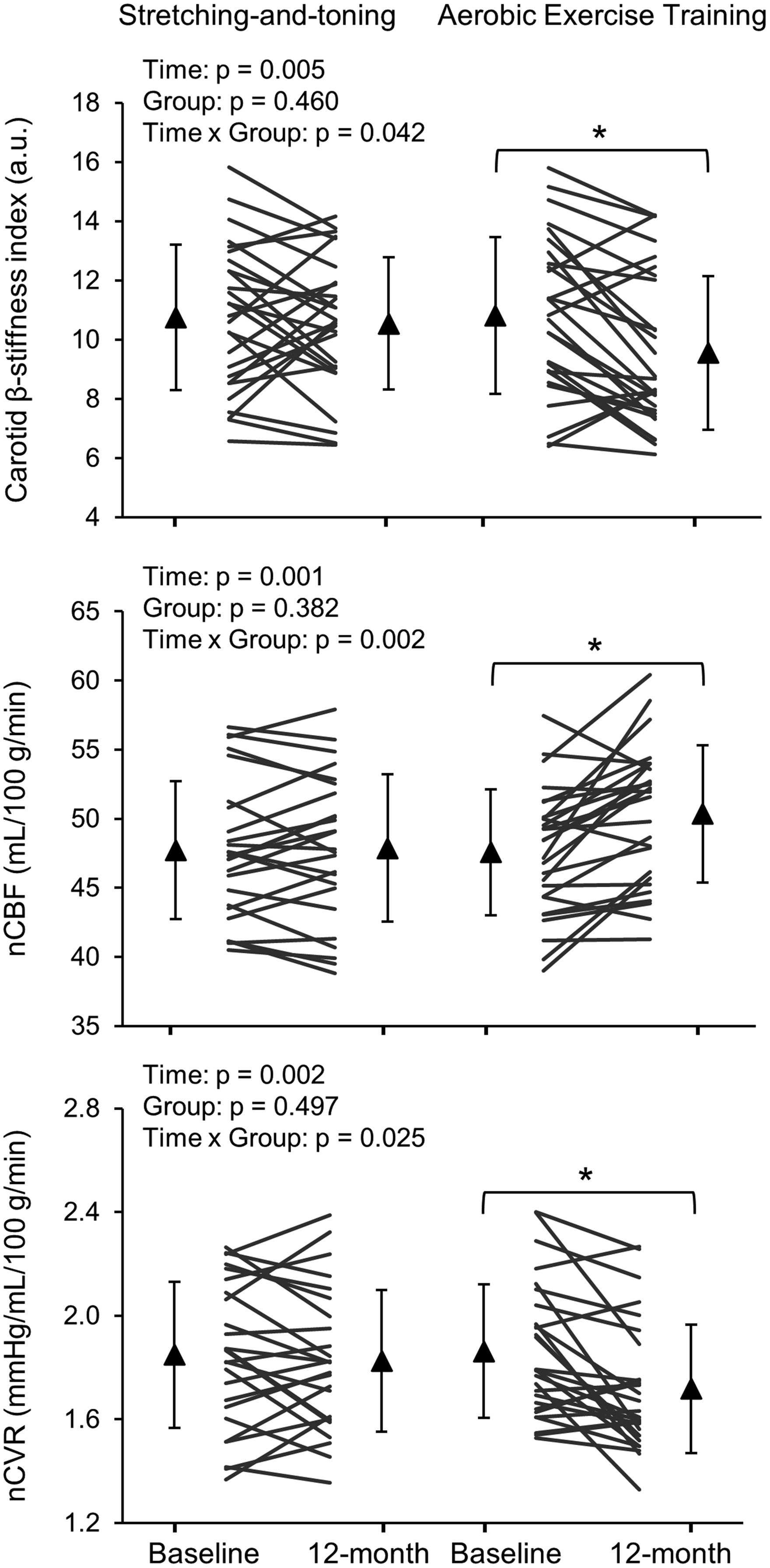
Changes in carotid β-stiffness index (upper panel), normalized cerebral blood flow (nCBF) (middle panel), and normalized cerebrovascular resistance (nCVR) (lower panel) after one-year stretching-and-toning or aerobic exercise training. Thin lines represent individual changes. Triangles show mean values and the error bars represent standard deviations. ∗p < 0.05 compared with baseline after Bonferroni correction.
Intervention effects: Group differences in cerebral hemodynamic measurements and brain tissue volumes
From the repeated measures ANOVAs conducted on cerebral and brain volume variables, Time, Group, and time-by-group terms again served as predictors. Figure S2 shows representative ultrasonography images of blood flow measurements in the ICA and VA at baseline and 12-month from one subject in the aerobic exercise training group. Significant time-by-group interactions revealed that aerobic training increased total CBF (ηp2 = 0.128) (%change of total CBF: 5 ± 7% vs. 0 ± 5%, p = 0.007) and nCBF (ηp2 = 0.172) (%change of nCBF: 6 ± 7% vs. 0.3 ± 5%, p = 0.002) and decreased nCVR (ηp2 = 0.097) (%change of nCVR: −7 ± 10% vs. −1 ± 9%, p = 0.022) at 12-months compared to stretching-and-toning (Table 3 and Figure 1 and S3). Total CVR showed reductions over time in both groups. Of note, volumetric blood flow of the ICA (summed from both the right and left sides) increased more after aerobic training than after stretching-and-toning (ηp2 = 0.115) (% change of volumetric blood flow of the ICA: −7 ± 11% vs. −1 ± 7%, p = 0.007). However, volumetric blood flow, the vessel diameter, and velocity in each of the ICA and VA vessels did not show statistically significant changes after either aerobic training or stretching-and-toning (Table S1). There were time effects of increases in CBF velocity at the MCA and decreases in CVRi for both groups, but no time-by-group interactions after the one-year stretching-and-toning or aerobic training (Table 3). No intervention effect was found for PI. Total brain and GM (but not WM) volumes decreased equally in both groups (Table 3 and Figure S3).
Cerebral hemodynamic measurements and brain tissue volume by groups.
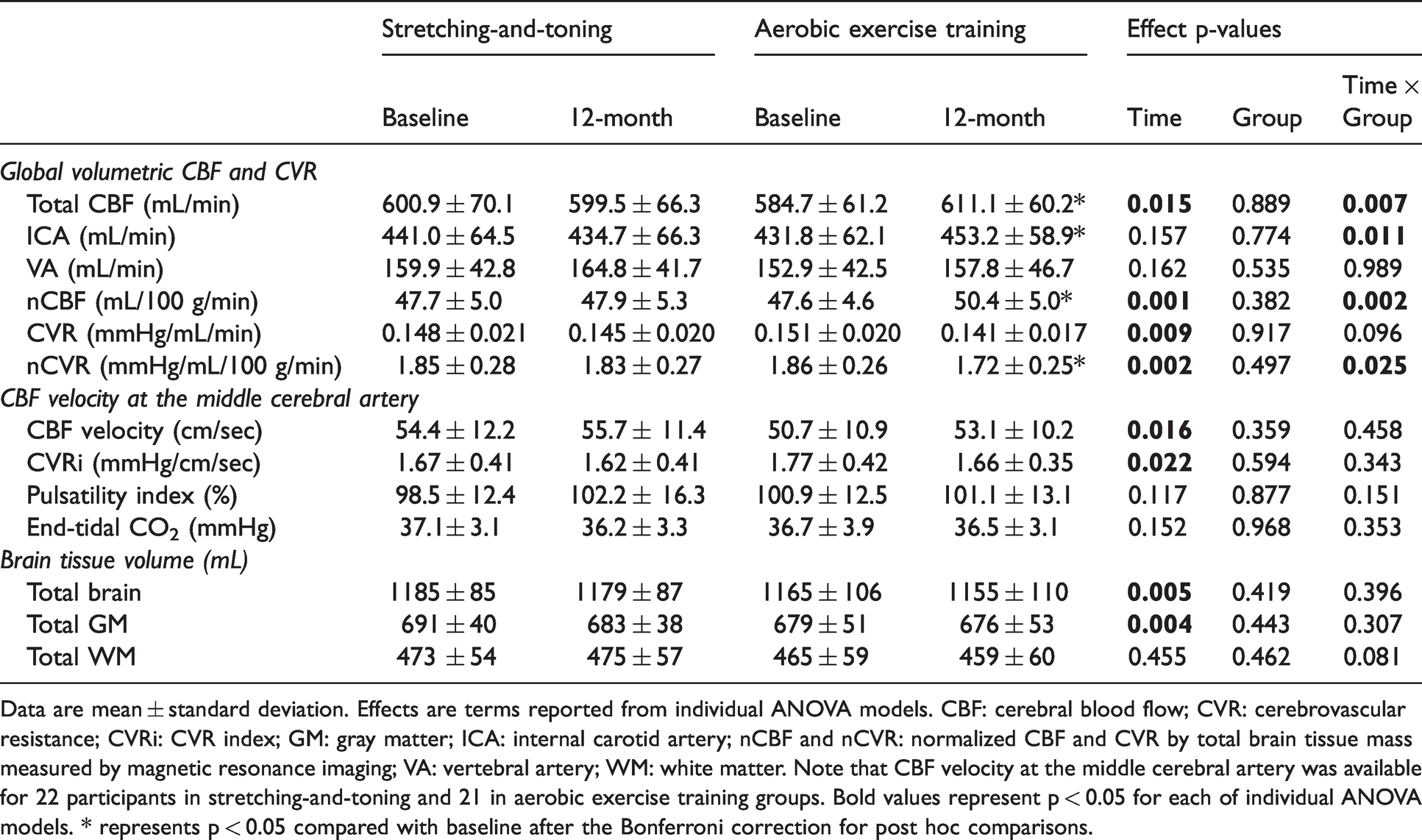
Data are mean ± standard deviation. Effects are terms reported from individual ANOVA models. CBF: cerebral blood flow; CVR: cerebrovascular resistance; CVRi: CVR index; GM: gray matter; ICA: internal carotid artery; nCBF and nCVR: normalized CBF and CVR by total brain tissue mass measured by magnetic resonance imaging; VA: vertebral artery; WM: white matter. Note that CBF velocity at the middle cerebral artery was available for 22 participants in stretching-and-toning and 21 in aerobic exercise training groups. Bold values represent p < 0.05 for each of individual ANOVA models. * represents p < 0.05 compared with baseline after the Bonferroni correction for post hoc comparisons.
Intervention effects: Group differences in cognitive performance
Results from the repeated measures ANOVAs for the cognitive variables were more homogenous. No intervention group effects or time-by-group interactions were found for the cognitive variables. However, most cognitive variables, including tests of reasoning, episodic memory, and verbal abilities showed small but statistically significant increases in cognitive performance over time, regardless of group (Table 4).
Neurocognitive testing scores by groups.
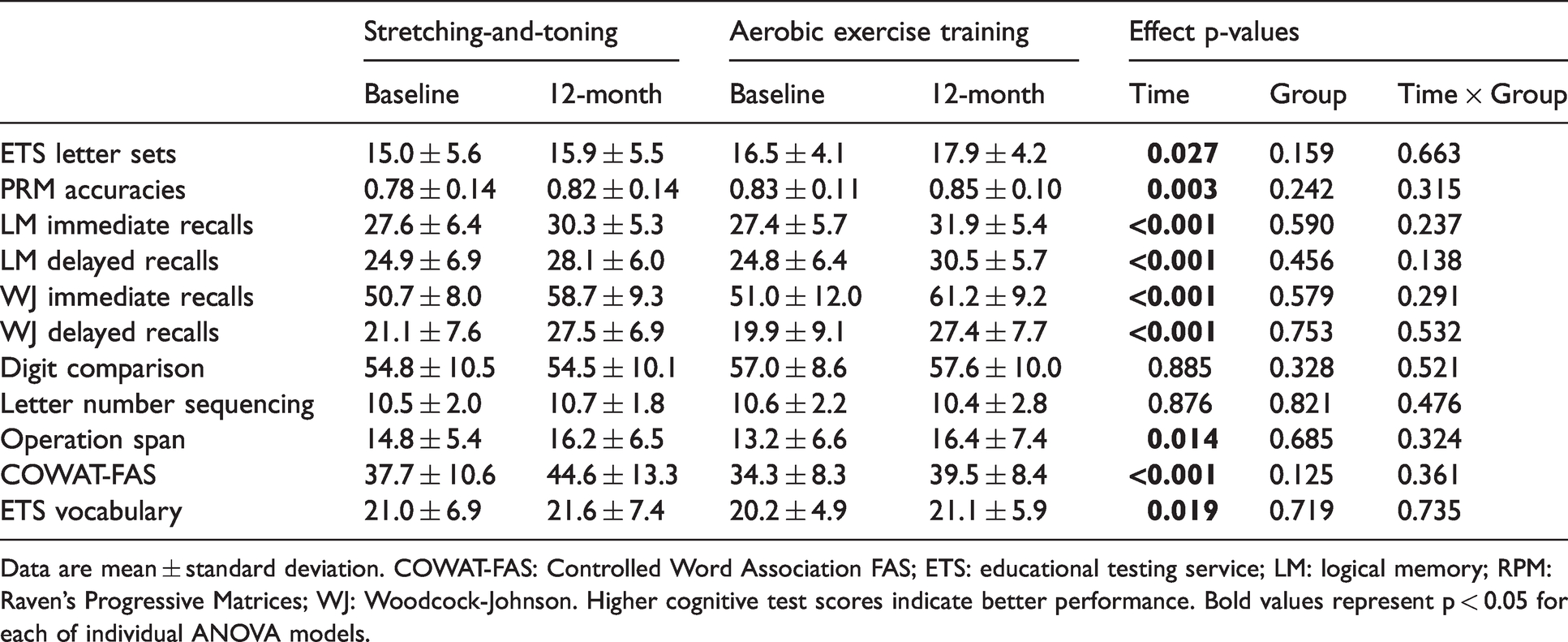
Data are mean ± standard deviation. COWAT-FAS: Controlled Word Association FAS; ETS: educational testing service; LM: logical memory; RPM: Raven’s Progressive Matrices; WJ: Woodcock-Johnson. Higher cognitive test scores indicate better performance. Bold values represent p < 0.05 for each of individual ANOVA models.
Associations among changes in
O2peak, Central arterial stiffness, cerebral hemodynamics, and cognitive performance
Inspection of zero-order Pearson correlations for each group suggested that increased
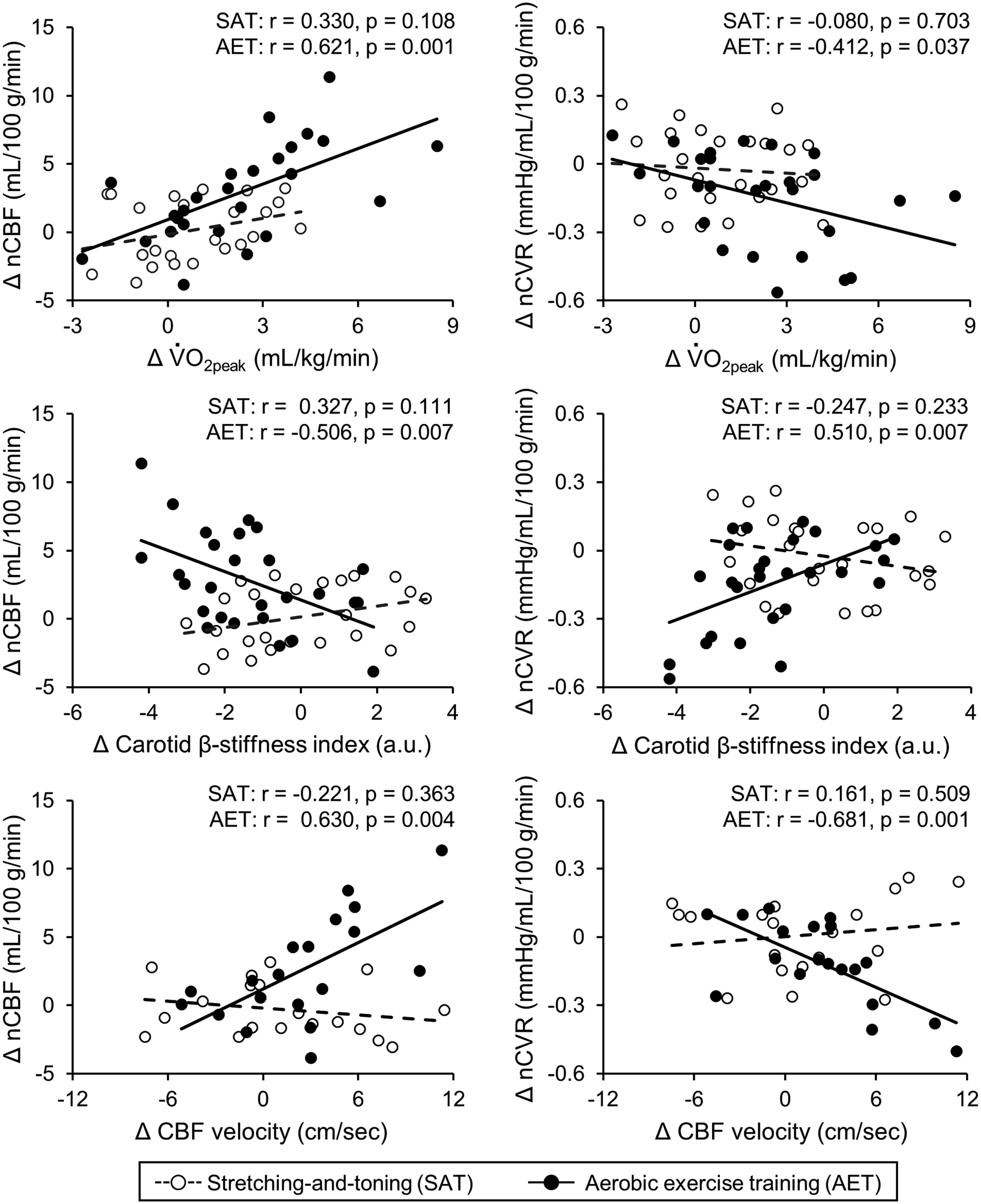
Correlations of changes in peak oxygen consumption (V̇O2peak: upper panel), carotid β-stiffness index (middle panel), and mean cerebral blood flow (CBF) velocity measured at the middle cerebral artery (MCA, lower panel) with normalized CBF (nCBF: left side panels) and normalized cerebrovascular resistance (nCVR: right side panels) in the stretching-and-toning and aerobic exercise training groups. Note that the mean CBF velocity at the MCA was available 22 in stretching-and-toning group and 21 in aerobic exercise training group.
Further correlation analysis by groups revealed that individual changes in carotid and cerebral hemodynamics after the one-year intervention were associated with the changes in cognitive test scores (Table S3 and Figure 3). Notably, decreased nCVR and carotid β-stiffness index were associated with improvements in the Logical Memory and Woodcock-Johnson immediate recall test scores in the aerobic training group but not in the stretching-and-toning group (Figure 3).
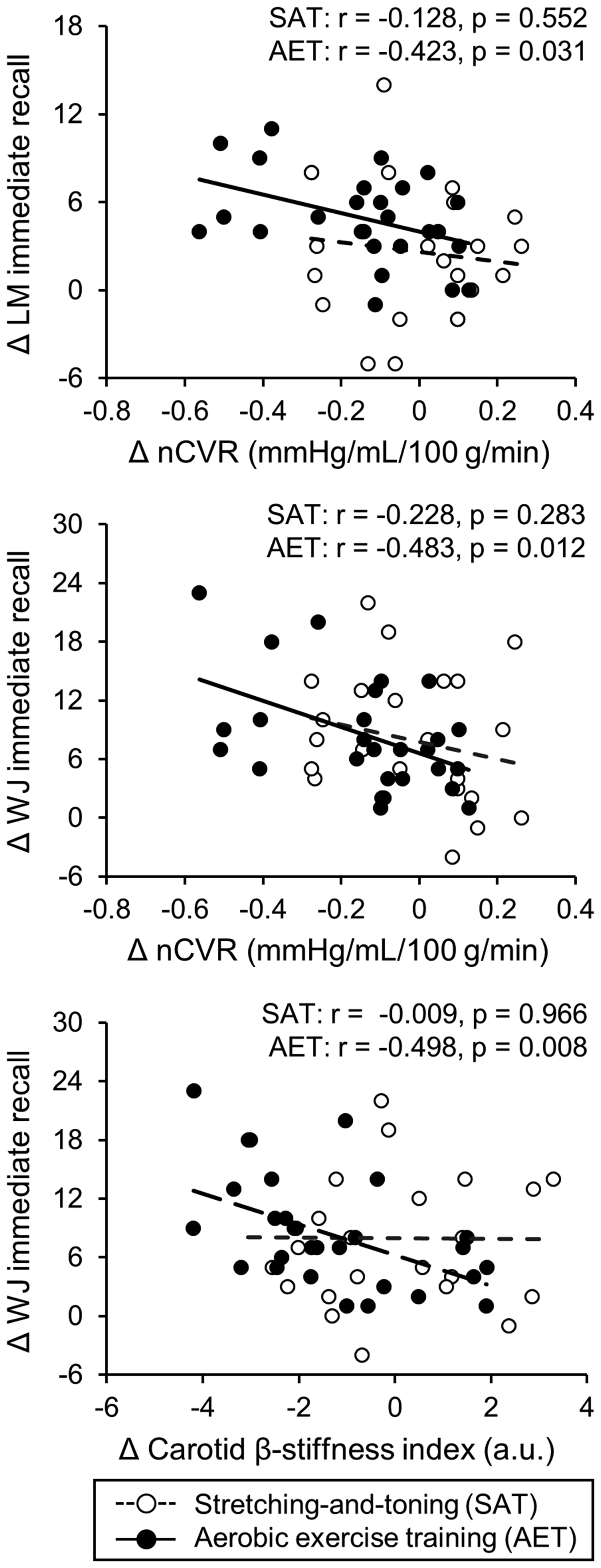
Correlations of changes in normalized cerebrovascular resistance (nCVR) with logical memory (LM) immediate recall (upper panel) and Woodcock-Johnson (WJ) immediate recall (middle panel) and changes in carotid β-stiffness index with WJ immediate recall (lower panel) in the stretching-and-toning and aerobic exercise training groups.
Discussion
This study revealed several interesting findings. First, one-year progressive moderate-to-vigorous aerobic exercise training increased global CBF while decreasing CVR and carotid arterial stiffness in cognitively normal older adults. Second, improved cardiorespiratory fitness assessed by
Effects of aerobic exercise training on cerebral blood flow
At present, the beneficial effects of aerobic exercise training on CBF are inconclusive.14,17 The methodological changes in CBF measurement may partially explain the inconsistent findings.14,17 A recent systematic review and meta-analysis of the effects of cardiorespiratory fitness and aerobic exercise training on CBF reported that higher cardiorespiratory fitness was associated with higher CBF velocity measured at the MCA using TCD among older adults in cross-sectional studies. However, interventional studies with moderate intensity of aerobic exercise training for a duration of 2–12 months had little effect on the MCA CBF velocity and global cerebral perfusion measured using MRI arterial spin labeling (ASL). 17 One major limitation in measuring changes in CBF using TCD is that changes in CBF velocity do not necessarily equal changes in volumetric CBF. 38 In addition, measurements of global cerebral perfusion using ASL are limited by a low signal/noise ratio in the white matter and some arbitrary model parameter assumptions which may be altered by aerobic exercise training or stretching-and-toning. 39 In this study, we did not observe time-by-group interactions of changes in CBF velocity at the MCA consistent with previous findings. 17 However, compared with stretching-and-toning, aerobic exercise training increased global CBF measured as the sum of volumetric blood flow from both the ICA and VA using 2D color-coded duplex ultrasonography which may overcome the limitations of measurement of global CBF using TCD and ASL.32,33
The differences in the study design (e.g., single-arm vs. two-arm trial), exercise protocol (e.g., mode, frequency, intensity, and duration), or study population characteristics (e.g., healthy adults, older adults, middle-aged, and patients with MCI) may also influence the aerobic exercise training effects on CBF.14,17 In this regard, vigorous-intensity aerobic exercise training has been recommended to improve CBF because it was argued that the benefit of aerobic exercise training on CBF may only be manifested when
In this study, aerobic exercise training increased
Associations between carotid arterial stiffness and CBF
Regular physical activities ameliorate age-related arterial stiffening in healthy older adults.13,46,47 We can only speculate on possible mechanisms. Arterial stiffening is determined mainly by the elastin and collagen contents as well as the smooth muscle tone of the arterial wall. 47 The elastin-collagen composition of the arterial wall represents a major component of arterial stiffness and is unlikely to be altered with short-term aerobic exercise training. 47 In this regard, several previous studies of 3 - 4 months of aerobic exercise training suggested that reduced vascular smooth muscle tone related to improved endothelial function, decreased sympathetic neural activity, or enhanced sympatholysis mediated by nitric oxide may be the underlying mechanism of exercise-related reduction of central arterial stiffness in older adults.47,48 Thus, if aerobic exercise training reduced carotid artery and large cerebral artery smooth muscle tone which then would lead to reduction in CVR and increases in global CBF observed in the present study.16,48
The findings that aerobic exercise training increased CBF and decreased CVR were associated with reduced carotid arterial stiffness also support the Windkessel effect hypothesis of CBF regulation.4,5,12,48 The wall of large central elastic arteries (e.g., aorta and carotid artery) expands and recoils within each cardiac cycle to attenuate arterial pulsations from the heart in order to maintain continuous blood flow into the peripheral vascular beds, which is referred to as the Windkessel effects. 6 It has been proposed that impaired Windkessel effects and elevated arterial pulsation may cause cerebral endothelial dysfunction, increase cerebrovascular tone (i.e., increased CVR), and reduced CBF.5,7,8 Thus, aerobic exercise training decreased-carotid arterial stiffness may lead to reductions in arterial pulsation as reflected by the attenuated CBF PI in the aerobic exercise training groups and improvement in endothelial function and CBF (Table S2 and Figure 2). Further mediation analysis also shows that aerobic exercise training-induced reduction of CVR, reflecting improved endothelial function, is related to the reduction in carotid arterial stiffness (Figure S4). Finally, we observed that changes in CBF velocity in the MCA were associated positively with changes in nCBF and negatively with changes nCVR in the aerobic exercise training group, suggesting that increases in the cerebral blood vessel wall shear stress may lead to nitric oxide mediated vasodilation and improvement in CBF (Table S2 and Figure 2). In addition, exercise-induced increases in the capillary density 49 and/or increases in cerebral metabolic rate of oxygen may also contribute to increased CBF through neurovascular coupling. 14 Future studies are needed to understand the underlying molecular and cellular mechanisms of increased CBF after aerobic exercise training.
Cognitive performance and brain volume
There is a significant knowledge gap in our understanding of the potential influence of aerobic exercise training-related changes in central arterial stiffness and CBF on cognitive decline or dementia prevention.14,48 Increases in central arterial stiffness,8–10 brain hypoperfusion, 2 and elevated CVR 3 have been recognized as strong predictors of cognitive decline and development of ADRD. Population-based studies reported that lower CBF and higher CVR and central arterial stiffness in older adults are associated with accelerated cognitive decline and increased the risk of dementia.2,3,11 These findings suggest that improving cardio- and cerebrovascular function may prevent and slow cognitive decline and reduces the risk of dementia. There is an increasing recognition that aerobic exercise training may improve neurocognitive function in middle-aged and older adults in addition to the amelioration of cardio- and cerebrovascular function.14,15 In this study, we observed that cognitive performance, mainly memory function, was improved slightly but significantly in both groups. In addition, aerobic exercise training-induced reductions in carotid β-stiffness index and CVR were associated with improved Woodcock-Johnson immediate recall scores in the aerobic exercise training group. These findings are consistent with previous observational studies which suggested that exercise-related reductions in central arterial stiffness and CBF regulations may improve memory function.45,50 However, aerobic exercise training did not prevent brain gray matter reduction in the present study. We speculate but cannot prove that aerobic exercise training-induced improvements in cerebrovascular function may precede changes in brain structure and that it is also possible that it may take a longer time of aerobic exercise training to have cumulative effects on brain structure.
Clinical perspectives
At present, there are no effective treatment strategies to prevent or slow age-related cognitive decline or ADRD.
51
Brain pathophysiology, in particular vascular dysfunction, can begin 10–20 years before the onset of cognitive impairment.51,52 Therefore, lifestyle modification to improve vascular function during the latent phase of ADRD (e.g., the cognitively normal phase) is critical to maintaining brain health.4,7,8,12 Mounting evidence indicates that elevated central arterial stiffness and CVR and reduced CBF may accelerate age-related cognitive decline and increase the risk of ADRD.2,3,8,10,11,53 In this study of cognitively normal older adults, we showed one-year progressive moderate-to-vigorous aerobic exercise training increased physical fitness as measured by
Study strengths and limitations
There are several strengths of our study. First, this is the first RCT study in cognitively normal older adults that investigated the effects of one-year aerobic exercise training on central arterial stiffness and cerebral hemodynamics and their associations with neurocognitive performance. The objective measurement of
The findings from this study should be interpreted in the context of the following limitations. First, the sample size was relatively small and the sample included more women than men, and more than 90% of participants were well-educated Caucasians, which reduces the generalizability of our findings. Also, the attrition rate was relatively high (∼23%) which may bias our results. Therefore, future studies with larger sample sizes, along with racially and ethnically diversified populations are needed to confirm the findings of this study. This is particularly important in ADRD research due to the existing health care disparities in ADRD. 51 Second, although we observed that both aerobic exercise training and stretching-and-toning improved cognitive scores, this change was minimal and likely related to a practice effect in the repeated measures of cognitive performance,54,55 which may limit the clinical relevance of our findings. In addition, for post hoc comparisons of the main outcomes of the study, that is, changes in CBF and carotid arterial stiffness revealed with ANOVA, we used Bonferroni corrections to reduce type I errors. However, given the exploratory nature of other modeling and data analysis, we did not control the overall study statistical error <5%. We must also acknowledge that the associations observed between changes in CVR, carotid arterial stiffness, and memory performance with aerobic exercise training do not indicate the presence of a causal relationship. A potential neurovascular coupling relationship with aerobic exercise needs to be elucidated in further studies. Third, CVR was calculated based on MAP and CBF measured in the supine position under resting condition; thus, CVR does not take into account possible fluctuations in venous or intracranial pressure (ICP). ICP in the supine position is ∼15 mmHg which is relatively stable under resting conditions. 56 Theoretically, cerebral perfusion pressure (CPP) = MAP-ICP and CVR = CPP/CBF. Since it is difficult to measure ICP invasively in healthy human subjects, CVR, in most studies, was estimated as CVR = MAP/CBF.3,16,17,19 Lastly, the one-year trial duration may still be too short to reveal the cumulative effect of aerobic exercise training on brain structure and function relative to stretching-and-toning given that these effects are likely to be accumulated over years for a significant impact or may occur at microstructural level which cannot be detected with the current resolution of MRI.
Conclusion
This study demonstrates that in cognitively normal older adults, 1) one-year progressive moderate-to-vigorous aerobic exercise training increased global CBF, decreased CVR, and reduced carotid arterial stiffness, 2) aerobic exercise training-induced increase of
Supplemental Material
sj-pdf-1-jcb-10.1177_0271678X221133861 - Supplemental material for One-year aerobic exercise increases cerebral blood flow in cognitively normal older adults
Supplemental material, sj-pdf-1-jcb-10.1177_0271678X221133861 for One-year aerobic exercise increases cerebral blood flow in cognitively normal older adults by Tsubasa Tomoto, Aryan Verma, Kayla Kostroske, Takashi Tarumi, Neena R Patel, Evan P Pasha, Jonathan Riley, Cynthia D Tinajero, Linda S Hynan, Karen M Rodrigue, Kristen M Kennedy, Denise C Park and Rong Zhang in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the National Institutes of Health (R01HL102457) and the Josephine Hughes Sterling Foundation.
Acknowledgements
The authors thank all our study participants for their willingness, time, and effort devoted to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
T Tomoto wrote the manuscript; DP and RZ designed research; T Tarumi, JR, CT, KR, and KMK performed data collection; T Tomoto, AV, KK, T Tarumi, NP, EP, and LH analyzed data. AV, T Tarumi, JR, KMK, KMR, DP, and RZ edited the manuscript. All of the authors have approved the final version of the manuscript and agree to be accountable for all aspects of the work. All persons designated as authors qualify for authorship, and all those who qualify for authorship are listed.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.