
Abstract
A 7-year-old boy presented with retrosternal chest pain for 2 months. Physical examination, blood tests, chest X-ray, and electrocardiogram were normal. Two-dimensional echocardiography showed a mildly dilated right atrium and ventricle with mild tricuspid regurgitation, but the right coronary artery was not visualized. Coronary computed tomography angiography revealed an anomalous origin of the right coronary artery from the left main coronary artery with an inter-arterial course. The treadmill test showed no ischemia, but due to the risk of sudden cardiac death, the patient was advised to restrict physical activities. He remained asymptomatic at 6-month and 1-year follow-up. This case emphasizes the importance of considering coronary artery anomalies in pediatric chest pain, utilizing two-dimensional echocardiography as a screening tool and coronary computed tomography angiography as the gold standard for diagnosis. Management should be individualized based on symptoms and the type of coronary artery anomaly.
Introduction
Coronary artery anomalies (CAAs) consist of abnormal origin or course of any of the three main epicardial coronary arteries. They are rare diseases with 0.1%-1.15% prevalence. 1 Clinical manifestations vary from asymptomatic or angina-like chest pain to sudden cardiac death, hence leading to either misdiagnosis or missed diagnosis. The treatment options have to be tailored to the patient’s characteristics and have a variable prognosis. We report a case of an incidental finding of a CAA: right coronary artery (RCA) arising from the left main coronary artery (LMCA) with inter-arterial course in a 7-year-old child.
A 7-year-old, developmentally normal male child, born to a non-consanguineous couple with no significant birth history and age-appropriate immunization status presented with complaints of chest pain in the retrosternal area, not varying with exertion, on and off for 2 months. General physical examination revealed stable vitals, with a pulse rate of 98 beats per minute, regular rhythm, good volume, peripheral pulses well felt, no radio-radial or radio-femoral delay, a respiratory rate of 22 per minute, blood pressure in all four limbs between 5th to 50th centile, and saturation above 97% in all four limbs with normal jugular venous pressure (6 cm). His growth was appropriate for his age. The head-to-toe examination did not reveal any positive findings. Cardiovascular systemic examination revealed normal intensity of first (S1) and second (S2) heart sounds, with a normal split of S2 with no murmurs. Other systemic examinations were unremarkable.
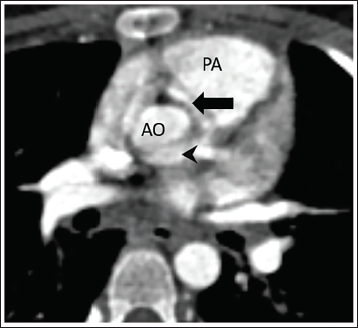
Complete blood count was normal. Chest X-ray appeared normal with a cardiothoracic ratio of 0.4. Twelve-lead electrocardiogram (ECG) was normal with normal rate, rhythm, and intervals, with no ischemic changes (Figure 1). To evaluate for a cardiac cause of chest pain, two-dimensional (2D) echocardiography (ECHO) was performed, which showed a mildly dilated right atrium and ventricle with mild tricuspid regurgitation (gradient 22 mmHg). There was no evidence of pulmonary artery hypertension. Good biventricular function was noted. The LMCA appeared normal, but the RCA was not visualized. Hence, a computed tomography (CT) angiography (Siemens Somatom go Top 128-slice dual energy) was performed, which showed the anomalous origin of the RCA from the LMCA with an inter-arterial course, no pulmonary thromboembolism, and normal bilateral lung fields (Figure 2). A stress thallium study could not be performed due to the poor socioeconomic status of the patient; hence, a treadmill test was performed after 10 days with all precautions to look for exercise-induced ischemia, which was normal but another manifestation of the diagnosis could be sudden cardiac death; hence, he was advised to exercise restriction. At 6-month and 1-year follow-up, the child was asymptomatic and is under follow-up every 6 months.
Discussion
In children, most coronary artery diseases are congenital, and there is sparse literature on them in the pediatric age group. The subsequent course to the right ventricle between the pulmonary artery and aorta may result in compression of the vessel, myocardial ischemia, and sudden death, especially in teenagers. 2 An anomalous RCA with an intra-arterial course is more common among right coronary anomalies, with a prevalence estimated at 0.1%. 3 Electrocardiogram may show ST-T or Q wave abnormalities, but even if it is normal it is important to screen with 2D ECHO. The parasternal short-axis view allows visualization of LMCA origin, which is normally at approximately 4 o’clock, and the RCA origin, which is at approximately 11 o’clock. Color mapping with Doppler can help identify the inter-arterial course. Subcostal windows are more useful in infants and smaller children. 4 A computerized coronary angiogram is the recent gold standard. 1 Due to the possibility of CAAs causing symptoms during exercise, even if the baseline ECG is normal, it is pertinent to perform an exercise ECG or a treadmill test, which could help unmask the underlying ischemia. In a consensus statement provided by a working group in 2017, provocative testing is recommended in asymptomatic patients with an intramural/inter-arterial RCA. Asymptomatic patients with no evidence of ischemia clinically or with provocative testing may be allowed to participate in competitive athletics with caution after counseling and preparedness for cardiac events. Surgical intervention (unroofing or coronary artery bypass grafting) is recommended for those with signs or symptoms of myocardial ischemia. 5 Unroofing involves incising the common wall between the aorta and the intramural segment of the anomalous coronary artery. This procedure relocates the coronary orifice, enlarges it, eliminates the intramural component, and removes the vessel from between the great arteries. 6
Yumeng Gao et al. reported CAAs in eight children aged 8-16 years who presented with syncope, six of whom were diagnosed with a right anomalous coronary artery from the opposite sinus (ACAOS), while two patients were diagnosed with a left ACAOS. Coronary unroofing procedures were conducted in four patients, while the other four received routine medical treatment for vasovagal-like syncope. 7
In a retrospective study by Li et al., they reported four female pediatric patients (ages 7-14) with ALCA-R who presented with exercise-induced syncope, acute myocardial infarction, and left heart failure. All showed elevated creatine kinase and troponin levels, and ECG indicated left main coronary artery occlusion. Coronary CT angiography confirmed the anomalous origin of the left coronary artery from the right sinus. Two patients underwent unroofing surgery, while the others were advised to avoid strenuous activities. All patients survived without recurrent cardiovascular events during 12-43 months of follow-up. 8
Amioka et al. reported a 17-year-old boy with anomalous origin of left coronary artery with an intramural aortic course who experienced exercise-induced syncope and chest pain. During a treadmill test, his blood pressure dropped significantly, and ECG showed ST-segment changes. Coronary CT angiography confirmed the anomalous coronary origin. After unroofing surgery and neo-ostium reconstruction, his symptoms resolved. 9
This case report highlights the importance of cardiac evaluation of clinically significant chest pain. Following routine evaluation with X-ray and ECG, a screening 2D ECHO indicated the possibility of an anomalous origin of the coronary arteries. Computed tomography angiography revealed the diagnosis of anomalous origin of the RCA with an inter-arterial course. Since the anomalous intra-arterial course of the RCA (between the pulmonary artery and the aorta) is notoriously known to produce ischemia during exercise, a Bruce protocol-based treadmill test was performed, which did not reveal any ischemia. Hence based on a team discussion, a decision was made to follow up with the child.
Although similar cases have been reported earlier, such occurrences remain rare. Diagnosing these cases in peripheral settings is crucial and can be lifesaving. This case report reinforces the need for pediatricians to consider CAAs as a potential cause of unexplained chest pain. In conclusion, in an otherwise structurally normal heart, it is important to rule out cardiac causes of chest pain. Though ECG might point us to evaluate in terms of CAA, we suggest 2D ECHO as a screening tool for diagnosing congenital CAAs. Computed tomography angiography would help us give the final diagnosis and hence is the gold standard currently. Management should be individualized based on the patient’s symptoms and the type of CAA.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not obtained because patient consent was secured. The case report is retrospective, using de-identified data, and no active intervention was performed for the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Patient consent was obtained for this study.