
Abstract

Keywords
Compassionate Communities are gaining momentum as a public health approach for palliative care across the Americas, Asia-Pacific and Europe. 1 It first emerged as an effort to restore the social and spiritual aspects of hospice care, which had become overlooked when hospice services were mainstreamed as palliative care. 2 It represents a fundamental paradigm shift, mobilising entire communities to share the responsibility of supporting individuals facing dying, death and grief, transforming palliative care from solely a healthcare service into a form of civic engagement. Emerging evidence suggests that Compassionate Communities decrease unnecessary healthcare utilisation, leading to significant cost savings 3 and improve quality of life 4 and social connectedness. 5
However, as healthcare systems worldwide aspire to adopt Compassionate Communities to address the needs of ageing populations and rising demands for palliative care, we encountered three myths or misconceptions that warrant clarification. While the paradigm shift from medical to civic engagement is clear in theory, important distinctions are often misunderstood in practice, making clarifications necessary for the effective implementation and evaluation of these initiatives.
First, the Compassionate Communities approach to care is not simply another model of healthcare service delivery, although most Compassionate Communities initiatives are service-led.6,7 When healthcare services lead these initiatives, communities become recipients rather than drivers of change. This fosters dependency, with communities waiting for professional guidance instead of building their own capacity to handle dying, death and grief. The fundamental shift from “death is a medical or professional problem” to “death is everyone’s business” 8 does not happen because communities continue to see end-of-life care as solely a professional concern.
Thriving Compassionate Communities recognise clearly defined, complementary roles: healthcare professionals manage complex medical and social issues, while communities offer social support, belonging, meaning and ongoing participation, which clinical care alone cannot provide. When communities lead these social aspects and when healthcare services offer supporting expertise rather than control, both function from positions of strength and assets. This requires healthcare services to resist the urge to lead or impose their institutional approach. Instead, they should engage in open-minded and collaborative partnerships that allow communities to reclaim death as a shared social experience.
Second, Compassionate Communities do not replace palliative care services. Instead, they identify and connect the extensive yet fragmented support systems that already exist – families, neighbours, faith-based groups, volunteers, community programs, and health and social care services – by weaving them into cohesive networks. 7 This approach recognises that most caregiving happens outside of clinical settings, with family caregivers and social networks providing the majority of care while often facing health and social challenges.5,9 By mapping existing resources and creating visible pathways between them, Compassionate Communities transform scattered acts of individual compassion into coordinated collective action, ensuring no one navigates dying and grieving alone. 10
Third, Compassionate Communities is a practice committed to social and system change through building and enhancing community capacity. We refer to this as developing “compassion capital,” which is the collective capacity to recognise and respond to suffering related to dying, death and grief. It is an ethical imperative or a central value to generate a public health approach to end-of-life care. Currently, there is an overemphasis on educational and awareness-raising activities in building this capital. Many activities, such as death cafes and grief festivals, focus on providing death and grief literacy, hoping to foster more activated citizens to contribute to compassionate care. However, such activities alone are insufficient to develop compassion capital and activate Compassionate Communities.
Health promotion research shows knowledge alone rarely produces sustained behaviour change without addressing structural barriers. 6 Similarly, compassion capital requires practical skills, reciprocal relationships and repeated care experiences, all of which are fostered through social and systemic changes. Without these reforms, education remains ineffective, unable to translate understanding into sustained community action. The focus must shift from merely raising awareness to advocating for social and system changes and promoting civic responsibilities towards palliative and end-of-life care.
We showcase a strategy undertaken by Compassionate Communities Australia (CCAus) (https://compassionatecommunities.au) to advocate for social and system changes. We intend the showcase to be a reference example of how such advocacy could be conducted. We recognise that each country or region has its unique cultural, political and social contexts to develop its own advocacy approach.
CCAus organised an inaugural National Forum on Compassionate Communities that took place on 9 September 2025 in Brisbane, Australia. Over 150 representatives from local government, healthcare providers, workplaces and community groups across the country participated. The representatives shared experiences, collaborated and developed Advocacy Statements through roundtable discussions across seven settings and contexts: health services, home, hospices, local government, residential aged care, workplaces, and equity and diversity.
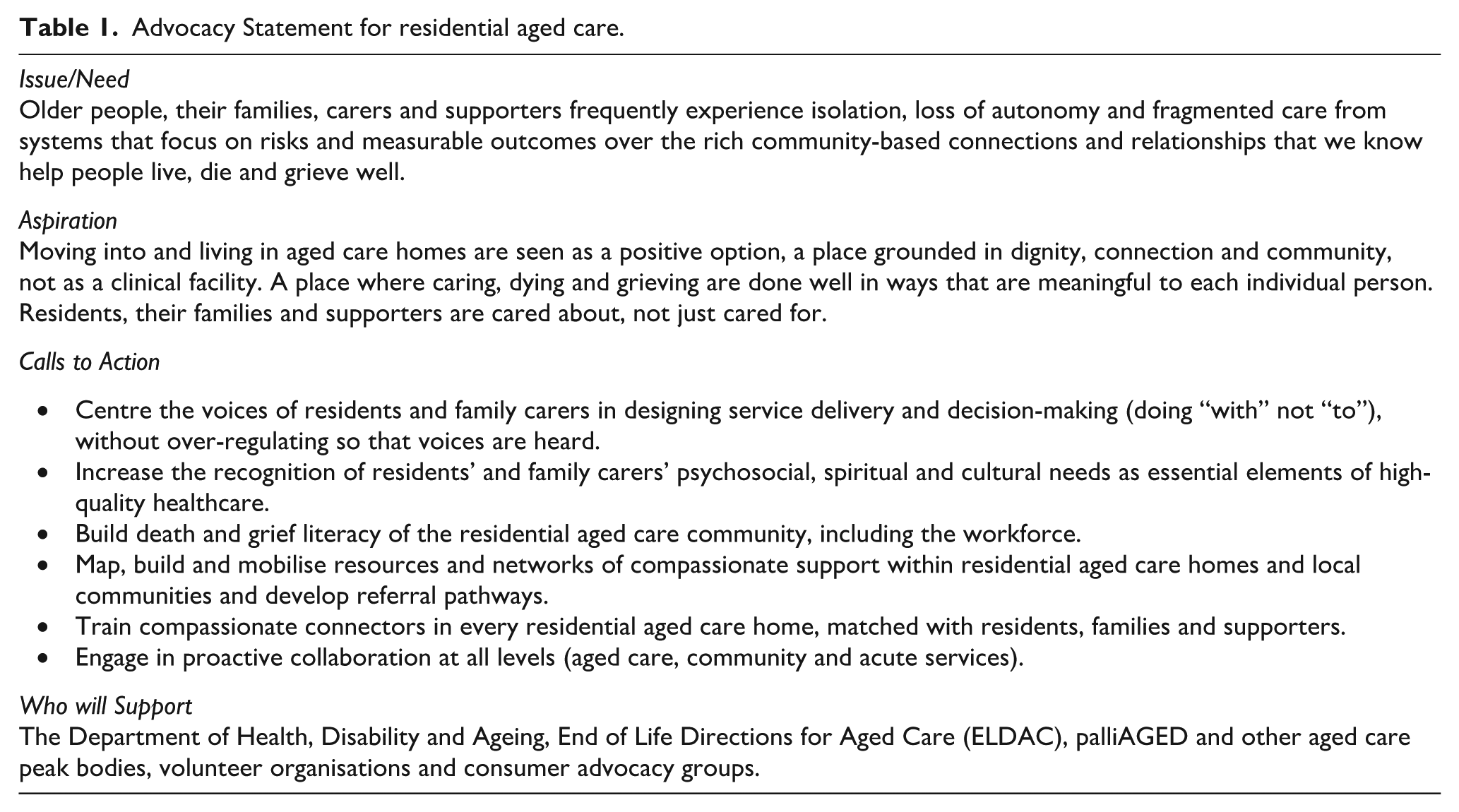
Each Statement identified issues and needs within its setting, articulated aspirations to address them, developed specific action points, and named potential partners for implementation. These Statements represent a collective call-to-action to strengthen and sustain Compassionate Communities, improve collaboration between community members, formal services, and civic organisations and recognise the social dimensions of care alongside clinical approaches. The Statements serve as conversation starters for individuals or organisations to initiate system changes. Table 1 shows an example of a Statement for the residential aged care sector.
Advocacy Statement for residential aged care.
CCAus launched its National Advocacy in Action Campaign to promote the use of the Advocacy Statements and inspire further actions. The year-long Campaign will showcase these advocacy statements one at a time, supported by national panel discussions, focusing on relational care rather than transactional care in every setting. The public can also share thoughts and ideas that help the case for social and systems change through the Campaign platform.
To conclude, with populations ageing at scale and palliative care demands escalating, activating Compassionate Communities is both a moral imperative and a practical necessity. Healthcare professionals, policymakers, funders and community members must unite beyond traditional boundaries to transform how societies support anyone experiencing caregiving, dying and grieving.
Footnotes
Author contributions
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Professor Samar Aoun AM is the chair of Compassionate Communities Australia, a registered charity.
Data availability statement
Not applicable.