
Abstract
Background:
Palliative care patients desire more symptom management interventions that are complementary to their medical treatment. Within the multi-professional team, nurses could help support pain management with non-pharmacological interventions feasible for their practice and adaptable to palliative care patients’ needs.
Objectives:
The objective was to identify non-pharmacological interventions feasible in the nursing scope of practice affecting pain in palliative care patients.
Design:
A systematic review.
Data sources and methods:
A defined search strategy was used in PubMed, CINAHL, PsycINFO, and Embase. Search results were screened double-blinded. Methodological quality was double-appraised with the Joanna Briggs Institute Critical Appraisal Tools. Data were extracted from selected studies and the findings were summarized. The methodological quality, quantity of studies evaluating the same intervention, and consistency in the findings were synthesized in a best-evidence synthesis to rank evidence as strong, moderate, limited, mixed, or insufficient.
Results:
Out of 2385 articles, 22 studies highlighted non-pharmacological interventions in the nursing scope of practice. Interventions using massage therapy and virtual reality demonstrated most evidentiary support for pain management, while art therapy lacked sufficient evidence. Mindful breathing intervention showed no significant reduction in pain. Hypnosis, progressive muscle-relaxation-interactive-guided imagery, cognitive-behavioral audiotapes, wrapped warm footbath, reflexology, and music therapy exhibited promising results in pain reduction, whereas mindfulness-based stress reduction program, aromatherapy, and aroma-massage therapy did not.
Conclusion:
Despite not all studies reaching significant changes in pain scores, non-pharmacological interventions can be clinically relevant to palliative care patients. Its use should be discussed for its potential value and nurses to be trained for safe practice. Methodologically rigorous research for non-pharmacological interventions in nursing scope of practice for pain relief in palliative care patients is necessary.
Trial registration:
The protocol for this study is registered in the International Prospective Register of Systematic Review (PROSPERO registration number: CRD42020196781).
Keywords
Introduction
Palliative care aims to optimize the quality of life in patients with life-limiting illnesses. It prevents and relieves health-related suffering through early identification, correct assessment, and treatment of pain and other problems. 1 Pain is one of the most frequent and serious symptoms experienced by palliative care patients. 1 Pain management is required for patients experiencing pain suffering from incurable nonmalignant and malignant diseases. 1
The total pain concept describes pain as a multidimensional experience with interacting components in physical, psychological, social, and spiritual dimensions. 2 Therefore, management of pain requires a multi-professional approach. 2 Besides conventional pharmacological interventions, prescribed by physicians, palliative care patients desire more symptom management interventions that are complementary to their medical treatment. 3 As part of a multi-professional team, pain management plays an important role in supporting palliative care patients. Various specialized professionals, including psychologists, physiotherapists, chaplains, and social workers, offer interventions and specialized knowledge to manage pain. Nurses are also a crucial part of this team, often being the first healthcare professionals to encounter patients’ pain. 4 When interventions or techniques are general, nurses can incorporate them into their scope of practice. Therefore, by including non-pharmacological interventions (NPI) in the nursing scope of practice in patients’ pain management plans, pain management can be improved.
For this study, NPI are set within integrative nursing and are defined as complementary interventions within the nursing scope of practice. 5 NPI can be classified based on their primary therapeutic input or their working mechanisms. For this review, NPI are classified according to their working mechanisms, using four modalities: (1) mind–body interventions, (2) biologically based treatments, (3) manipulative and body-based practices, and (4) energy therapies, as this classification system has less overlap between categories and supports the clarity of this review. 6 Mind–body interventions, such as meditation, are based on the human mind and affect the human body and physical health. Biologically based treatments involve natural substances, such as herbs or essential oils. Manipulative and body-based practices, such as massage therapy, consist of therapies involving movement or manipulation of one or more parts of the patients’ body. Energy therapies, such as reiki or therapeutic touch, are defined as influencing and applying energy fields to the body. 7
NPI could be beneficial for reducing pain through the stimulation of endorphin release enhancing natural pain killer cells, relaxation, and distraction by refocusing pain perception and relieving tension in the body. 3 Thereby, it can add value to a pain management plan by providing extra relief measures as well as reducing the doses of medication and potential side effects. Importantly, NPI can be adapted according to palliative patients’ needs, for example, gentler techniques or other types of interventions because being touched is too painful or uncomfortable. 8 Additionally, NPI could benefit patients’ ability to proactively participate in their pain management plan. 9 If appropriate, fitting the values, wishes, and needs of patients and their carers, patients could learn to apply some of the interventions themselves or by their informal caregiver without the interference of a nurse, having an immediate influence on pain and supporting autonomy. When training or getting instructions on interventions is considered to be an additional burden by patients or caregivers, support from nurses stays best suited.
There have been quite some efforts in research on complementary and integrative medicine across different fields and regarding symptom burden. Complementary therapies such as acupressure, acupuncture, aromatherapy massage, breathing, hypnotherapy, massage, meditation, music therapy, reflexology, herbal supplements, support groups, healing touch, and reiki are associated with a reduction in symptom burden of palliative care patients.10,11 However, these complementary therapies are often administered or taught by a trained practitioner or expert, for example, acupuncture, or use of herbal supplement which entails specialized knowledge and training. The nursing scope of practice cannot accommodate these interventions. However, since nurses play a vital role in pain management and are part of a multi-professional team, integrating NPI into nursing practice can help support palliative care patients who are experiencing pain.
There is a lack of knowledge regarding NPI being feasible for nursing staff in care settings for pain relief in adult patients receiving palliative care. This systematic review aimed to identify NPI feasible in the nursing scope of practice affecting pain in palliative care patients and to give nurses evidence-based interventions to support palliative care patients experiencing pain effectively.
Methods
Protocol and registration
This systematic review was conducted according to the Cochrane Handbook for Systematic Reviews of interventions and was written from 27 July 2020 until 28 August 2022. Results were described using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 12 The completed PRISMA checklist is available in the Supplemental Material. This review is registered in the International Prospective Register of Systematic Review (PROSPERO registration number: CRD42020196781). 13
Literature search
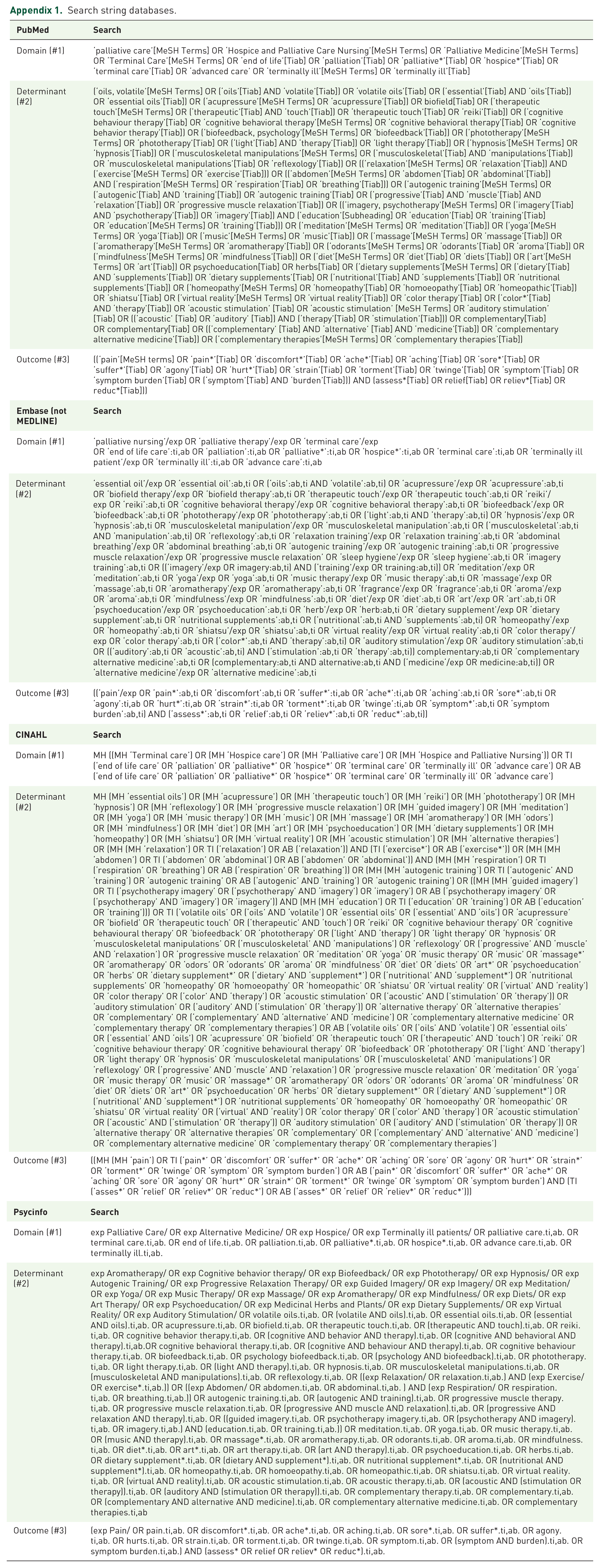
A literature search was conducted in electronic databases: MEDLINE through PubMed, CINAHL, PsycINFO, and Embase for studies assessing the efficacy of NPI in the nursing scope of practice for pain relief in palliative care patients. The final search was conducted on 15 July 2022. Specific terms were used according to the preferred terminology defined for each database. Medical subject heading terms, headings, thesaurus terms, and Emtree terms were used. Searches were based on the domain, determinant, and outcome (DDO) framework. The search terms were grouped per database according to the DDO framework and linked with Boolean operators into one search phrase. The defined search strategy was used for MEDLINE and was adapted to the other databases (see Appendix 1). From the eligible studies, reference lists were checked for other studies.
Eligibility criteria
Studies were eligible for inclusion when they involved adult patients (⩾18 years) with advanced and incurable diseases who received palliative care in a hospital, in outpatient care, or were admitted to a palliative ward/hospice. Eligible NPI were interventions that: (a) fit within the nursing scope of practice (e.g. music therapy with guitar is excluded whereas headphones are included), (b) can require instruction or training to secure safe practice of the interventions, and (c) is not restricted to in- or outpatient facilities (e.g. biofeedback with the use of sonogram is excluded). All types of quantitative effect studies and articles written in English or Dutch were eligible for inclusion. Studies stating a diagnosis of dementia or mild cognitive impairment were excluded to ensure reliability on pain scores. Case studies and qualitative design studies were excluded to be able to summarize NPI affecting pain scores. If interventions require specialized knowledge or techniques, the studies are excluded because they do not fit within the nursing scope of practice.
Study selection
Results were screened double-blinded by two reviewers (SvV and EdG) on title and abstract using the online program Rayyan. 14 Differences in selection were discussed between reviewers, and a consensus was achieved for all selected studies.
Data extraction and study quality
Data extraction was conducted by one reviewer and recorded in a data-extraction table with items for (a) general characteristics of the study compromising author, year of publication, country, study design, sample, measuring scale used, data collection interval(s), and statistical analysis; (b) characteristics of the NPI used and the professional performing the intervention during study; and (c) results on pain scores.
The methodological quality in the included studies was assessed independently by two reviewers (SvV and HD) using the Critical Appraisal Tools from the Joanna Briggs Institute. 15 They were employed to determine whether a criterium was met, whether it was unclear if it was met, or if that criterion was not applicable. 15 One point was awarded for each criterion that was met. The number of points was summed and compared to the maximum points possible. If an item was not applicable, the maximum number of points was reduced by one item. The checklists for randomized controlled trials (RCTs) and quasi-experimental studies were used in accordance with the study designs. Differences in the appraisal were discussed with a third reviewer (EdG), and consensus was achieved between all reviewers concerning the methodological quality of all studies.
Best-evidence synthesis
A best-evidence synthesis approach was used to synthesize the data to allow reviewers to compare the outcomes of studies, taking into account the heterogeneity in the included studies in terms of interventions and outcome measures. 16 The best-evidence synthesis considers the methodological quality, quantity of studies evaluating the same intervention, and consistency in their findings to rank evidence as strong, moderate, limited, mixed, or insufficient. 16 The methodological quality of the studies was placed into three quality categories: high (⩾85%), medium (50–85%), or low (⩽50%). 17 A strong level of evidence indicated a recommendation for practice while moderate, limited, and mixed evidence indicated considerations for practice. The best-evidence synthesis described by Kennedy et al. 17 was adapted by the authors to determine and establish cutoff values and propose recommendations for daily practice for this systematic review. 17 The best-evidence synthesis is summarized in Table 1.


Results
Study selection
In total, 2385 studies were identified through database searching. Duplicates (n = 246) were removed, and the first selection based on title and abstract resulted in 87 articles. Of these, 65 were excluded because (a) the intervention was not in the nursing scope of practice (n = 27), (b) the sample did not include palliative patients or patients with advanced illnesses without curative options (n = 17), (c) wrong outcome (n = 7), (d) full-text was unavailable even after contacting the first author (n = 3), (e) wrong publication type or a congress abstract (n = 6), and (f) wrong study design (n = 5). Of the eligible studies, reference lists were checked resulting in the addition of one study to this systematic review for a total of 22 studies. A flow chart of the study selection procedure is presented in Figure 1.

PRISMA 2020 flow diagram of selected studies.
Data extraction and study quality
The included studies consisted of 12 quasi-experimental and 10 RCT’s involving a total of 1463 patients (ranging from 14 to 380 patients). Patient settings were inpatient (n = 15) and outpatient facilities (n = 7). Pain was measured on the one-item pain scales of numerical rating scale (NRS) (n = 13) and visual analog scale (VAS) (n = 8), and one study used a combination of the VAS and NRS. All studies were published between 2000 and 2021. Cancer was the primary diagnosis of patients in all but one of the studies, and four studies also included a non-cancer diagnosis. Results of the NPI in the nursing scope of practice found in this review are divided and described into the four modalities. 8 Eight different interventions were ascertained on mind–body interventions, one for biologically based treatments and three for manipulative and body-based practices. No studies were found that could be ascertained into the modality of energy therapies. The NPI studied were massage (n = 6),18–23 mindful breathing (n = 3),24–26 art therapy (n = 2),27,28 aromatherapy massage (n = 1), 29 aromatherapy (n = 1), 30 progressive muscle-relaxation and interactive guide imagery (PMR-IGI) (n = 1), 31 mindfulness-based stress reduction (MBSR) program (n = 1), 32 cognitive-behavioral audiotapes (n = 1), 33 hypnosis (n = 1), 34 wrapped warm footbath (n = 1), 35 reflexology (n = 1), 36 virtual reality (VR) (n = 2),37,38 and music therapy (n = 1). 39 An overview of the characteristics of the included studies is presented in Table 2.
Study characteristics and data-extraction table.

BPI, Brief Pain Inventory; MBSR, Mindfulness-Based Stress Reduction; MPAC, Memorial Pain Assessment Card; NRS, numerical rating scale; PID, pain intensity difference; PMR-IGI, progressive muscle-relaxation and interactive guide imagery; PPI, present pain intensity; VAS, visual analog scale; VR, virtual reality; ESAS-r, Edmonton System Assessment System-revised; IQR, Interquartile range.
The methodological quality was assessed for the individual studies. Of the RCTs, one study was rated as having high methodological quality, 18 eight with medium quality,24–26,29,31,33,35–36 and one with low quality. 19 The low and medium-quality studies lacked consistent documentation on randomization, concealment of treatment groups, similar groups at baseline and analyzed in randomized groups, and blinding processes. Of the quasi-experimental design, three studies were rated as high methodological quality,32,34,37 seven of medium quality,20–22,27,30,38,39 and two as low quality.23,28 The high-quality studies generally scored well on describing a control group, given similar treatment, and participants in any comparison being equal. Low-quality studies lacked these descriptions and did not measure multiple pre-intervention measurements when there were multiple post-intervention measurements. The quality assessment per item and an overall methodological quality appraisal are listed in Table 3.
Critical appraisal . 15

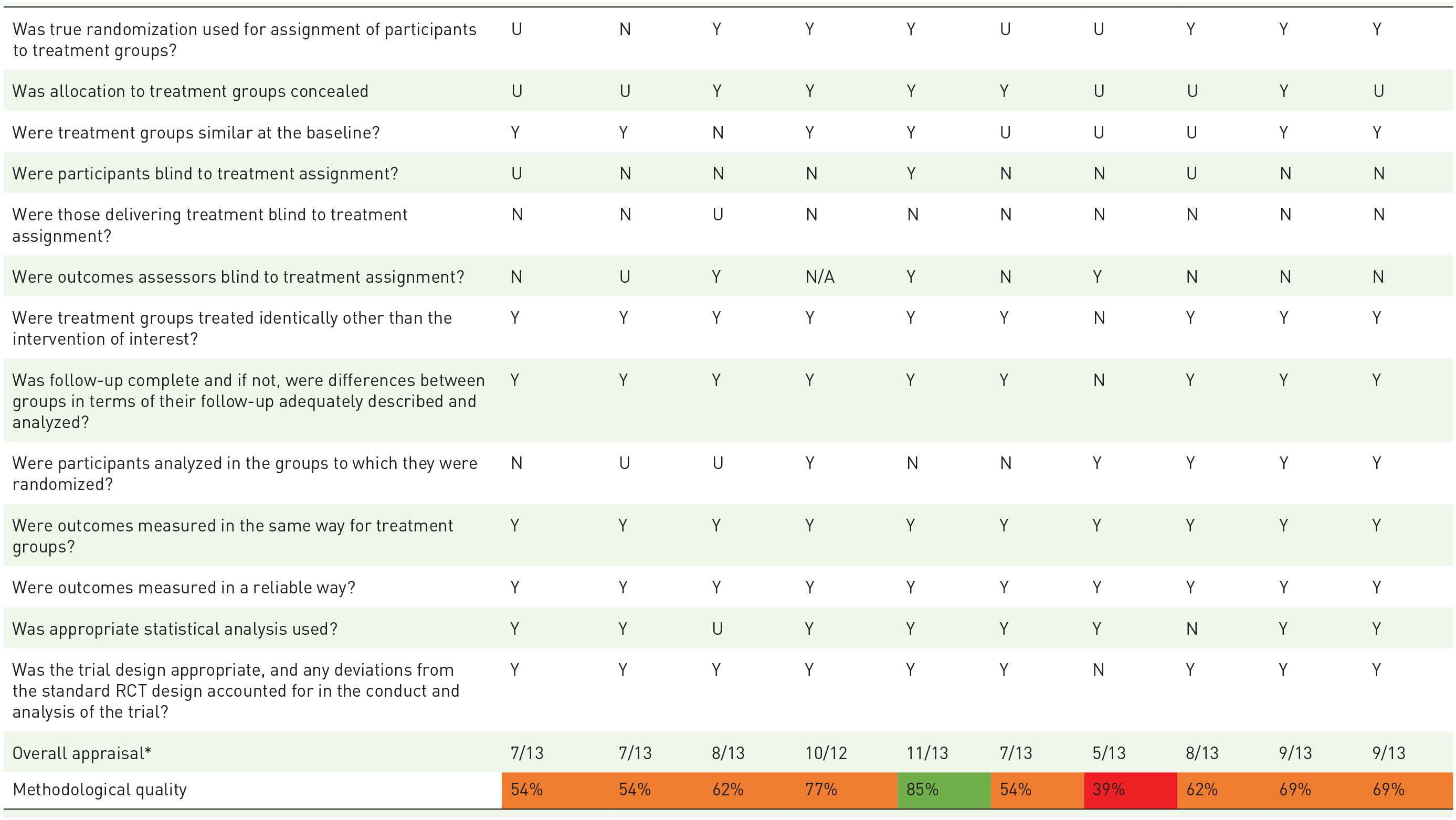
The number of points were summed and compared to the maximum points possible. If an item was not applicable, the maximum number of points was reduced by one item.
Green = high methodological quality, orange = medium and red = low.
N, no; N/A, not applicable; RCT, randomized controlled trial; U, unclear; Y, yes.


The number of points were summed and compared to the maximum points possible. If an item was not applicable, the maximum number of points was reduced by one item.
Green = high methodological quality, orange = medium and red = low
N, no; N/A, not applicable; U, unclear; Y, yes.
Mind–body interventions
Within the modality mind–body interventions, eight different interventions were found.
Mindful breathing
Two studies reported a 20-min mindful breathing intervention, and one study described a 5-min mindful breathing intervention, guided breathing exercises were provided in all of them.24–26 A single session of 20 min of mindful breathing did not significantly reduce pain (−0.5 points; p = 0.468), and the control group consisting of 20 min of conversation also did not reach statistical significance (+1.0; p = 0.152). Compared with the control group, the latter intervention was not significantly reducing pain (p = 0.149). 26 Another 20-min mindful breathing intervention was compared to an active control group consisting of supportive listening. A within-group analysis showed a statistically significant pain score reduction at all intervals compared to baseline (−1.35–(−2.25), p = 0.0–0.1) in the intervention group but not in the control group. The between-group comparison showed no statistically significant improvements in pain scores at all intervals up to 20 min (p = 0.22–0.81). 25 The 5-min mindful breathing intervention showed no statistically significant reduction in pain scores in comparison to active control (5 min of normal listening) within and between groups (p > 0.05). 24
Art therapy
Two studies outlined art therapy interventions.27,28 The art therapy session in which patients chose techniques of painting, drawing, photography, modeling, and sculpturing improved pain from a median of 2.0 to a median of 1.3 (p < 0.001). 27 A 60-min daily or alternate-day art therapy session with techniques of drawing, painting, making a collage, and modeling showed significant pain score reduction after one, three, and five therapy sessions (T1 = −0.3, T3 = −0.59, T5 = −0.6; p < 0.005). 28
Progressive muscle-relaxation and interactive guided imagery
The PMR-IGI intervention consisted of 4-min prolonged deep breathing guided with a chosen script (IGI) and relaxation of the main muscle groups (PMR). The study described that the within-group pain intensity difference (PID) was significant in the intervention group (PMR-IGI) as well as in the control group (usual care). The mean PID between the PMR-IGI and control group was 1.28 (95% CI: 0.30, 2.26). Based on the average value, a greater effect was found in the intervention group (PID = 1.83, p < 0.0001) in comparison with usual care (PID = 0.55, p < 0.0001). 31
MBSR program
The MBSR program consisted of: a body scan that concentrated and gave attention to the body from head to toe to observe and experience the sensations felt in each area of the body, sitting meditation, some group discussions in which patients had time to share experiences, and mindfulness in communication and everyday life. The intervention was once a week for 8 weeks with a duration of 2 h and also daily home practice with 54 min of mindfulness practices from compact discs. This study reported the effect of improving average pain (−0.33 points) compared to the control group (+1.33). A change in scores was not statistically significant between groups (p = 0.080). 32
Cognitive-behavioral audiotapes
The cognitive-behavioral audiotapes intervention used 20-min audiotapes including: (a) positive mood statements and positive imagery suggestions; (b) standard progressive muscle-relaxation instructions; and (c) topics on history, foreign language, geography, or vocabulary. This study showed patients in the relaxation-tape group (−0.9, 95% CI: 0.16, 1.65; p = 0.023) and distraction-tape group (−1.16, 95% CI: 0.47, 1.85; p = 0.004) reported significantly reduced pain intensity immediately after listening to the tapes. No significant differences in pain intensity were found at the 2-week follow-up. 33 Pairwise comparisons at each time point indicated no significant differences between the groups.
Hypnosis
The hypnosis intervention used the following techniques: the exercise ‘warm hands’, transferred symptoms techniques, positive visualization technique, desensitization of pain technique, self-hypnosis technique, and self-hypnosis on compact disc method. It showed a statistically significant decrease in perceived pain in the hypnosis group after 1- and 2-year follow-up compared to the control group (95% CI: −23.1, −9.3). The pain scores on a 100-point scale decreased from 81.0 baseline to 45.9 after 1-year follow-up, to 38.9 after 2-year follow-up (p = 0.0001). The scores in the control group were 78.5, 62.1, and 57.1, respectively. The hypnosis therapy was associated with a decreased risk of 66% of needing to increase opioids treatment for pain control (p = 0.03). 34
Virtual reality
Two studies described a VR intervention.37,38 The VR intervention with Google Earth software in which patients could ‘travel’ to a familiar or desired place reported significantly improved observed pain (2.35 ± 2.25 to 1.15 ± 2.03, p = 0.005), with 30% of patients reporting moderate to severe pain before VR travel and 15% after VR travel. 37 Specifically, pain significantly improved for those who ‘traveled’ to memorable places (p = 0.018). For the patients who virtually went to places they desired to visit but never had, pain scores did not statistically differ (p = 0.317). 37 A VR intervention with noninteractive and/or interactive contents significantly improved pain (1.06 ± 0.25 to T1: 0.66 ± 0.1, p ⩽ 0.01). There was no minimum or maximum on usage time nor on the number of sessions. 38
Music therapy
One music intervention consisting of 20 min of listening to music administered by headphones with instrumental Indian music showed a statistically significant reduction in pain scores in the music group (−1.43 ± 0.78, p = 0.003). The control group that was kept occupied with 20 min of talking to them showed no statistically significant results in pain scores (p = 0.356). Compared with the control group, the music group significantly reduced posttreatment pain scores (−1.71 ± 0.71, p = 0.034). 39
Biologically based treatments
There was one intervention found within the modality biologically based treatments.
Aromatherapy
The aromatherapy intervention consisting of 60 min of humidified inhalation of 3% essential lavender oil did not reach a significant statistical reduction in pain scores after both the lavender treatment (−0.34 points, 0–10 scale) and the humified water (active control group) (−0.43 points) compared with the control group (no intervention) (+0.32 points). 30
Manipulative and body-based practices
Three different interventions were found within the modality manipulative and body-based practices.
Massage
Seven studies investigated massage interventions. The massage techniques that were primarily used included effleurage (smooth and sliding strokes), petrissage (squeezing, rolling, and kneading the muscles), and trigger point release (concentrated finger pressure). Multiple sessions were conducted in three studies,18–20 whereas there was only one massage session for the remainder. The duration of a massage session fluctuated between 15 and 45 min per session across the studies.
A 20- to 30-min massage intervention consisting of smooth and sliding strokes (effleurage) with some pressure on trigger points reported significantly decreased pain intensity by 1.65 ± 2.14 (0–10 scale, p < 0.001). 21 A massage group was compared with an active control group (simple touch). It consisted of six sessions of a 30-min massage consisting of light effleurage, squeezing, rolling, and kneading of the muscles (petrissage), and trigger point release. In both groups pain scores immediately improved with the massage group with −1.87 points (0–10 scale, 95% CI: −2.07, −1.67) and the control group with −0.97 points (95% CI: −1.18, −0.76). The mean difference between study arms (−0.9, 95% CI: −1.19, −0.61; p < 0.001) showed massage as the better intervention for improving pain intensity, and there were no between-group differences over time in pain or analgesic medication use. 18 One full-body massage intervention of 45 min showed immediate, short-term, intermediate, and long-term effects (p = 0.000) on pain intensity. The most significant impact occurred 15 (p < 0.002) or 20 min (p < 0.000) after the intervention. 22 Another massage intervention consisted of a 30- to 45-min full-body massage twice weekly for 2 weeks. The massage therapy intervention was compared with a control group receiving usual care. Pain intensity significantly reduced immediately after the massages. Compared at baseline, the massage group reported higher pain intensity (0–10 scale, 2.4 ± 2.8) than the control group (1.6 ± 2.1). On average, pain decreased by 42% for the intervention group compared to 25% for the control group (p > 0.05). Massage therapy significantly reduced pain intensity immediately after the first and third massages but did not reach statistical significance after the fourth massage (p < 0.09). 19 Tactile massage intervention which consisted of a soft and superficial form of massage with slow strokes, light pressure, and circling movement on the feet, hands, and/or back for 15 to 45 min reported pain improvement by 1.7 points (SD 1.6). Additionally, the rescue doses for pain were reduced from 1.6 to 0.84 doses/patient (p = 0.0005) compared with the same patients as controls (p = 0.20). 23 One study reported on massage therapy sessions lasting for 20–45 min and applied up to three sessions every 1–2 weeks. It showed a median change of pain intensity scores of 0 (−6.0, 7.0), indicating no significant temporal change in pain (p = 0.378). 20 The aromatherapy back massage intervention that lasted for 30 min using lavender essential oil and sweet almond oil showed statistically significant pain score reduction in the aromatherapy massage group (−1.15, p = 0.01) and in the aromatherapy group (−1.55, p = 0.03) after the second of four massages. The mean change from baseline to the final assessment did not show a statistically significant reduction in pain scores in the aromatherapy (p = 0.87), massage (p = 0.63), combined massage (p = 0.69), and control group (p = 0.32). There were no significant long-term benefits of improving pain control with aromatherapy or massage. 29
Wrapped warm footbath
Wrapped warm footbath is an intervention that entails the following procedure: lower legs and feet are rubbed with olive oil, soaking of the feet, modulation of hot water to 38°C, patient’s legs wrapped with a plastic bag, covering of the legs with a blanket, and washing feet with foamy body shampoo using cotton gloves. 35 This study reported that changes in VAS scores (4.11 ± 2.58 to 1.78 ± 1.82) showed that the wrapped warm footbath gave significant pain relief (p = 0.047) compared to the control group (2.44 ± 2.30 to 2.54 ± 2.54, p = 0.813). 35
Reflexology
One study described a home-based reflexology intervention on the feet and entails applying firm walking motion pressure to specific areas on the feet, referred to as reflexes, for 15 min/foot. The intervention was applied once per week for 4 weeks and was more successful in its effect on pain than the attention control (odds ratio = 1.84; 95% CI: 1.05, 3.23; p = 0.03). 36
Best-evidence synthesis
Moderate evidence was ascertained for the use of massage therapy interventions based on two studies of low quality, four of medium quality, and one of high methodological quality. One study of low methodological quality did not have significant improvements in pain scores (p < 0.05), whereas the remainder did find significant improvement in pain scores. For the aromatherapy massage intervention insufficient evidence was found based on one medium methodological quality study not reaching statistical significance.
Moderate evidence for no effect was determined for mindful breathing interventions based on three medium methodological quality studies that failed to reach statistical significance.
Limited evidence was found for the VR intervention based on one medium and one high methodological quality study for which both reached statistically significant reduced pain scores. For one intervention, the reduction in pain scores was only statically significant when patients virtually visited a memorable place.
Insufficient evidence was found for the art therapy interventions based on one medium and one low methodological quality study for which both reached statistically significant reduced pain scores.
All other interventions were single studies with different methodological qualities; therefore, insufficient evidence was found for these interventions.
In order of the level of methodological quality of the study and the intervention reaching statistically significant reduction in pain scores, insufficient evidence was found for: (a) hypnosis, based on one high methodological quality study with a statistically significant reduction in pain scores immediately and at the 1- and 2-year follow-up and (b) PMR-IGI, cognitive-behavioral audiotapes, wrapped warm footbath, reflexology, and music therapy based on one medium methodological quality study.
In order of the level of methodological quality of the study and the interventions not reaching statistical significant reduction in pain scores, insufficient evidence was found for: (a) MBSR based on one high methodological quality study that failed to reach statistical significance even at the follow-up of 8 weeks and home-practice exercises and (b) aromatherapy intervention based on one medium methodological quality study that did not reach statistically significant results on pain reduction.
An overview of the results of the best-evidence synthesis is provided in Table 4.
Results of the best-evidence synthesis.


Colors are consistent with methodological quality table and based on the determined level of evidence found. Orange = moderate or limited evidence, Red = insufficient evidence.
MBSR, Mindfulness-Based Stress Reduction; PMR-IGI, progressive muscle-relaxation and interactive guide imagery; VR, virtual reality.
Discussion
Main findings
The objective of this systematic review was to identify NPI in the nursing scope of practice to help manage pain in palliative care patients. This review found moderate evidence supporting the use of massage therapy and limited evidence for the use of VR in reducing pain. Art therapy, which did show significant pain reduction, had insufficient evidence to support its use. Moreover, moderate evidence was found that mindful breathing did not reduce pain. All other interventions were insufficiently investigated. Hypnosis, PMR-IGI, cognitive-behavioral audiotapes, wrapped warm footbath, reflexology, and music therapy showed promise in reducing pain. However, MBSR, aromatherapy, and aroma-massage therapy did not. Although some interventions showed positive results on pain reduction, the evidence is still insufficient due to the small number of studies per intervention. Based on the available evidence, massage therapy and VR are the most recommended NPI for nurses to use in pain management. Art therapy had insufficient evidence due to lower quality studies but showed potential due to significant reduction in pain scores. Art therapy has potential but requires more research. Mindful breathing did not support pain management.
Implications for practice
Despite not always finding a statistical significance or being a low methodological quality study, the potential of NPI in this systematic review should not be overlooked. The studies included in this review did not state or report any adverse effects. All studies showed an immediate short-term change in pain scores. For palliative care patients, these possible benefits without any identified risks could be valuable in their pain management. Nurses are essential in the identification of pain, providing pain management (information and interventions), and evaluating its effect. 4 The NPI identified all fit within the nursing scope of practice, either by providing information and/or providing NPI. Most interventions found were not delivered by nurses, but by other professionals. Therefore, to ensure safe practice of these interventions instructions or training of nurses is advised and/or presence of the professional in administering the interventions when instructing patients, providing physical touch, or actively participating in the intervention. 40 If appropriate, certain NPI can be easily self-administered by patients themselves or their informal caregivers, promoting autonomy and a sense of control.
With the feasibility of the NPI to nursing scope of practice, nurses can help alongside the multi-professional team in direct pain management in palliative care patients. The local context matters for the feasibility of the interventions in the nursing scope of practice. The fact that nurses can perform or learn these interventions can increase the transfer to other contexts, of course the availability of resources is a possible limiting factor in this transfer.
Comparisons with literature
The NPI with evidentiary support identified in this review, VR, massage therapy, and art therapy, a promising trend is seen in comparison with other studies. A systematic review on the effect of VR on acute pain stated that 83% of all studies found (n = 23) reported pain reduction while using VR compared with no VR use. 41 This review highlights the importance of acknowledging the patient’s sense of presence and levels of immersion, interaction, and interest when deploying VR, which will also be very important in palliative care, taking the vulnerable cognition into account. 41 Visual art therapy in general cancer care showed that program-based art-making may provide participants with opportunities for learning about themselves, support, enjoyment, and distraction. Learning about self-management of pain and a sense of control were also mentioned within the individual art-making. 42 The distraction component is something that was apparent in many studies identified in this systematic review as well the presence and engagement with others may have reduced the pain scores. 42 Massage therapy is a common practice proposed for many painful conditions. Its potential is thoroughly researched, as various conditions may respond differently to massage. In the evidence map-article on massage for pain, the authors identified 49 systematic reviews on this topic. 43 The authors state that the conclusions have a low strength of evidence because few primary studies with large samples and rigorous methods had been conducted, leaving knowledge gaps about specific massage types for specific pain. 43 In this systematic review the evidence on massage therapy was found within the same population of interest, palliative care patients. Within the best-evidence synthesis, massage therapy interventions were compared, and they had some comparisons in massage techniques that were used and differences in duration and frequencies. 43 The findings were contradictory within immediate and sustained outcomes, and the methodological quality differed between studies. The trend showed that most massages statistically significantly reduced pain. 43
Strengths and limitations
This systematic review has some strengths and limitations. One strength is its adherence to a reproducible methodology outlined in the Cochrane Handbook for Systematic Reviews of Interventions. Furthermore, various stages of the review were double-checked such as the detailed search strategy, title and abstract selection, and the methodological quality of individual studies. Another strength is the use of a best-evidence synthesis to draw a conclusion from the found evidence despite the heterogeneity of the interventions, subjective measurement tools, and differences in populations.
This systematic review also had some limitations. Studies could have been missed that were written in languages other than English or Dutch. Despite contacting the authors, three articles remained unavailable in full-text. Therefore, not all current information could be presented, potentially influencing the conclusion. A couple of limitations had an influence on the generalizability of this review. Most studies had pretest and posttest measurement(s). Some studies examined the immediate and sustained effect of the intervention on pain scores. The sustained effect varied from hours after intervention delivery to 8–9 weeks using the intervention. One study assessing hypnosis and self-hypnosis had a long-term follow-up of 1 and 2 years and was performed on outpatients of a pain therapy clinic with varying chronic diagnoses. A long-term follow-up might have been possible due to these patients having a different life expectancy than the participants in the other studies. The baseline pain scores were also high, and their referral to the pain clinic might indicate that this intervention could be helpful for palliative care patients with severe chronic pain conditions. Referral to the pain clinic is indicated for patients with more severe pain, this can influence the effect of intervention in terms of pain scores. Many studies did not specify the type of pain, acute or chronic, for which the intervention was provided. This also applies to this review on the total pain experience. Also, most studies assessed the effects of the intervention on symptom burden, such as anxiety of distress. Although this fits the total pain approach, a direct pain-relieving factor is difficult to ascertain. For several studies, it remains unclear whether the intervention was fully accountable for the change in pain scores or if it was partly due to the attention given to the palliative care patients. Various study designs were used, and what was considered ‘control’ differed among them. Depending on what is considered as an NPI, the active control groups of a study may be considered as another NPI. Another limitation on generalizability was the country- or culture-specific interventions. A study on music therapy was conducted in India, utilizing a particular type of traditional music. It is possible that the results may differ if the intervention is tested in a different country, suggesting that culture-specific music may be more effective in reducing pain scores rather than Indian music itself. Other interventions are not limited to a specific culture. Therefore, the application of such studies should be assessed as the intervention techniques may vary depending on the country. Some studies had a small sample size concerning the generalizability of the results to the population of palliative care patients. Although getting a large enough sample in this vulnerable group of patients is a challenge at the onset, the results could be falsely concluded because the true effect can be underestimated due to the smaller sample sizes.
The studies were divided into the four modalities of NPI according to the Dutch national standard. Results could have been grouped differently when divided into the international standard for complementary therapies provided by the National Center for Complementary and Integrative Health. No studies were ascertained into the modality of energy therapies. This might be due to this review assessing their effect on pain and not on other symptoms or energy therapies being researched in other populations other than palliative care patients. For the population of oncology patients and patients with chronic illnesses, reviews were found on the use of energy therapies. A review on energy therapies in general oncology nursing showed that reiki, therapeutic touch, and healing touch are used to help patients feel relaxed, calm, or soothed; to decrease anxiety; improve the ability to fall asleep and stay asleep; reduce pain; and increase inner peace. 44 It showed the potential of this modality on the value for cancer patients. 44 A review of energy healing on chronic illnesses indicated some improvement in illness symptoms; however, high-level evidence consistently demonstrating efficacy is lacking. 45 Furthermore, it is unclear which elements of energy healing interventions are associated with positive outcomes. 45 Both reviews show promising results on symptom management and quality of life and thus robust trials to assess its effect on pain scores in palliative care patients are necessary.
To increase the level of evidence for NPI, more clinical trials should be performed, comparing NPI and studying the length of their effect. Besides, studies should include a thorough description of the intervention and the comparison, including the professional performing the intervention and the definition and measure of the outcome of interest.
Conclusion
This systematic review identified studies of NPI in the nursing scope of practice for pain relief in palliative care patients. VR, massage therapy, and art therapy are NPI identified with the most evidentiary support within the best-evidence synthesis. VR and massage therapy have moderate and limited evidence and art therapy has insufficient evidence to support pain management. Despite not all studies reaching statistically significant changes in pain scores, the changes can be clinically relevant to palliative care patients as there are no adverse effects. All NPI can be applied in pain management in which the palliative care patients’ needs and wishes, together with disease progression and contra-indications are to be reviewed. Nurses would need specific instructions or training to deliver most of the interventions to ensure safe practice. Evidence-based NPI in the nursing scope of practice have a possible influence on pain and thereby on patients’ quality of life and care in an end-of-life situation. In educating nurses, awareness should be increased about their competencies and tasks with regard to NPI in pain management for their patients. It should be discussed with the patient for consideration because of its potential value, however, methodologically rigorous research for NPI in the nursing scope of practice for pain relief in palliative care patients is still a necessity.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524231222496 – Supplemental material for Non-pharmacological interventions feasible in the nursing scope of practice for pain relief in palliative care patients: a systematic review
Supplemental material, sj-docx-1-pcr-10.1177_26323524231222496 for Non-pharmacological interventions feasible in the nursing scope of practice for pain relief in palliative care patients: a systematic review by Suzan van Veen, Hans Drenth, Hans Hobbelen, Evelyn Finnema, Saskia Teunissen and Everlien de Graaf in Palliative Care and Social Practice
Footnotes
Appendix
Search string databases.
| PubMed | Search |
|---|---|
| Domain (#1) | ‘palliative care’[MeSH Terms] OR ‘Hospice and Palliative Care Nursing’[MeSH Terms] OR ‘Palliative Medicine’[MeSH Terms] OR ‘Terminal Care’[MeSH Terms] OR ‘end of life’[Tiab] OR ‘palliation’[Tiab] OR ‘palliative*’[Tiab] OR ‘hospice*’[Tiab] OR ‘terminal care’[Tiab] OR ‘advanced care’ OR ‘terminally ill’[MeSH Terms] OR ‘terminally ill’[Tiab] |
| Determinant (#2) | (‘oils, volatile’[MeSH Terms] OR (‘oils’[Tiab] AND ‘volatile’[Tiab]) OR ‘volatile oils’[Tiab] OR (‘essential’[Tiab] AND ‘oils’[Tiab]) OR ‘essential oils’[Tiab]) OR (‘acupressure’[MeSH Terms] OR ‘acupressure’[Tiab]) OR biofield[Tiab] OR (‘therapeutic touch’[MeSH Terms] OR (‘therapeutic’[Tiab] AND ‘touch’[Tiab]) OR ‘therapeutic touch’[Tiab] OR ‘reiki’[Tiab]) OR (‘cognitive behaviour therapy’[Tiab] OR ‘cognitive behavioral therapy’[MeSH Terms] OR ‘cognitive behavioral therapy’[Tiab] OR ‘cognitive behavior therapy’[Tiab]) OR (‘biofeedback, psychology’[MeSH Terms] OR ‘biofeedback’[Tiab]) OR (‘phototherapy’[MeSH Terms] OR ‘phototherapy’[Tiab] OR (‘light’[Tiab] AND ‘therapy’[Tiab]) OR ‘light therapy’[Tiab]) OR (‘hypnosis’[MeSH Terms] OR ‘hypnosis’[Tiab]) OR (‘musculoskeletal manipulations’[MeSH Terms] OR (‘musculoskeletal’[Tiab] AND ‘manipulations’[Tiab]) OR ‘musculoskeletal manipulations’[Tiab] OR ‘reflexology’[Tiab]) OR ((‘relaxation’[MeSH Terms] OR ‘relaxation’[Tiab]) AND (‘exercise’[MeSH Terms] OR ‘exercise’[Tiab])) OR ((‘abdomen’[MeSH Terms] OR ‘abdomen’[Tiab] OR ‘abdominal’[Tiab]) AND (‘respiration’[MeSH Terms] OR ‘respiration’[Tiab] OR ‘breathing’[Tiab])) OR (‘autogenic training’[MeSH Terms] OR (‘autogenic’[Tiab] AND ‘training’[Tiab]) OR ‘autogenic training’[Tiab] OR (‘progressive’[Tiab] AND ‘muscle’[Tiab] AND ‘relaxation’[Tiab]) OR ‘progressive muscle relaxation’[Tiab]) OR ((‘imagery, psychotherapy’[MeSH Terms] OR (‘imagery’[Tiab] AND ‘psychotherapy’[Tiab]) OR ‘imagery’[Tiab]) AND (‘education’[Subheading] OR ‘education’[Tiab] OR ‘training’[Tiab] OR ‘education’[MeSH Terms] OR ‘training’[Tiab])) OR (‘meditation’[MeSH Terms] OR ‘meditation’[Tiab]) OR (‘yoga’[MeSH Terms] OR ‘yoga’[Tiab]) OR (‘music’[MeSH Terms] OR ‘music’[Tiab]) OR (‘massage’[MeSH Terms] OR ‘massage’[Tiab]) OR (‘aromatherapy’[MeSH Terms] OR ‘aromatherapy’[Tiab]) OR (‘odorants’[MeSH Terms] OR ‘odorants’[Tiab] OR ‘aroma’[Tiab]) OR (‘mindfulness’[MeSH Terms] OR ‘mindfulness’[Tiab]) OR (‘diet’[MeSH Terms] OR ‘diet’[Tiab] OR ‘diets’[Tiab]) OR (‘art’[MeSH Terms] OR ‘art’[Tiab]) OR psychoeducation[Tiab] OR herbs[Tiab] OR (‘dietary supplements’[MeSH Terms] OR (‘dietary’[Tiab] AND ‘supplements’[Tiab]) OR ‘dietary supplements’[Tiab] OR (‘nutritional’[Tiab] AND ‘supplements’[Tiab]) OR ‘nutritional supplements’[Tiab]) OR (‘homeopathy’[MeSH Terms] OR ‘homeopathy’[Tiab] OR ‘homoeopathy’[Tiab] OR ‘homeopathic’[Tiab]) OR ‘shiatsu’[Tiab] OR (‘virtual reality’[MeSH Terms] OR ‘virtual reality’[Tiab]) OR ‘color therapy’[Tiab] OR (‘color*’[Tiab] AND ‘therapy’[Tiab]) OR ‘acoustic stimulation’ [Tiab] OR ‘acoustic stimulation’ [MeSH Terms] OR ‘auditory stimulation’ [Tiab] OR ((‘acoustic’ [Tiab] OR ‘auditory’ [Tiab]) AND (‘therapy’[Tiab] OR ‘stimulation’[Tiab])) OR complementary[Tiab] OR complementary[Tiab] OR ((‘complementary’ [Tiab] AND ‘alternative’ [Tiab] AND ‘medicine’[Tiab]) OR ‘complementary alternative medicine’[Tiab]) OR (‘complementary therapies’[MeSH Terms] OR ‘complementary therapies’[Tiab]) |
| Outcome (#3) | ((‘pain’[MeSH terms] OR ‘pain*’[Tiab] OR ‘discomfort*’[Tiab] OR ‘ache*’[Tiab] OR ‘aching’[Tiab] OR ‘sore*’[Tiab] OR ‘suffer*’[Tiab] OR ‘agony’[Tiab] OR ‘hurt*’[Tiab] OR ‘strain’[Tiab] OR ‘torment’[Tiab] OR ‘twinge’[Tiab] OR ‘symptom’[Tiab] OR ‘symptom burden’[Tiab] OR (‘symptom’[Tiab] AND ‘burden’[Tiab])) AND (assess*[Tiab] OR relief[Tiab] OR reliev*[Tiab] OR reduc*[Tiab])) |
|
|
|
| Domain (#1) | ‘palliative nursing’/exp OR ‘palliative therapy’/exp OR ‘terminal care’/exp OR ‘end of life care’:ti,ab OR ‘palliation’:ti,ab OR ‘palliative*’:ti,ab OR ‘hospice*’:ti,ab OR ‘terminal care’:ti,ab OR ‘terminally ill patient’/exp OR ‘terminally ill’:ti,ab OR ‘advance care’:ti,ab |
| Determinant (#2) | ‘essential oil’/exp OR ‘essential oil’:ab,ti OR (‘oils’:ab,ti AND ‘volatile’:ab,ti) OR ‘acupressure’/exp OR ‘acupressure’:ab,ti OR ‘biofield therapy’/exp OR ‘biofield therapy’:ab,ti OR ‘therapeutic touch’/exp OR ‘therapeutic touch’:ab,ti OR ‘reiki’/exp OR ‘reiki’:ab,ti OR ‘cognitive behavioral therapy’/exp OR ‘cognitive behavioral therapy’:ab,ti OR ‘biofeedback’/exp OR ‘biofeedback’:ab,ti OR ‘phototherapy’/exp OR ‘phototherapy’:ab,ti OR (‘light’:ab,ti AND ‘therapy’:ab,ti) OR ‘hypnosis’/exp OR ‘hypnosis’:ab,ti OR ‘musculoskeletal manipulation’/exp OR ‘musculoskeletal manipulation’:ab,ti OR (‘musculoskeletal’:ab,ti AND ‘manipulation’:ab,ti) OR ‘reflexology’:ab,ti OR ‘relaxation training’/exp OR ‘relaxation training’:ab,ti OR ‘abdominal breathing’/exp OR ‘abdominal breathing’:ab,ti OR ‘autogenic training’/exp OR ‘autogenic training’:ab,ti OR ‘progressive muscle relaxation’/exp OR ‘progressive muscle relaxation’ OR ‘sleep hygiene’/exp OR ‘sleep hygiene’:ab,ti OR ‘imagery training’:ab,ti OR ((‘imagery’/exp OR imagery:ab,ti) AND (‘training’/exp OR training:ab,ti)) OR ‘meditation’/exp OR ‘meditation’:ab,ti OR ‘yoga’/exp OR ‘yoga’:ab,ti OR ‘music therapy’/exp OR ‘music therapy’:ab,ti OR ‘massage’/exp OR ‘massage’:ab,ti OR ‘aromatherapy’/exp OR ‘aromatherapy’:ab,ti OR ‘fragrance’/exp OR ‘fragrance’:ab,ti OR ‘aroma’/exp OR ‘aroma’:ab,ti OR ‘mindfulness’/exp OR ‘mindfulness’:ab,ti OR ‘diet’/exp OR ‘diet’:ab,ti OR ‘art’/exp OR ‘art’:ab,ti OR ‘psychoeducation’/exp OR ‘psychoeducation’:ab,ti OR ‘herb’/exp OR ‘herb:ab,ti OR ‘dietary supplement’/exp OR ‘dietary supplement’:ab,ti OR ‘nutritional supplements’:ab,ti OR (‘nutritional‘:ab,ti AND ‘supplements‘:ab,ti) OR ‘homeopathy‘/exp OR ‘homeopathy‘:ab,ti OR ‘shiatsu’/exp OR ‘shiatsu’:ab,ti OR ‘virtual reality’/exp OR ‘virtual reality’:ab,ti OR ‘color therapy’/exp OR ‘color therapy’:ab,ti OR (‘color*’:ab,ti AND ‘therapy’:ab,ti) OR ‘auditory stimulation’/exp OR ‘auditory stimulation’:ab,ti OR ((‘auditory’:ab,ti OR ‘acoustic’:ab,ti) AND (‘stimulation’:ab,ti OR ‘therapy’:ab,ti)) complementary:ab,ti OR ‘complementary alternative medicine’:ab,ti OR (complementary:ab,ti AND alternative:ab,ti AND (‘medicine‘/exp OR medicine:ab,ti)) OR ‘alternative medicine’/exp OR ‘alternative medicine’:ab,ti |
| Outcome (#3) | ((‘pain’/exp OR ‘pain*’:ab,ti OR ‘discomfort’:ab,ti OR ‘suffer*’:ti,ab OR ‘ache*’:ti,ab OR ‘aching’:ab,ti OR ‘sore*’:ab,ti OR ‘agony’:ti,ab OR ‘hurt*’:ti,ab OR ‘strain*’:ti,ab OR ‘torment*’:ti,ab OR ‘twinge’:ti,ab OR ‘symptom*’:ab,ti OR ‘symptom burden’:ab,ti) AND (‘assess*’:ab,ti OR ‘relief’:ab,ti OR ‘reliev*’:ab,ti OR ‘reduc*’:ab,ti)) |
|
|
|
| Domain (#1) | MH ((MH ‘Terminal care’) OR (MH ‘Hospice care’) OR (MH ‘Palliative care’) OR (MH ‘Hospice and Palliative Nursing’)) OR TI (‘end of life care’ OR ‘palliation’ OR ‘palliative*’ OR ‘hospice*’ OR ‘terminal care’ OR ‘terminally ill’ OR ‘advance care’) OR AB (‘end of life care’ OR ‘palliation’ OR ‘palliative*’ OR ‘hospice*’ OR ‘terminal care’ OR ‘terminally ill’ OR ‘advance care’) |
| Determinant (#2) | MH (MH ‘essential oils’) OR (MH ‘acupressure’) OR (MH ‘therapeutic touch’) OR (MH ‘reiki’) OR (MH ‘phototherapy’) OR (MH ‘hypnosis’) OR (MH ‘reflexology’) OR (MH ‘progressive muscle relaxation’) OR (MH ‘guided imagery’) OR (MH ‘meditation’) OR (MH ‘yoga’) OR (MH ‘music therapy’) OR (MH ‘music’) OR (MH ‘massage’) OR (MH ‘aromatherapy’) OR (MH ‘odors’) OR (MH ‘mindfulness’) OR (MH ‘diet’) OR (MH ‘art’) OR (MH ‘psychoeducation’) OR (MH ‘dietary supplements’) OR (MH ‘homeopathy’) OR (MH ‘shiatsu’) OR (MH ‘virtual reality’) OR (MH ‘acoustic stimulation’) OR (MH ‘alternative therapies’) OR (MH (MH ‘relaxation’) OR TI (‘relaxation’) OR AB (‘relaxation’)) AND (TI (‘exercise*’) OR AB (‘exercise*’)) OR (MH (MH ‘abdomen’) OR TI (‘abdomen’ OR ‘abdominal’) OR AB (‘abdomen’ OR ‘abdominal’)) AND (MH (MH ‘respiration’) OR TI (‘respiration’ OR ‘breathing’) OR AB (‘respiration’ OR ‘breathing’)) OR (MH (MH ‘autogenic training’) OR TI (‘autogenic’ AND ‘training’) OR ‘autogenic training’ OR AB (‘autogenic’ AND ‘training’) OR ‘autogenic training’) OR ((MH (MH ‘guided imagery’) OR TI (‘psychotherapy imagery’ OR (‘psychotherapy’ AND ‘imagery’) OR ‘imagery’) OR AB (‘psychotherapy imagery’ OR (‘psychotherapy’ AND ‘imagery’) OR ‘imagery’)) AND (MH (MH ‘education’) OR TI (‘education’ OR ‘training’) OR AB (‘education’ OR ‘training’))) OR TI (‘volatile oils’ OR (‘oils’ AND ‘volatile’) OR ‘essential oils’ OR (‘essential’ AND ‘oils’) OR ‘acupressure’ OR ‘biofield’ OR ‘therapeutic touch’ OR (‘therapeutic’ AND ‘touch’) OR ‘reiki’ OR ‘cognitive behaviour therapy’ OR ‘cognitive behavioural therapy’ OR ‘biofeedback’ OR ‘phototherapy’ OR (‘light’ AND ‘therapy’) OR ‘light therapy’ OR ‘hypnosis’ OR ‘musculoskeletal manipulations’ OR (‘musculoskeletal’ AND ‘manipulations’) OR ‘reflexology’ OR (‘progressive’ AND ‘muscle’ AND ‘relaxation’) OR ‘progressive muscle relaxation’ OR ‘meditation’ OR ‘yoga’ OR ‘music therapy’ OR ‘music’ OR ‘massage*’ OR ‘aromatherapy’ OR ‘odors’ OR ‘odorants’ OR ‘aroma’ OR ‘mindfulness’ OR ‘diet’ OR ‘diets’ OR ‘art*’ OR ‘psychoeducation’ OR ‘herbs’ OR ‘dietary supplement*’ OR (‘dietary’ AND ‘supplement*’) OR (‘nutritional’ AND ‘supplement*’) OR ‘nutritional supplements’ OR ‘homeopathy’ OR ‘homoeopathy’ OR ‘homeopathic’ OR ‘shiatsu’ OR ‘virtual reality’ OR (‘virtual’ AND ‘reality’) OR ‘color therapy’ OR (‘color’ AND ‘therapy’) OR ‘acoustic stimulation’ OR (‘acoustic’ AND (‘stimulation’ OR ‘therapy’)) OR ‘auditory stimulation’ OR (‘auditory’ AND (‘stimulation’ OR ‘therapy’)) OR ‘alternative therapy’ OR ‘alternative therapies’ OR ‘complementary’ OR (‘complementary’ AND ‘alternative’ AND ‘medicine’) OR ‘complementary alternative medicine’ OR ‘complementary therapy’ OR ‘complementary therapies’) OR AB (‘volatile oils’ OR (‘oils’ AND ‘volatile’) OR ‘essential oils’ OR (‘essential’ AND ‘oils’) OR ‘acupressure’ OR ‘biofield’ OR ‘therapeutic touch’ OR (‘therapeutic’ AND ‘touch’) OR ‘reiki’ OR ‘cognitive behaviour therapy’ OR ‘cognitive behavioural therapy’ OR ‘biofeedback’ OR ‘phototherapy’ OR (‘light’ AND ‘therapy’) OR ‘light therapy’ OR ‘hypnosis’ OR ‘musculoskeletal manipulations’ OR (‘musculoskeletal’ AND ‘manipulations’) OR ‘reflexology’ OR (‘progressive’ AND ‘muscle’ AND ‘relaxation’) OR ‘progressive muscle relaxation’ OR ‘meditation’ OR ‘yoga’ OR ‘music therapy’ OR ‘music’ OR ‘massage*’ OR ‘aromatherapy’ OR ‘odors’ OR ‘odorants’ OR ‘aroma’ OR ‘mindfulness’ OR ‘diet’ OR ‘diets’ OR ‘art*’ OR ‘psychoeducation’ OR ‘herbs’ OR ‘dietary supplement*’ OR (‘dietary’ AND ‘supplement*’) OR (‘nutritional’ AND ‘supplement*’) OR ‘nutritional supplements’ OR ‘homeopathy’ OR ‘homoeopathy’ OR ‘homeopathic’ OR ‘shiatsu’ OR ‘virtual reality’ OR (‘virtual’ AND ‘reality’) OR ‘color therapy’ OR (‘color’ AND ‘therapy’) OR ‘acoustic stimulation’ OR (‘acoustic’ AND (‘stimulation’ OR ‘therapy’)) OR ‘auditory stimulation’ OR (‘auditory’ AND (‘stimulation’ OR ‘therapy’)) OR ‘alternative therapy’ OR ‘alternative therapies’ OR ‘complementary’ OR (‘complementary’ AND ‘alternative’ AND ‘medicine’) OR ‘complementary alternative medicine’ OR ‘complementary therapy’ OR ‘complementary therapies’) |
| Outcome (#3) | ((MH (MH ‘pain’) OR TI (‘pain*’ OR ‘discomfort’ OR ‘suffer*’ OR ‘ache*’ OR ‘aching’ OR ‘sore’ OR ‘agony’ OR ‘hurt*’ OR ‘strain*’ OR ‘torment*’ OR ‘twinge’ OR ‘symptom’ OR ‘symptom burden’) OR AB (‘pain*’ OR ‘discomfort’ OR ‘suffer*’ OR ‘ache*’ OR ‘aching’ OR ‘sore’ OR ‘agony’ OR ‘hurt*’ OR ‘strain*’ OR ‘torment*’ OR ‘twinge’ OR ‘symptom’ OR ‘symptom burden’) AND (TI (‘asses*’ OR ‘relief’ OR ‘reliev*’ OR ‘reduc*’) OR AB (‘asses*’ OR ‘relief’ OR ‘reliev*’ OR ‘reduc*’))) |
|
|
|
| Domain (#1) | exp Palliative Care/ OR exp Alternative Medicine/ OR exp Hospice/ OR exp Terminally ill patients/ OR palliative care.ti,ab. OR terminal care.ti,ab. OR end of life.ti,ab. OR palliation.ti,ab. OR palliative*.ti,ab. OR hospice*.ti,ab. OR advance care.ti,ab. OR terminally ill.ti,ab. |
| Determinant (#2) | exp Aromatherapy/ OR exp Cognitive behavior therapy/ OR exp Biofeedback/ OR exp Phototherapy/ OR exp Hypnosis/ OR exp Autogenic Training/ OR exp Progressive Relaxation Therapy/ OR exp Guided Imagery/ OR exp Imagery/ OR exp Meditation/ OR exp Yoga/ OR exp Music Therapy/ OR exp Massage/ OR exp Aromatherapy/ OR exp Mindfulness/ OR exp Diets/ OR exp Art Therapy/ OR exp Psychoeducation/ OR exp Medicinal Herbs and Plants/ OR exp Dietary Supplements/ OR exp Virtual Reality/ OR exp Auditory Stimulation/ OR volatile oils.ti,ab. OR (volatile AND oils).ti,ab. OR essential oils.ti,ab. OR (essential AND oils).ti,ab. OR acupressure.ti,ab. OR biofield.ti,ab. OR therapeutic touch.ti,ab. OR (therapeutic AND touch).ti,ab. OR reiki.ti,ab. OR cognitive behavior therapy.ti,ab. OR (cognitive AND behavior AND therapy).ti,ab. OR (cognitive AND behavioral AND therapy).ti,ab.OR cognitive behavioral therapy.ti,ab. OR (cognitive AND behaviour AND therapy).ti,ab. OR cognitive behaviour therapy.ti,ab. OR biofeedback.ti,ab. OR psychology biofeedback.ti,ab. OR (psychology AND biofeedback).ti,ab. OR phototherapy.ti,ab. OR light therapy.ti,ab. OR (light AND therapy).ti,ab. OR hypnosis.ti,ab. OR musculoskeletal manipulations.ti,ab. OR (musculoskeletal AND manipulations).ti,ab. OR reflexology.ti,ab. OR ((exp Relaxation/ OR relaxation.ti,ab.) AND (exp Exercise/ OR exercise*.ti,ab.)) OR ((exp Abdomen/ OR abdomen.ti,ab. OR abdominal.ti,ab. ) AND (exp Respiration/ OR respiration.ti,ab. OR breathing.ti,ab.)) OR autogenic training.ti,ab. OR (autogenic AND training).ti,ab. OR progressive muscle therapy.ti,ab. OR progressive muscle relaxation.ti,ab. OR (progressive AND muscle AND relaxation).ti,ab. OR (progressive AND relaxation AND therapy).ti,ab. OR ((guided imagery.ti,ab. OR psychotherapy imagery.ti,ab. OR (psychotherapy AND imagery).ti,ab. OR imagery.ti,ab.) AND (education.ti,ab. OR training.ti,ab.)) OR meditation.ti,ab. OR yoga.ti,ab. OR music therapy.ti,ab. OR (music AND therapy).ti,ab. OR massage*.ti,ab. OR aromatherapy.ti,ab. OR odorants.ti,ab. OR aroma.ti,ab. OR mindfulness.ti,ab. OR diet*.ti,ab. OR art*.ti,ab. OR art therapy.ti,ab. OR (art AND therapy).ti,ab. OR psychoeducation.ti,ab. OR herbs.ti,ab. OR dietary supplement*.ti,ab. OR (dietary AND supplement*).ti,ab. OR nutritional supplement*.ti,ab. OR (nutritional AND supplement*).ti,ab. OR homeopathy.ti,ab. OR homoeopathy.ti,ab. OR homeopathic.ti,ab. OR shiatsu.ti,ab. OR virtual reality.ti,ab. OR (virtual AND reality).ti,ab. OR acoustic stimulation.ti,ab. OR acoustic therapy.ti,ab. OR (acoustic AND (stimulation OR therapy)).ti,ab. OR (auditory AND (stimulation OR therapy)).ti,ab. OR complementary therapy.ti,ab. OR complementary.ti,ab. OR (complementary AND alternative AND medicine).ti,ab. OR complementary alternative medicine.ti,ab. OR complementary therapies.ti,ab |
| Outcome (#3) | (exp Pain/ OR pain.ti,ab. OR discomfort*.ti,ab. OR ache*.ti,ab. OR aching.ti,ab. OR sore*.ti,ab. OR suffer*.ti,ab. OR agony.ti,ab. OR hurts.ti,ab. OR strain.ti,ab. OR torment.ti,ab. OR twinge.ti,ab. OR symptom.ti,ab. OR (symptom AND burden).ti,ab. OR symptom burden.ti,ab.) AND (assess* OR relief OR reliev* OR reduc*).ti,ab. |
Acknowledgements
None.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.