
Abstract
Introduction
Coronavirus Disease 2019 (COVID-19) is associated with an increased incidence of thromboembolic events.1–4 Furthermore, critically ill patients are at a particularly higher risk of venous thromboembolism (VTE). 2 Thus, prophylactic anticoagulation has been a cornerstone of managing critically ill patients with COVID-19. Several anticoagulation regimens have been utilized in practice with the aim of achieving the balance between preventing thromboembolic disease and avoiding bleeding.2–5
Currently the evidence supporting the use of increased dose prophylactic anticoagulation (also referred to as intermediate dosing) in critically ill patients with COVID-19 is scarce.1–5 There are several approaches institutions are utilizing in hospitalized COVID-19 patients with the intent to prevent thrombotic events. These approaches consist of standard dose thromboprophylaxis, intermediate dosing thromboprophylaxis, and therapeutic anticoagulation. 5
Several guidelines recommend the use of standard thromboprophylaxis in critically ill patients with COVID-19 pneumonia.6–8 Recent updates continue to support use of prophylactic low molecular weight heparin (LMWH) or unfractionated heparin (UFH) over therapeutic anticoagulation in critically ill patients. However, the current standard thromboprophylaxis dose may not provide optimal protection and may result in supratherapeutic or subtherapeutic effects in the COVID-19 critically ill population due to extremes in body weight, severity of illness and multi-organ dysfunction. This retrospective study aimed to assess a more individualized approach to anticoagulant dosing in critically ill patients with COVID-19 infection and evaluate outcomes associated with anti-Xa directed anticoagulation compared to other strategies.
Material and Methods
Study Design and Participants
This was a multicenter retrospective cohort study within a single health-system including critically ill patients with COVID-19 from 5 different hospitals. The study period was from March 1st, 2020 to April 30th, 2021. The study was approved by the Saint Luke's Health System's Institutional Review Board (IRB number SLHS-20-109; initial approval August 24, 2020 and addendum approval June 7, 2021).
Patients
Inclusion criteria were: (1) age of 18 years or more, (2) laboratory-confirmed COVID-19 infection, (3) receipt of COVID-19 directed therapy, (4) admission to the intensive care unit (ICU) for at least 24 h, and (5) receipt of anticoagulation during the hospitalization. Exclusion criteria were: (1) receipt of extracorporeal membrane oxygenation (ECMO) support or (2) ICU admission that was deemed to be unrelated to COVID-19.
Outcomes
The primary outcomes were composite of thrombotic events and composite of clinically important bleeding events. Secondary endpoints included deep vein thrombus (DVT) and/or pulmonary embolism (PE), gastrointestinal (GI) bleeding, or other significant bleeding events. The total daily dose of LMWH in anti-Xa directed LMWH was compared to intermediate LMWH dosing. Other outcomes included the need for invasive mechanical ventilation, hospital length of stay (LOS), ICU LOS, the overall incidence of thrombotic and bleeding events, and the type of thrombotic and bleeding events. Baseline characteristics, past medical history and pertinent laboratory values and inflammatory markers were also described.
Anticoagulation Regimens
Anticoagulation regimens were classified into five categories as outlined in Table 1.
Anticoagulation Categories.

Abbreviations: SQ, subcutaneous; LMWH, low molecular weight heparin; mg/kg, milligrams per kilogram; IV, intravenous.
Enoxaparin dosing based on established collaborative drug therapy management agreement (CDTM), Supplemental Appendix 1.
Standard dose thromboprophylaxis was defined as subcutaneous heparin (SQH) 5000 units 2-3 times daily or LMWH (per an established collaborative drug therapy management agreement—Supplementary Appendix 1). During the pandemic, our health system developed a COVID-19 Clinical Taskforce comprised of physicians, pharmacists, and other integral members of the healthcare team. Given the scarcity of data and unknowns regarding empiric therapeutic anticoagulation, the taskforce provided recommendations for intermediate dose thromboprophylaxis, which was defined as LMWH 0.5 milligrams per kilogram (mg/kg) every twelve hours or 7500 units SQH three times daily. Anti-Xa monitoring was utilized at the discretion of the treating clinicians. Our institution utilizes anti-Xa peak values once drug concentrations are at steady state, generally drawn four hours after the third dose of LMWH. Dosing adjustments could be done by pharmacists via our established collaborative drug therapy management (CDTM) agreement (Supplemental Appendix 1). The anti-Xa directed category included patients who received intermediate LMWH dose initially with subsequent adjustment to achieve goal anti-Xa level of 0.2-0.5 IU/mL. A slightly higher anti-Xa goal was used relative to our LMWH CDTM given the concern for hypercoagulability in COVID-19 patients and under the guidance of the health-system COVID-19 taskforce recommendations. Crossovers between different anticoagulation regimens were recorded.
Definitions
Composite of thrombotic events was defined as confirmed PE, DVT, ischemic stroke and/or myocardial infarction (MI). Composite of clinically significant bleeding events was defined as a bleeding that meets at least one of the following criteria: requiring medical intervention, leading to increased level of care (eg, transfer from medical ward to ICU), requiring holding or stopping anticoagulation therapy, bleeding in a critical area or organ, and/or fatal bleeding. An unfavorable outcome was defined as the first event of bleeding or thromboembolism. All the thrombotic and bleeding events were diagnosed by the primary care team based upon clinical findings and were not investigated prospectively. COVID-19 directed therapy included antiviral therapies, monoclonal antibody products, and or immunomodulators. Chronic anticoagulation included prior to admission use of warfarin, apixaban, rivaroxaban, edoxaban, dabigatran, betrixaban, or therapeutic enoxaparin (1 mg/kg twice daily or 1.5 mg/kg daily).
Statistical Analysis
Baseline characteristics and outcomes were described using frequencies with percentages, means with standard deviations (SD) and medians with interquartile ranges (IQR) as appropriate.
Independent samples T-test was used to compare the mean dose of LMWH between the intermediate LMWH regimen and the anti-Xa directed dosing regimen.
To account for the cross-over between different anticoagulation regimens during the hospitalization, survival analysis with the anticoagulation regimen as a time-dependent variable was used to compare the risk of bleeding or thrombosis among different anticoagulation regimens. Patients who did not receive any anticoagulation during the hospitalization were excluded, however, the survival analysis with the anticoagulation regimen as a time-varying covariate accounted for periods of anticoagulation interruption. Hazard ratio (HR) and their 95% confidence interval (CI) were reported. Only the first event was considered in the analysis of its type (ie, recurrent events of the same type were not counted in the same analysis). The analysis of thrombotic events was adjusted for sex, age, history of stroke, history of VTE, VTE on admission, malignancy, antiplatelet therapy and receiving mechanical ventilation. The analysis of bleeding events was adjusted for sex, age, antiplatelet therapy, chronic kidney disease (CKD) and/or receiving renal replacement therapy (RRT) and receiving mechanical ventilation.
Two-sided P-values less than .05 were considered statistically significant. All the analyzes were performed using Stata MP 16.0 for Windows (StataCorp).
Results
Description of the Population
A total of 695 critically ill patients were included in the study (Figure 1). The patients had mean age of 67.4 years (SD = 14.3) and mean body mass index (BMI) of 31.8 Kg/m2 (SD = 8.9). The majority were males (60%) and white (70%). The most common comorbidities were hypertension (HTN) (75.7%), diabetes mellitus (DM) (54.2%), CKD (28.2%) and heart failure (24.5%). Chronic anticoagulation therapy prior to admission was reported in 108 patients (15.5%). Three hundred and two (43.5%) patients required invasive mechanical ventilation. The overall in-hospital mortality rate was 29.9% while the mortality rate in patients who received invasive mechanical ventilation was 52%. Twenty-seven patients (3.9%) were diagnosed with DVT and/or PE on presentation. Table 2 summarizes additional baseline characteristics and past medical history.
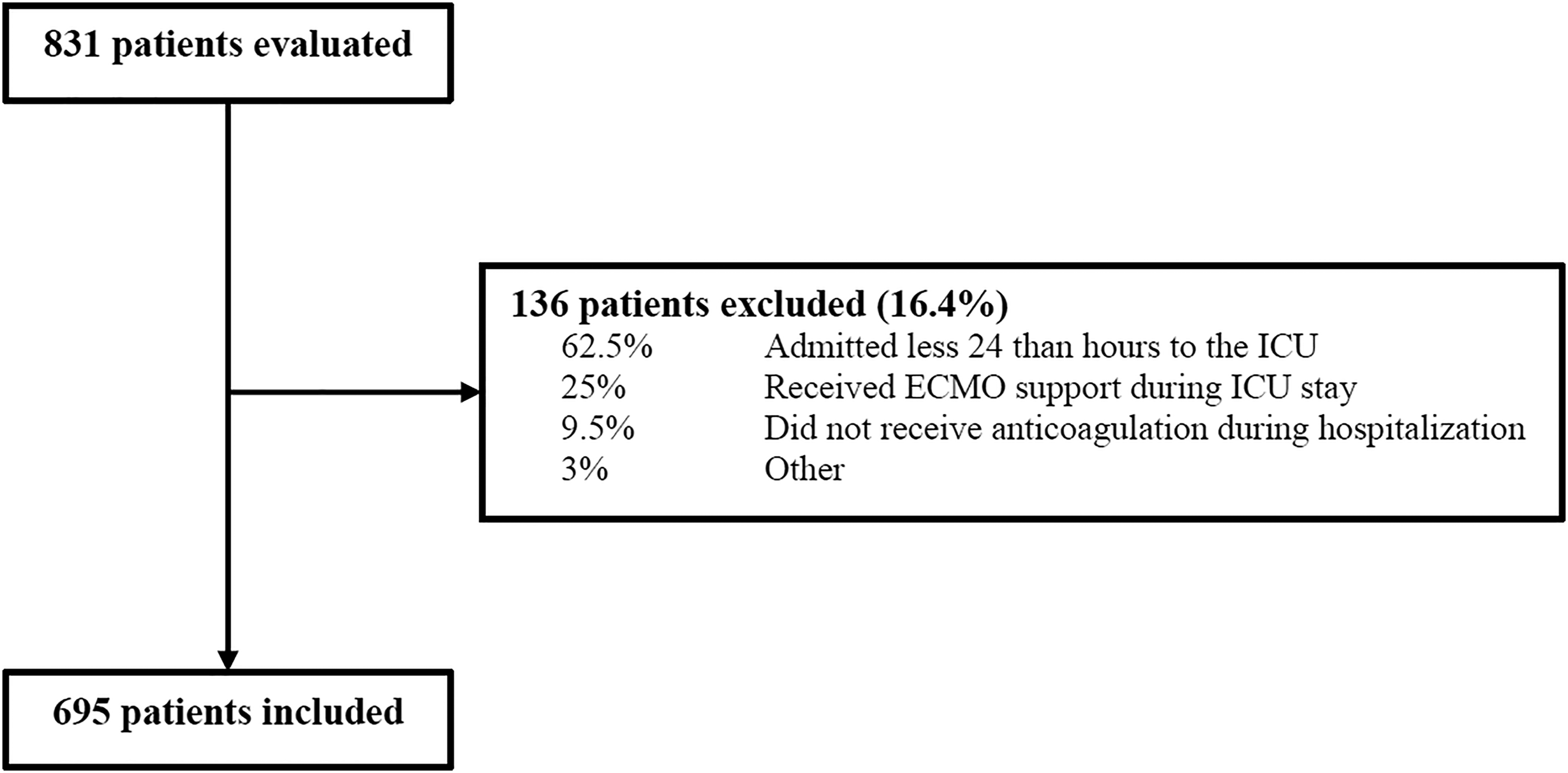
Evaluation, Exclusion, and Inclusion of Patients.
Baseline Characteristics and Past Medical History.
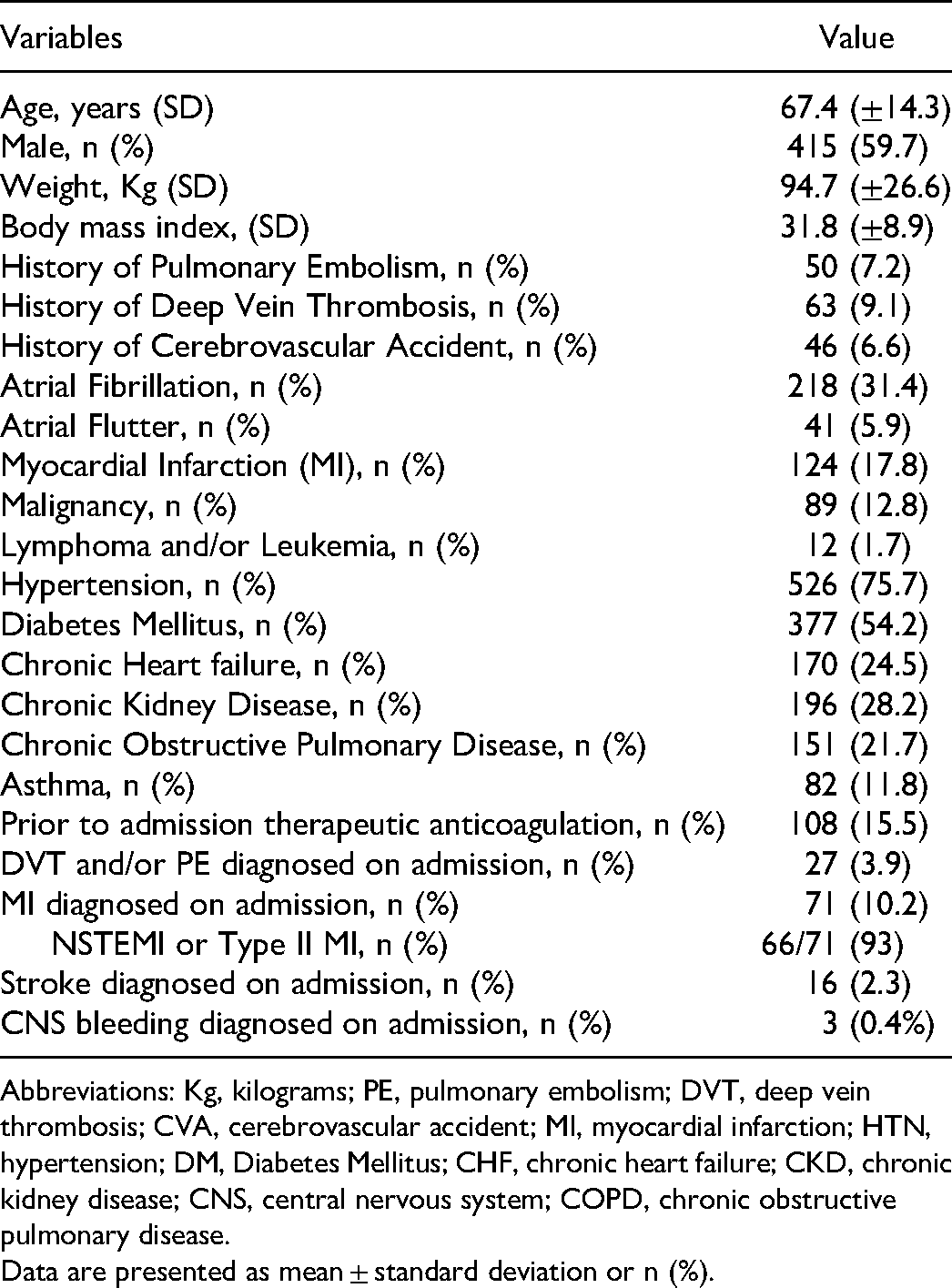
Abbreviations: Kg, kilograms; PE, pulmonary embolism; DVT, deep vein thrombosis; CVA, cerebrovascular accident; MI, myocardial infarction; HTN, hypertension; DM, Diabetes Mellitus; CHF, chronic heart failure; CKD, chronic kidney disease; CNS, central nervous system; COPD, chronic obstructive pulmonary disease.
Data are presented as mean ± standard deviation or n (%).
Laboratory and Inflammatory Markers Results
At hospital admission, patients had mean serum creatinine of 1.58 mg/dL (SD) = 1.84)). Patients had mean initial D-dimer levels of 2.3 mg/L (SD = 3), ferritin of 760 mcg/L (SD = 856) and lactate dehydrogenase of 1120 IU/L (SD = 638). The mean maximum D-dimer level during hospital stay was 2.75 mg/L (SD = 3.6) (Supplementary Table 1).
Interventions
The majority of patients received corticosteroids (93.5%). Therapeutic anticoagulation was utilized in 285 patients (41%) at some point during their hospital stay and thromboprophylaxis was changed to therapeutic anticoagulation in 115 patients (16.5%) (Supplementary Table 2).
Thrombotic Outcomes
DVT and/or PE was diagnosed in 42 patients (6%) during hospitalization. The incidence of any thrombotic event during hospitalization was 9.4% (Table 3). Thrombotic events in the anti-Xa directed thromboprophylaxis cohort was similar to the intermediate LMWH (HR 0.63, 95% CI 0.24-1.6, P = .33). After adjustment for confounding factors, there was also no difference in any thrombotic events between these groups (HR 0.61, 95% CI 0.24-1.56, P = .3). There was no difference in thrombotic events between all the other groups compared to the intermediate LMWH. Twelve patients (1.7%) had a fatal bleeding or thrombotic event in this study. The adjusted analysis of thrombotic events and VTE are shown in Tables 4 and 5, respectively. The detailed and full results the unadjusted and adjusted analysis of thrombotic events and VTE are shown in Supplementary Tables 3 and 4.
Outcomes of the Overall Study Cohort (695 Patients).

Abbreviations: PE, pulmonary embolism; DVT, deep vein thrombosis; MI, myocardial infarction; GI, gastrointestinal; CNS, central nervous system; RP, retroperitoneal; ICU, intensive care unit; CRRT, continuous renal replacement therapy; IQR, Interquartile range; LOS, length of stay.
The number reflects the first documented event
The total number of events differs from the number of patients with at least one event as some patients had more than one event
Defined as platelet less than 100 × 109 per L
Primary Outcomes (Adjusted Analysis).

Adjusted for sex, age, VTE history, mechanical ventilation, history of CVA, history of any malignancy, DVT and/or PE diagnosis on admission, and Antiplatelet therapy.
Adjusted for sex, age, antiplatelet therapy, mechanical ventilation, and CKD and/or RRT.
Secondary Outcomes (Adjusted Analysis).

Adjusted for sex, age, VTE history, mechanical ventilation, history of CVA, history of any malignancy, DVT and/or PE diagnosis on admission, and antiplatelet therapy.
Adjusted for sex, age, antiplatelet therapy, mechanical ventilation, and CKD and/or RRT.
Adjusted for sex, age, VTE history, mechanical ventilation, history of CVA, history of any malignancy, DVT and/or PE diagnosis on admission, CKD and/or RRT, and antiplatelet therapy.
Bleeding Outcomes
The incidence of all major bleeding events during hospital stay was 16.3% (n = 113). GI bleeding was the most common bleeding event in the study (7.2%) and constituted 44.2% of all major bleeding events. Four patients experienced central nervous system (CNS) bleeding events during hospitalization (0.6%). Major bleeding was higher on standard DVT prophylaxis (HR 2.87, 95% C.I. 1.19-6.88, P = .018), intermediate dose SQH (HR 2.95, 95% C.I. 1.45-6, P = .003), and therapeutic anticoagulation (HR 4.03, 95% C.I. 2.17-7.5, P < .001) compared to intermediate dose LMWH in the unadjusted analysis. The increased hazard of major bleeding remained statistically significant on standard DVT prophylaxis (HR 2.6, 95% C.I. 1.1-6.3, P = .03), intermediate dose SQH (HR 2.4, 95% C.I. 1.15-5, P = .019), and therapeutic anticoagulation (HR 3.6, 95% C.I. 1.88-6.8, P < .001) after adjusting for confounding factors (Table 4). GI bleeding was higher on intermediate dose SQH (HR 3.2, 95% C.I. 1.2-8.7, P = .02), and therapeutic anticoagulation (HR 3.1, 95% C.I. 1.3-7.8, P = .013) compared to the intermediate dose LMWH in the unadjusted analysis. However, GI bleeding was not statistically significant for intermediate dose and therapeutic anticoagulation compared to the intermediate dose LMWH in the adjusted analysis. The full results of the adjusted primary and secondary bleeding outcomes are shown in Tables 4 and 5.
Intermediate dose SQH and therapeutic anticoagulation were associated with increased risk of unfavorable outcomes compared to intermediate dose LMWH in the unadjusted analysis and the adjusted analysis (Table 5 and Supplementary Table 4).
Anti-Xa Directed Thromboprophylaxis
Anti-Xa directed thromboprophylaxis was utilized in 125 patients. Sixty-one patients (49%) had an anti-Xa within target, while 54 patients (n = 43%) were above the peak target and ten patients (8%) fell below goal with the first anti-Xa result.
The mean daily LMWH dose in the anti-Xa directed LMWH dosing group (n = 125) was 0.82 mg/kg/day compared to 0.99 mg/kg/day in the intermediate dose LMWH (n = 231) (P < .001).
Discussion
To our knowledge, this is the first study to evaluate anti-Xa directed thromboprophylaxis compared to other anticoagulation strategies in critically ill COVID-19 patients. In this retrospective analysis, the hazard of thrombotic and bleeding events on anti-Xa directed thromboprophylaxis was similar to the intermediate dose LMWH (standard practice at our institution) with 20% lower mean daily dose of LMWH.
The overall incidence of any thrombotic event in our study was 9.4%, which is consistent with the 9% major thrombotic events rate reported in the REMAP-CAP, ACTIV-4a, and ATTACC trials. 9 In-hospital mortality in our cohort was 29.9%, which is consistent with ICU mortality reported by the Society of Critical Care Medicine Discovery Viral Infection and Respiratory Illness Universal Study (VIRUS): COVID-19 Registry at 35.3%. 10 Mortality in patients who received mechanical ventilation was 52% which is also comparable to mortality rates of 34% to 70.5% reported by other studies.11–14
The anti-Xa goal of 0.2 to 0.5 IU/mL was adapted from previously published literature.15–17 A small prospective study evaluated whether anti-Xa peak goal of 0.2 to 0.5 was achieved on standard dose LMWH. Sixty eight percent (74 cases) were below the anti-Xa peak goal. 15 Small retrospective studies evaluated anti-Xa activity in COVID-19 patients on thromboprophylaxis.18,19 Standard dose LMWH prophylaxis may not be sufficient to provide adequate VTE prophylaxis in critically ill COVID-19 patients as forty nine percent required a LMWH dose of 1 mg/kg/day to achieve the goal peak range in our study. Nevertheless, there were a significant number of patients (43%) that had anti-Xa peak levels above target, which could lead to an increased risk of bleeding. Our findings suggest the potential benefit for offering an individualized approach for anticoagulation dosing in critically ill patients in general, and specifically in critically ill patients with COVID-19.
The incidence of major bleeding events reported by other COVID-19 studies was 2.3–6.3%, significantly lower than the incidence in our study.9,20–22 A recent retrospective study compared the bleeding risk on anticoagulation in critically ill patients with COVID-19 to other respiratory viral illnesses. The incidence of major bleeding events was 14.7%, which is consistent with our findings. 23 A single center retrospective study reported 21% incidence of hemorrhagic events in critically ill COVID-19 patients. However, the authors did not include their hemorrhagic event definition, which limits the extrapolation of their data. 24 The definition and criteria for major bleeding events used in this study was different from the definition by International Society of Thrombosis and Haemostasias for non-surgical patients, which was used in previously published studies. 9 We did not include patients with an acute hemoglobin drop of 2 g/dL in our major bleeding criteria due to the retrospective nature of our study. However, all other criteria were similar to guideline definitions. In our study, 41% of patients received therapeutic anticoagulation. In addition, 43% of patients in the anti-Xa directed LMWH group were above target at the first anti-Xa, which can likely be extrapolated to be true for the rest of the intermediate dose LMWH cohort. Our anticoagulation strategies therefore may have been considered more aggressive than standard of care, thus explaining our findings of increased bleeding events.
In a retrospective study of 3334 patients hospitalized in New York City for COVID-19, the rate of DVT/PE was 6.2%. Events rates for critically ill patients (n = 829) were 6.2% and 9.4% for PE and DVT, respectively. 25 The INSPIRATION trial, a multi-center randomized trial evaluating intermediate-dose vs standard-dose prophylactic anticoagulation in critically ill COVID-19 patients also reported a DVT/PE rate of 3.4%. 26 Additionally, the STOP-COVID trial, a multicenter cohort study including 3239 critically ill COVID-19 patients, observed 6.3% incidence of VTE in their population. 27 The incidence of DVT and/or PE overall (including diagnosis on presentation and during hospital stay) and during hospitalization in our study was 9.9% and 6%, respectively. Our results are consistent with rates reported in other major studies.
In a recent retrospective study by Tacquard et al, the use of high dose prophylactic anticoagulation compared to standard DVT prophylaxis was associated with a significant reduction in the thrombotic events critically ill COVID-19 patients. 28 In our study, we did not observe a reduction in DVT/PE or any thrombotic event with any of our dosing strategies. This difference can be explained by the difference in the comparator groups since the majority of our patients either received intermediate dose LMWH, intermediate dose SQH or therapeutic anticoagulation at the discretion of the providers. Forty-one percent of patients received therapeutic anticoagulation at some point during their hospitalization. Our findings highlight the similar outcomes between different high-dose prophylactic anticoagulation and therapeutic anticoagulation in preventing thrombotic events. This further adds to the growing evidence suggesting that therapeutic anticoagulation should not be used empirically in critically ill patients with COVID-19, as there is no reduction in VTE events and may result in increased risk of bleeding.9,27
Previous studies have reported that the median time to thrombotic and bleeding events were 6 and 15 days, respectively.29,30 The reported median hospital LOS for patients on mechanical ventilation was 17 days (IQR: 9.7, 28). 10 The median hospital and ICU LOS in our cohort were 15 (IQR: 9, 23) and 7 (IQR: 3.5, 14.3) days, respectively. The median hospital and ICU LOS for the mechanically ventilated patients in our cohort were 21 (IQR: 13.3, 30) and 15 (IQR: 7.6, 24) days, respectively. Outcomes were collected throughout the hospital and ICU stay, which allowed us to assess for a longer period of time compared to other studies where the data collection was limited to 14 days. 28
In our study, standard dose DVT prophylaxis (SQH or LMWH) had a significantly higher incidence of all major bleeding compared to intermediate dose LMWH. The most utilized DVT prophylaxis in COVID-19 patients in our health system is intermediate dose LMWH. Given the retrospective design of this study, it would have been challenging and impractical to discern why prescribers elected to use standard dosing vs. intermediate dose LMWH in certain patients. We believe that the standard DVT prophylaxis may have been utilized in patients already deemed to be at an increased risk of bleeding. This may explain why we saw an increased bleeding incidence in the standard prophylaxis cohort.
We believe that our results present a potential benefit for anti-Xa monitoring in critically ill COVID-19 patients, as 46% of patients were supratherapeutic in the anti-Xa group. Without anti-Xa monitoring, many of the patients in the intermediate dose LMWH group would have been categorized as therapeutic anticoagulation, which did not show to improve outcomes or decrease VTE risk in critically ill COVID-19 patients and increase risk of bleeding events.
We attempted to control for some of the confounding variables within our study. Patients in the intermediate dose SQH cohort had a higher incidence of all major bleeding, GI bleeding (unadjusted analysis), and other major bleeding. This regimen was primarily used in patient with CKD or acute kidney injury, or in whom LMWH would be otherwise contraindicated. The risk of major bleeding is generally increased in patients with CKD. 31 We believe an individualized SQH approach with monitoring may be warranted to help reduce the risk of bleeding. There is limited data on the best practice for this and further studies are required to identify the optimal monitoring parameters in high risk patients.
Limitations
The retrospective nonrandomized design is the main limitation of our study. There was a significant crossover between the various anticoagulation regimens, which we attempted to account for by utilizing the time varying covariate analysis. We collected the exact time and date of starting and stopping each anticoagulation regimen, and we accounted for each anticoagulation duration of action when determining the stop date and time in an effort to account for continuing anticoagulation effect. However, we cannot control or estimate all the lingering or sustained effects of certain anticoagulants after the switch to a different therapy, which may impact thrombotic or bleeding events. We did not report time to event in the study given the crossover between the anticoagulation regimens. Given the retrospective nature of the study we were unable to collect all data elements. Nevertheless, we were able to collect all data required for the primary and secondary analysis. Lastly, we adjusted for some of the confounding factors that would impact thrombotic and bleeding events. It is possible that there are other confounding factors we were unable to account for, and might have influenced prescribers to use certain anticoagulation regimen over another.
Conclusion
Our findings suggest that LMWH dosed to achieve an anti-Xa peak goal of 0.2 to 0.5 IU/mL provides comparable protection against thrombotic events in COVID-19 patients with lower mean daily doses. We believe this strategy offers the advantage of a more individualized approach for anticoagulation in critically ill COVID-19 patients. Our findings also suggest that therapeutic anticoagulation does not provide additional benefits and has a higher risk of major bleeding. Further randomized controlled trials are needed to confirm our findings.
Supplemental Material
sj-docx-1-cat-10.1177_10760296221116350 - Supplemental material for Anti-Xa Directed Thromboprophylaxis in Critically Ill Patients with Coronavirus Disease 2019
Supplemental material, sj-docx-1-cat-10.1177_10760296221116350 for Anti-Xa Directed Thromboprophylaxis in Critically Ill Patients with Coronavirus Disease 2019 by Adham Mohamed, PharmD, Shelby M Shemanski, PharmD, Mohamed O Saad, PharmD, Jeannette Ploetz, PharmD, FCCM, Michelle M Haines, MD, Andrew B Schlachter, MD, and Majdi S Hamarshi, MD, FCCP, FCCM in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-2-cat-10.1177_10760296221116350 - Supplemental material for Anti-Xa Directed Thromboprophylaxis in Critically Ill Patients with Coronavirus Disease 2019
Supplemental material, sj-docx-2-cat-10.1177_10760296221116350 for Anti-Xa Directed Thromboprophylaxis in Critically Ill Patients with Coronavirus Disease 2019 by Adham Mohamed, PharmD, Shelby M Shemanski, PharmD, Mohamed O Saad, PharmD, Jeannette Ploetz, PharmD, FCCM, Michelle M Haines, MD, Andrew B Schlachter, MD, and Majdi S Hamarshi, MD, FCCP, FCCM in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-3-cat-10.1177_10760296221116350 - Supplemental material for Anti-Xa Directed Thromboprophylaxis in Critically Ill Patients with Coronavirus Disease 2019
Supplemental material, sj-docx-3-cat-10.1177_10760296221116350 for Anti-Xa Directed Thromboprophylaxis in Critically Ill Patients with Coronavirus Disease 2019 by Adham Mohamed, PharmD, Shelby M Shemanski, PharmD, Mohamed O Saad, PharmD, Jeannette Ploetz, PharmD, FCCM, Michelle M Haines, MD, Andrew B Schlachter, MD, and Majdi S Hamarshi, MD, FCCP, FCCM in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-4-cat-10.1177_10760296221116350 - Supplemental material for Anti-Xa Directed Thromboprophylaxis in Critically Ill Patients with Coronavirus Disease 2019
Supplemental material, sj-docx-4-cat-10.1177_10760296221116350 for Anti-Xa Directed Thromboprophylaxis in Critically Ill Patients with Coronavirus Disease 2019 by Adham Mohamed, PharmD, Shelby M Shemanski, PharmD, Mohamed O Saad, PharmD, Jeannette Ploetz, PharmD, FCCM, Michelle M Haines, MD, Andrew B Schlachter, MD, and Majdi S Hamarshi, MD, FCCP, FCCM in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-5-cat-10.1177_10760296221116350 - Supplemental material for Anti-Xa Directed Thromboprophylaxis in Critically Ill Patients with Coronavirus Disease 2019
Supplemental material, sj-docx-5-cat-10.1177_10760296221116350 for Anti-Xa Directed Thromboprophylaxis in Critically Ill Patients with Coronavirus Disease 2019 by Adham Mohamed, PharmD, Shelby M Shemanski, PharmD, Mohamed O Saad, PharmD, Jeannette Ploetz, PharmD, FCCM, Michelle M Haines, MD, Andrew B Schlachter, MD, and Majdi S Hamarshi, MD, FCCP, FCCM in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
The authors thank Ozzy Hoversten, PharmD for his assistance with the initial IRB submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.