
Abstract
Introduction
With the rapid advancement of technology, smart technologies have permeated various sectors, including palliative care in healthcare. Based on the available literature, similar studies have elucidated the application of individual and isolated smart technologies in palliative care, with their benefits, and limitations. This research, therefore, focuses on the conceptualisation of various smart technologies and makes holistic recommendations on the effective and efficient use of smart technologies in healthcare to enhance palliative care.
Purpose
The purpose of this study is to systematically review the existing literature to conceptualise the role of various key smart technologies in palliative care, and their benefits and make recommendations on how smart technologies can enhance healthcare in palliative care.
Methodology
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines were adopted in this study. Using the keywords: ‘smart technologies’, ‘healthcare’ and ‘palliative care’ (using Booleans AND/OR in different ways, including their synonyms), an exhaustive search was done on four major databases: MEDLINE, PubMed, Scopus and CINAHL. Resultantly, 19 articles met the inclusion criteria and were analysed.
Findings
The main results reveal that smart technologies enhance the quality of life and efficiency of palliative care, notably telemedicine, wearable devices, and mobile health apps. They reduce hospital visits and carer stress by improving patient-doctor communication, enabling remote monitoring, and forecasting health outcomes. However, there are challenges such as the digital divide, privacy issues, and the need for comprehensive integration and training into the current frameworks.
Conclusion and implications
The study emphasises the significant impact of smart technologies in improving palliative care. It emphasises the importance of considering technological, ethical, and practical factors to ensure that these advancements truly enhance palliative care. This research has important implications for healthcare professionals and policymakers, indicating a need for a patient-centred palliative care model that integrates technology more effectively.
Introduction
Palliative care is an important aspect of healthcare, especially for patients dealing with long-term illnesses.1,2 According to Ooko et al., 3 the main goal of palliative care is to provide patient-centred support and improve the quality of life for individuals with life-limiting conditions. However, there are challenges in delivering effective palliative care, especially in remote or resource-limited areas.4,5 The emergence of smart technologies in healthcare offers potential solutions to these challenges. 6 The integration of smart technologies in palliative care is a new and exciting area that has not been fully explored. By utilising advanced technologies like the Internet of Things (IoT), sensors, blockchain, cloud computing, telemedicine (also referred to as telehealth), artificial intelligence (AI), and 5G technologies, amongst others, smart healthcare systems can transform how palliative care is delivered.6–9 These technologies enable remote monitoring, personalised care, and improved communication between patients and clinicians, making it possible to bridge the gap in remote palliative care services. 4 Despite their potential benefits, the integration of smart technologies into palliative care is still at an early stage, with a lack of comprehensive remote healthcare systems (or distance access) specifically tailored for palliative care needs. This systematic review aims to examine and summarise the current state of smart technologies in palliative care, analysing their impact, obstacles, and future possibilities. The primary objective of this study is to address the research question: ‘How can smart technologies enhance the delivery and effectiveness of palliative care in remote settings?’
Background
Defining palliative care and its objectives
According to the World Health Organisation (WHO), palliative care is a method of providing care that aims to improve the quality of life for individuals and their families who are facing life-limiting illnesses.3,10,11 It aids in preventing and relieving suffering through early detection, evaluation, and management of pain in addition to attending to the physical, psychological, and spiritual needs of the patient. 12 Even when mortality is inevitable in palliative care, there must be some consensus and concerted effort to improve palliative care. Unquestionably, early integration of this treatment is essential since it prevents and addresses physical, psychological, and spiritual manifestations of the condition.11,13 In fact, improved supportive care and early palliative care have been confirmed to lead to better results.14,15 When palliative care is incorporated into treatment plans on time, it can save expenditures, improve quality of life by reducing symptoms, satisfy patients, families, and staff, and shorten stays in intensive care units and hospitals.16,17 For this reason, palliative care seeks to enhance the quality of life for those who are facing terminal illnesses or chronic conditions. 18
The burden of chronic conditions on healthcare
One of the most significant economic and social challenges that any country has to confront is healthcare, especially chronic conditions. 19 Chronic conditions that require palliative care include cancer, heart conditions such as congestive heart failure (CHF), kidney failure, Alzheimer's, and chronic obstructive pulmonary disease (COPD) among many others. 14 There is no hope for recovery in palliative care scenarios and therefore, the principal objective should be to lessen the effects of the illness through better management of symptoms, higher levels of satisfaction with the care received, and less psychological distress.17,20 This includes taking care of the patient's discomfort and symptoms as well as their family's psychological problems and stress.3,18 With the rapid advancement of technology, smart technologies have permeated various sectors, including healthcare. As a result, palliative care could greatly benefit from integrating smart technologies.
Evolution and direction of smart technologies in palliative care
Smart technologies in palliative care have progressed from basic telehealth services to complex, interconnected systems that use wearable gadgets, mobile health apps, IoT sensors, and AI. 21 This advancement highlights a growing emphasis on individualised, patient-centric care to enhance the well-being of individuals with life-limiting illnesses. In contrast to the broader realm of smart healthcare technologies that typically concentrate on diagnosing, treating, and preventing various conditions, smart technologies in palliative care are specifically designed to address the distinct requirements of patients in need of comfort, symptom control, and emotional support, according to Payne et al. 22
Additionally, the trend of smart technologies in end-of-life care is moving towards improving interaction among patients, caregivers, and healthcare professionals; enabling remote tracking and control of symptoms; and aiding in end-of-life preparation and decision-making. 23 Nonetheless, Mills et al. 24 argue that this progression highlights a move from a responsive to a preventative method in addressing end-of-life care requirements, allowing for timely actions and individualised care strategies.
Comparative analysis: palliative care versus general healthcare technologies
Smart technologies used in palliative care, such as telehealth, remote monitoring and electronic medical records have similarities with general healthcare technologies. 4 They leverage data analysis and artificial intelligence to influence medical judgments and boost patient results. 22 Nonetheless, their distinctiveness lies in their emphasis on enhancing quality of life and the total management of symptoms resulting from terminal diseases. Smart technologies also give prominence to delicate communication and psychological support. Virtual care strategies, such as video calls and various smartphone applications, have proven to be secure and efficient in end-of-life and palliative care settings, showing comparable or even better results for quality of life compared to in-person care according to Dolan et al. 25 Yet, the barriers to the adoption of these tools include a lack of digital literacy, privacy concerns, and the associated costs. 26
Smart technologies in palliative care: a specific focus
A smart healthcare system connects people, resources, and healthcare-related institutions through technologies like IoT, sensors, blockchain, cloud computing, telemedicine, AI and 5G technologies, amongst others.6,8,9 It then actively manages and intelligently responds to the needs of the medical ecosystem. Typically, smart sensors, a remote server, and a network make up a smart healthcare system. 27 In addition to guaranteeing that participants receive the services they require, smart healthcare may encourage communication between all parties involved in the healthcare industry, support an equitable distribution of resources, and assist in making informed decisions. 9 Healthcare administrators are currently faced with a difficult trade-off of how to deliver individualised care to patients undergoing increasingly sophisticated treatments without sacrificing safety. 28 This is due to the growing demand for high-quality healthcare services at lower costs. 29 The main challenge arises from the deficit of automated patient monitoring technologies, which forces carers to frequently monitor vital biometric information including body temperature, blood pressure, heart rate and respiratory rate. 30
The use of smart technologies in palliative care, a profession that has historically relied on in-person treatment modalities, has been the subject of recent studies. For example, Hughes et al. 31 looked at telemedicine use in palliative care settings and found that patient satisfaction and treatment accessibility significantly improved. Their study demonstrated that higher levels of satisfaction with telemedicine can be attributed to better video accessibility and a strong internet connection. Similarly, Rejeb et al. 32 argued that the use of wearables in healthcare applications has improved patient engagement and satisfaction while streamlining doctor-patient contact. According to their findings, ongoing, real-time monitoring could improve patient comfort and lower hospital admission rates by facilitating prompt treatments and better symptom control and saving overall medical costs.
Although smart health technologies have shown great promise in enhancing patient care, 33 their application in palliative care is yet to mature. Healthcare professionals benefit from adopting and relying on smart technologies, as they lessen the need for recurring yet routine chores and enable them to make proactive decisions by using the data they acquire. 30 Relying on traditional methods has its challenges in adequately monitoring the palliative patient's everyday activities. 34 Though many studies have been done on the adoption and use of various smart technologies in palliative care, none have focused on the optimal smart technologies in enhancing palliative care. Therefore, this study focuses on conceptualising the role of various key smart technologies in palliative care and makes recommendations on the effective and efficient use of smart technologies in healthcare to enhance palliative care.
Methodology
Study design
This research employed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) protocol, which necessitates the systematic synthesis of the literature to determine, select, prioritise, analyse, and summarise relevant published findings. 35 The PRISMA flowchart is shown in Figure 1. Due to the necessity of the topic and the limited amount of evidence available, the researcher did not register the protocol for this systematic review.

PRISMA 2020 flow diagram. 38
Search strategy
A comprehensive search was conducted on 5 October 2023 on the following four databases: MEDLINE, PubMed, Scopus and CINAHL. Using the keywords and their synonyms, searches were conducted on the four databases. Medline, Scopus and CINAHL used the same search string with the Boolean connectors structured as follows: (‘Smart Technologies’ OR ‘Digital Health’ OR ‘Health Technology’ OR ‘Mobile Health’ OR ‘mHealth’ OR ‘Telemedicine’ OR ‘Telehealth’ OR ‘Wearable Technology’) AND (‘Palliative Care’ OR ‘End-of-Life Care’ OR ‘Hospice Care’ OR ‘Supportive Care’). For PubMed, a unique search was conducted, with the keywords and Boolean connectors structured as follows: (‘Smart Technologies’ OR ‘Telemedicine’ [MeSH] OR ‘Mobile Applications’ [MeSH] OR ‘Wearable Electronic Devices’ [MeSH] OR ‘Telehealth’ [MeSH] OR ‘mHealth’) AND (‘Palliative Care’ [MeSH] OR ‘Hospice Care’ [MeSH] OR ‘Terminal Care’ [MeSH] OR ‘Supportive Care’). The search returned 12,350 documents, comprising journal articles and conference proceeding articles.
Inclusion and exclusion criteria
The research incorporated the PICOS (Population, Intervention, Comparator, Outcomes, and Study Design) framework in smart technologies to improve palliative care in a virtual setting. The PICOS protocol helps to formulate precise and achievable research questions for systemic reviews.36,37 The PICOS protocol was summarised as follows:
Population (P): The focus is on patients who are undergoing palliative care, specifically those with chronic illnesses such as dementia, heart disease, or cancer.
Intervention (I): The use of smart technologies such as wearables, mobile applications, and telemedicine. These technologies have the potential to augment support for patients and caregivers, facilitate communication, and manage symptoms in the context of palliative care.
Comparator (C): Focuses on conventional palliative care delivery methods like in-person visits and telephone-based support.
Outcomes (O): Palliative care outcomes include patient satisfaction, management of symptoms, and quality of life. Excluded are outcomes unrelated to palliative care.
Study design (S): The review includes qualitative, observational, and randomised controlled trials on smart technologies in palliative care. Exclusions apply to non-peer-reviewed studies, editorials, non-systematic reviews, and unpublished studies.
The systematic review included studies that met the specified criteria below.
Time frame: The review includes studies published in the last five years to ensure relevance in the evolving field of healthcare technology.
Language: Only studies published in English are considered to manage language constraints.
Type of paper: The focus is on research published in peer-reviewed journals and conference proceedings. Commentary pieces, book chapters, editorials, and grey literature are excluded.
Publication status: The review only considers studies in their final published form. Unpublished manuscripts, abstracts, and preliminary findings are excluded.
Research area focus: The review exclusively focuses on studies that apply smart technologies in palliative care. Studies not directly addressing this nexus are excluded.
Keywords: Research must include ‘smart technologies’, ‘healthcare’, and ‘palliative care’ as keywords. Studies relevant to these themes separately but not within the context of palliative care are excluded.
The inclusion and exclusion criteria (incorporating PICOS) are summarised in Table 1.
Inclusion and exclusion criteria.

Data extraction and synthesis
To ensure that all relevant information was gathered and to streamline the data-collecting process, an Excel data extraction form was designed. The two authors (K.M. and B.M.N.) independently screened the full texts of the articles to eliminate irrelevant articles based on the inclusion-exclusion criteria. Discrepancies between the researchers were resolved by a discussion between the authors.
Quality assessment of studies
The Newcastle-Ottawa Scale (NOS) was used to assess the quality of observational studies. The NOS offers a comprehensive framework for evaluating three crucial domains: selection, comparability, and outcome. Firstly, in the domain of selection, studies are evaluated based on the representativeness of the exposed cohort, the selection of non-exposed cohorts, and the identification of the intervention. It also ensures that the outcomes of interest were not preexisting at the start of the study. Secondly, in the comparability domain, studies are evaluated based on their ability to control for important variables, like disease stage, patient demographics, and socio-economic status. This ensures a fair comparison between groups using smart technologies and those receiving traditional care. Lastly, the NOS assesses outcome measurement methods, follow-up period adequacy, and follow-up completeness. The NOS helps evaluate methodological quality and ensures reliable evidence. This assessment reduces bias and enhances validity in the field of palliative care.
Results
Of the 1358 articles identified from the various database searches, 647 were removed as duplicates before screening and 461 based on publication type. From the remaining 250 articles, 155 were excluded based on abstracts and 95 articles were screened based on abstracts. With 22 articles excluded based on abstracts, 76 articles were assessed for eligibility based on full text. Of these, 57 articles were excluded as not meeting the criteria, and eventually, 19 articles were included in the systematic review. This is summarised in Figure 1.
The final screening is important because it dictates which article will be analysed in the systematic review. A total of 57 articles were excluded for the following reasons:
Reviews and editorial articles—Although the researchers explicitly indicated that journal articles and conference proceedings were the key document sources considered for this review, it was noted that some other review articles and editorials were part of the final documents for full review. As such, these were screened and excluded from analysis in the final review. A total of 9 articles were excluded based on this screening criterion. Emphasis on the COVID-19 pandemic—Articles that placed more emphasis on the COVID-19 pandemic were excluded in the final review. In this review, the focus was on articles that explore smart technologies that have been implemented and evaluated over an extended period, ensuring that the findings are based on established methodologies. In contrast, COVID-19 called for immediate adjustments in enhancing lives. A total of 31 articles were excluded based on this screening criterion. Theoretical studies—The study mainly focused on articles that were either qualitative, quantitative, or mixed research in using smart technologies for palliative care. In other words, the research was supposed to be practical or empirical. Studies that focused on theoretical suggestions or reviews (in any form) for technologies used in palliative care were not considered. A total of 17 articles were excluded based on this screening criterion.
Resultantly, 19 articles were included in the systematic review. These were distributed as shown in Figure 2.
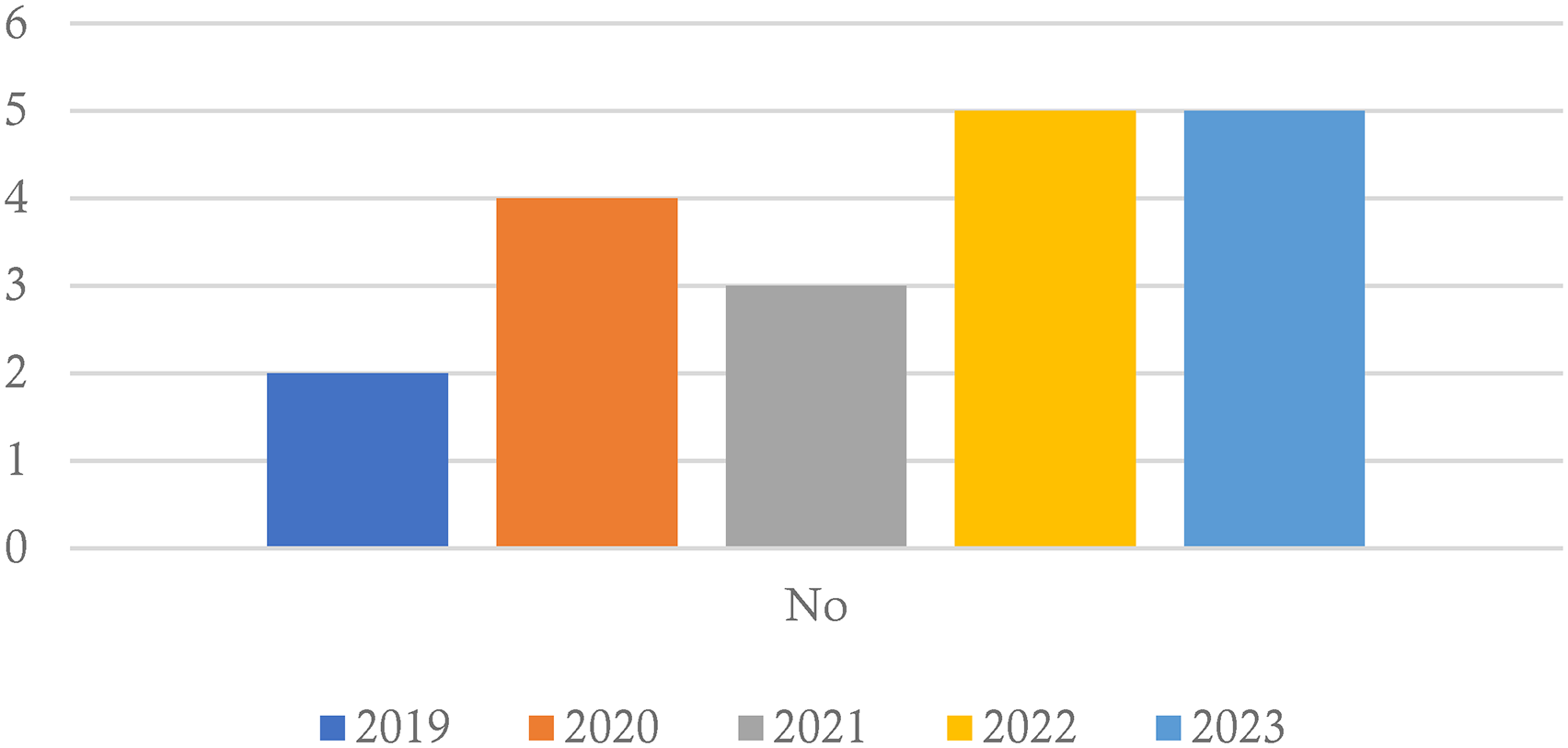
Year of publication for the articles.
Figure 2 depicts that generally, there was an increase in the number of publications focusing on the use of smart technologies in palliative care based on the screening criteria. The publications rose from two in 2009 to five in 2023. This can be attributed to various reasons including the permeative nature of smart technologies as an emerging trend spanning many domains including healthcare, or a general awareness of the potential of smart technologies within palliative care scenarios. The USA leads in smart technology research in palliative care from 2019 to 2023, showcasing its pivotal role. Australia's active participation in 2021 and 2022 signals growing influence. Uganda, Nigeria, and Zimbabwe's joint efforts in 2021 and 2023 reflect emerging expertise in palliative care technology in Africa. Switzerland, Ireland, Taiwan, Germany, Spain, the Netherlands, and China's involvement indicates a diversification in research contributions. This diversity is crucial for global progress in palliative care technologies. Overall, global interest in smart technologies for palliative care is on the rise.
Table 2 summarises the 19 articles based on the author's name(s), the aim or objective of the research, the condition or illness within the study, the country where research was conducted, the research design, the smart technology used in the study, summary of findings and the limitations or recommendations of the study.
Characteristics of the included articles.

Based on the 19 articles analysed in Table 2, several findings can be articulated. According to Guo et al., 39 telemedicine is preferred for palliative care at home in China, reducing strain on nurses and expanding access to care. This was also echoed by Katz, 52 who posited that smart technologies greatly improved the quality of life for patients with Parkinson's disease within the U.S. In addition, smart technologies proved to have saved time for cancer patients, enhancing patient-physician interaction. 55 Smart technologies like the use of telemedicine were found to be very effective for end-of-life care in lung cancer patients, according to Chua et al. 56 The consensus emerging is that smart technologies enhance patient care. 40 However, most of these findings were from a developed countries perspective.
Discussion
Benefits of smart technologies in palliative care
Smart technologies improve care continuity, reduce errors, and improve palliative care team effectiveness, enabling remote monitoring of patients with serious illnesses.42,43,49 This is in line with 57 research that underscores the potential benefits of smart healthcare technologies in cancer treatment, encompassing patient instruction, symptom monitoring, and emotional assistance. This also applies to the use of mobile health technologies, which were found to empower patients and reduce costs in palliative cancer care, 44 which was also echoed by Kamran and Dal Cin 53 as they opined that mobile apps foster effective communication in palliative care. The use of advanced technologies in palliative care has led to comparable costs with traditional face-to-face services, while also enhancing efficiency by enabling palliative care to reach a larger number of patients and improving staff job satisfaction.48,50
The application of smart technologies can also enhance access to healthcare services, regardless of geographical location, particularly when in-person interactions are not practical or financially viable. 49 This concurs with a study by Nguyen, 58 who noted that these technologies have demonstrated utility and user-friendliness among healthcare professionals and managers, especially in facilitating remote communication and data exchange. Implementing smart technologies, such as videoconferencing, for clinical consultations provides an appropriate and suitable model of care, especially when patients and caregivers actively participate in the decision-making process. In a study by Karera et al., 44 patients voiced their contentment with the use of mobile devices in consulting healthcare professionals. They argued that it lessens the workload of having to do various pre-processes compelled during physical checking. In the same study, patients also indicated their preference for consulting online as it empowers them to express themselves comprehensively since the platform empowers them with a sense of comfort. Studies59,60 concurs that smart technologies can also enable patients, enabling them to convey their requirements more fully.
Smart technologies used
While many smart technologies were adopted and used within the inclusion articles, there are multiple instances where the actual technology adopted was not explicitly mentioned. Rather, they were just mentioned as telemedicine or telehealth interventions. In the context of this study, these are described as general telemedicine services, as revealed in Table 2. They include studies31,39,52 for general palliative care at home. Similarly, other technologies were described as digital technologies in palliative care. A study 42 adopted digital technologies in healthcare delivery. This is also similar to Nkhoma et al. 49 who adopted digital technologies in healthcare delivery.
Mobile technologies and mobile applications were also used for palliative care. These contributed to a higher percentage of the studies analysed and were adopted by Burner-Fritsch et al. 41 as part of the electronic patient-reported outcome measure (ePROM); 40 for the electronic health application; 53 for the mobile application; 44 for mobile technologies in healthcare; 42 for an intelligent remote patient monitoring system with mobile accessibility and 51 for mobile technologies.
The use of mobile technologies can be extended to traditional audio and video calls. The use of virtual reality and 360° video conferencing to improve the mental health and well-being of elderly patients in palliative care in Ireland; 46 telephone and videoconferences; 50 web-based videoconferences; 55 and video conferencing 56 are all various mobile technologies that were analysed in palliative care administration to enhance healthcare. Within the scope of the included studies, wearables were minimally adopted. They were used to predict end-of-life admissions in palliative care for cancer patients in Taiwan. 45 This represents a new dimension in palliative care administration. Overall, when adopted properly, the use of smart technologies in palliative care improves efficiency and staff satisfaction. 50
Challenges of smart technologies adoption in palliative care
While the use of electronic health systems is advocated for, it is difficult when dealing with palliative care scenarios particularly for patients with declining health. 41 Similarly, Hughes et al. 31 posited that although technologies like telemedicine increase access to palliative care, there is a need to address the digital divide, especially in developing countries. In this context, the digital divide refers to the technological gaps that exist between developed and developing countries in terms of infrastructure, digital literacy, and resources for palliative care. The cost of mobile phones continues to be a significant barrier, preventing individuals from lower socioeconomic backgrounds and with lower levels of education from accessing and using mobile technologies.44,48,49 Gallegos-rejas et al. 61 concurs with the review finding that the digital divide in palliative care, especially in developing countries, poses a significant obstacle to equitable access to telehealth and mobile health services. Furthermore, Rasekaba et al. 62 concurred that this gap is further exacerbated by low digital and health literacy rates among older adults in rural areas.
The use of smart technologies, according to Chua et al. 56 and Dickman Portz et al., 51 also presents a challenge in how healthcare providers discuss sensitive subjects, such as end-of-life preferences and advanced care planning, with patients and their families through telehealth. Delivering such sensitive news, including scans, laboratory results or diagnosis via some portal is negatively perceived by both the patients and their families. 51 These types of discussions would typically necessitate in-person interaction. Regrettably, a significant proportion of individuals receiving palliative care are expected to experience confinement to their homes because of the advancement of their motor manifestations. For instance, this trend is prominently observed among patients afflicted by Parkinson's disease and its associated conditions, where reliance on a wheelchair or confinement to a bed represents a prevalent functional outcome in the later phases of these degenerative conditions affecting movement. 52 Subsequently, these individuals will necessitate comprehensive caregiving assistance.
Inquiries were made regarding the precision of data gathered from wearable technologies in palliative care environments. 45 According to Huang et al., 45 these include inaccuracies observed in patients exhibiting reduced and leisurely motions, the inefficacy of accelerometers in capturing swift movements, imprecise evaluations of step tallies, the necessity for frequent recharging and synchronisation of data, as well as occurrences of malfunction, impairment, and loss of said wearable gadgets.
Conditions or illness
Like the technologies used, many conditions or illnesses were never explicitly described by more than half of the studies. These were considered general palliative care illnesses in this study. Studies31,39,41,50 focused on general palliative care at home;42,43 focused on digital tech for general palliative care continuity for the elderly; 46 used VR for mental health in elderly palliative care and51,53 focused on mobile apps for general palliative care. These could represent anything that falls within the scope of palliative care conditions or illnesses.
Cancer proved to be a condition or illness that calls for continuous attention, as a palliative condition. Various forms of cancer were noted in this study. 44 focused on advanced palliative cancer care; 45 focused on the use of wearables for breast cancer patients; 40 developed an electronic-health app for multiple myeloma (white blood cell cancer) patients; 49 focused on breast cancer administration; 55 focused on cancer palliative care and 56 focused on advanced lung cancer. Additionally, 52 Katz also focused on palliative care for Parkinson's disease and related disorders.
The role of the caregiver in palliative care
Smart technology solutions within palliative care must include support for caregivers and their family members as they directly interact with the patients.49,51 The adoption of smart technologies and digital technologies such as video consultation allows for the communication of caregivers with multiple patients simultaneously as well as health professionals, thereby enhancing the effectiveness of their influence.44,50 The role of caregivers in palliative care is further supported in another study where an electronic health application was designed to deliver alerts, messages, care plans and other useful information to the caregivers. 40 Furthermore, patients who are unable to complete the Palliative Care Outcome Scale (POS) are represented by caregivers. 48 In a different study, patients’ caregivers served as their primary information source and source of well-being. 63 This is consistent with another study that shows caregivers have an active involvement in the progression of the disease where new care goals must be discussed and agreed upon by caregivers. 51
Theoretical implications and contributions
The results indicate that incorporating smart technologies into palliative care can profoundly transform traditional healthcare approaches. The role of technology in enhancing the interaction between patients and physicians, improving care efficiency, and predicting health outcomes for comprehending the delivery of palliative care. This suggests a move towards more patient-centred, data-driven, and accessible care models. Furthermore, this review adds to the expanding literature on smart technologies in palliative care by offering a comprehensive synthesis of their role and impact. It enhances current knowledge by emphasising the diverse uses of these technologies, ranging from telemedicine to wearable devices, to virtual reality and mobile technologies, and how they are specifically beneficial in different palliative situations, like cancer care and many other palliative care scenarios. The review also emphasises the evolving nature of palliative care, incorporating technology to improve patient outcomes.
Practical implications
The study emphasises the potential of smart technologies to help healthcare systems and enhance patient experiences. For healthcare professionals and policymakers, these insights can serve as a guide for implementing technology-enhanced strategies in palliative care. More importantly, the insight from the findings underscores the significance of training, security, and privacy considerations in this process. However, more research is needed in developing nations. The articles in this review mostly emanated from developed nations. More insights from a developing nation's perspective are needed, as the health response might be different.
Limitations of the study
The review recognises certain limitations.
The variability of smart technologies used in palliative care and the diversity of conditions being studied make it difficult to draw general conclusions about their effectiveness. Many studies lack long-term data on the benefits and potential risks of technology interventions. The scalability and integration challenges of smart technologies in different healthcare settings were not fully explored, hindering their adoption and effectiveness in palliative care. There is a lack of detailed exploration into ethical concerns regarding privacy risks associated with smart technologies in palliative care contexts, emphasising the need for comprehensive ethical analysis and privacy protection measures in future studies. Smart technologies and digital interventions adopted in palliative care have not been explicitly mentioned by the reviewed studies. Thus, the technologies used were analysed using the general terms provided. An explicit mention of these tools could have provided a deeper understanding of the opportunities and challenges they present in palliative care. This review included papers published from 2018 to October 2023 from four selected databases. There is a possibility that there are more recent studies that were not included that were published after this search. These articles could have provided a deeper insight into smart technologies for palliative care. This research only analysed papers written in the English language. This poses language bias and a risk that more substantive papers might have been written in other languages.
Future perspectives and research agenda
The focus of future research should be on:
Enhancing training and addressing technical challenges Prioritising data security, privacy, and ethical considerations Bridging the digital divide User-centric design and engagement Continual assessment and system integration Need for a framework for smart technology adoption
Developing comprehensive training programs is crucial in the palliative care ecosystem to address technical challenges and improve training. This includes providing training for nurses, clinical professionals, healthcare personnel, family caregivers, and patients.39,43 These are the critical stakeholders in the palliative care ecosystem. The proficiency and confidence of these stakeholders in utilising smart technologies are essential for their effectiveness in palliative care. Limited exposure to electronic patient-reported outcome measures (ePROMs) among healthcare professionals needs to be addressed.
41
Additionally, patient training in telemedicine and expanding telehealth services while providing training can contribute to a more holistic approach toward education and skill enhancement in smart palliative care technologies.52,55
Given the prevalence of data breaches, safeguarding patient information in digital palliative care settings is of utmost importance. Research emphasises the necessity for robust protocols to guarantee data precision, protection, and smooth integration with current healthcare systems.
42
Studies44,49 underscore the importance of enhancing training programs to encompass patient privacy and data confidentiality. Therefore, there is a need to broaden the use of smart technologies in end-of-life care beyond the current functions. Delving into emerging technologies such as blockchain for secure management of patient information can greatly enhance security and privacy concerns in palliative care. It is imperative to note that these privacy and security measures need to be contextualised as a one-size-fits-all mechanism cannot be used. Security and privacy policies, data protection regulations and ethical concerns may differ from one country to another.
64
The digital gap, which was previously described as the technological gaps between developed and developing nations in terms of infrastructure, digital literacy and resources, is especially evident in developing countries, presenting a major obstacle to fair access to smart palliative care technologies. Hughes et al.
31
propose efforts to reduce this gap, guaranteeing that telehealth services reach disadvantaged and underprivileged communities. Addressing access barriers due to socioeconomic factors and digital literacy is crucial for ensuring equitable access to technology-driven palliative care solutions. This entails improving internet connectivity, increasing the affordability of technology, and offering digital education to ensure that all patients and caregivers can take advantage of the progress in palliative care. Some recommendations to the Ministry of Health to bridge the digital divide include: improving infrastructure by investing in and expanding telecommunications, especially in rural areas, to ensure widespread high-speed internet access; working with service providers to lower internet and device costs, making technology more affordable for all; launch digital literacy programs to enable more effective internet use; encourage public-private partnerships to develop digital infrastructure and implement regulatory measures to foster competition among service providers and improve services at lower prices.
To improve user engagement and satisfaction, Kupczik et al.
46
propose creating telemedicine apps with simple interfaces and user-friendly experiences. Dickman Portz et al.
51
also recommend exploring digital strategies to encourage user participation in mobile health technologies for palliative care. This is important as users must engage with smart technologies with ease. Kamran and Dal Cin
53
highlight the significance of design thinking and advocate for continuous enhancements in mobile apps based on feedback from users. This approach that prioritises the needs of users is essential for enhancing the usability and acceptance of smart technologies in palliative care.
The significance of ongoing evaluation and updates of telemedicine applications in the dynamic and ever-changing healthcare field is emphasised by Geerts et al.
40
Additionally, Chua et al.
56
support the incorporation of new telehealth platforms into current electronic systems for patient scheduling and billing to ensure smooth operation and minimise disruptions to existing workflows.
Development of a framework for the adoption of smart technologies in palliative care that can act as a guide to healthcare practitioners as well as policymakers into the need to adopt smart technology for palliative care.
Conclusion
The integration of smart technologies into palliative care signifies a fundamental shift towards more personalised, efficient, and accessible care models. The findings from this comprehensive review affirm the substantial impact of technologies such as telemedicine, wearable devices, and mobile applications in improving the quality of life for palliative care patients and reducing the burden on caregivers. However, to fully harness the benefits of these technologies, there is an urgent need for targeted training programs, robust privacy and security safeguards, and strategic efforts to bridge the digital divide. Additionally, the study calls for the development of a cohesive framework to guide the implementation and evaluation of these technologies within palliative care settings. Future research should focus on addressing the identified gaps and exploring the long-term implications of integrating smart technologies in palliative care, ensuring that these innovations meaningfully contribute to patient-centred care and healthcare excellence.
Footnotes
Acknowledgements
We would like to acknowledge the support from the Information Technology department in organising a writing retreat towards the completion of this systematic review article.
Contributorship
Conceptualization: K.M.; formal analysis: K.M. and B.M.N.; methodology: K.M. and B.M.N.; results: K.M. and B.M.N.; writing original draft: K.M.; writing, review and editing: K.M. and B.M.N. All authors (K.M. and B.M.N.) have read and agreed to this final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable, the institution does not require ethical approval for this type of research.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
K.M.