
Abstract
Objective:
To analyze the data of the cardiac comorbidities, investigational modalities, laboratory parameters, and outcomes of patients with COVID-19 related to cardiovascular system hospitalized in our center.
Methods:
Confirmed cases of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) COVID-19 infection by positive result on polymerase chain reaction testing of a nasopharyngeal sample, who were admitted to Indraprastha Apollo Hospital, Delhi, were included in the study. Demographics, baseline comorbidities, and test results related to cardiovascular diseases were collected and analyzed.
Results:
The study included 1012 patients, admitted in our institute with a COVID-19 positive report. The mean age of the patients was 54.6 ± 6.8 years. The male to female ratio was 1.7:1. The demographic characteristics included diabetes in 38%, hypertensives 45%, history of coronary artery disease 22%, and chronic kidney disease 30%. A total of 426 patients were all treated on HCQS. A total of 7 patients were primigravida with full term pregnancy. The patients were also stratified according to age and demographic characteristics were noted. The total number deceased were 41 with 971 patients making complete recovery. The results showed no change in QTc interval in survivors and nonsurvivors. D-dimer, ferritin, and LDH were raised in all nonsurvivors compared to survivors. Even thrombocytopenia and low albumin levels were noted in nonsurvivors.
Conclusions:
The study revealed no significant change in QTc interval in survivors and nonsurvivors on HCQS. Critically ill patients showed the trends of being underweight, low albumin levels, thrombocytopenia, raised D-dimer, lactate dehydrogenase (LDH), and ferritin levels. Further studies on larger numbers are needed to confirm these findings.
Introduction
Since end of the year 2019, covid-19 has rapidly spread across the globe resulting in a pandemic. COVID-19 is caused by severe acute respiratory syndrome coronavirus 2. This virus invades cells through the angiotensin-converting enzyme 2 (ACE2) receptor and leads to spread of injection. Previous literature states that preexisting cardiovascular disease (CVD) and cardiovascular (CV) risk factors enhance vulnerability to COVID-19. 1 This infection has been associated with CV conditions including acute myocardial injury, myocarditis, arrhythmias, and venous thromboembolism. Also, the response to COVID-19 can compromise the rapid triage of non-COVID-19 patients with CV conditions. As per literature patients with COVID-19 and associated CV comorbidities have higher mortality, 2 and the severity of COVID-19 disease correlates with CV manifestations, 3 it is important to understand the interaction of covid-19 and CVD. This article is aimed at understanding the interrelationship between COVID-19 pandemic and CV morbidity and mortality in a single center.
Methods
This observational study was performed at the Indraprastha Apollo Hospital (IAH), Delhi. All consecutive patients with laboratory-confirmed SARS-CoV-2 infection, and subsequently admitted, were enrolled. The institutional ethics board of IAH approved this study and due to the nature of it being an observational study, waived the need for informed consent from individual patients.
According to the WHO guidance, laboratory confirmation for SARS-Cov-2 was defined as a positive result of real-time reverse transcriptase-polymerase chain reaction (RT-PCR) assay of nasal and pharyngeal swabs.
Clinical data were collected from all patients admitted in ICU and ward. The recorded data included demographic parameters, risk factors, clinical comorbidities, investigational modalities, and laboratory parameters. The subjects were segregated by 2 categories: according to age and according to survivors and nonsurvivors. Various laboratory parameters were compared with these 2 categories and noted. The mean values of the demographic variables were calculated and noted.
The patients underwent ECG and laboratory investigations, which included routine blood investigations like complete blood count, renal function tests, liver function tests, and COVID-19 related investigations like ferritin, LDH, D-dimer, and troponins Echocardiography could be done only in 33% (334) patients, with respect to the clinical condition of the patient and the treating physician. QTc was calculated in all patients on daily basis.
Results
The study analyzed 1012 patients, admitted in our institute with a COVID-19 positive report.
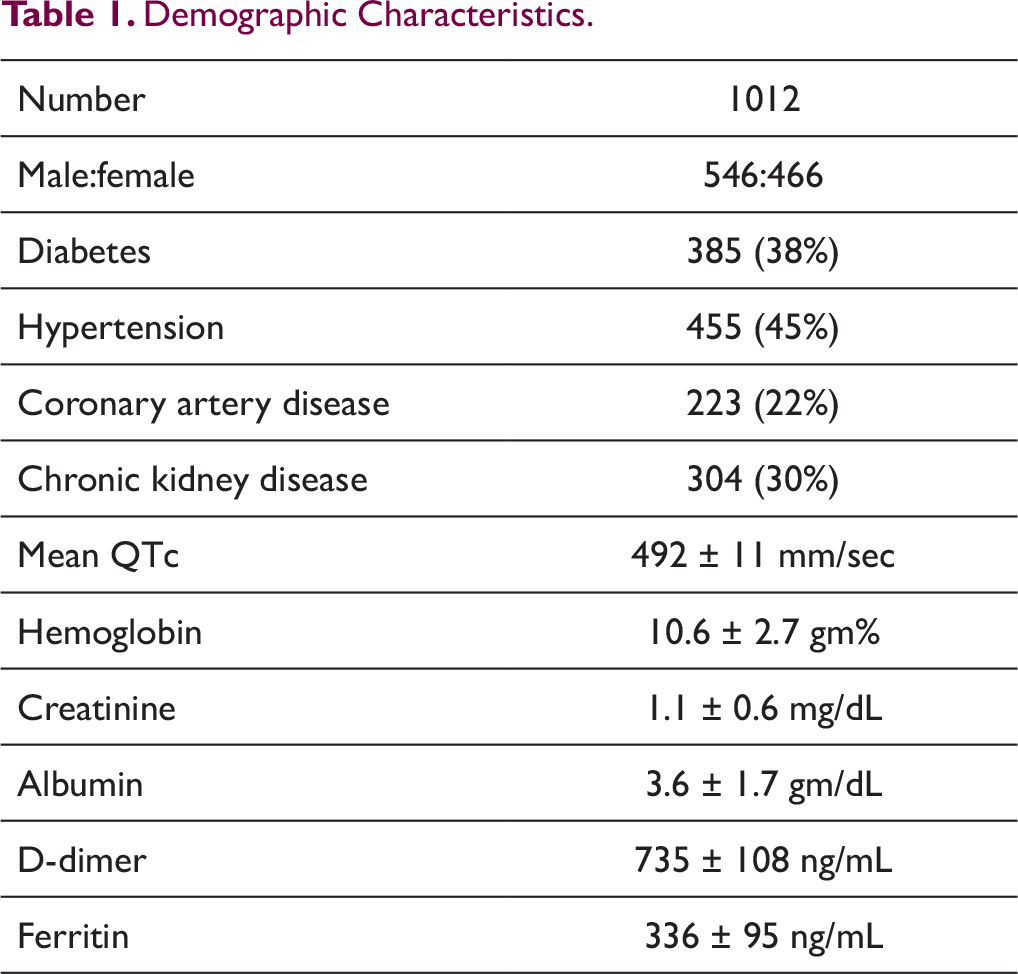
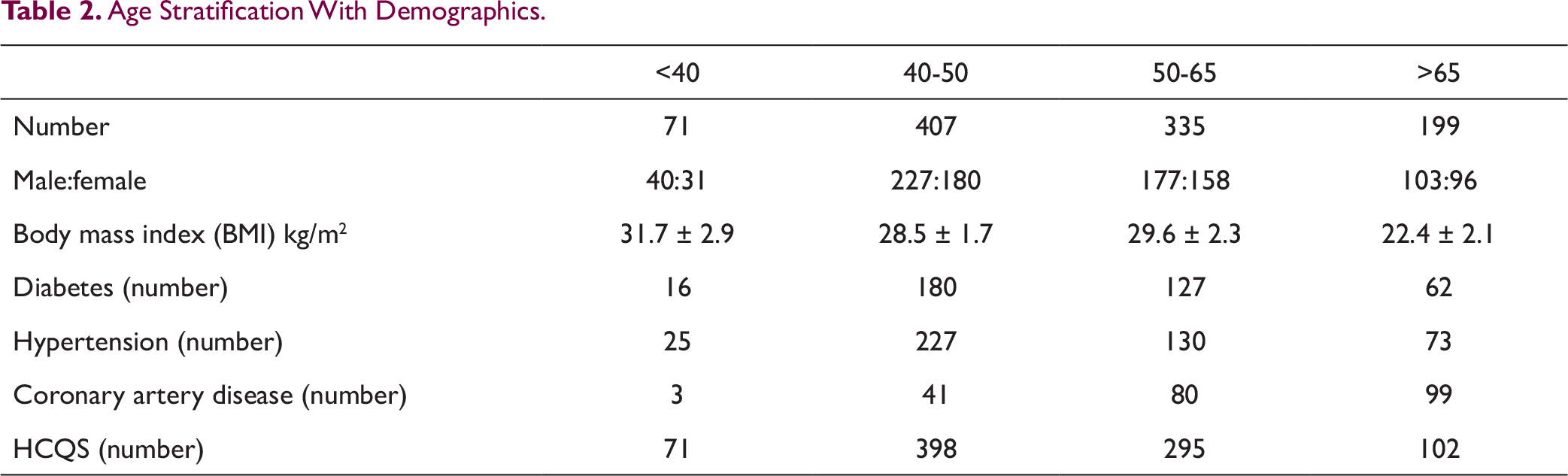
The mean age of the patients was 54.6 ± 6.8 years. The male to female ratio was 1.7:1. The demographic characteristics included diabetes in 38%, hypertensives 45%, history of coronary artery disease 22%, chronic kidney disease 30% (Table 1). In total, 7 patients were primigravida with full term pregnancy. The patients were also stratified according to age and demographic characteristics were noted (Table 2).
Demographic Characteristics.
Age Stratification With Demographics.
Correlation of Indices and Investigations Between Survivors and Nonsurvivors.
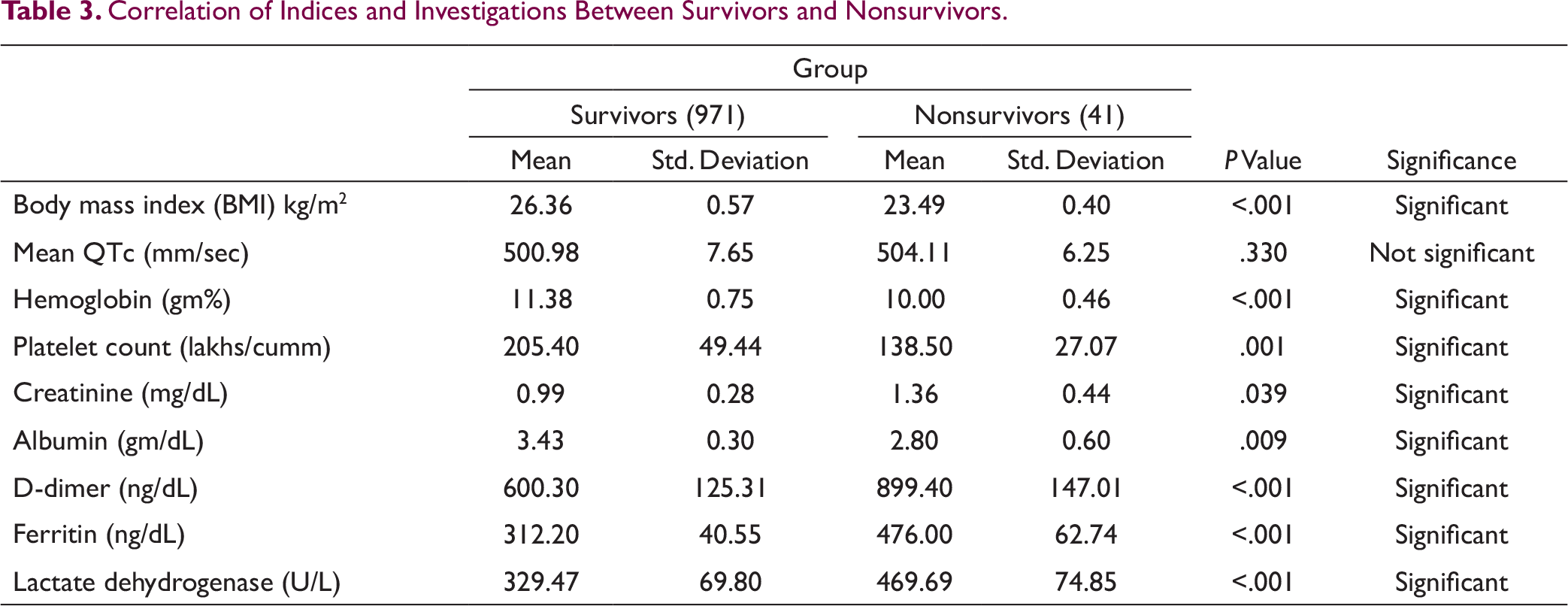
Though many studies have shown prevalence of CV comorbidities like diabetes, hypertension, vascular diseases and others, to have detrimental response in COVID patients. Our study compared these between survivors and nonsurvivors but were not able to conclude with correlation between the pandemic and CV risk factors. The reason may be attributed to the small number of cases.
Discussion
SARS-CoV-2 (COVID-19) is caused by the novel enveloped RNA beta coronavirus. There are various species of this virus, and they can lead to fatal illnesses like SARS, MERS, and COVID-19. Though primary target for SARS-CoV-2 is the respiratory system but there are several mechanisms of CV system involvement.
The common manifestations of CV system leading to CV complications are as follows4, 5:
Direct myocardial injury: SARS-CoV-2 binds to ACE2, a membrane bound aminopeptidase in heart and lungs. The binding of SARS-CoV-2 to ACE2 can result in alteration of ACE2 signaling pathways, leading to acute myocardial and lung injury. Systemic inflammation: COVID-19 may present with severe symptoms, which may be a result of acute systemic inflammatory response and cytokine storm, resulting in multiorgan failure.6, 7 Disproportionate myocardial demand-supply: Impaired myocardial oxygen demand-supply relationship due to raised metabolic demand secondary to systemic infection and hypoxia can lead to acute myocardial injury. Plaque rupture, hypercoagulability, and coronary thrombosis: Systemic inflammation leading to prothrombotic milieu and increased coronary blood flow can precipitate plaque rupture resulting in acute myocardial infarction. Electrolyte imbalances: Electrolyte imbalances can occur in systemic illness and precipitate arrhythmias, esp. in patients with cardiac comorbidities. The interaction of COVID-19 virus with renin-angiotensin-aldosterone system can lead to hypoxia which in turn can lead to tachyarrhythmias.
Cardiovascular Correlation
The literature till date has shown that in patients, severity of COVID-19 disease is related to preexisting CVDs. The studies also showed these comorbidities to be directly proportional to the clinical outcomes.5, 7-9
A meta-analysis of 6 studies of 1527 patients with COVID-19 positivity showed 9.7%, 16.4%, and 17.1% prevalence of diabetes, cerebrovascular disease, and hypertension respectively. 5 In our single center the prevalence was 38% in diabetics and 45% in hypertensives.
A report from the Chinese Center for Disease Control and Prevention described that the case fatality rate (CFR) was 2.3% in 44 672 confirmed cases of COVID-19. 10 When associated with cardiac comorbidities the fatality rate increased to 6%, 7.3%, and 10.5% in patients with hypertension, diabetes, and CVD, respectively. It has been postulated that the impact of various CV comorbidities on outcome of COVID vary among various ethnicity and geographic locations. This data is lacking at present.
Although the prevalence of cardiac comorbidities was noted in our study, but no significant correlation could be established between survivors and nonsurvivors.
Studies have described ST-segment elevation myocardial infarction in COVID-19, but the incidence seems to be low, which was same as observed in our study. Although myocardial insult could have been diagnosed by biochemical parameters, but many patients did not undergo any Trop I investigation in view of no symptoms and no finding in echocardiography.
Tachyarrhythmia and bradyarrhythmia both have been noted in literature. A study of Chinese population with COVID-19 reported 16.7% incidence of arrhythmia. 10 However, no arrythmias were noted in subjects of our study.
Though low number of echocardiography was done in our study. They were consistent with the findings that revealed 30% patients had RV dilatation and dysfunction. This observation was more pronounced than the assumed LV dysfunction. We contemplate that this RV dilatation and dysfunction may be due to pulmonary embolism secondary to VTE or hypercoagubility. 11
Plasma levels of various interleukins IL-6, IL-8, and TNF-∞ have been found to be significantly higher in patients with severe COVID-19. 4 Other inflammatory markers like ferritin can also be elevated in cytokine storm.
In this study the biochemical parameters of nonsurvivors in patients with COVID-19 showed elevated ferritin and IL-6 levels and this may suggest that cytokine release contributes to mortality. 12
Patients with COVID-19 are at increased risk of VTE, which may be related to prolonged immobilization, hypercoagulable state, active inflammation and propensity for DIC. 13 They have significant higher level of D-dimer, fibrin degradation products (FDP), and fibrinogen, compared with healthy controls. 14 Also the levels of D-dimer and FDP titers were higher in patients with severe COVID-19 than those with mild disease. 14
Our data showed similar findings in patients in COVID positive patients having raised D-dimer and ferritin levels. Also, in our study the levels of these inflammatory markers were higher in nonsurvivors compared to survivors.
Laboratory parameters play an important role in patients with COVID-19 and are helpful in prognostication of these patients. The abnormalities include lymphopenia, 15 thrombocytopenia, elevation in lactate dehydrogenase, and raised inflammatory markers, such as C-reactive protein, D-dimer, and ferritin. 16 IL-6 levels have been found to directly correlate with the severity and procoagulant profile of the COVID patients. 17
Among all the parameters—thrombocytopenia 18 and increased D-dimer levels 19 are the most consistently deranged laboratory values with COVID-19, also these have been associated with a higher risk of requiring mechanical ventilation, intensive care unit (ICU) admission and death. When considering other lab parameters, the data is less certain and often contradictory.20, 21
Recently, Tang et al 22 assessed 183 COVID positive patients, 21 (11.5%) of whom died. Among the notable and significant difference between the nonsurvivors and survivors was the increased levels of D-dimer.
D-dimer has been an important marker for venous thromboembolism, and it has been attributed that many sudden deaths may be due to pulmonary embolism secondary to VTE. Thus, the use of prophylactic parenteral anticoagulation may show the single most important benefit in prevention of this CVD by reducing mortality and morbidity.
Our study also revealed a correlation between morbidity, mortality, and BMI. This may be attributed to the “obesity paradox,” which suggests that slight overweight individuals with respect to BM1 do better in most procedures rather than underweight and normal weight patients.
In most patients trop I levels were either normal or mildly elevated, which were not suggestive of coronary syndrome rather it can be attributed to direct myocardial injury due to noncoronary mechanism. Thus, these elevations appear to be myocardial insult and injury and not due to ACS.
Anticoagulant Therapy
In previous literature, various other viral outbreaks like SARS, MERS, influenza also have been shown to have VTE as a thrombotic and thromboembolic event. These VTE may be the result of inflammatory cytokine release. Recent studies have shown similar mechanism in COVID-19, where inflammatory response may lead to thrombotic events.
It is yet unknown whether the hemostatic changes are the direct and specific effect of the virus per se or a consequence of cytokine storm that precipitates the onset of severe respiratory inflammatory syndrome.23-26
In our study we were able to confirm the raised levels of D-dimer, LDH, ferritin with thrombocytopenia between survivors and nonsurvivors.
COVID-19 and VTE—“The Correlation for Prognosis”
A recent study from China indicated that 40% of COVID-19 positive hospitalized patients were at higher risk of venous thromboembolism. 27 Studies have concluded that hospitalized patients with COVID-19, who have respiratory failure, cardiac, and procoagulant comorbidities, 28 patients who are bedridden, and those admitted in ICUs, should receive pharmacological VTE prophylaxis unless any significant contraindications. Also, the choice of agents and dosing should be based on the available guideline for VTE.29-31 The World Health Organization recommends prophylactic daily low-molecular-weight heparins (LMWHs), or twice daily subcutaneous unfractionated heparin (UFH). 32 If these pharmacological prophylaxis has absolute contraindication then mechanical VTE prophylaxis (intermittent pneumatic compression) should be considered.32, 33
In our patients the use of LMWH prophylaxis was initiated late considering the recent inflow of literature on their use worldwide. The number of patients on VTE prophylaxis were low but all showed good and rapid recovery. Thus, emphasizing that the use of VTE prophylaxis in COVID-19 may be a key aspect. The risk of VTE is increased during pregnancy and the postpartum period, though the data regarding this is lacking.34, 35 All patients of primigravida, full term pregnancy and COVID positive received prophylactic anticoagulation in our study, this could have led to good outcomes in their case.
More studies with multivariate analysis are needed to determine how COVID-19 and thrombotic events interact. The data could help to illustrate the various comorbidities associated with COVID-19 especially thromboembolic events. It would also help to identify management strategies to improve outcomes in these patients.
A large international registry of patients with venous thromboembolism—The RIETE registry is in process and would help us answer these questions. Another prospective registry—CORONA-VTE registry is being initiated to study COVID-19 and other CV outcomes.
Conclusions
With the little data available we can postulate that underweight and normal weight individuals according to BMI, low albumin levels, and greater illness severity were associated with increased risk of in-hospital mortality.
The study revealed no change in QTc interval in survivors and nonsurvivors on HCQS (33% of the subjects). Critically ill patients showed the trends of low albumin levels, thrombocytopenia, raised D-dimer, LDH, and ferritin levels.
The need for use of anticoagulation as preventive and therapeutic strategies should be kept in mind to mitigate the thrombotic and hemorrhagic events in these high-risk patients.
Though further studies from round the globe with larger numbers are needed to establish these findings.
Limitations
There were many limitations in our study as follows:
The cardiovascular investigation and management approach was nonuniform and on discretion of the respective treating physician. Troponin and echocardiography were done only of few selected patients. Evaluation of various COVID patient with echocardiography and venous doppler was dependent of the availability of the echocardiographer.
Highlights
No change in QTc interval in survivors and nonsurvivors on HCQS.
Critically ill patients showed the trends of low albumin levels, thrombocytopenia, and raised D-dimer, LDH, and ferritin levels.
Anticoagulation with LMWH provides significant benefit from VTE and hypercoagubility state.