
Abstract
Background:
Pain relief is a fundamental human right, yet evidence suggests access to analgesia is not equitably distributed. People with severe mental illness (SMI) experience significant disparities in healthcare during life, which may also be mirrored at the end of life. This systematic review examines the extent of inequities and underlying factors contributing to disparities in pain care for people with SMI and life-threatening diseases.
Methods:
A mixed-methods systematic review of MEDLINE, EMBASE, AMED, CINAHL, PsycINFO and EThOS (January 2000–September 2024), hand-searching key journals and citation tracking. Two reviewers independently screened studies, and data were extracted using a standardised approach. A narrative synthesis was used to integrate findings.
Results:
Two thousand nine hundred seven records were identified, with eight studies meeting the inclusion criteria. Study quality ranged from ‘very low’ to ‘high’. All quantitative studies were retrospective analyses of routine healthcare data, examining analgesic prescribing for people with schizophrenia. Despite variability in outcome measures, all studies found that individuals with schizophrenia received significantly less analgesia than those without SMI. Four qualitative studies explored clinicians’ views on providing pain care to patients with SMI; only one study included patient experiences. Identified barriers to optimal pain management included patient-related factors (e.g. difficulties in pain expression, behavioural symptoms), clinician-related factors (e.g. diagnostic overshadowing, stigma) and systemic issues (e.g. fragmented care, restrictive prescribing practices).
Conclusion:
There is a striking lack of research on pain assessment and management for people with SMI and life-threatening illnesses, yet available evidence indicates clear inequities in care. These disparities may be driven by intersecting structural, social and clinical barriers, contributing to poorer end-of-life experiences. Addressing this gap requires urgent action from clinicians, policymakers and researchers. Future work should combine population-based studies to quantify prescribing disparities with qualitative research involving people with lived experience of SMI and their carers. Participatory, co-produced approaches are essential.
Keywords
Introduction
Pain is a common symptom associated with life-threatening illnesses, for example, cancer. 1 At the end of life, 80%–96% of cancer patients will experience pain.2–5 Relief from pain is a human right.6,7 Good symptom management is associated with improved patient and family quality of life 8 and is demonstrated to confer survival advantages.9–11 Opioids are highly successful in controlling pain in around 90% of patients with advanced cancer 12 and are considered a ‘quality marker’ for end-of-life care. 13 Despite their ubiquity and availability of management guidelines,14,15 evidence demonstrates that prescribing opioids is not uniformly distributed across society.16–19
Severe mental illnesses (SMIs) are those that are prolonged and recurrent, impair activities of daily living and require long-term treatment. 20 Although there is some debate about which conditions come under the SMI umbrella, there is consensus that the term includes schizophrenia, bipolar disorder and depression with psychotic symptoms. Several other conditions are sometimes included, such as schizoaffective disorder and persistent delusional disorder, with symptoms that overlap with schizophrenia, bipolar disorder or severe depression.21,22 People with SMI have markedly reduced life expectancy, typically 12–15 years fewer than the general population.23–28 Most excess deaths are from natural causes (notably cardiovascular disease, cancer, respiratory disease and diabetes), with suicide and injury contributing a smaller share.26–28 Drivers include lifestyle risks, medication-related metabolic syndrome and systemic barriers to physical healthcare.23–28 Together, these factors lead to earlier onset and poorer control of long-term conditions and underpin the observed mortality gap.
Inequity in access to and provision of healthcare for people with SMI has been previously reported.22,29–32 Unfortunately, these inequities have been shown to extend to end-of-life care. A ground-breaking systematic review of the literature on palliative care for people with SMI conducted by Woods et al. 20 in 2008 identified four main themes contributing to inequitable care: decision-making capacity and advance care planning, access to care, provision of care and system issues. In 2019, Donald and Stajduhar 33 updated this review and, despite identifying 29 new articles, the themes remained broadly similar. The MENLOC study, 34 a robust mixed-methods systematic review, identified four themes associated with these inequities that included the structure of the system, professional issues, contexts of care and living with SMI, and made some recommendations for addressing them. Most recently, a systematic review of 43 articles by Sadowska et al. examined psychiatric co-morbidities and outcomes in palliative and end-of-life care. 35
Whilst these reviews allude to pain assessment and management for people living with SMI that may potentially be influenced by these themes, none made pain a detailed focus of their investigation. Consequently, important questions remain about the equity and adequacy of treatment for this symptom, which is central to patients’ experiences. The aim of this systematic review was, therefore, to examine to what extent inequities are present in the assessment and management of pain between people with and without SMI living with life-threatening diseases, and if present, why might they exist.
Methods
Protocol and registration
The study protocol was prospectively registered with PROSPERO (CRD42023416706). 36 Reporting follows Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Design
We conducted a mixed-methods systematic review including a narrative synthesis of quantitative and qualitative studies. Although our inclusion of diverse study designs shares some features with a scoping review, our research question was deliberately narrow and we applied systematic review methodology throughout, in line with PRISMA guidance. We therefore describe this work as a systematic review, whilst acknowledging that the breadth of study designs reflects the exploratory state of the evidence base. The research paradigm underpinning this review is represented by pragmatism.37,38 This approach is based on the proposition that researchers should use the philosophical and/or methodological approach that works best for the research problem that is being investigated. It is here that pragmatist researchers consider the research question to be more important than either the methods they use or the paradigms that underlie the methods. 39 Moreover, Maxcy suggests that pragmatism emerges as both a method of inquiry and a device for the settling of battles between research purists and more practical-minded scientists. 40 We adhere to this sentiment and rationalise the conjoint use of quantitative and qualitative methods as being complementary and necessary to address the overarching aim of this review.
Criteria for considering studies for this review
We included studies published in English in any journal from 2000 onwards. We chose to focus on contemporary healthcare structures, diagnostic coding practices and research evidence. The widespread adoption of ICD-10 diagnostic coding systems across European and other high-income countries during the late 1990s and early 2000s created greater consistency in healthcare data and research. Further, the WHO Cancer Pain Relief Guidelines Second Edition were published in 1996, feeding into post-2000 practice. Papers could be included if they had any reference to pain assessment or pain management in the population of interest. Table 1 describes inclusion and exclusion criteria based on characteristics of the publication, setting, study type, population, outcome and comparison. In line with the findings of a preliminary scoping search, our criteria for ‘life-threatening disease’ were purposefully wide to allow for the inclusion of data from retrospective studies starting at the point of death, where some deaths may have been sudden or unexpected. By referring to ‘life-threatening diseases’, we aimed to include the possibility of people facing the risk of death of any cause, not only through advanced life-limiting disease, and even if they ultimately survived. Our rationale was that in the face of a threat to life, pain should be assessed and managed regardless of the underlying illness and not only within the scope of what is usually referred to as ‘palliative care’.
Inclusion and exclusion criteria.

SMI: severe mental illness.
Information sources and search strategy
Electronic databases were searched from January 2000 to April 2023, and subsequently updated to September 2024: MEDLINE, AMED (Allied and Complementary Medicine), EMBASE (Excerpta Medica Database) and PsycINFO were searched via Ovid. CINAHL (Cumulative Index to Nursing and Allied Health Literature) was searched via EBSCO. EThOS (Electronic Theses Online Service) was searched via the British Library website in May 2023, but an updated search in September 2024 was not possible due to a cyber-attack. 41 Manual searching of key journals from 2019 to 2024 included Palliative Medicine, Journal of Pain and Symptom Management, Journal of Psychosomatic Research, Psychological Medicine and Pain. Grey literature and web searches were conducted to identify leads to published articles, including Marie Curie online, European Association for Palliative Care, Macmillan online, NICE (National Institute of Clinical Evidence) evidence search, OpenGrey and conference abstracts on EMBASE (and manual searches). The reference lists of included studies, as well as relevant book chapters, systematic reviews, narrative reviews and other relevant publications were manually searched for other potentially relevant publications. Search results were imported to EndNote 21 (ClarivateTM) and duplicates were removed.
The search terms were developed by G.E., J.K. and A.P. based on preliminary scoping searches, which yielded key papers on the topic of palliative care for people with SMI. The search strategy combined populations of ‘people with a life-threatening disease’ and ‘people with SMI’ with ‘pain assessment’ or ‘pain management’. Search terms included subject headings and free text terms and were adapted for each electronic database. The search terms used for the EMBASE search are available as Supplemental File 1.
Study screening process
Using eligibility criteria, G.E. screened titles and, where appropriate, abstracts that were identified from any information sources. Where eligibility could not be determined based on title and abstract, full texts were retrieved and reviewed against eligibility criteria. S.L.-C. repeated this process independently for all titles identified by electronic searches. A final decision regarding the inclusion of reports in the systematic review was reached through discussion between G.E., S.L.-C. and J.K. All decisions were made unanimously.
Data collection process
Data were extracted from each of the included reports independently by G.E. and J.K. using an agreed data extraction proforma. This included information about the manuscript, study, participants, methods, results and authors’ conclusions. Quantitative and qualitative results were extracted regarding the original study’s main outcome measure as well as those outcome measures which were relevant to our review question and were categorised as relating to ‘pain assessment’ or ‘pain management’. We recorded whether SMI diagnoses were explicitly stated. If not, we noted ‘diagnosis not specified’ and, where relevant, used service type as a proxy indicator only; such studies were not used to make SMI-specific inferences. The level of statistical or clinical significance was recorded as reported within the papers. We noted any assumptions made about the study data or findings as comments in the data extraction form. A final form was mutually agreed upon following discussion.
Quality assessment and weight of evidence
The methodological quality of each study and its risk of bias were independently assessed by G.E. and J.K. using Critical Appraisal Tool Checklists published by The Joanna Briggs Institute (JBI). 42 Disagreements were resolved through discussion. Based on conventions used in a previous study, 43 we rated the quality of reports as ‘high’ for scores 90%–100% on the checklist, ‘medium’ for scores 80%–89%, ‘low’ for scores 70%–79% and ‘very low’ for scores <70% Conflicts were resolved by discussion. Evidence was weighted using Gough’s Weight of Evidence (WoE) Framework, 44 independently scored by G.E. and J.K., and the agreed total WoE was used to inform conclusions drawn from the results.
Data analysis and synthesis
We used a narrative approach to describe data from included studies using tables and text. For quantitative data, the main findings relating to the assessment or management of pain in each study were described, alongside the measures used to estimate them, regardless of quality assessment. Meta-analysis was not undertaken because the measures were heterogeneous.
For qualitative data, we conducted a framework analysis following the steps described by Furber. 45 These included familiarisation with the data, development of an a priori analytical framework informed by our research questions, indexing through systematic coding of study findings and charting data into matrices to enable comparison across studies. Coding was carried out independently by two reviewers (G.E. and J.K.), with discrepancies resolved through discussion to ensure consistency and rigour. Data were then synthesised thematically, with emergent themes refined iteratively through team discussions with A.P. and S.L.-C.
Further narrative synthesis of results across quantitative and qualitative studies considered the quality assessment and total WoE for each paper.
Results
Included papers
The results of electronic and manual searches are summarised in the PRISMA flow diagram (Figure 1). The electronic search yielded 2907 manuscripts. After de-duplication, 2794 records were screened, of which 33 warranted full-text evaluation. Five papers met all inclusion and none of the exclusion criteria and were included in this review. Three further papers were identified through citation or reference list searching and included.
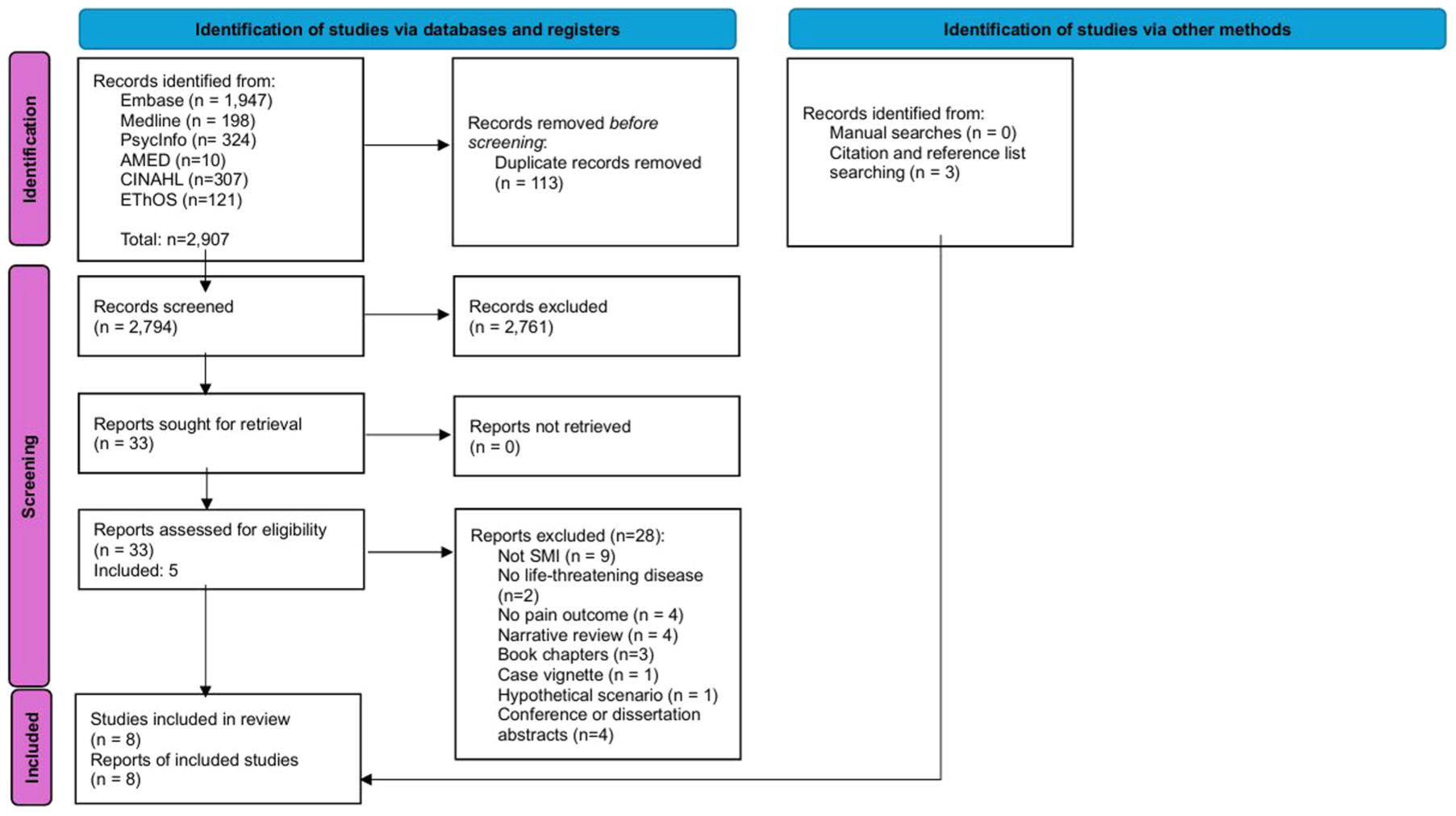
PRISMA flow diagram.
Characteristics of included studies
Study design
Three quantitative,46–48 four qualitative49–52 and one mixed-methods 53 studies were included, and their main characteristics and findings are summarised in Tables 2 and 3. Of the quantitative studies, two46,47 used a population-based retrospective cohort study design, which was based on routinely collected administrative data. The third quantitative study 48 used a retrospective cross-sectional design. Only the study by Lin et al. 46 was specifically designed to examine pain management, but all three reported prescribing analgesics during a designated period before death. These quantitative studies drew on evidence originating in Taiwan, 46 Canada 47 and the United States. 48
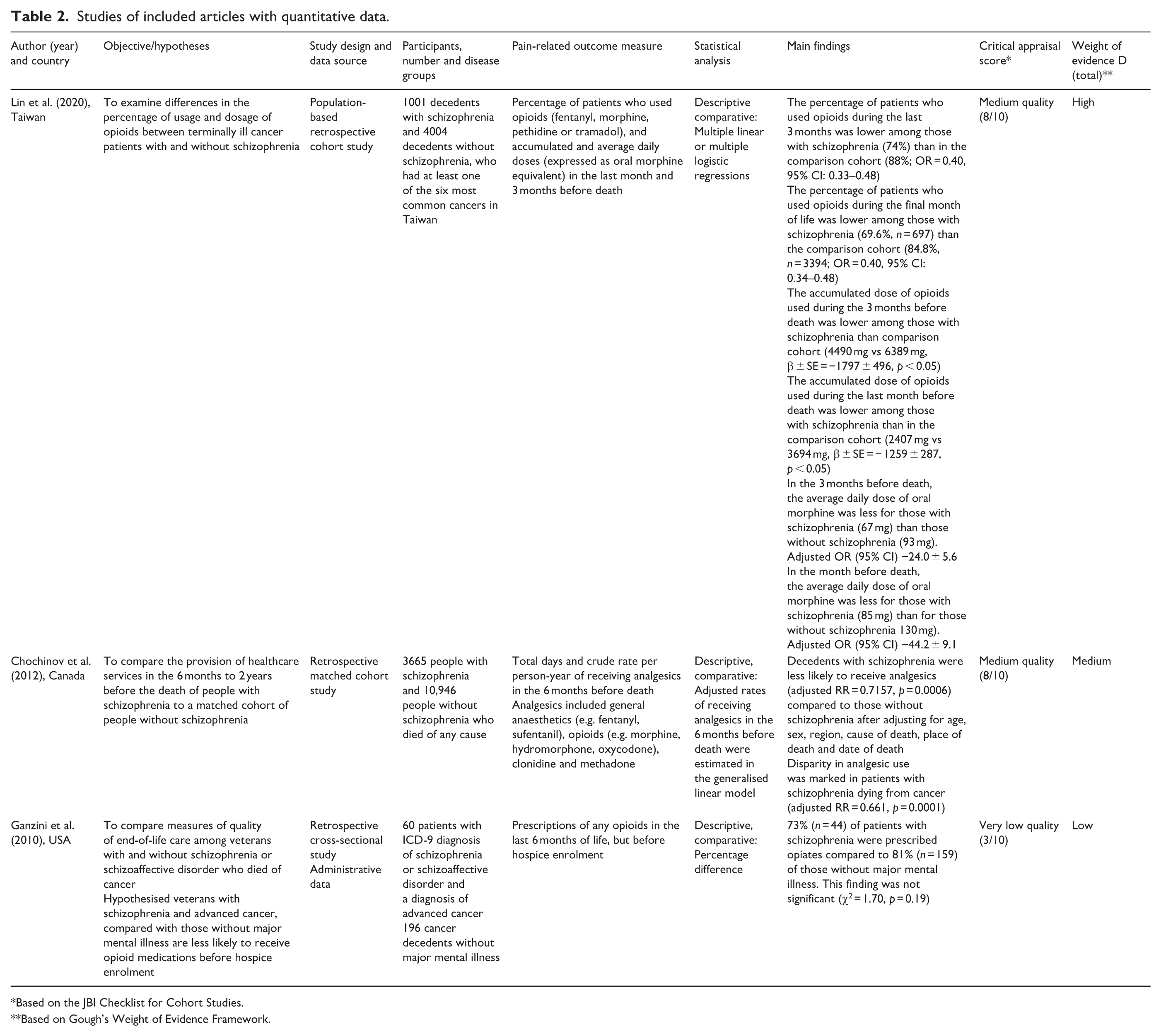
Studies of included articles with quantitative data.
Based on the JBI Checklist for Cohort Studies.
Based on Gough’s Weight of Evidence Framework.
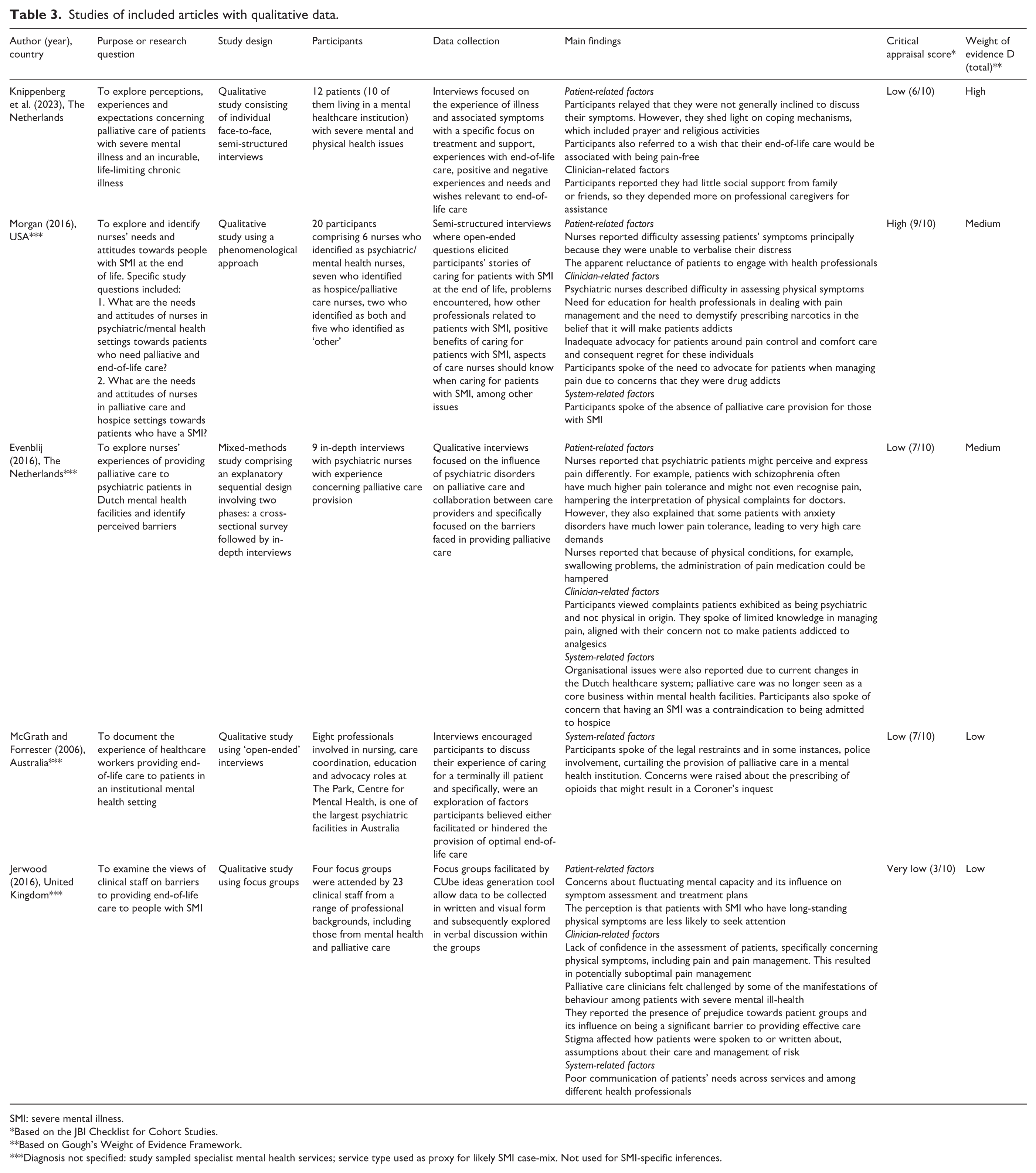
Studies of included articles with qualitative data.
SMI: severe mental illness.
Based on the JBI Checklist for Cohort Studies.
Based on Gough’s Weight of Evidence Framework.
Diagnosis not specified: study sampled specialist mental health services; service type used as proxy for likely SMI case-mix. Not used for SMI-specific inferences.
The study by Evenblij et al. 53 was reported as a mixed-methods study; however, outcomes relating to pain assessment or pain management were only identified in the qualitative findings. Consequently, we designated it as a qualitative study. Participants in four qualitative studies were clinicians working in the United Kingdom, 50 United States, 49 Netherlands 53 and Australia. 51 The fifth qualitative study included people with SMI and a life-limiting diagnosis from the Netherlands. 52
Participants and comparator
Two quantitative studies46,48 included only patients who had died of cancer and one 47 included people who died of any cause. SMI diagnosis in these studies was limited to schizophrenia (also schizoaffective disorder in Ganzini et al. 48 ). Whilst pain was not documented as a symptom in the original administrative data, we assumed that many decedents for whom analgesia was prescribed experienced pain, as this is the most common indication for prescribing analgesics. In each quantitative study, the comparison (control) cohort was selected in a 1:3 to 1:4 ratio from within the same population of decedents but had no mental illness diagnoses.
Four qualitative studies sampled clinicians working in specialist mental health facilities or services in Western health systems.49–51,53 These settings typically manage people with severe mental disorders; however, specific SMI diagnoses were not reported in these studies. We therefore treated service type as a pragmatic proxy for a likely SMI case-mix, flagged these studies as diagnosis not specified in Table 3, and did not use them to make SMI-specific inferences. Instead, we interpreted their findings alongside Knippenberg et al., 52 the only patient-participant study that explicitly reported diagnoses (severe depression, bipolar disorder, schizophrenia or substance use disorder) and life-threatening conditions (diabetes, COPD, chronic heart failure or incurable cancer). We recognise that admission and eligibility thresholds for specialist mental healthcare vary by country and over time; accordingly, these inferences may not generalise beyond Western settings.
Outcome measures
Quantitative studies reported different measures of analgesic prescription. Lin et al. 46 studied both the proportion of decedents receiving analgesics and the accumulated and average daily dose of oral opioids in milligrams, whilst Chochinov et al. 47 examined adjusted relative rates of receiving analgesics. Ganzini et al. 48 used a binary variable of ‘opioid prescription’. From the qualitative studies, themes relating to pain assessment and pain management were extracted from manuscripts.
Quality assessment and weight of evidence
Methodological quality (JBI) varied across the eight included studies: 1/8 high, 2/8 medium, 3/8 low and 2/8 very low (Tables 2 and 3). Only one study was rated high quality. 49 We then applied Gough’s WoE, which considers methodological quality and relevance/fit to the review question. WoE ratings were high for two studies – Lin et al. 47 and Knippenberg et al. 52 – medium for three, and low for three.
We integrated WoE ratings into the narrative synthesis as follows: (i) within each theme, studies were ordered by WoE; (ii) core claims were supported primarily by high-WoE studies; (iii) medium/low-WoE studies were used to add context, demonstrate variation or generate hypotheses; and (iv) where findings conflicted, we privileged higher-WoE evidence and noted residual uncertainty.
Quantitative data analysis
Table 2 summarises the characteristics and main findings of the three quantitative studies. Lin et al. 46 identified that the percentage of patients who received opioids in the last 1 or 3 months of life was lower in patients with schizophrenia compared with controls (74% vs 88% for the 3-month analysis). The average daily doses in mg (expressed as oral morphine equivalent) and accumulated doses in milligrams were lower for those with schizophrenia during the same periods (85 mg vs 130 mg, and 2407 mg vs 3694 mg, respectively, for the month before death). These differences were statistically significant after adjusting for age, sex, primary malignancy, year of death and income.
Results by Chochinov et al. 47 were similar, where in the 6 months before death, decedents with schizophrenia were, after adjusting for age, sex, region, cause of death, place of death and date of death, less likely to receive analgesics compared to controls, with a relative rate (aRR) of 0.7157 (p = 0.0006). This disparity was more marked in those dying from cancer (aRR = 0.661, p = 0.0001).
Ganzini et al. 48 reported that 73% of decedents with schizophrenia had been prescribed any opioids in the last 6 months of life (before hospice enrolment) compared with 81% of controls. However, this was not statistically significant (χ2 = 1.70, p = 0.19). No propensity score adjustment was made for potential differences between the two groups in age, marital status and financial situation. Furthermore, this comparison relied on ‘prescription of any opioids’ at any time during the last months of life and did not consider the dose in milligrams, duration of medication, recurrence or frequency of such prescriptions. Given these limitations, the WoE of this paper was assessed as ‘low’.
Taken together, the quantitative data rely exclusively on retrospective analysis of medical records and suggest that people with SMI were prescribed fewer opioids in the last months of life than people without mental illness diagnoses.
Qualitative data analysis
Five of the studies contributed qualitative data: three49,52,53 used semi-structured interviews, one used open-ended interviews 51 and one 50 used focus groups. Their characteristics and main findings are summarised in Table 3. In the four studies with clinicians, participants were nurses or other staff, as in Jerwood et al. 50 and McGrath and Forrester. 51 The studies were designed to explore their experiences and views about working with patients with SMI at the end of life and to identify barriers to good end-of-life care. None of the studies explicitly mentioned pain assessment or management in their objectives. However, Evenblij et al. 53 adapted their semi-structured interview guide to include a question about how patients interpreted or expressed their illness-related pain. Knippenberg et al. 52 represented the only study using semi-structured interviews to specifically explore perspectives of people living with SMI and a life-threatening condition. Their interview guide included questions about ‘symptoms’ but did not focus on pain assessment or management.
Overall, the relative volume of data concerning pain assessment or pain management was low. We have included quotes expressing participants’ experiences and attitudes regarding end-of-life care when issues that could also affect pain assessment or pain management are present. Themes were grouped into patient-related factors, clinician-related factors and system factors (refer to Table 4).
Presentation of themes and subthemes from qualitative studies.

SMI: severe mental illness.
Of the patient-related factors, issues relating to pain communication and engagement with healthcare were expressed by clinicians and patients alike, and appeared to be the most prevalent. Clinician-related factors were expressed by clinicians working in palliative care and in mental health, and were not mentioned by patients. Of the system-related factors, fragmentation was consistently present. Legal consequences were only referred to by the Australian paper. 51 Taken together, the qualitative findings highlight a complex interplay of patient-, clinician- and system-level influences on pain assessment and management for people with SMI. Patients were often reluctant or unable to verbalise their symptoms, whilst clinicians described difficulties in recognising pain and a tendency to prioritise psychiatric explanations over physical ones. Systemic barriers such as fragmented services and restrictive policies compounded these challenges. Yet, alongside these difficulties, some accounts pointed to advocacy by staff and patients’ clear desire for pain-free care, illustrating both gaps and opportunities for improvement. Importantly, only one study captured patient perspectives, leaving their voices largely absent from the evidence base.
Discussion
To our knowledge, this is the first attempt to collate and analyse evidence about the assessment and management of pain in patients with SMI living with life-threatening conditions. Our main finding is that to date, the scientific and clinical communities appear to have paid very little attention to this question; therefore, the volume of research that has been conducted is extremely low. Eight publications of variable quality and WoE were included in this mixed-methods systematic review, of which seven were designed for other purposes.
However, the synthesis of this limited body of evidence through the analysis of quantitative and qualitative data together has revealed noteworthy themes, which are presented in Figure 2. The main finding of the quantitative studies was that people with schizophrenia (the only category of SMI to have been studied) are prescribed less analgesia at the end of life than people without a mental illness diagnosis. The themes raised in the qualitative studies shed light on reasons for this difference: clinicians are less competent and/or confident in assessing and managing pain in people who may express pain differently and demand less medical attention, and this is exacerbated by a disjointed system which does not easily lend itself to partnership working. In some jurisdictions, this can be further complicated by a concern about a police inquiry after the death. The impact of this situation is heightened by the recognition that some people with SMI may require more analgesia and active advocacy.

Synthesis of quantitative and qualitative results.
Main findings of included studies
People with SMI are prescribed less analgesia at the end of life
Different outcome measures were used in the quantitative studies; therefore, their results could not be pooled. However, all indicate decedents with schizophrenia received less analgesia in the last months of their lives compared with those without mental illness. This finding is worrying as it suggests inequitable and likely suboptimal pain management in a vulnerable patient group. By using a mixed-methods approach to our systematic review, we were able to explore why differences may be present. This exercise confirmed some hypotheses raised by the authors of the quantitative studies,46,47 and revealed other important themes.
People with SMI may communicate their distress differently
Clinicians in two of the qualitative studies49,53 reported that people with SMI may either experience or express pain differently, for example, through behaviours rather than words and that this, in turn, could affect the way clinicians respond to their pain. There are published reports of patients with schizophrenia who presented with restlessness but denied pain in the context of cancer or myocardial infraction.54,55 Whether these findings reflect differential pain experience or expression in people with schizophrenia has been debated in subsequent papers, albeit not in the context of a terminal disease. In a narrative review, Bonnot et al. 56 wrote: ‘many case reports concerning patients with schizophrenia who had painful medical illnesses without reports of pain contributed to the concept of pain insensitivity in schizophrenia’. However, their review of clinical and experimental data supports the conclusion that this is related to different modes of pain expression, not experience. Later reviews reached similar conclusions in non-cancer pain.57,58
Knippenberg et al. 52 observed that patients affirmed this theme of reduced pain expression, articulating very little concern about their current physical symptoms. Indirectly, further evidence for this silence comes from clinicians interviewed by McNamara et al., who raised a variety of issues regarding their work with patients with schizophrenia at the end of life, however, pain was rarely mentioned. 59
Like others, people with SMI desire to be pain-free
Studies from clinicians’ perspectives did not address patients’ expectations for the future, but Knippenberg et al. reported that patients expressed a wish to be free of pain at the end of life and emphasised they expected appropriate attention to their somatic problems as part of overall high-quality care. 52 This was an important finding of three other qualitative studies60–62 which did not meet the criteria for inclusion in our review. Participants in these studies had SMI but not a life-threatening condition and were presented with hypothetical scenarios for end of life. They found that most people with SMI were inclined to accept a higher dose of analgesia, even if it resulted in impaired communication. They rated ‘being in pain and suffering’ as an important end-of-life concern.60,62
This muted yearning to be pain-free, coupled with the largely non-verbal expression of pain, places greater responsibility on clinicians to be mindful and attentive to pain and its management in people with SMI. This recommendation was also emphasised by Onwumere et al. 63 whose systematic review of pain management in people with SMI highlighted inequities in the inclusion of people with pain and SMI in clinical trials and their access to clinical interdisciplinary services for pain management.
Access to healthcare for people with SMI is limited by engagement and accessibility
Clinicians and patient participants in the included qualitative studies mentioned a reluctance of people with SMI to engage with healthcare professionals. From the patients’ perspective, this was manifested by a need to be left alone, 52 and from a clinician’s perspective, a frustration around issues of compliance with medical or nursing recommendations.49,50 Over and above patients’ ability to engage with healthcare, clinicians and the health system itself can present barriers to access to good pain assessment and management. This theme is present in other studies exploring end-of-life care for people with SMI.20,33,34,64,65 In the studies included in our review, clinicians raised concerns about the fragmentation of the healthcare system. These include a lack of an appropriate place to provide good palliative and end-of-life care to people with SMI. Calls for partnership between palliative care and psychiatry or mental health services have been made by several authors,20,33,34,65–67 but successful models have been anecdotal. One model is the Ottawa Inner City Health Project, which successfully provided shelter-based palliative care to homeless people with a life-threatening diagnosis, the majority of whom also had SMI. 68 This programme relied on care delivered by nurses, care workers, physicians and palliative care specialists and resulted in good pain control for 24 of 25 patients.
Case studies and opinion pieces (which were not included in this systematic review) provide some useful advice, for example, good multi-disciplinary team collaboration, 69 case-conferencing between palliative care and mental health specialist nurses, 70 or using consultation-liaison psychiatrists as leaders for improvement. 71 Spilsbury et al. point out that access to non-palliative community services by decedents with schizophrenia in Australia was not lower than that of their counterparts without schizophrenia, concluding that barriers to access are at least partly health system-driven rather than patient-driven. 72 We did not identify any established model which demonstrated sustainable success in reducing healthcare system fragmentation to achieve good pain assessment and management for people with SMI and life-threatening illnesses. However, models of care used within mental health services outside the context of end-of-life care could potentially be adapted. 73
Clinician-related factors: Confidence and competence, and biases and preferences
A consistent theme in the qualitative studies related to clinicians’ confidence and competence in managing patients who present with psychiatric as well as physical needs, for example, diagnostic overshadowing. This concern has been widely expressed in previous literature.33,34,59,66,74,75 Problems related to insufficient training in pain management, end-of-life care or psychiatry in primary nursing training, amplified by a lack of joint working and cross-training opportunities during the working lives of most nurses. A strong recommendation to deliver cross-training was unanimously and repeatedly presented.20,33,34 Foti et al. provide a good example of a local model which tested various methods to deliver this education. 76
Another issue for clinicians has been referred to as ‘stigma’. Within included studies, we found quotes indicating clinicians felt averse to caring for people with SMI at the end of life, either through fear or through personal preference to avoid certain types of interactions. This sentiment spans decades and geographies in the published literature,20,25,34,59,64,66,71,77,78 and has been acknowledged by the Lancet Commission on Global Mental Health. 79 Through its impact on social relationships, psychological and behavioural responses and the availability of resources, stigma is a known barrier to social inclusion, which in turn could result in reluctance to seek help, for example, from healthcare services. 80 One approach to addressing this is through campaigns that create opportunities for inter-personal contact between people with and without the lived experience of mental disorders. 81 Negative encounters in mental health services, including coercion, seclusion and restraint, are associated with psychological harm, erosion of therapeutic alliance and subsequent avoidance or delay in future service use. 82 These traumatic experiences can undermine trust and engagement with physical and palliative healthcare; services may wish to adopt trauma-informed approaches. 83
Poor attention to pain assessment and management in people with SMI is not limited to end of life. Stubbs et al. found that one-third of community patients with psychoses experienced clinically relevant pain, which was associated with more severe psychiatric symptoms and a poorer quality of life, yet <3% were prescribed analgesics. 84
The neglect of patients’ voices
Only one study directly explored the views and experiences of people with SMI living with a life-threatening disease. 52 In this example, using semi-structured interviews, participants were specifically asked about their symptoms. Many participants had to be prompted to discuss their symptoms, and some openly acknowledged that they were not inclined to discuss them. From the little shared about pain, it appears that patients were accustomed to their illness and symptoms’, and yet that they ‘considered experiencing no pain or unnecessary suffering to be important aspects of their end of life’. The latter theme resonates loudly with the findings of studies that explore hypothetical end-of-life scenarios with people with SMI.61,62,85
This absence of voices of people with SMI in published research reiterates the absence of social justice and the centre-place of those with SMI as a marginalised group in research who live and die in society.20,33,86 Published papers often focus on challenges faced by researchers in obtaining these voices,55,59 but it is important to acknowledge that people with SMI are rarely asked to participate. Indeed, there are good examples of successful recruitment of people with SMI to research about end-of-life care,60–62 where they have provided rich accounts. These examples should be used as a guide for future research.
Quality of the included studies
The quality and WoE of the eight included studies were variable and ranged from ‘high’ to ‘very low’, which may affect confidence in the results. By JBI criteria, Ganzini et al. 48 rates ‘low quality’, important since this study is frequently cited to demonstrate that the quality of end-of-life care was higher for people with schizophrenia than it was for others. This may reflect their unique population (veterans receiving care from the Department of Veterans Affairs), or the accuracy of the medical records upon which the study relied.
Strengths and limitations
This systematic review is the first to examine the important question of how pain is assessed and managed in people living with SMI and life-threatening diseases. The overall review includes experiences of 19,872 patients from clinical records and 72 interviews, including 12 people with SMI. The main strength of the review lies in the systematic mixed-methods design, enabling us to examine differences in care and why these may be present. This consequently reveals a complex and nuanced picture of pain assessment and management.
However, our review has limitations. Despite an attempt to apply widely inclusive search terms, three studies were not captured by the electronic search. These studies were not designed to address our research question and none included information about pain in their abstract. Future search terms may need to include physical symptoms and not just pain to increase sensitivity.
The quantitative studies only included people with schizophrenia or schizoaffective disorder. We had to make assumptions about the data, for example, that in a population-based retrospective cohort, most patients died of life-threatening disease (not from unnatural causes). When the cohort included decedents over 10 years old, 47 we assumed most would have been adults >18 years. We assumed that for the majority of patients, analgesia was prescribed principally for physical pain, yet there was no mention of pain severity or the effectiveness of analgesia. We had to accept that authors’ choices of what medications to include as ‘analgesics’ accurately reflected prescribing habits in their respective populations.
Some qualitative studies explored clinicians’ views about working in mental health services without specifying the diagnoses of those cared for in these facilities. We assumed most would have SMI. Quotes did not always directly relate to pain assessment or management, and we had to infer meanings whilst remaining transparent in our reporting. We had limited information about clinicians’ ability to make comparisons to care given to people without SMI. We could not consider recall bias and its effect on the themes raised. We also did not have access to the original data, so we relied on the interpretation of the original authors.
All the research studies included in this review were undertaken in high-income countries with developed health systems. Evidence from low- to middle-income countries is currently absent, although SMI is present. This warrants attention in future research. We are also aware there is a general lack of consensus surrounding the term ‘severe mental illness’ which presented itself as a challenge for database and related searching. Whilst we believe we have included appropriate search terms, we may have missed some published material.
Finally, our study design excluded published case reports as well as any publications in languages other than English. During data collection and thematic analysis, we realised that themes raised by reflections on individual cases strongly resonated with themes we identified in the included studies.
Recommendations
For individual clinicians, proactive enquiry about and assessment of pain in people with SMI and life-threatening illness is essential. Diagnostic overshadowing and atypical expression of symptoms that include pain should be considered. People with lived experience of SMI and their carers must be involved in the co-production of processes to routinely improve the assessment and management of pain, alongside clinicians from primary to tertiary care, including palliative care and pain management teams, healthcare commissioners, policymakers and third-sector organisations.
Healthcare systems should facilitate effective structures for joint working and training between physical health and mental health providers so that the complex needs of this population are adequately recognised and met. Some advocate that this could be enhanced by the development of subspecialist palliative care psychiatry, encapsulating the psychiatric care of patients receiving palliative care, integrated palliative care, and psychiatric care in both medical and psychiatric settings and training of psychiatrists in palliative care skills. 87 Training of mental health nurses, who are central to the provision of mental health services, must include specific attention to the assessment and management of pain at the end of life.
Further research is needed to understand why differences are present in pain assessment and management for people with SMI and life-threatening conditions, their causes and how they can be overcome. Neglecting these issues is ethically indefensible, deepening health inequity and compromising principles of fairness and dignity.88,89 Including people with lived experience of SMI as patients or carers in the co-design of research projects to explore these issues will enhance relevance, respect and equity.
People with SMI may face other intersectional barriers to pain management for example, those from minority ethnic communities 43 and those from materially deprived areas, which makes the fragile position of this at-risk population more vulnerable. The paucity of research in this area may reflect perceived difficulties of conducting research among marginalised, vulnerable and very ill populations90,91 where access to patients is difficult, mental capacity is sometimes questionable, 92 consent is challenging to obtain, and the benefit-to-burden ratio is difficult to determine. However, these assumptions must be challenged and useful lessons drawn from research that was successfully conducted.52,62
The next stage of research should begin with a population-based observational study to examine the rates and doses of analgesics prescribed to people with and without SMI who are living with life-limiting conditions such as cancer, where pain is common. Building on this, qualitative studies involving people with lived experience of SMI, their relatives, and unpaid carers are needed to understand why disparities in pain care persist. People with lived experience and their carers should be actively involved in the co-production of processes to improve pain assessment and management. Future research should therefore prioritise participatory approaches that centre the voices of people with SMI, working alongside clinicians, commissioners and policymakers to ensure relevance, respect and equity. Finally, examples of successful models of good practice should be identified, critically evaluated and tested for scalability.
Conclusion
There is a striking lack of research on pain assessment and management for people with SMI and life-threatening illnesses, and the patients’ voice is missing from all but one research paper addressing this topic. However, available evidence indicates that compared with the general population, people with SMI are prescribed less analgesia at the end of life, and their engagement with palliative care services is complicated by deeply rooted patient-, clinician- and system-related factors such as miscommunication, stigma, clinical competence and structural inequity. Addressing this gap requires urgent attention from clinicians, policymakers and researchers. Future research should prioritise participatory approaches that centre the voices of people with SMI and explore interventions that integrate mental health and palliative care to reduce inequities.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251397552 – Supplemental material for Are there inequities in the assessment or management of pain for people with severe mental illness living with life-threatening diseases? A mixed-methods systematic review
Supplemental material, sj-docx-1-pcr-10.1177_26323524251397552 for Are there inequities in the assessment or management of pain for people with severe mental illness living with life-threatening diseases? A mixed-methods systematic review by Gilli Erez, Sophie Law-Clucas, Annabel Price and Jonathan Koffman in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524251397552 – Supplemental material for Are there inequities in the assessment or management of pain for people with severe mental illness living with life-threatening diseases? A mixed-methods systematic review
Supplemental material, sj-docx-2-pcr-10.1177_26323524251397552 for Are there inequities in the assessment or management of pain for people with severe mental illness living with life-threatening diseases? A mixed-methods systematic review by Gilli Erez, Sophie Law-Clucas, Annabel Price and Jonathan Koffman in Palliative Care and Social Practice
Footnotes
Acknowledgements
This report is independent research part funded by the National Institute for Health and Care Research, Yorkshire and Humber Applied Research Collaborations NIHR200166. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health and Care Research or the Department of Health and Social Care.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Any other information in this review is available from the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.