
Abstract
Background:
An independent evaluation sought to understand the broader impacts of the West Australian National Partnership Agreement for Comprehensive Palliative Care in Aged Care projects on residents and their families.
Objective:
This study aimed to gain a bereaved carer perspective on palliative care in Western Australian residential aged care homes (RACHs), identify challenges/gaps in care provision, and consider how service delivery can be improved to meet community needs and expectations.
Design:
An online survey of bereaved family carers of people who died in RACHs from 2021 to 2024.
Methods:
The questionnaire was structured according to the six strategic priorities outlined in Western Australia’s End-of-Life and Palliative Care Strategy (2018–2028). Descriptive analyses were conducted.
Results:
Three hundred and seventeen bereaved carers across 46 RACHs responded. 40.6% of carers reported their relative accessed visiting palliative care services during their residential aged care stay, 30.6% did not access, and 28.8% did not know. Overall, bereaved carers whose relatives accessed palliative care reported better experiences for residents and themselves compared with those who did not. However, the respondents called for a more person-centred care system encompassing residents’ needs, more timely information, better communication, and appropriate resources to feel supported before and after bereavement. They also wanted to be more involved in care decisions undertaken within RACH. These needs were reflected in priorities 2 (care is person-centred) and 4 (families and carers are supported), which were rated the lowest among the six priorities.
Conclusion:
This study makes three contributions to ageing policy discourse. First, it provides empirical evidence that despite policy directives towards person-centred care, residential aged care continues operating through institutional “caring for” rather than relational “caring about” frameworks. Second, it reveals implementation gaps in palliative care policies, particularly in bereavement support and family involvement in care decisions. Third, it proposes a compassionate communities approach to care as a social practice and policy framework addressing both quality concerns and sustainability challenges.
Keywords
Introduction
The global population is ageing at scale, with the number of people aged 60 and above projected to nearly double from 12% in 2015 to 22% in 2050. 1 Australia exemplifies these trends, with the number of those aged 65 and over expected to more than double over the next 40 years. Australia also has the highest proportion among 12 high-income nations of older adults living in residential aged care homes (RACHs). It is estimated that over 90% of deaths in these homes could benefit from palliative care (PC) approaches, 2 making palliative care a fundamental requirement rather than an exceptional need in this setting.
Current funding assessments narrowly confine palliative care to the final days of life, under-resourcing the sector and overlooking both non-cancer conditions and bereavement support needs.2,3 These systemic challenges are compounded by the experiences of family carers, who face guilt about placement decisions and struggle with fragmented services,4,5 including poor collaboration between palliative care and RACH services, communication barriers rooted in ageist attitudes, and staff unable to recognise terminal illness phases.6,7 Some families may also face stigma around residential care placement. 5 The quality of palliative care provided directly impacts not only residents but also family carers’ bereavement experiences. 8 Yet, quality palliative care requires effective communication, respect for residents’ preferences through shared decision-making, and care teams that extend beyond clinical staff to include family members and direct care workers.4,9
Addressing these challenges requires comprehensive staff training in recognising the approach of death and implementing person-centred approaches to palliative care.6,10 Recognising these challenges, the Australian Government established the National Partnership Agreement for Comprehensive Palliative Care in Aged Care (NPA CPCiAC), in collaboration with the states and territories, to enhance access to and the quality of palliative care in RACHs. 11
Understanding how policy initiatives address real-world challenges requires examination from multiple stakeholder perspectives, including that of family carers. Family carers provide unique insights into palliative care quality: while specialist teams primarily engage with staff, family carers bear the direct impacts of care decisions through their ongoing involvement and subsequent bereavement experiences. Carers are an important yet understudied group 12 who experience their own support needs as they navigate complex end-of-life (EOL) care decisions for their family members. Their perspective is essential for understanding whether policy initiatives address the fragmented services and communication barriers they face. This study of their responses forms one part of a comprehensive three-part evaluation study commissioned by the Western Australian Department of Health End-of-Life Care Program to assess palliative and EOL care initiatives in RACHs from both family carer and service provider perspectives.
Objectives
This article reports findings from the first phase of the evaluation study that focused on the experiences of bereaved family carers with palliative care in Western Australian RACHs. The specific objectives were to: (i) gain a bereaved carer perspective on palliative care in RACHs, (ii) identify key challenges/gaps in the provision of care, and (iii) consider how service delivery can adapt and improve to meet community needs and expectations.
Methods
Setting
In Australia, RACHs offer permanent or respite accommodation and round-the-clock care for older people who can no longer live independently at home. RACHs provide personal and clinical care, accommodation services including meals and laundry, social activities, and staff assistance with daily tasks such as bathing and medication management. 13 Access to RACH services is facilitated through a government-funded system that requires an assessment to establish eligibility. 14 In Western Australia, 40 principal service providers operate 206 RACHs. Access to palliative care in RACHs is via self or professional referral. Specialised palliative care teams comprising doctors, nurses, social workers, and other clinicians visit RACHs to provide support to residents, families, and staff. However, these visiting teams primarily work with RACH staff rather than directly with families.
Study design
A cross-sectional survey was conducted to collect quantitative metrics and qualitative responses concerning bereaved carers’ experiences and perspectives of palliative care delivery. The survey was based on a 2020 consumer survey framework developed initially to understand broader palliative care perspectives across all settings in Western Australia. 15 The questionnaire from the 2020 survey was adapted for this study through consultation with the 2023 project reference group members to ensure its appropriateness for the bereaved carer population and residential aged care context. The project reference group comprised representatives from major stakeholders, including the Western Australia Department of Health, RACH service providers, clinicians, academics, and leaders from advocacy groups. The questionnaire has gone through two rounds of pilot testing in 2020 and 2023 with a total of 10 bereaved carers from rural and urban areas. The 2020 project reference group established 65% as the threshold for positive service provision (i.e. what is working well), and this threshold was adopted by the 2023 project reference group. This study aimed for a sample size of 400 balancing a low sampling error (5%) and maintaining economic efficiency. 16
The questionnaire was structured according to the six strategic priorities outlined in Western Australia’s End-of-Life and Palliative Care Strategy (2018–2028). 17 It consisted of a set of 44 quality indicators grouped under: Priority one – Care is accessible to everyone, everywhere (9 indicators), Priority two – Care is person-centred (14 indicators), Priority three – Care is coordinated (5 indicators), Priority four – Families and carers are supported (7 indicators), Priority five – All staff are prepared to care (5 indicators), and Priority six – The community is aware and able to care (4 indicators).
Survey questions were organised under subheadings addressing carer and resident demographics, experiences with and quality of care within the RACHs, and formal and informal support provision across three temporal phases: before death, at the time of death, and following death. The questionnaire comprised a maximum of 138 questions, incorporating logical flow structures, of which 28 were open-ended questions designed to capture qualitative insights. These questions aimed to capture carers’ perspectives on care provided to residents and support for themselves.
The project reference group agreed that lay respondents may not understand references to “specialist” or “generalist” palliative care services. Hence, to ensure comprehension, the questionnaire used simpler wording, asking, for example, “Was your relative seen by a ‘visiting palliative care team’ in the residential aged care home?”
Data collection
Data collection took place over 11 weeks, from February to May 2024, via an online survey platform hosted on REDCap and accessible through a dedicated webpage on the Perron Institute’s website, a research institute affiliated with the University of Western Australia, and hosting the current study. Eligibility criteria restricted participation to bereaved carers whose relatives or friends had died in a Western Australian RACH between 2021 and 2024, a period that fits with the NPA CPCiAC projects’ timeframe. The survey was extensively promoted using multiple online and traditional advertising methods, such as paid Facebook advertising, mass email distribution, and third-party promotional activities. Only authorised personnel have access to the REDCap system containing the collected data. Participants who completed the questionnaire are presumed to have given implied consent to participate, a process approved by the University of Western Australia’s Human Research Ethics Committee. The collected data are all self-reported by the respondents.
Analysis
Data analysis was conducted using SPSS (Version 29). Possible duplicate entries were searched by examining four variables: age, gender, location of residence, and the deceased’s death date. No duplicates were found. Descriptive statistics were used to summarise the characteristics of the respondents and deceased residents. They were also used to summarise the quality indicators across the six priority areas. Comparative analyses of quality indicators were conducted across three key variables to examine potential disparities in care experiences. These variables included palliative care service usage, categorised as palliative care users, non-users, or those with uncertain user status; the geographic location of the RACH, distinguished between metropolitan and rural settings; and carer role, differentiated between main and secondary carers. This analytical framework enabled an examination of how these factors influenced the perceptions of bereaved carers regarding care quality and service delivery. Group differences within each of the three variables were tested using chi-square tests. Illustrative quotes, both positive and negative, from the free-text survey responses are purposefully selected (in Boxes) to highlight participants’ voices within each priority, and reveal some nuances not captured in the numerical data. In-depth qualitative analyses will be presented in a forthcoming article.
Results
Missing data
Missing data were minimal, with most responses complete. The highest number of missing responses for any question was eight (for the indicator “contacted by the RACH about 6 months after resident death”), accounting for <3% of the total sample. Given the low level of missing data, each response was analysed using only available data, with missing values omitted. When demographic data were missing, responses to open-ended questions were cross-referenced to fill in gaps, if available (e.g. the resident’s relationship with the respondent). No sensitivity analysis was performed, as the missing data had little impact on the overall results.
Characteristics of bereaved carers
Table 1 presents the characteristics of the 317 bereaved carers from 46 RACHs. These respondents had a median age of 51 years, with 63.1% being female. There was limited cultural diversity, with non-English-speaking participants accounting for 8.2% of responses and Aboriginal and Torres Strait Islander peoples comprising 2.8% of the sample. Nearly half (47.0%) hold university qualifications, and an additional 29.7% hold trade-based credentials.
Bereaved carers’ profile (N = 317).

RACH: residential aged care home.
% may not always add up to 100% because of rounding.
Aboriginal Torres Strait Islanders also indicated they are Australians.
Most carers were in a relationship, with 61.5% identifying as married or partnered. Over half (54.9%) were female family members of the deceased, predominantly daughters or granddaughters. Before RACH placement, 60.9% of carers had provided direct hands-on care for their relative on a daily or intermittent basis, indicating substantial pre-existing involvement in their relative’s care journey, and 29.3% identified themselves as the main carer.
Characteristics of deceased residents
Characteristics of the 317 deceased residents as reported by respondents are shown in Table 2. There were a slight female majority (54.2%) and a median age of 86 years at the time of death. Most residents (83.3%) lived in metropolitan areas, with deaths occurring between January 2021 and May 2024 across 46 different RACHs.
Deceased residents’ profile (N = 317).

RACH: residential aged care home.
% may not always add up to 100% because of rounding.
Indicated categories do not sum to the total sample size of 317, as some respondents selected multiple options. The associate percentage is based on the total sample size.
Clinical presentations included high rates of age-related conditions, with nearly half of residents having a documented dementia diagnosis (45.7%) and a similar proportion experiencing co-occurring frailty due to advanced age (49.2%). About two-thirds (67.5%) of residents were reported to have had at least one visit to the emergency department during the whole length of stay at the RACH, and nearly half (47.3%) had at least one such visit in the last month of life. Residents had spent a median duration of 1.8 years in residential aged care prior to death.
Less than half of carers (40.6%) reported that their relative had accessed visiting palliative care services during their residential aged care stay. 30.6% of carers reported their relative did not receive palliative care services. 28.8% of carers were uncertain about whether such services had been provided or accessed.
Residents’ place of death
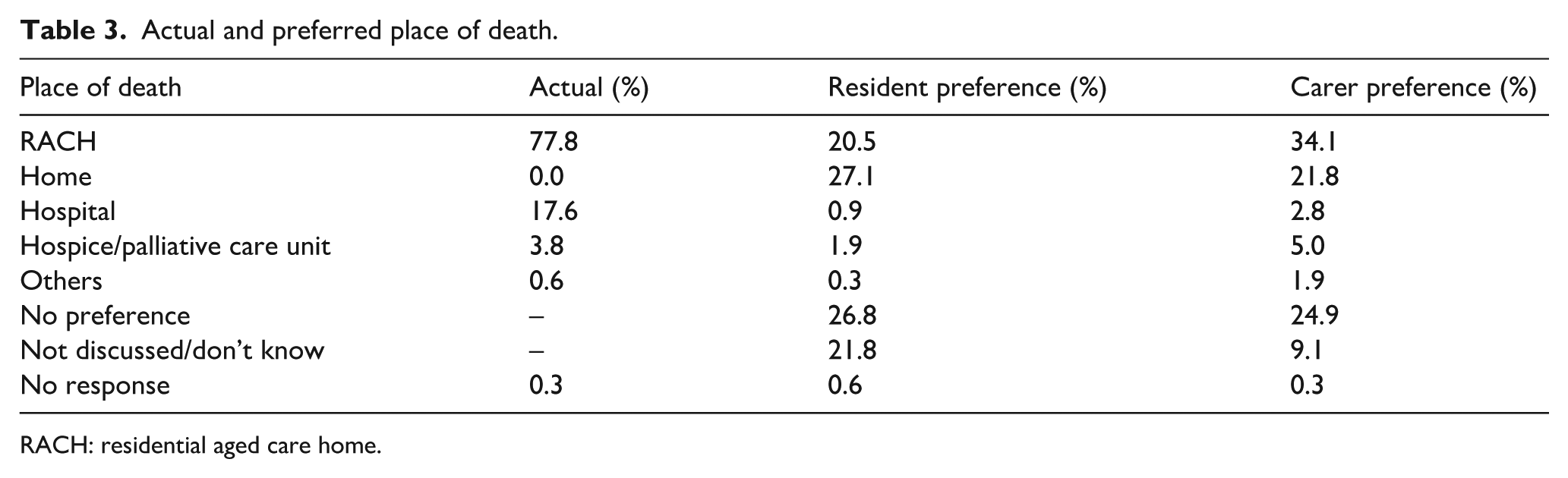
Table 3 contains detailed information about the actual and preferred place of death, as reported by the carers. Most residents (77.8%) died within the RACH setting. Half of the residents have either no documented preference regarding their place of death or no record of such discussions. Only 20.5% of the residents and 34.1% of their carers expressed a preference for dying in the RACH, with about a quarter with no preferences at all.
Actual and preferred place of death.
RACH: residential aged care home.
Overall results of quality indicators across six priorities
Table 4 presents quality indicators across the six priorities. Priority 5 (All staff are prepared to care) was strongly supported, with four of five indicators meeting the performance threshold. For Priority 3 (Care is coordinated), satisfactory performance was achieved in three of five indicators. Priority 1 (Care is accessible to everyone, everywhere) showed moderate performance, with five of nine indicators reaching acceptable levels. Over the total sample, the lowest indicators were in:
Quality indicators across the six priorities.

EOL: end of life; RACH: residential aged care home.
Priority 2 (person-centred care), particularly in the indicators where residents/carers being asked about EOL documentation; carers/residents involved in care decisions at EOL as much as wanted; emotional support provided to the residents; cultural background respected and considered; spiritual/religious beliefs respected and considered.
Priority 4 (Families and carers are supported), especially in the indicators on emotional support to carers; offered information about grief and bereavement services; could stay at RACH overnight; contacted in the weeks or months after resident death; carers spoke to services about their experience of illness/death.
By contrast, Priority 6 had high-quality indicators for informal support by the community and by not-for-profit organisations and for the perceived helpfulness of these informal networks.
Comparison of quality indicators with key variables within each priority
Quality indicators varied according to palliative care service use (PC users, non-PC users, or unsure), geographic location of RACH (metropolitan or rural), and carer’s role (main carer or otherwise). For this study, bereaved carers are classified as “PC users” if they indicated that their relative received care from a visiting PC team at the end of life. There were more secondary carers and more rural respondents in the unsure group: 35% of secondary carers were in the unsure group versus 14% of main carers (p < 0.001); and 43% of rural respondents were in the unsure group versus 26% of metropolitan respondents (p = 0.006). Figure 1 illustrates the compositions of each key variable.

Comparison groups.
Priority 1: Care is accessible to everyone, everywhere
PC users reported higher quality scores across most Priority 1 indicators compared to non-PC users and those unsure about PC service provision (Figure 2). Among the PC users, the overall quality of care (81%) and quality of care at the end of life (77%) were rated the top two. Conversely, the lowest-scoring indicator was receiving adequate support after the resident’s death (47%), followed by receiving sufficient support at the time of death (59%).

Comparison by palliative care user group (Priority 1).
Statistically significant differences across the three groups emerged for the indicator, “carers received as much support as they wanted from RACH” (p = 0.003), with 62% of PC users indicating yes compared to 53% of unsure carers and 39% of non-users. Another statistically significant difference was found for “RACH has provided enough support at the time of death” (p = 0.007). A positive response was indicated by 59% of PC users, compared to 45% of non-PC users and 39% of unsure caregivers. Geographic location and carer role did not demonstrate statistically significant differences in quality indicator performance. Box 1 presents the contrasting experiences of two bereaved carers regarding Priority 1.
Bereaved Carers’ Illustrative Quotes for Priority 1.

Priority 2: Care is person-centred
PC users rated service provision across many Priority 2 indicators more positively compared to non-PC users and those uncertain (Figure 3). Among users, the highest-performing indicators were consideration of documented residents’ wishes (92%) and respect for values (78%). Conversely, the lowest-scoring indicators for PC users were spiritual support provided (52%) and residents being involved in care decisions (57%). Across the total sample, 17% of decisions were made without the carer or resident wanting it, with this proportion being lower among PC users (13%–16%) and higher among non-PC users (21%–22%).

Comparison by palliative care user group (Priority 2).
Six indicators demonstrated statistically significant differences with PC users indicating higher scores: carers able to discuss their worries and concerns with RACH staff (p = 0.014), carers being asked about EOL formal documentation (p < 0.001), carer involvement in EOL care decisions (p = 0.03), respect for resident’s cultural background (p = 0.035), respect for resident’s cultural and religious beliefs (p = 0.021), and spiritual support to residents (p = 0.013).
Geographic disparities emerged in two indicators: metropolitan respondents were more frequently asked about pre-existing EOL documentation than rural respondents (65% vs 51%, p = 0.049), while care decisions that residents would not have wanted were more prevalent in rural settings (25% vs 15%, p = 0.090). Primary carers reported higher rates of being consulted about pre-existing EOL documentation than secondary carers (85% vs 54%, p < 0.001). Box 2 provides some qualitative insights regarding Priority 2.
Bereaved Carers’ Illustrative Quotes for Priority 2.

Priority 3: Care is coordinated
PC users reported high levels of coordination across multiple domains, with 80% or more indicating that coordination worked well or to some extent among palliative care team members and between RACH staff and palliative care teams (Figure 4). Additionally, 87% reported effective collaboration with general practitioners, 67% found emergency department visits helpful, and 72% had planned out-of-hours care arrangements. Non-PC users and those uncertain about PC services reported considerably lower proportions across these indicators, with all differences reaching statistical significance.

Comparison by palliative care user group (Priority 3).
Geographic variations in care coordination were evident between respondents from metropolitan and rural areas. Metropolitan participants reported high coordination levels (over 80%) within palliative care teams and between RACH staff and palliative care teams, compared to rural participants (50%).
Main carers reported marginally higher rates of planned out-of-hours care than secondary carers (67% vs 56%), with the difference approaching statistical significance (p = 0.056). Box 3 highlights some feedback from bereaved carers regarding Priority 3.
Bereaved Carers’ Illustrative Quotes for Priority 3.
Priority 4: Families and carers are supported
Priority 4 was least endorsed by the carers across all priorities, with low-quality scores for family and carer support indicators (Figure 5). Support after a resident’s death was the lowest-scoring indicator, with PC users indicating only 20%–30% quality scores, scoring higher than non-PC users and those uncertain about service provision. Three indicators demonstrated statistically significant differences between groups, with PC users indicating higher scores: information provided to carers about the resident’s condition (p = 0.037), allowing carers to stay overnight (p < 0.001), and carers being offered information about grief and bereavement services (p < 0.001). Box 4 quotes reflect some of the carers’ experiences within Priority 4.
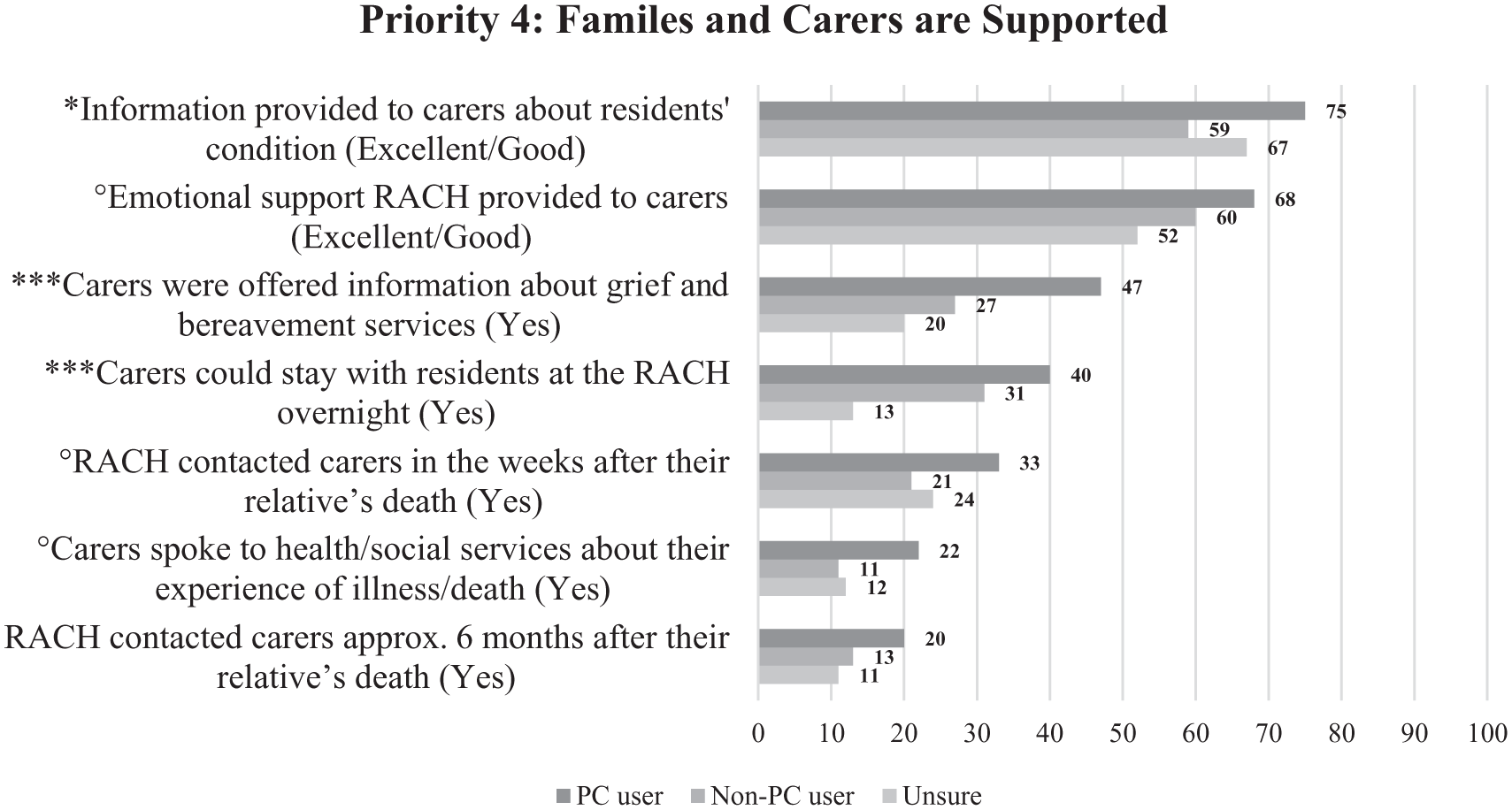
Comparison by palliative care user group (Priority 4).
Bereaved Carers’ Illustrative Quotes for Priority 4.

Priority 5: All staff are prepared to care
Priority 5 has some of the highest quality indicators, with PC users and those uncertain about service provision reporting scores in the high 80% range for being treated with respect and dignity, receiving compassionate and kind care, and staff competence (Figure 6). The non-PC user group reported lower ratings of staff competence than the other two groups (p = 0.025). PC users reported higher scores for receiving information when requested (p = 0.027). Geographical location and carer’s role did not show notable differences in Priority 5 indicators. Box 5 quotes articulate some carers’ experiences as related to Priority 5.
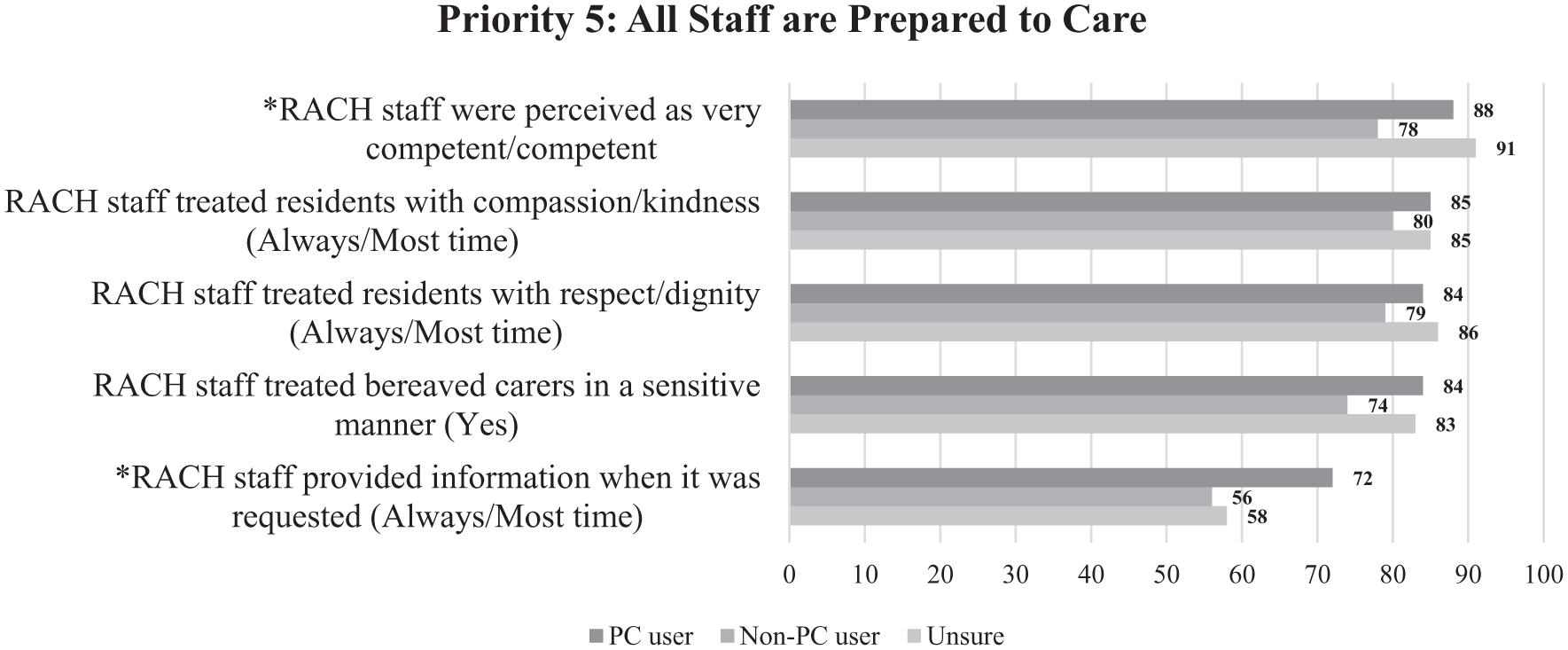
Comparison by palliative care user group (Priority 5).
Bereaved Carers’ Illustrative Quotes for Priority 5.

Priority 6: The community is aware and able to care
Informal support, encompassing assistance from family, friends, and not-for-profit organisations, received quality indicator scores in the high 80% range for both helpfulness before and after death (Figure 7). PC users reported receiving more informal support before death compared to non-PC users and those uncertain about service provision (p = 0.029). No differences were observed in regional distribution or carer status for Priority 6 indicators. Carers offered their qualitative insights regarding Priority 6 in Box 6.
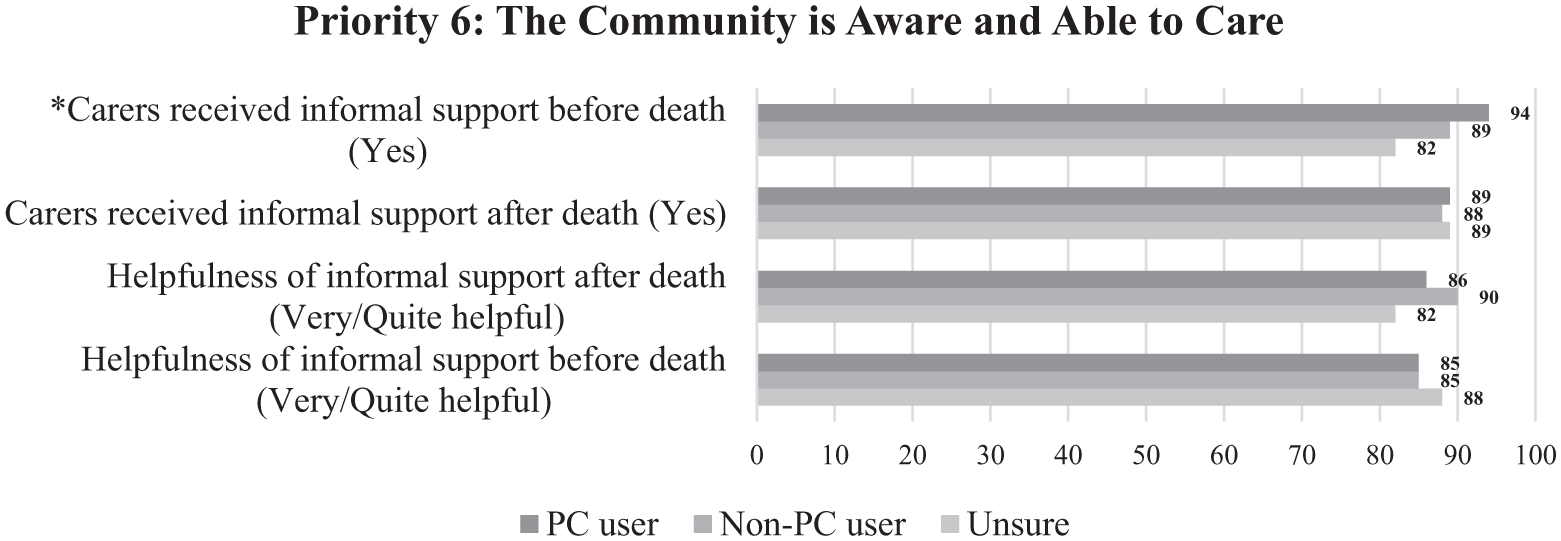
Comparison by palliative care user group (Priority 6).
Bereaved Carers’ Illustrative Quotes for Priority 6.

Discussion
This study has shown how “care” has been operationalised through quality indicators that are grounded in the six strategic priorities. The feedback reveals that while palliative care services generally improved bereaved carers’ and residents’ experiences across most aspects of care, significant gaps existed in support before and after bereavement (Priorities 2 and 4). In contrast, the carers rated informal support from social networks and not-for-profit organisations positively (Priority 6), highlighting the potential for community-integrated care models.
Essentially, the carers wanted a person-centred care system that addressed residents’ physical, psychosocial, and spiritual needs and also their own. While they had, of necessity, delegated their residents’ everyday care to the RACH, family carers still required more timely information, better communication, and appropriate resources to feel supported before and after bereavement. They needed to continue to be involved in care decisions undertaken within the RACHs. These findings align with systematic review evidence showing that family caregivers of RACH residents experience complex grief, loss, and bereavement needs throughout the resident’s journey, from admission through death and beyond. 18 Quality of communication and involvement in care decisions have been consistently identified as critical factors influencing bereavement outcomes.
The poor results in Priorities 2 and 4 suggest a need to move beyond approaches to care that prioritise tasks – caring for residents – towards relational approaches that care about them as individuals with unique needs, relationships, and social contributions. While it is possible, however, to juxtapose “caring for” and “caring about” approaches, the goal is to integrate caring tasks within relational approaches in a strategy that the Western Australian Residential Aged Care Guideline calls “holistic person-centred care.” 19
The persistence of institutional “caring for” culture
While aged care policy in Western Australia and, more widely Australia, calls for person-centred, rights-based approaches to care, 19 we find here that only 21% of Priority 2 indicators met the 65% threshold, suggesting that aged care culture remains predominantly focused on caring for residents through task-oriented protocols more than caring about them as individuals. The contrast between high-performing indicators, such as consideration of documented residents’ wishes (92% among palliative care users), and areas with lower ratings, like spiritual support (52%) and resident involvement in care decisions (57%), suggesting the limitations of institutional approaches that focus on documented procedures and seems to struggle to engage meaningfully with residents’ lived experiences and evolving needs. Research on palliative care in long-term care facilities has similarly documented this tension between task-oriented compliance and relational care provision. 20
This pattern of higher ratings in procedural areas compared to relational engagement reflects a fundamental issue with current aged care systems, which remain structured around task completion and administrative compliance more than facilitating meaningful connections between residents and their communities.20,21 It should, of course, be acknowledged that recent developments in aged care policy seek to preserve the autonomy and agency of residents and their social networks. Our findings suggest that implementing person-centred policy in RACHs, which under previous aged care policies have been structured around functional compliance with caring tasks, requires new strategies to facilitate caring about residents as individuals within their broader relational and community contexts. That is, recent policy changes may remain aspirational without significant changes to the way care services are structured, particularly the care pathways that progressively disrupt aged people’s social networks as their care needs increase, and they become the recipients of professional services and, for some, residents in professionalised institutional contexts.
Reframing the important role of formal care services
This structural critique does not diminish the vital role that formal aged care services can and must play in supporting older adults with complex health needs and declining functional capacity. Instead, it highlights how these services might be reconceptualised as facilitators of social connection rather than inadvertent barriers to it. Professional care providers possess specialised clinical expertise and resources that informal networks cannot replicate, yet these same services could be structured to strengthen rather than fragment the relational contexts. The challenge lies in developing care pathways that preserve clinical competence while embedding professional services within frameworks that prioritise relational continuity, thereby positioning formal care as a bridge between residents and their communities rather than as a replacement for these essential connections.
Bereavement care as an indicator of relational care
Priority 4 results reveal the most significant area requiring attention, with only 14% of indicators meeting the threshold. The particularly low ratings in post-death support, where even palliative care users achieved only 20%–30% quality scores, seem to indicate significant gaps between the way RACHs see their responsibility to bereaved carers and the expectations or needs of those carers.
The low rates of follow-up contact (27%) in the weeks following death and 15% at approximately 6 months reflect “caring for” logic that views responsibility as ending when the care recipient dies. Bereaved carers in other studies reported their need to discuss their loss with empathetic service providers who have known the resident, a need that may not be met.22,23 This gap could have been created by institutional policies that separate care work from relationship work, placing bereavement outside the scope of residential care, as the lack of any relevant policy confirms. Ideally, as in palliative care, the focus of residential care would be on the resident and their family (and/or social network) as recipients of care, allowing care for families to extend into bereavement. 24 There are, of course, obvious practical barriers, including funding, to extending RACHs’ scope of practice to include bereavement care, let alone the fact that the most effective bereavement care is provided by community networks, not professional services. In light of these findings, it seems important that residential care offer some initial bereavement support whilst recognising that any service-provided bereavement care should collaborate with broader care systems that encompass both formal services outside of RACHs and sources of informal support.25,26
Towards sustainable models of care
The higher ratings in Priority 6 (Community Awareness and Ability to Care) provide a basis for why current aged care models should incorporate community-based “caring about” approaches. With 89% of carers receiving community support and 86% finding it helpful, these results demonstrate that community-based models naturally embody a caring approach to residents and carers by maintaining their connections to broader social networks and relationships. The contrast between these strong community ratings and weaker institutional support for carers underscores the benefits of community-integrated approaches.
Formal services that “care for” residents are essential. However, continued expansion of such services is not sustainable in terms of cost or capacity, given that ageing at scale will keep escalating and resources are limited. The strong community performance here suggests that shifting the focus of aged care towards both caring for and about ageing people and their carers through community integration represents both a quality improvement and a strategy for sustainability. This shift is underpinned by the new Aged Care Act 2024, which takes effect from 1 November 2025. However, as noted above, the policy directives do not seem to account for the cultural shift required of current services to reconceptualise care. 27 Critically, the Inspector-General of Aged Care’s 2025 progress report 28 on the Australian aged care system identifies a significant gap between the Act’s holistic vision and its funding implementation. Government funding mechanisms mainly support clinical care, neglecting the social, emotional, and spiritual dimensions that older people prioritise, which this study identifies as crucial but are either underfunded or require co-payments.
The public health palliative care approach provides a framework for the required reconceptualisation. This approach integrates healthcare, community, and civic efforts to enhance quality of life by recognising that caring about someone means addressing their social, emotional, and relational needs alongside clinical requirements. 29 It bridges institutional boundaries by emphasising relationships, community support, and recognition of dying, caregiving, and grieving as shared community experiences rather than isolated institutional events. 30
A central strategy of a public health approach to palliative and EOL care (model outlined in Aoun et al-ref 15) is compassionate communities, community structures that reduce suffering while empowering community members to provide ongoing support. 31 This strategy recognises that truly caring about someone means understanding them in the full context of their relationships and community connections, forming the new essentials of palliative care. 32
In Western Australia, the Compassionate Connectors Program demonstrated compassionate communities as a successful public health palliative care initiative. This volunteer-led program enhanced social networks for families living with chronic or life-limiting illnesses, demonstrating significant improvements in social connectedness while reducing burden and pressure.33,34 An economic analysis showed that investing in this approach to care reduced hospital admissions and presentations at emergency departments and, as a consequence, reduced health sector expenditure while improving outcomes. 35 This Program seems particularly relevant in aged care, considering the residents’ emergency department presentations in this study, where about two-thirds had at least one presentation during their entire stay (median of 1.8 years), and about half had at least one presentation during the last month of their life (Table 2). The Program’s success in reducing hospital admissions and improving social connectedness among community-dwelling older adults suggests strong potential for adaptation within RACHs, offering a strategy to address both the sustainability challenges of ageing populations, and the quality concerns identified in this study.
Recognition of this potential is growing in the aged care sector itself, with Bupa Aged Care Australia 36 formally incorporating a compassionate communities approach to care as a pillar in its palliative and EOL care framework, committing to social network mapping, training compassionate connectors, and building death literacy in their aged care homes. This sector-led adoption demonstrates acknowledgement that addressing the relational gaps identified here requires systematic integration of community-based approaches alongside traditional clinical care.
While these developments demonstrate increasing recognition of the potential of compassionate communities, successful implementation requires careful navigation of tensions and pitfalls. Recent reviews suggest that most compassionate communities initiatives remain mainly service-driven, 37 risking positioning communities as recipients rather than as drivers of change. 38 Success depends on clearly defined, complementary roles: healthcare professionals manage complex medical and social issues, while communities provide social support, a sense of belonging, and meaning that clinical care alone cannot provide.36–38 Community members must be involved at all stages of design and implementation, as no single approach benefits all communities. 39 Therefore, translating this potential into residential aged care requires a sustained commitment to genuine community empowerment beyond mere policy adoption.
Strengths and limitations
This study offers several strengths. It utilises a comprehensive assessment framework that incorporates 44 quality indicators, aligned with Western Australia’s End-of-Life and Palliative Care Strategy. The inclusion of diverse carer relationships and geographic representation across metropolitan and regional areas enhances the validity of findings within the Western Australian context. The study captures the care experiences of residents who died between 2021 and 2024, providing relevant baseline data for future follow-up to assess any improvements during the implementation period of the strategy.
The convenience sample may not be representative of the general RACH population because of the sampling framework, where we could only rely on social media and several carer and service provider networks to recruit bereaved carers. The high proportion of secondary caregivers (69.7%) likely reflects the nature of family involvement in residential aged care, where adult children and grandchildren often remain actively engaged in care decisions and facility interactions, especially when the spouse/partner of the resident, considered the main carer, is also ageing and needs family support. The online survey format may have also been more accessible to younger family members with greater digital literacy.
Despite using various recruitment methods, including social media and service provider networks, 317 bereaved family carers responded within the limited data collection period. This sample size is similar to that obtained in a previous similar study 15 and remains adequate for examining the family carer perspective. Among other strengths, there were important similarities between this study sample and the general RACH population, including age distribution of residents, 59% versus 58% for those aged 85 years and over, 40 proportions of residents living with dementia, 46% versus 54%, 41 proportion of rural residents,16% versus 15%, 42 proportion of residents dying in RACHs, 78% versus 79%, 43 and median length of stay in RACHs, 1.8 years versus 1.7 years. 44 These similarities strengthen the validity of carer feedback and support the study’s conclusions and recommendations.
This study’s cross-sectional design does not capture changes over time or causal relationships between interventions and outcomes. The retrospective nature of carer reporting may be influenced by grief processes and the time elapsed since death, potentially affecting the accuracy of recalled experiences. Carers who were unsure about palliative care provision may not have been aware of interventions delivered to residents by visiting palliative care teams through RACH staff. While nearly 3% of the sample respondents are from an Aboriginal and Torres Strait Islander background, which aligns with their population distribution in Western Australia, different methodologies that capture their experiences are more suitable. The sample’s limited cultural diversity, in terms of 8% being from non-English-speaking backgrounds, limits the generalizability of the findings to Australia’s multicultural population and may not capture structural barriers affecting these groups. Further studies specific to these marginalised groups are needed. Similarly, future surveys should specifically target rural and remote areas, especially since 43% of rural respondents did not know whether they received palliative care.
Conclusion
This survey provides baseline data for evaluating Western Australia’s End-of-Life and Palliative Care Strategy (2018–2028) while highlighting a key tension in residential aged care: the gap between policy goals for person-centred care and the reality of task-focused institutional practices. Although palliative care services have improved many aspects of care, notable gaps in relational support, including communication, emotional and spiritual care, carer involvement in decisions, and grief support before and after bereavement, suggest limitations of models that focus on caring for residents and carers rather than caring about them within their community relationships. The contrast between strong informal community support and weak institutional relational care points towards a solution in terms of a cultural shift and system change: Integrating compassionate communities principles into formal aged care systems.
As Australia’s Aged Care Act 2024 takes effect, current services need this cultural shift to reconceptualise care: Transforming residential services from isolated providers into facilitators of community connections and networks becomes both a quality necessity and a sustainability strategy for an ageing population, aiming to ameliorate the loneliness, learned helplessness, lack of self-agency, and internalised ageism of residents. Key areas for implementation research include evaluating community-integrated care models in residential settings, through networks of care, and examining barriers faced by culturally diverse and rural populations to ensure equitable access to relational, person-centred, and network-centred EOL care.
Footnotes
Acknowledgements
The research team would like to thank the contribution of the Project Reference Group members and the organisations and individuals who actively promoted the consumer survey. Thanks to Denise Howting and Natasha Bear for advising on the statistical analyses. Special thanks to the bereaved carers who enriched this project with their experiences and insights for improving palliative care and aged care services in Western Australia.
Ethical considerations
Ethical approval was obtained from The University of Western Australia’s Human Research Ethics Committee (ethics approval number 2023/ET000833).
Consent to participate
Completion of the questionnaire implied consent, which is permissible as per the approved ethical review application at the time.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This evaluation was jointly funded by the Australian Government and End-of-Life Care Program, Western Australian Department of Health.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Ethical approval precludes the data from being used for another purpose or being provided to researchers who have not signed the appropriate confidentiality agreement. Specifically, the ethical approval specifies that all results are in aggregate form to maintain confidentiality and privacy and precludes individual-level data from being made publicly available. All aggregate data for this study are freely available and included in the article. Interested and qualified researchers may send requests for additional data to Samar Aoun at samar.aoun@perron.uwa.edu.au.