
Abstract
Background:
As Compassionate Communities (CCs) are developing worldwide, there is a growing need to systematically assess if they are having the expected effects on the community. Although having a single strategy would be ideal in terms of standardization and comparison, due to the inherent heterogeneity of CCs, it is not known how feasible this would be.
Objectives:
To assess the feasibility of creating a general strategy, based on the results of a series of focus groups conducted across three diverse CCs, to guide the evaluation of already existing programs and the development of new ones.
Design:
Focus groups in three cities, including different types of stakeholders, were conducted to identify potential outcomes (benefits) from CCs, as the base of a general strategy to assess CCs.
Methods:
We coded the discussions and built a list of the outcomes mentioned. Then, we merged those similar enough into a more general one that encompassed the others. We extracted from reviews all the CCs outcomes that have been measured. We merged the outcomes from the focus groups and the reviews and built a single list.
Results:
We obtained a final list of 46 outcomes; 44 were reported from the focus groups, and two more were added from the reviews. Of the 44 from the focus groups, 22 (50%) were present in the three CCs, 14(32%) were present in two CCs, and the remaining 8 (18%) were present only in one compassionate community. There were outcomes commonly reported both in the three CCs and in the literature reviews related to training the general community in compassion and end-of-life topics, facilitating the development of community networks, and generating public spaces for social integration.
Conclusion:
Half of the identified outcomes were reported in the three CCs. This indicates the feasibility of creating a single strategy but also reflects the need to leave room to include other aspects specific to each community according to its context in the assessment.
Plain language summary
Compassionate Communities (CC) aim to support people in need by fostering a culture of care and compassion in neighborhoods and other social spaces. It is important to know if these communities are working and bringing the benefits as intended and to help new ones develop effectively. However, since every region is different socially and culturally, creating a single list of benefits might be challenging. In our study, we wanted to see if it is possible to develop a general list of benefits that can be used to assess how existing Compassionate Communities are working and guide the creation of new ones. We conducted focus groups in three diverse cities, involving various stakeholders to gather their insights. These discussions helped us identify different positive outcomes (benefits) that CCs might achieve. We held 14 focus groups and analyzed the discussions to compile a list of outcomes. We then combined similar outcomes and included additional outcomes from scientific papers. In total, we identified 46 outcomes, with 44 coming from our focus groups and 2 from the scientific papers. Out of the 44 focus group outcomes, half were reported in all three cities, 32% were seen in two cities, and the remaining 18% were unique to one city. Some common outcomes across all three cities and the scientific papers included educating the community about compassion and end-of-life issues, creating community networks, and providing public spaces for social integration. Our findings suggest that some core outcomes are consistent across different Compassionate Communities, indicating the possibility of creating a unified list of outcomes (benefits). However, the list should also be flexible enough to include outcomes specific to each community’s unique context. This approach could help ensure that Compassionate Communities are effectively supporting their members while being adaptable to different cultural and socioeconomic environments.
Keywords
Introduction
The Compassionate Communities (CCs) initiative is a social model of care in which a social networking community promotes health, recognizes end-of-life needs, and proactively shares in holistic end-of-life care. 1 CCs foster and support actions at individual, group, and societal levels to prevent or alleviate suffering associated with serious illness, death, dying, and loss. They recognize these experiences as natural aspects of everyday life, actively encourage health and well-being, and empower their members. 2 Furthermore, CCs promote the creation of resilient cities by empowering members of specific communities to help each other during illness and caregiving.3,4 Creating and sustaining CCs requires a great deal of time, resources, effort, and work. However, due to the lack of systematic evaluation of these programs, it is not known whether CCs are having the benefit they are expected to have. Herein lies the importance of a CC evaluation strategy or tool contributing to solving the question.
A general evaluation strategy or tool would bring several advantages, such as being able to assess if the outcomes of the different initiatives match the expected ones and comparing initiatives with each other to provide feedback. Through a collaboration led by Switzerland and two Latin American countries (Argentina and Colombia) that also includes representation from other countries, we intend to create, as a long-term goal, a strategy to evaluate already existing CC programs and to guide the development of new ones. 5 For the development of the evaluation strategy, it is essential to identify the outcomes or, as we prefer to call them, benefits that CCs should have. Since they can be multiple and varied, we aim to identify those that could be essential to all programs as a medium-term goal. To identify such benefits, we adopted the methodology proposed by The Core Outcome Measures in Effectiveness Trial (COMET) initiative.6,7 The COMET approach recommends four stages for Core Outcomes Set development: (1) a systematic review of the literature to identify outcomes that have already been evaluated, (2) fieldwork to collect information to identify outcomes from the point of view of different experts, (3) a Delphi process to rank both the outcomes from the systematic review and the fieldwork and (4) a consensus meeting to propose and agree on the final set of core outcomes.
In this paper, we present the outcomes or benefits identified in steps 1 and 2, that is, the outcomes from literature reviews and the fieldwork in three cities, Bern, Buenos Aires, and Medellin, different in terms of geography, population size, culture, and resources. Our short-term goals in this paper are to (1) compare the benefits identified in the fieldwork with those previously reported in literature reviews and (2) assess if and how the benefits vary across cities as a preliminary way to assess to which extent cultural and socioeconomic backgrounds affect the experience of CCs, and thus the feasibility of creating a single strategy.
Methods
Study design
This is a multicenter multiple-methods study 5 that follows the methodology developed by COMET, 7 which involves: (i) reviewing the literature to identify outcomes that have already been reported in studies, (ii) identifying outcomes from the perspective of different experts, (iii) carrying out a Delphi survey to rank all the previously identified outcomes, and (iv) agreeing on a final set of outcomes during a consensus meeting.
To identify existing outcomes from other studies, we included four reviews that had been published before October 2023 on outcomes or the effectiveness of CCs.8 –11
For the fieldwork, we conducted focus groups in three cities. The compassionate community programs of the chosen cities follow Kellehear’s theoretical framework of a compassionate community. 12 We included representatives of four stakeholder groups in each city: (1) users of the compassionate community, (2) healthcare providers, (3) members of (non-) governmental organizations allied with the compassionate community, and (4) the coordinators of the compassionate community. Users included citizens who had participated in local compassionate community activities such as caregivers, family members, and members of the neighborhood networks. Healthcare providers included physicians, nurses, psychologists, social workers, and occupational therapists. Nongovernmental organizations included representatives of churches, funeral homes, and schools. Governmental institutions included the local health department and public institutions involved in the care of the elderly or persons with complex needs. Finally, in the group of coordinators were those persons who collaborated in the creation of the compassionate community or who oversaw its operation.
We asked the coordinators of each CC program to recruit between 5 and 12 participants for each focus group. Since each program is managed in different ways, the recruitment process was left to the preference of each program (convenience recruitment). In Bern, participants were contacted via email from a database with the information of all people who have been part of the compassionate community (attending events, volunteering, and creating institutional alliances). In Buenos Aires, the coordinators of the program contacted key collaborators or allies from the medical sector and governmental and nongovernmental institutions via phone and invited key representatives of or leaders from the community also via phone. Finally, in Medellin, events and alliances are managed using a WhatsApp group that links different types of people and institutions to the network, as well as individual groups (e.g., a group including all the caregivers who have attended the compassionate care courses). The coordinating group in Medellin then used this medium to invite participants. In Bern and Buenos Aires, focus groups were held in rooms adjacent to the wards of a hospital involved in the coordination of the programs. In Medellin, the facilities of the university that coordinates the program were used.
After obtaining signed informed consent from each of the participants, they provided written details about their demographic characteristics: Age, gender, role in the compassionate community, and how long they had been part of it. Then, we made a presentation about the overall structure of the local compassionate community and the aims and the methods of the study so the attendees had a clearer picture of the program and the study before discussing (potential) benefits of the program. We started the presentation by introducing ourselves, our job, and our role in the research. The presentation did not mention intended outcomes or benefits but rather showed the chronological history of the program as well as the different lines of action and initiatives that are part of the program. Each compassionate community had many actions, and not all the focus group attendees had participated or were necessarily aware of all the activities within their compassionate community. After the presentation, we conducted a group discussion following a semi-structured interview, including questions such as if they believed that the compassionate community brought benefits and, if so, which benefits had brought to them or the community in general; if the community still had unmet needs that the compassionate community could support, among others (Supplemental Material 1). All the questions were focused on identifying either benefit that they thought the program had already brought or those that had not yet been achieved but that they believed the program could bring, that is, potential benefits. In each focus group, at least three members from the research team were present: One moderator (VGJ, SF), one person taking field notes to support the coding process (MJ, MCV, and VGJ), and one supporting the logistics such as delivery of the documents collecting the informed consent, and voice-recording the discussions (SO, FL, TN, SM). Besides the researchers and the participants, there were no other attendees in the focus groups. None of the moderators had an established relationship with the participants from the study, whereas the persons taking field notes and supporting the logistics of the focus groups knew the participants from previous encounters with the compassionate community.
Setting
As explained, this study was conducted in three cities, each from a different country: Bern (Switzerland), Buenos Aires (Argentina), and Medellin (Colombia). More information about each setting and context can be found in the study protocol 5 and Table 1.
Characteristics of the Compassionate Communities and the focus groups.

CC, Compassionate Community.
Data analysis
Systematic review
At the time this research was conceived, we had identified two reviews8,9 reporting outcomes or attempts to measure CC effectiveness. Therefore, we did not conduct a systematic review but, instead, extracted the outcomes from the published ones. To make sure we were not overlooking any other possible review, we conducted a search in PubMed ((“compassionate communities” OR “compassionate cities”) AND (review[pt] OR “systematic review”[pt] OR “meta-analysis”[pt] OR review[tiab] OR “systematic review”[tiab] OR “meta-analysis”[tiab]) AND (outcomes OR effectiveness OR evaluation OR measurement OR benefit OR model)). To capture more outcomes, we did not limit it to systematic reviews but also included other types of reviews, such as scoping reviews. Two independent reviewers screened the titles and abstracts and then conducted full-text reviews to evaluate potentially relevant articles. Reviewers resolved disagreements through discussion. In the case of a lack of consensus between the reviewers, a third reviewer was available to solve any disagreement. However, this was not necessary. Two members of the team independently extracted the outcomes from each of the reviews, and then compared results to make sure all were included.
Focus groups
This part of the study is reported following the Consolidated criteria for reporting qualitative research (COREQ) guideline 13 (Supplemental Material 2).
We used conventional content analysis 14 to identify expected benefits/outcomes. A researcher (VGJ) and one research assistant coded the first focus group independently using EXCEL; both of whom then compared the results aiming to ensure that the researcher that was going to independently code the rest of the focus groups paid attention to all significant occurrences. VGJ is a female MD and PhD working at the time of the study as a postdoc in a palliative care research team, with experience in both quantitative and qualitative research in epidemiology and public health. LV is a female psychologist working as a psychologist and research assistant of a palliative care research team with experience in qualitative research. We did not use a predetermined list of categories or subcategories but assigned codes inductively.
Once all focus groups were coded, VGJ first put duplicate codes together. Then, VGJ put together those codes that were similar enough to be merged into a more general one that encompassed the key ideas. Then, VGJ, SCZ, and SE put together outcomes that discussed similar topics: without eliminating any content, we merged similar codes by creating longer sentences.
To present the benefits more logically and to facilitate their visualization, we decided to group them by categories. Since there is currently no classification system for the benefits or outcomes of CCs, VGJ, SCZ, and SE created the categories. SCZ is a female psychologist and PhD, working as an assistant professor at the time of the study, with experience in qualitative research. SE is a male MD working as a physician and head of a palliative care research group during the time of the study, with experience in both quantitative and qualitative research.
Results
General characteristics of the participants
We conducted 14 focus groups across the three cities. Although we had initially scheduled five for each city, in Bern, we had to merge the nongovernmental organizations and the governmental organizations due to the lack of response from the invited people. All those who declined the invitation claimed a lack of time availability. A total of 98 persons participated in the focus groups, of which 83% were women. Of the participants, 25% were caregivers or other general community members, 20% were healthcare providers, 32% were part of a governmental or nongovernmental organization, and 21% were part of the coordinating group. The ages of the participants ranged from 22 to 78 years (Table 1).
General characteristics of the outcomes identified
We extracted 861 benefits from the focus groups. After pooling duplicates, 326 unique ones resulted. After pooling those that were similar enough to merge, a total of 70 outcomes remained. We then merged these benefits thematically for a final list of 44 benefits from the focus groups. We identified two additional benefits in the reviews and added them to the list, for a total of 46 benefits.
From our literature search of reviews reporting outcomes of CCs, we identified 38 potentially relevant citations (the last search was in October 2023). We screened titles and abstracts and selected the full texts of 10 articles to evaluate in detail. After a full-text assessment, we included four reviews that included papers assessing outcomes, effectiveness, or ways to evaluate CCs.8 –11 Then, we crossed these outcomes with the ones from the focus groups and tried to match each of the review outcomes with one of the 46 from the focus groups. This was possible for the majority of the outcomes. However, we found that two of the outcomes of the reviews did not have an equivalent from the focus groups list and, therefore, added them for a total of 46 benefits (Table 2).
Total list of outcomes by theme.

The resulting categories grouping the benefits to present them more logically were: “Advocacy and Policy Impact,” “Community Awareness and Preparedness,” “Community Engagement/Connection and Social Support,” “Cultural and Attitudinal Change,” “Health and Health System,” “Information and Resource Accessibility,” “Local collaboration and Exchange Among Institutions,” and “Training and Education” (Table 2).
Comparison between outcomes reported in the literature reviews and those reported in the focus groups
Among the list of 46 benefits, 12 were part of the top 25% most reported during the focus groups, and 7 were part of the top 25% most reported in the reviews. There was some overlap among those more commonly reported at each source (focus group or reviews): five benefits were commonly reported in both sources; two were only present at the top of the literature reviews, and only seven were present at the top of the focus groups (Table 3). The ones that were commonly reported in both sources were about training the general community in end-of-life aspects, improving the quality of patient care, facilitating the creation of community networks, influencing public policies, and transforming society into a more compassionate one. Of the two outcomes that were present only in the top 25% of the reviews, one, which was the third most reported in the reviews, was not mentioned in the focus groups: “Promote home care, decreasing hospitalizations and visits to emergency departments, ultimately decreasing costs.” Of the seven benefits that were only part of the top 25% of the focus groups, three were not reported in the reviews: “Make visible, characterize, and prioritize the caregivers and their needs while increasing their confidence by both receiving training and feeling supported in caregiving,” “ Support caregivers and help them to find respite by providing substitutes or helping them with formalities and paperwork,” and “Make people feel represented, looked upon, valued, and part of the compassionate community network” (Table 3).
Comparison of the top 25% most commonly reported outcomes in the focus groups and in the literature review.
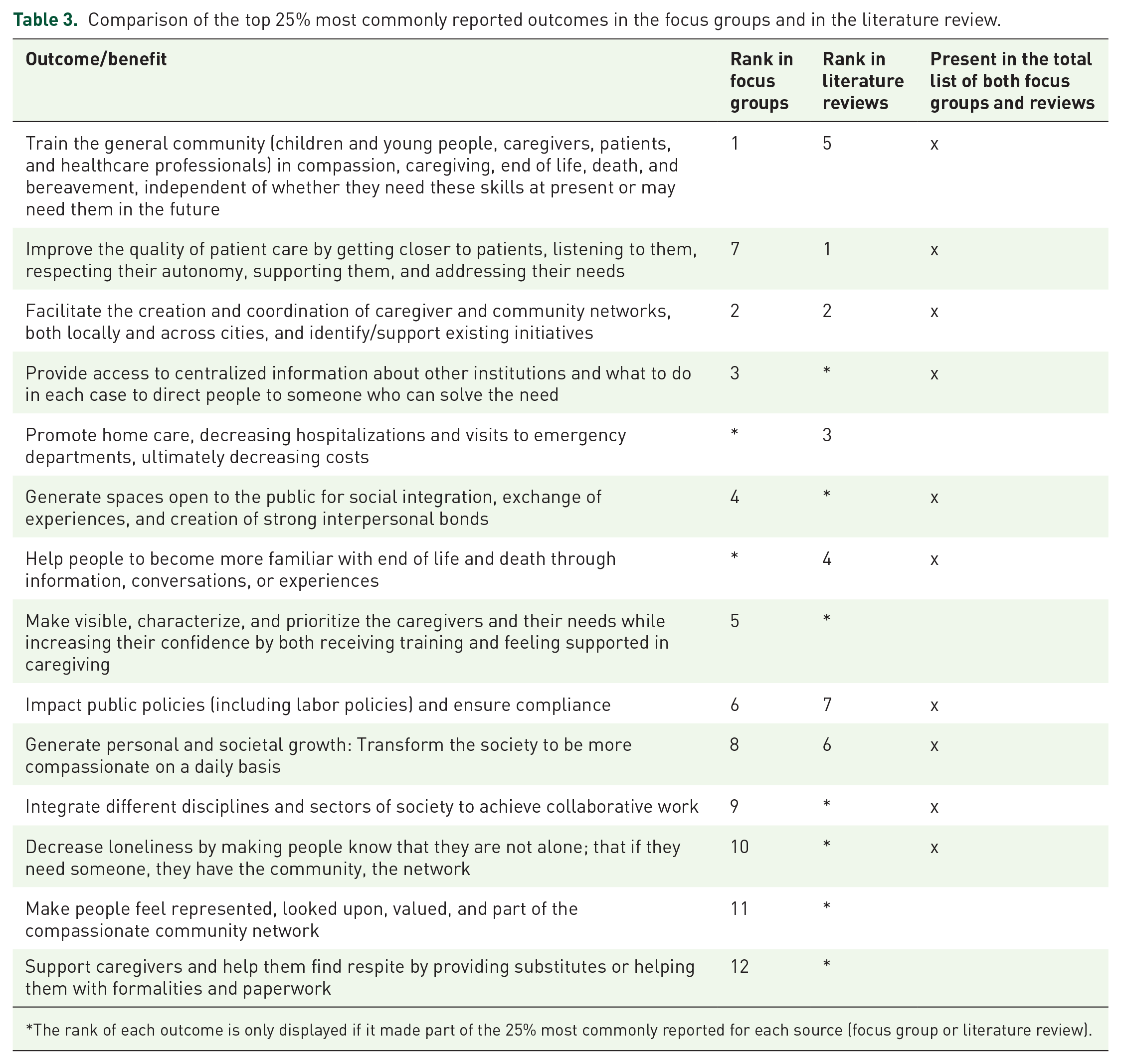
The rank of each outcome is only displayed if it made part of the 25% most commonly reported for each source (focus group or literature review).
Comparison of reported outcomes among cities
Of the 44 benefits that resulted from the focus groups in the three cities, 22 (50%) were present in the three programs, 14 (32%) were present in two of the programs, and the remaining 8 (18%) were present only in one of the programs (Table 4).
Comparison of the top 25% most commonly reported outcomes in the focus groups at each city.

The rank of each outcome is only displayed if it is part of the 25% most commonly reported for each city.
Benefits commonly reported in all three cities related to training the general community in caregiving, death, and bereavement, supporting existing community initiatives and encouraging the creation of new ones, centralizing information about institutions that could help people meet their needs, and transforming society into a more compassionate one. Also commonly reported in the three cities were benefits related to helping people feel that they are valued and cared for by being part of a network and reducing loneliness by being part of a community that will be there if the person needs companionship or help.
Of the benefits that were present only in one city, three were only mentioned in the focus groups conducted in Bern: “Provide people tools to support others regardless of their condition or level of dependency,” “Help to understand when and how to use institutions for the elderly or sick,” “Contribute to current social and demographic challenges.” Two were only mentioned in the focus groups from Buenos Aires: “Raise awareness in issues related to caregiving, illness, death, and dying through art” and “Make hospitals a more welcoming place.” Three were only mentioned in the focus groups from Medellin: “Help to relieve pain,” “Foster research in the field of CC,” and “Enable access to and redistribution of care supplies.”
Ten outcomes were part of the top 25% most commonly reported in Bern, 10 of the top 25% in Buenos Aires, and 11 of the top 25% in Medellin (Table 4). Of all of them, three were present at the top for the three cities: (i)“Train the general community (children and young people, caregivers, patients, and healthcare professionals) in compassion, caregiving, end of life, death, and bereavement, independent of whether they need these skills at present or may need them in the future,” (ii) “Facilitate the creation and coordination of caregiver and community networks, both locally and across cities, and identify/support existing initiatives,” and (iii) “Generate spaces open to the public for social integration, exchange of experiences, and creation of strong interpersonal bonds.”
Discussion
Key findings
We aimed to identify the benefits of CCs from the literature and perspective of key stakeholders from CC programs in three cities. There were outcomes commonly reported both in the three cities and in the literature reviews related to training the general community in compassion and end-of-life topics, facilitating the creation of community networks, and generating public spaces for social integration. While there was considerable overlap between the total list of outcomes/benefits reported in the reviews and those extracted from the focus groups, one of the most reported outcomes in the literature reviews, related to cost reduction, was not even part of the outcomes reported during the focus groups. Benefits commonly reported in the focus groups, especially regarding caregivers and the need to prioritize their needs and support them in caregiving, were not reported in any of the literature reviews. Most of the outcomes mentioned in the focus groups were common for at least two of the three cities with similar priority reflected by the rank position, especially those related to fundamental aspects of the CCs and the objectives described in the charter. 15
Differences between literature reviews and focus groups
Of the outcomes reported in literature reviews, 95% were also mentioned during the focus groups, but only 50% of those in the focus groups had been reported in the scientific articles. This shows the great contribution of conducting fieldwork with the community in developing the lists of the most important benefits to be assessed. Although there are many outcomes in common, it is noteworthy that one of the most commonly reported outcomes in the articles was not present in the focus groups: the one referring to the reduction of costs associated with hospital use. It is probably not surprising that, traditionally, studies have focused on evaluating costs as a strategy to justify to government agencies the creation or continuation of CC programs.
Differences among cities
Although in the coding process, the benefits reported by each participant were pooled and regrouped together for the three cities at the end of the analysis, some benefits were unique to each of the cities, potentially reflecting the idiosyncrasies of each of the contexts and the programs (Figure 1). Those eight benefits that were reported in only one of the three cities can be seen as indicators of the capacity of each health system to cover basic needs. For example, the three benefits that were exclusive for Medellin were “Foster research in the field of Compassionate Communities,” “Enable access to and redistribution of care supplies,” and “Help to relieve pain.” The first one is not surprising because the compassionate community has been actively involved in research since it started in Medellin in 2015. In addition, a very important component of the current program in Medellin is to allow, via a WhatsApp group involving multiple stakeholders, the exchange of healthcare supplies, including access to wheelchairs, diapers, or medicines that are not available to all those in need. Generally, access to them can be gained by people with limited resources after lengthy legal processes to demand them from the public social security system or by people with sufficient socioeconomic resources, either via private complementary health insurance or by covering the costs themselves. Therefore, it is not surprising either that one of the three benefits that were present only in this city was “Enable access to and redistribution of care supplies,” and reflects the role of the compassionate community program in this city. Regarding the outcome “Help to relieve pain,” according to the latest report of the Colombian Observatory of PC, although Medellin occupies the second place with more PC services in the country, this region is classified as one with high needs for palliative care nationally. 16 The atlas reports that 36% of the population who died there, had PC needs and did not receive it. 16 Therefore, the fact that this outcome related to pain was reported in Medellin, may reflect current barriers to accessing medical personnel trained in PC (either generalist or specialist) and therefore trained in the use of pain medications such as opioids. A recently published study that surveyed 806 physicians from Colombia found that 75% of them found barriers to both the availability and accessibility of opioid medications in the country in their medical practice. 17

Outcomes identified across the three Compassionate Communities.
The two outcomes that were unique for Buenos Aires, “Raise awareness in issues related to caregiving, illness, death, and dying through art” and “Make hospitals a more welcoming place,” reflect the activities that were being carried out as part of the local compassionate community as well as the main allies to the program. One of the first activities of the compassionate community in Buenos Aires was to promote the well-being of inpatients and make hospitals a more comfortable environment for them by bringing them a mobile library to enrich their hospital stay. Another form of art is also present in the compassionate community in this city: Community theater groups are one of the main allies of the program, and after hearing of the compassionate community initiative, they decided to contribute by staging plays about illness, death, and grief as a way to increase awareness and normalize these topics through art.
According to the World Bank, Switzerland is in the top five countries with the highest life expectancy in the world. 18 This might explain why the outcomes that were exclusively reported during the focus groups in this city were “Help to understand when and how to use institutions for the elderly or sick” and “Contribute to current social and demographic challenges.” In contrast with Medellin and Buenos Aires, basic healthcare needs, or adequate infrastructure in hospitals seem to be guaranteed, whereas more overarching topics arose, such as navigation through the healthcare/support system and a more societal perspective on how to increase awareness in public for the sensitive topic of end of life in an aging society. Another factor might be the pharmaceutical and medical technology industry within Switzerland and the impression that, in this country, any medicine is available for curing and “preventing from dying.” This might contribute to the perception that being ill and dying is not considered an option because there is a perception that health can be bought.
Feasibility of building a general strategy
Half of the benefits were reported in all three cities despite the differences among them and their CCs programs, and an additional 32% of the benefits were reported by two of the programs; that is, 82% of the benefits were reported in at least two of the cities. Additionally, the majority of the benefits that were part of the top 25% most commonly reported were reported in the three cities (16 out of 19). This is indicative of the possibility of creating a general strategy, at least among these three specific contexts, with the potential of being expanded. However, the outcomes that were reported only in one of the cities and which represent their context and idiosyncrasies reflect the need that, as part of a general evaluation strategy, there is room to evaluate aspects specific to each community according to its peculiarities and context. Taking the example of the cities included in this study, a CC program in a context like Medellin, where most of the population does not have access to all the medical supplies that they should be able to access, but more openly discusses the issues of illness, unmet needs, death, and bereavement, could then focus on helping people access medical supplies. Whereas a CC program in a city like Bern, where most of the population has basic medical needs covered but is less open to talking about illness or death, focusing on raising awareness of death and fostering spaces for dialogues about it, trying to improve the attitude toward the end of life at the population level is justified.
As stated by Vanderstichelen et al., 2 there is an increasing demand for knowledge and expertise on how to develop, implement, and evaluate CCs, but research on outcomes and how to achieve systematic community-level change remains scarce. A recent review identified suitable frameworks to study the development, implementation, and underlying mechanisms of CCs that can be used in combination. 19
Having a tool or a strategy to examine if each CC is bringing the benefits they are supposed to bring and monitor changes accordingly is relevant to improving the outcomes of CCs. Moreover, this strategy has been developed in co-creation by multiple participants of different CCs. In this sense, having a core set of outcomes or benefits would be useful for orienting actions and identifying their effects on the community and society. Away from trying to standardize CCs, such a strategy could be useful for their development, funding, and sustainability. 20
Implications and future research
The ideal assessment strategy would be one in which the health system manages to meet the medical needs of the population and programs or initiatives such as CCs, supported by public policies, further develop awareness of and competencies on how to deal with care, dying, and death as an emerging societal topic.
Future studies focused on the outcomes that are essential to evaluate different CC programs, such as the Delphi study and consensus meeting that will be undertaken as the next steps of our research, 5 need to leave room to integrate benefits that are specific and relevant to each community.
One of the benefits reported in all three cities was to “seek gender equality in caregiving by encouraging that, in families, not only women take the caregiving role.” Moreover, in our focus groups, 83% of the attendees were women, a proportion also present in the co-authorship of this article. Historically, caregiving has been a task assigned to women due to persistent gender roles and stereotypes about “women’s work” and “men’s work.” As reported in the Global Gender Gap Report 2023, most of the paid care work is performed by women. Care work in the health and non-health sectors, as well as work in the education sector, is mainly performed by women. These jobs are often undervalued in today’s economic systems and are characterized by low pay and poor working conditions. 21 Additionally, the majority of unpaid care work is also carried out by women.21,22 A report on the Gender and Unpaid Care Work published by the Swiss Agency for Development and Cooperation (SDC), highlights the importance of recognizing unpaid care work, reducing it by investing in care work, and redistributing it in an equal way between genders. 22 Achieving shared responsibility for unpaid care work requires awareness and changes in gender roles for both women and men. Therefore, when designing or promoting CC programs, it is important to implement strategies to encourage active participation of all genders and to reduce the amount of unpaid care work performed by women. Investing in the care economy is key to achieving gender-inclusive societies and economies. 21
Conclusion
This article shows the importance of conducting fieldwork with the community and including outcomes not only outcomes evaluated in scientific articles but also those directly reported by key stakeholders involved in CC programs. Outcomes related to essential aspects of CC initiatives, such as the development of community networks and training in compassion and end-of-life were reported in the three CCs. While CCs from different contexts have these and other benefits in common, a feasible general assessment strategy must leave room to integrate and evaluate outcomes specific to each context.
Supplemental Material
sj-pdf-1-pcr-10.1177_26323524251314899 – Supplemental material for Assessing and comparing compassionate communities benefits across cities in diverse cultural contexts: a step toward the identification of the most important ones
Supplemental material, sj-pdf-1-pcr-10.1177_26323524251314899 for Assessing and comparing compassionate communities benefits across cities in diverse cultural contexts: a step toward the identification of the most important ones by Valentina González-Jaramillo, Alicia Krikorian, Vilma Tripodoro, Margarita Jorge, Sebastián Orellana, Francy López, Maria Clara Vélez, Tatiana Noguera, Silvina Montilla, Sibylle Felber, Sofía C. Zambrano and Steffen Eychmüller in Palliative Care and Social Practice
Footnotes
Acknowledgements
We would like to thank all the people who participated in the focus groups and shared with us their views on compassionate communities and their benefits. We also thank Laura Tamayo, research assistant, for her contribution to the focus groups in Medellin.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.