
Abstract
Background:
Studies have highlighted a perceived lack of information concerning end-of-life (EoL) decisions and discrepancies in communication between physicians and cancer patients, despite the fact that sharing these dimensions remains central to the therapeutic process.
Objective:
We aimed to investigate healthcare professionals’ disclosure of information on EoL, considering the perspectives of professionals and patients and relatives, and the professional factors that may affect communication.
Design:
The descriptive, mono-centric study E.L.D.Y.-CA.RE. (End of Life Decisions study – CAregivers RElatives) was conducted in 2018 at the Veneto Institute of Oncology in Padua, Italy.
Methods:
Three different questionnaires were created for professionals, patients, and caregivers to investigate EoL decisions, opinions, psychological reactions, and quality of communication. Descriptive analysis and logistic regression were carried out, in order to corroborate the data.
Results:
A total of 425 questionnaires were completed by 136 healthcare professionals, 171 patients, and 118 relatives. Some subjects were frequently discussed: diagnosis and purpose of medical treatment (89%) or possible complications (92%); less frequently discussed subjects were life expectancy (22%), existential and spiritual dimensions (11%), withholding/withdrawing life-sustaining treatment (11%), and the option of hastening death (3%). Discrepancies emerged especially regarding palliative options, care delivery problems, emotional/psychological, and social problems. Up to 55% of patients did not answer questions because they believed they were not relevant to their health and a consistent proportion of professionals still felt inadequate in communicating bad news and in confronting with terminally ill patients. As emerged from logistic regression models, role, gender, age, and previous training of healthcare professionals, as well as strength of their own and the patients’ beliefs, significantly influenced the subjects discussed.
Conclusion:
The perceptions of EoL communication in physician–patient and physician–relative relationships reveal ongoing problems in terms of sensitive and psychological issues, which are often experienced differently. At the same time, the management of terminally ill patients has an emotional impact on medical professionals and affects how they view death. Increased attention to palliative care and training in both communication and bioethics may help to improve professional communication skills and make healthcare professionals better prepared to manage the final stages of a patient’s life and personal reactions to death.
Keywords
Introduction
In recent years, international studies have highlighted how good, empathic communication is an essential factor in the relationship between healthcare professionals and cancer patients.1–3 There is certainly a greater tendency towards communication than last century, 4 and it remains a fundamental element of therapy that also conditions patients’ decisions. The Italian Law 219, introduced in 2017, defines correct involvement modalities of the patient in clinical decisions and medical relationship, from his informed consent through the advance treatment directives till shared care planning. In this sense, the Law reminds us that the time for communication must be considered as a ‘time of care’, in order to develop a good therapeutic relationship that includes knowledgeable informed consent from patients and their relatives, with real sharing of therapy decisions and adequate formulation, with the patient, of a shared care plan.5,6 Indeed, research shows that improved healthcare communication has been associated with improvements in patient satisfaction, adherence to treatment, and also physician well-being and job satisfaction.1,7 The healthcare professional’s ability to understand and to communicate patient emotions is seen by patients as an essential part of a meaningful therapeutic relationship, leading to a better understanding of their cognitive and affective states. 8 At the same time, shared decision-making and early communication with cancer patients and their relatives appears to be important for the quality of their end-of-life (EoL) experience, with a positive impact on their psychosocial well-being and relationship with healthcare professionals.3,9 Furthermore, the involvement of family members in the communication process helps them to accept and better understand the treatments and decisions made by both physicians and patients, leading to a better self-assessment of the relatives’ health.10,11 Healthcare professionals who initiate clear communication about treatments and their consequences are also able to engage patients in appropriate advance care planning, understand and reflect their preferences and needs, and achieve higher levels of patient satisfaction with care and lower rates of depression and anxiety among relatives. 12 All these findings show that the outcomes of global care also depend on the healthcare process experienced by the patient, which includes communication and emotional support from healthcare professionals.
Despite this evidence, open communication with patients and their relatives remains a critical issue in the oncological context, especially in EoL areas, in which healthcare professionals report feeling inadequately trained, uncertain, and worried about the impact of these subjects on the patient.11–14 Furthermore, where communication does occur, it appears to be predominantly focused on diagnosis, while prognosis, EoL options, and, in particular, social, existential, and spiritual issues seem to be less frequently discussed.15,16 This could be due to a more culturally rooted paternalistic view, most often found in southern European and Asian countries, by which the prognosis and sometimes the diagnosis are not communicated directly to patients in order to ‘protect’ them from emotional distress and with the mistaken belief of preserving hope.4,17,18
Differences in patient preferences also emerged between countries, particularly when considering Italy. 18 Although most patients choose to know the truth during the clinical pathway, a distinction still remains between those who prioritize its comprehensiveness and those who point out how the communication process must be adapted to the needs of the patient. Among the demographic variables considered, Bongelli et al. 19 emphasized how age seems to influence patients’ preferences the most. Indeed, in their mixed-method study, younger patients strongly reject the concealment of the truth, as a reaction against protective and paternalistic behaviour, but it could also reflect the fact that the fear of knowing may increase with age, or it could be an intergenerational change in ways of accessing information. The qualitative analysis they conducted revealed three main sources of problems in physician–patient encounters: the shortage of time, the absence of empathy, and the use of unintelligible language that makes it difficult for patients to take a more active role.
Difficulties in communicating with patients may also be related to an inability to cope with the negative consequences of empathy. This could be particularly true for healthcare professionals working in oncology settings, where they are required to empathize with users experiencing negative emotions and distress, increasing their stress related to compassion fatigue and emotional exhaustion.20,21 At the same time, the organizations themselves play an important role in facilitating doctor–patient communication and should actively contribute in providing healthcare professionals with the necessary training and structural resources to implement an effective, patient-centred communication. 22
The aim of the present study, implemented after the recent Law 219/2017, is to investigate healthcare professionals’ communication on EoL subjects, taking into account the perspectives of professionals, patients, and relatives. We also investigated the emotional experiences reported by healthcare professionals working in an oncological setting and their opinions about the main aspects of EoL care. In particular, we explored the relationship between certain characteristics of the professionals and the subjects they discussed with patients and relatives, as well as the opinions and reactions they reported in facing terminal illness and managing care.
Methods
Materials
A cross-sectional, mono-centric study was conducted between June and September 2018 at the Veneto Institute of Oncology (IOV), a comprehensive cancer centre in Padova, Italy. The study, called E.L.D.Y.-CA.RE. (End of Life Decisions study – CAregivers RElatives), resumed the E.L.D.Y. questionnaire,13,23 which was aimed exclusively at healthcare professionals and based on an Italian and multidisciplinary reworking of the EURELD 24 and ITAELD 25 studies. In the current study, the questionnaire was extended and three different versions were proposed for professionals, patients, and caregivers, respectively. People were invited to participate in the survey through direct contact within the oncological setting, and total confidentiality was guaranteed.
The healthcare professional questionnaire consisted of three parts, with a total of 80 items:
- the first part, addressed only to physicians and nurses, investigated the EoL decisions (ELDs) they had made in their recent experience of caring for cancer patients at the EoL;
- the second part, extended to all professionals involved in the patient’s care, explored opinions, attitudes, and psychological reactions in relation to the EoL, as well as communication they had with patients and their relatives;
- finally, the third part of the questionnaire, addressed to all professionals, investigated some personal characteristics of the respondents and their previous training in bioethics and palliative care.
In the second part of the questionnaire, we investigated the communication which occurred between clinicians and patient and/or their relatives, with a specific focus also on topics regarding ELDs: in particular, we asked about communication related to options of withholding/withdrawing treatments and ‘options of hastening death’ (e.g. euthanasia or assisted suicide, not allowed in the Italian legislative order).
The questionnaires adapted for patients and caregivers consisted of 40 and 41 items respectively and were also divided into three parts:
- the first part explored patients’ and caregivers’ opinions and beliefs about ELDs that they held prior to the patient’s admission to the institute;
- the second part aimed to explore their beliefs and opinions about ELDs during the care process within the institute and the content and quality of the communication they had with healthcare professionals;
- the third part collected some general characteristics of the respondents.
The study was approved by the Research Ethics Board of the IOV and patients provided written informed consent to participate.
Participants
Invitation to participate in the study was addressed to healthcare professionals who were not at the same time family members or caregivers of a patient recovering in the IOV. Patients were included according to the following criteria: possession of full legal and cognitive capacity; willingness to participate in the research; no diagnosed psychiatric pathologies. For family members and/or caregivers, the following criteria were adopted: presence of a continuous and significant care relationship with the patient for at least 1 year; presence near the bed during hospitalization; possession of full cognitive capacity; and willingness to participate in the survey.
Statistical analysis
Descriptive analyses were used to explore the distribution of communication-related questions in relation to questions in the healthcare professionals’ questionnaire on ‘discussion with the competent patient’ and ‘discussion with relatives without informing the patient’. In the present article, given the different professional roles and responsibilities regarding the discussion of clinical decisions, we have reported the responses of physicians and nurses only concerning the subjects discussed in the context of communication with users. It is important to note that the response options for items exploring communication differed slightly between the three questionnaires: in the healthcare professionals’ questionnaire, the options were ‘Yes, always’, ‘Yes, only when asked’, and ‘No’. While in the patients’ and relatives’ questionnaires, they were ‘Yes, always’, ‘Yes, only when asked’, ‘No and it’s okay’, and ‘No, but I wanted to talk about it’. Patients and relatives also had the option of answering ‘Question not relevant to my condition’, if they felt the question was not appropriate for the clinical condition the patient was in at the time the questionnaire was administered. We followed this breakdown when reporting data in text and figures.
Comparisons were made using Chi-squared test or Fisher’s exact test: gender (male vs female), age (<50 years vs ⩾50 years), training in palliative care (yes vs no), training in bioethics (yes vs no), importance of own religious and philosophical principles (very important/important vs unimportant/not important at all), and importance of patient’s religious and philosophical principles (very important/important vs unimportant/not important at all).
For the purposes of the logistic models, responses to the communication-related questions were dichotomized by combining ‘Yes, only on request’ with ‘No’. Univariate logistic regression models were performed to test the association between the responses to the communication-related questions and the exploratory variables.
Analyses were performed using R software, version 4.3.3. The significance level was set at 5%.
Results
A total of 1,595 questionnaires were distributed, and 425 questionnaires (27%) were completed: 136 healthcare professionals, 171 patients, and 118 caregivers. The main characteristics of the respondents are presented in Table 1. Specifically, among the professionals who responded to the questionnaire, 38 (28%) were physicians (28 oncologists, 4 surgeons, 3 radiotherapists, 1 anaesthetist, 2 other professions), 56 (41%) were nurses, 7 (5%) were psychologists, 16 (12%) were healthcare workers, and 19 (14%) were workers from different professions.
Characteristics of the professionals’ and patients/relatives’ samples: rounded percentages.
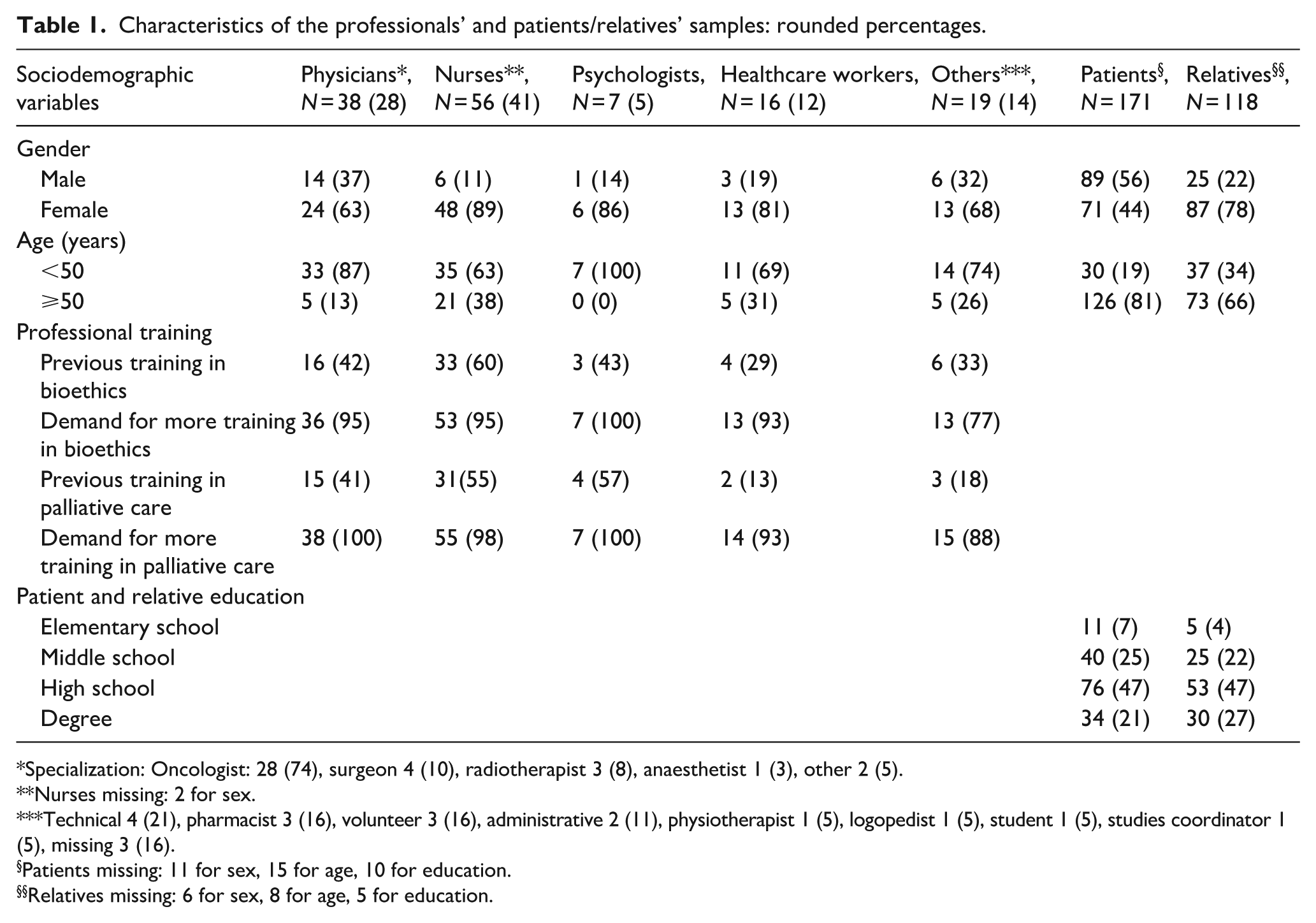
Specialization: Oncologist: 28 (74), surgeon 4 (10), radiotherapist 3 (8), anaesthetist 1 (3), other 2 (5).
Nurses missing: 2 for sex.
Technical 4 (21), pharmacist 3 (16), volunteer 3 (16), administrative 2 (11), physiotherapist 1 (5), logopedist 1 (5), student 1 (5), studies coordinator 1 (5), missing 3 (16).
Patients missing: 11 for sex, 15 for age, 10 for education.
Relatives missing: 6 for sex, 8 for age, 5 for education.
Communication between healthcare professionals, patients, and relatives
When analysing the clinical topics that emerged in the communication, special attention should be paid to the significant proportion of patients and relatives who did not answer questions by indicating that some issues were ‘not relevant to their condition’ (Figure 1). The patients always stated that the questions were not relevant to their condition more than their relatives. Even for some basic questions such as diagnosis, medical treatment, and possible complications, between 8% and 14% of users felt that it was not relevant to answer due to their condition. For some questions, the difference in answers between patients and relatives was important, such as incurability of the disease (reported by 35% of patients and 24% of relatives), social problems (42% of patients and 34% of relatives), life expectancy (29% of patients and 23% of relatives), and care delivery problems (42% of patients and 22% of relatives). For some questions, the proportion of users who considered the question not relevant rose to half or more of the sample considered, such as palliative care (for 52% of patients and 44% of relatives), withholding/withdrawing life-sustaining treatment (for 55% of patients and 48% of relatives), or options to hasten death (for 62% of patients and 58% of relatives).

Percentages of patients and relatives in which questions were considered ‘not relevant to their condition’.
In comparing the answers given by healthcare professionals and patients/relatives, keeping only those who had responded because they considered the questions relevant to their clinical condition, it was noticeable (Figures 2 and 3) that 89% of physicians, 94%–95% of patients, and 90%–87% of relatives reported that the diagnosis and purpose of medical treatment were discussed with the patient ‘yes, from the beginning’. Overall, healthcare professionals reported that they had discussed medical diagnosis and treatment with the patient from the beginning or at the patient’s request in 87%–100% of cases. On the other hand, it is interesting to note that they reported having discussed the diagnosis and purpose of treatment from the beginning with relatives only in 27% and 46% of cases respectively and, overall, in 57% and 67% of cases.

Percentages of topics of communication between MD and PT and between MD and RE.
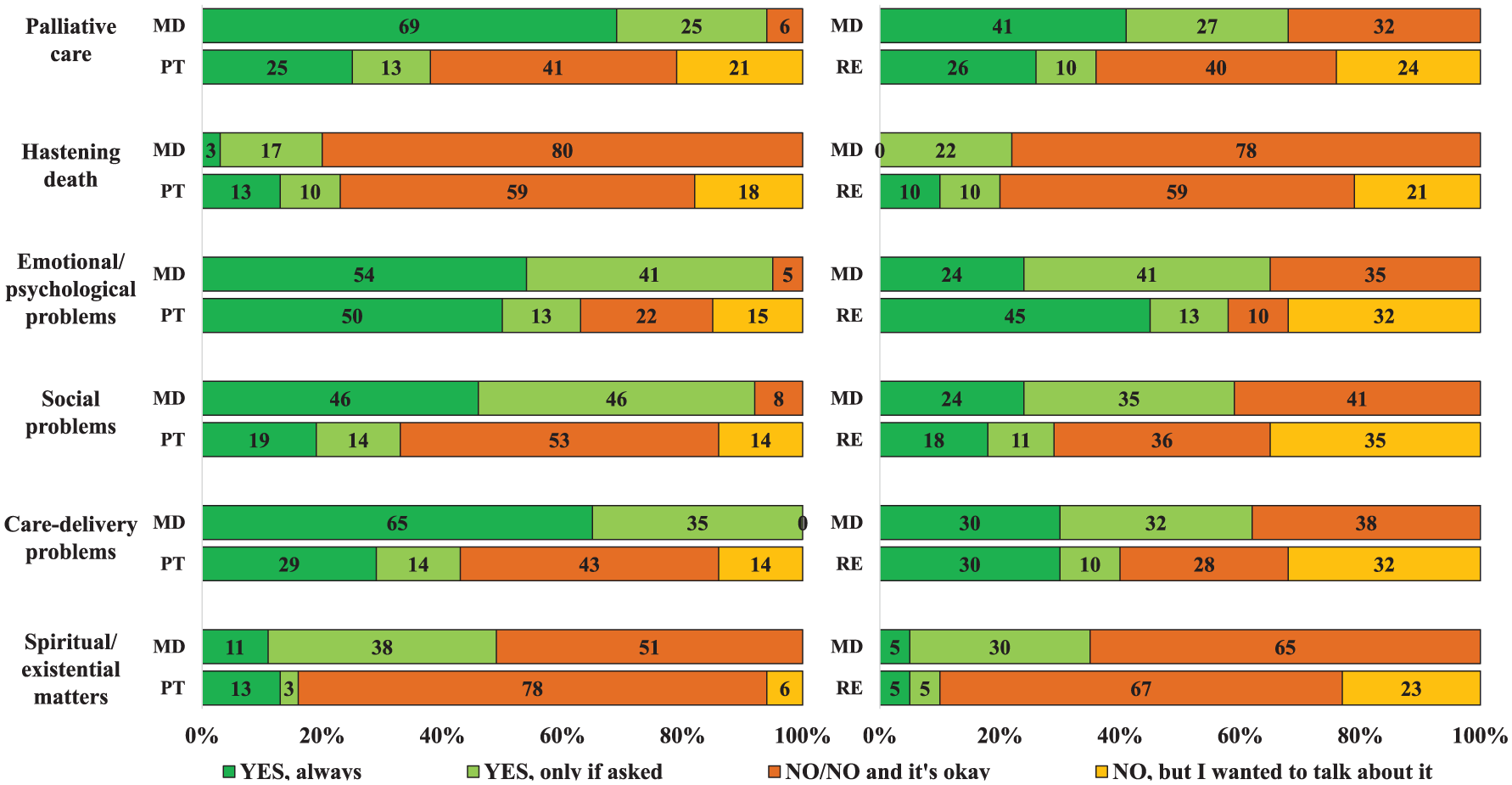
Percentages of topics of communication between medical doctors (MD) and patients (PT) and between MD and relatives (RE).
Similarly, 75% of patients and 68% of relatives reported having discussed possible complications from the beginning, while the majority of physicians (92%) reported having discussed this topic with patients, but only 43% with relatives.
A large percentage of patients reported not having discussed incurability (43%), life expectancy (49%), withholding and withdrawing treatments (75%), palliative care (62%), emotional and psychological problems (37%), social problems (67%), care delivery problems (57%), and spiritual and existential matters (84%), although a significant proportion stated that they would like to talk about these things. Interestingly, for these same issues, physicians reported not addressing them in much lower percentages of cases (8%, 11%, 19%, 6%, 5%, 8%, 0%, 51%, respectively).
Regarding these same issues, we found greater agreement between healthcare professionals and relatives in relation to what was communicated (both ‘always’ and ‘if requested’) and not (Figures 2 and 3).
There was significant agreement among responses concerning practices that could hasten death; the percentages were very similar among healthcare professionals, patients, and relatives, and showed broad agreement on avoiding this topic (as emerged in 80%–78% of physicians and in 59% of both patients and relatives).
As expected, when compared with nurses’ responses (complete data not shown in figures), physicians were more willing than nurses to discuss all areas with patients ‘always’. However, more than 50% of nurses reported that they ‘always’ discussed possible complications and care delivery problems with patients, and around 40% discussed purpose of treatment, emotional/psychological problems, and palliative options. In general, nurses were only willing to discuss EoL issues when patients asked for information.
When patients and relatives were asked to describe the quality of communication they had with physicians and nurses (Table 2, see in particular the numbers shown in bold), the majority rated it from sufficient to very/extremely warm, able to take into account their ability to understand and able to answer their questions, and clear and exhaustive. There was a very low rate of response that the communication they experienced was cold and detached.
Quality of professionals’ communication as perceived by PT and RE.

N = number (percentages).
PT: patients; RE: relatives.
Healthcare professional reactions and thoughts in dealing with the terminally ill and death
Using the E.L.D.Y.-CA.RE. questionnaire, we also investigated the feelings and opinions of healthcare professionals when caring for terminally ill patients. When professionals have to communicate bad news (multiple answers were possible), 45% of physicians, 24% of nurses, 33% of psychologists, and 8% of healthcare workers said that they felt adequately prepared. At the same time, 34% of physicians, 59% of nurses, 17% of psychologists, and 50% of healthcare workers admitted to feeling inadequate; a further 33% of psychologists felt scared (as opposed to 3% of physicians and 2% of nurses). Some professionals also admitted that they would like to delegate the task to someone else (11% of physicians, 8% of nurses, 17% of healthcare workers, but 0% of psychologists).
We then analysed another relevant emotional aspect: the reactions of professionals faced with the moment of a patient’s death (multiple answers were possible, Figure 4). A very significant proportion of professionals admitted contemplating the limits of their profession (55% of physicians, 36% of nurses, 50% of psychologists, and 31% of healthcare workers), talking about it with colleagues (40% of physicians, 39% of nurses, 67% of psychologists, and 63% of healthcare workers), bringing the suffering (18% of physicians, 29% of nurses, 50% of psychologists, and 13% of healthcare workers), and seeing it as part of their job (45% of physicians, 30% of nurses, 33% of psychologists, and 50% of healthcare workers). Other professionals reported thinking about their own death (8% of physicians, 20% of nurses, 33% of psychologists, and 19% of healthcare workers) or talking to their own relatives at home (16% of physicians, 18% of nurses, 17% of psychologists, and surprisingly half of healthcare workers). Another minority of professionals (physicians and nurses only) indicated ‘other’ reactions (such as a sense of freedom: 8% of physicians, 13% of nurses; indifference: 3% of physicians, 9% of nurses; or trying not to think about it: 3% of physicians, 9% of nurses).
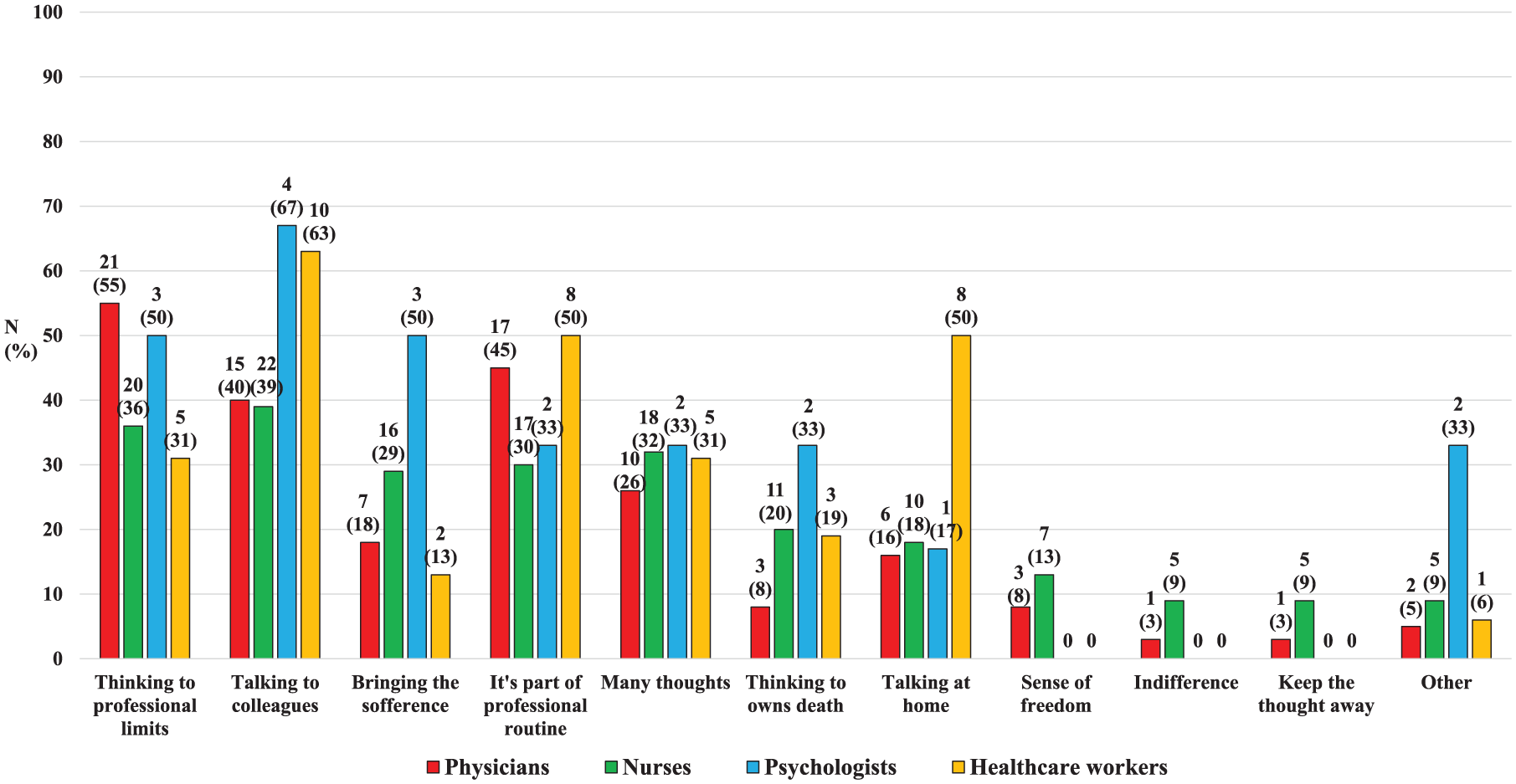
Professionals’ reactions facing with patient’s death.
Regarding the most important tasks in caring for a terminally ill patient (multiple responses were possible), respect for the patient’s dignity was considered the most important by all professionals (88%–100% of them). Respect for the patient’s desires and improving the patients’ quality of life were also seen as an important focus of the care (with responses ranging from 63% to 86% of professionals). Instead, respect for life itself was mentioned by 38% of physicians and 29% of nurses, 14% of psychologists, 31% of healthcare workers.
When caring for a terminally ill patient, compassion was the predominant feeling reported in all professions (53% of physicians, 57% of nurses, 67% of psychologists, and 80% of healthcare workers), followed by sadness (50% of physicians, 48% of nurses, 17% of psychologists, and 53% of healthcare workers). Worry and ‘other’ reactions (such as anxiety, empathy, support, understanding of the situation, but also feeling inadequate) were also reported by physicians and nurses in smaller percentages (<5%).
On the other hand, the most frequent approach when confronted with a family of a dying patient was for most professionals to help them understand the best way to help the patient (61% of physicians, 45% of nurses, 67% of psychologists, and 25% of healthcare workers), or attempting to share the clinical situation with family members (67% of psychologists, half of physicians, and a quarter of nurses). Many, particularly psychologists (100%) and healthcare workers (63%), reported in-depth listening, an option reported by only 34% of physicians and nurses. By contrast, 18%–19% of nurses and healthcare workers admitted trying to avoid direct contact.
Importance given to psychological and existential/spiritual dimensions
The questionnaire also asked about the psychological support patients received or were guaranteed: 32% of physicians, 59% of nurses, 20% of psychologists, and 44% of healthcare workers considered it to be inadequate/insufficient or absent.
Some questions asked about the importance of philosophical and/or religious beliefs in relation to EoL choices (Figure 5). Results confirmed that patients and relatives differed in their assessment of the importance of patients’ religious and/or philosophical beliefs in making ELDs: 49% of patients and 78% of relatives rated them as important/very important. Instead, it is interesting to note that a greater majority of relatives said that their own opinions were important/very important (68%), as opposed to the opinions of patients (43%). Conversely, more than half of patients (57%) and relatives (54%) rated professionals’ philosophical and religious beliefs as less important/not important in their own ELDs.

Importance given to professionals’ (MD, NU, PS, and HW), PT, and RE religious and/or philosophical beliefs in making EoL.
Considering the professionals’ point of view, a large majority of clinicians considered patient’s religious or philosophical beliefs important/very important in relation to their professional behaviour before making ELDs (with percentages ranging from 70% and 100%), while 26% of physicians, 14% of nurses, 0% of psychologists, and 6% of healthcare workers considered them less important/not important.
On the other hand, more contrasting results emerged in relation to the importance professionals attach to their own personal religious or philosophical beliefs in ELDs: 37% of physicians, 54% of nurses, 43% of psychologists, and 47% of healthcare workers considered them important/very important.
Healthcare professionals’, patients’, and relatives’ personal views of death
Finally, we explored the meanings that both professionals (Figure 6) and users (Figure 7) attached to death.

Professionals’ personal view of death.
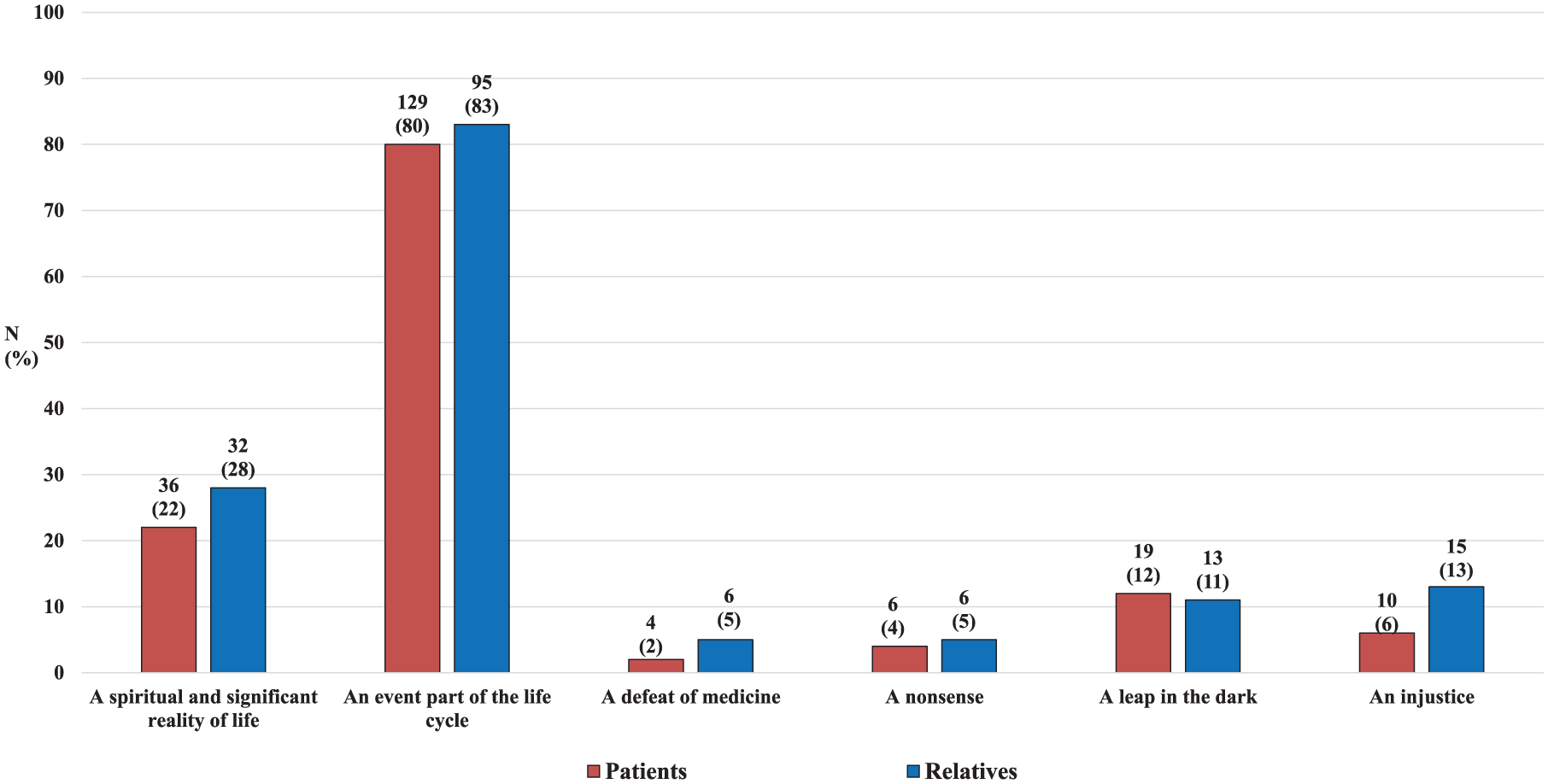
Patients’ and relatives’ personal view of death.
We found that most professionals saw death as an event that is part of the life cycle (68% of physicians, 89% of nurses, 100% of psychologists, and 88% of healthcare workers), while almost 40% of physicians and nurses and 100% of psychologists saw it as a spiritual and significant reality of life. A minority of professional respondents saw it as a leap in the dark (13% of physicians and 13% of nurses), a defeat for medicine (5% of physicians, 4% of nurses, and 25% of healthcare workers), a nonsense (3% of physicians, 4% of nurses, and 6% of healthcare workers), or an injustice (from 2% of nurses, and 19% of healthcare workers).
More than 80% of patients and relatives saw death as an event that was part of life, and around a quarter (22% of patients and 28% of relatives) saw it as a spiritual and meaningful reality of life. A minority of respondents saw death as a leap in the dark (12% of patients and 11% of relatives), an injustice (6% of patients and 13% of relatives), a defeat for medicine or nonsense (4% and 5% respectively).
Factors influencing professionals’ communication with patients
We then used logistic models to explore the respondent characteristics that may influence the subjects discussed. In particular, we observed the influence of the professionals’ role, gender, age, and the importance they attached to their or the patient’s religious and philosophical beliefs (Table 3). Specifically, in line with what was observed from the frequencies, it appeared that physicians were more likely to discuss with patients the diagnosis (p < 0.001), purpose of treatment (p < 0.001), the incurability of the disease (p = 0.003), possible complications (p = 0.001), palliative care options (p = 0.006), and social problems (p = 0.04). At the same time, healthcare professionals who were male (p = 0.02) and aged 50 years or older (p = 0.02) also appeared to be more likely to discuss the diagnosis with the patient. Those who considered patients’ religious and philosophical beliefs very important or important were more likely to discuss emotional and psychological problems with them (p = 0.03) and palliative care options with relatives (p = 0.05). Finally, it appeared that professionals who rated their own religious and philosophical beliefs as very important or important were more likely to discuss the patient’s diagnosis with their relatives (p = 0.05).
Association between the responses to the communication-related questions and the exploratory variables: odds ratios and confidence intervals from logistic univariate models.

Significativity in bold.
Discussion
Patients generally presented an attitude in which the important questions asked about EoL were less relevant to their condition than that reported by their relatives (Figure 1). This could also be the result of greater communication of bad news by healthcare professionals to the relatives than to the patient, which could indicate continuing paternalism (and sometimes perhaps even desired by older and less well-educated patients) in our society. This different perception of communicating bad news could also be due to the effect of denial mechanisms, which acts in different ways on patients and relatives. Indeed, our results showed that EoL-related issues remain difficult to discuss, for both professionals and users.26,27
In addition, a gap emerged between the perceptions of professionals and those of patients or relatives of the frequency of communication of these issues: physicians generally tended to report having discussed these topics more than patients or relatives. This difference in communication and the desire expressed by some patients and/or relatives to talk more about these dimensions may reflect a still unresolved need for physician–patient communication, which requires ad hoc training.4,7,28 Over time, training events have been implemented in this regard also within the IOV for all socio-healthcare professionals, with the aim of providing the necessary skills to address the communication needs of patients, and to explore and respect their wishes through the application of the tools provided by Law 219/2017.
At the same time, it is essential to consider the numerous organizational and environmental factors that influence the quality of communication both among professionals and between professionals and patients. 29 Indeed, healthcare organizations tend to focus on efficient organizational models, which, however, often fail to adequately support the communication process, frequently overlooking the different communication needs and timing of patients and their family members. It is, therefore, necessary to implement flexible organizational structures that ensure that each patient has sufficient time and space to process diagnosis and prognosis, and to approach ELDs. This includes adapting structural and logistical elements (e.g. such as the allocation of dedicated times and spaces for communication, the organization of communication processes and professional interactions, hierarchical division of spaces and resources, the presence of interruptions or noise, the use of supportive technologies, etc.) to the individual needs of the patient.28,29
This is in line also with previous studies in the literature that underline the need for healthcare professionals to be prepared to face communication, developing not only the ability to cope adequately with emotional events, but also the capability to reduce anxiety levels and burnout risks caused by the exposition to suffering and death.1,2 Training and adequate structural organization can help professionals in making communication more effective, providing instruments to support the patient’s gradual process of awareness-building of his health status and his participation in ELDs. 5 More recently, a care model, known as early palliative care, has emerged in the oncology setting and it has been adopted since 2015 at the IOV. 30 Early palliative care has been shown to improve quality of communication and the patient’s level of awareness and satisfaction,1,9,31 representing a clear example of the positive outcomes that can result from the introduction of dedicated time and space to address the specific communication needs of the patient, within a framework of multidisciplinary dialogue. In a recent experience at IOV, a joint evaluation of patients with advanced cancer by the oncologist and palliative care team was shown to enhance patients’ experience/satisfaction with care, such as listening, understanding, receiving information, symptom control, and decisions about the future. 31 In this special outpatient clinic shared between oncologist and palliative care team, which treats advanced cancer patients, shared care planning is implemented in accordance with Italian Law 219/2017. Early palliative care interventions, along with a more patient-centred communication, may be associated with an increased acceptance of death in patients with advanced cancer and their caregivers.1,32
Another relevant factor that emerges from the results of this study is the difference in the numbers of physicians (Figures 2 and 3, see bars marked ‘physicians’) who reported talking to patients as compared to relatives, with all subjects discussed most often with the patient and in less than half of the cases with relatives (in particular diagnosis, medical treatment, complications, palliative care), and this is true whether we consider what was discussed from the outset or only upon patient request. This may reflect a positive and less paternalistic attitude in directly involving patients in communication on certain basic clinical issues.
In addition, our study showed a significant percentage of physicians, and nurses who report contemplating the limits of their profession when faced with the death of a patient (Figure 4). Some also felt inadequate when having to communicate bad news. It is also possible that the diversity of roles and the diversification of tasks required to different professionals working in a healthcare setting affect the degree to which different professionals are involved in direct communication with patients or relatives, 33 and this could be the reason why clinical issues appear to be discussed more by physicians in the communication process,34,35 while 75% of nurses and 100% of healthcare workers involved in our study considered the communication of bad news to be outside their area of expertise.
These data could also appear consistent with the small percentage of physicians and nurses (34%) who reported engaging in deep listening, compared with the totality of psychologists, for whom it seems to be more a prerogative. This prompts reflection on heterogeneous conceptualizations of communication held by different professional categories, where physicians, in particular, may prioritize the technical aspects of care while potentially underestimating the therapeutic value of communication. 36 More specific training in this domain would foster a better awareness of the significance of the communication process, as emphasized by the Law 219/2017 itself, thereby facilitating the uniformity of relational skills across different healthcare professionals.
Physician guidelines on communication recommend discussing specific issues, such as goals of care and prognosis, treatment selection, EoL care, and facilitating family involvement in care. It is important to create communication opportunities to better understand who patients are and what matters to them, so that they can be more active participants in their care. 7 In order to facilitate open communication with the patient, it is similarly strategic to share information within the team, so as to facilitate dialogue and unambiguous communication between different health professionals and patients/family members. 1 Although physicians are formally responsible for EoL issues, nurses are likely to be involved in the decision-making process. In addition, most nurses think that patients would rather talk to them about EoL than to physicians, 37 and focus on their perception of patients’ expectations, severe symptoms, and emotional status. Nurses and physicians had a shared goal, which was to help patients and families through the process of making ELDs.
These findings, along with the professional differences observed in patient listening and communication, highlight the need to focus specifically on the implementation of training programmes that promote and support teamwork and interdisciplinary communication.28,38 Such programmes are essential for fostering a comprehensive and in-depth understanding of patients’ needs and characteristics, while also helping to address potential relational gaps due to an overly rigid division of professional roles. At the same time, shared, synergic teamwork can help professionals to prevent feelings of emotional overload, ineffectiveness and loneliness in their work, protecting them from health consequences, and increasing their own job satisfaction. In this regard, healthcare organizations should pay more attention in enhancing job satisfaction and reducing emotional overload by fostering more collaborative, supportive, and person-centred work environments. This may be achieved also through the reorganization of workloads, the integration of multidisciplinary teams, the establishment of spaces dedicated to emotional debriefing and clinical supervision, the implementation of psychological well-being programs for staff as well as adopting participatory leadership models and strengthening internal communication to increase healthcare professionals’ sense of belonging and autonomy. Collectively, these factors can play a significant role in reducing stress and promoting a healthier organizational environment.39–41 Furthermore, our findings suggest that professionals are aware of the importance of considering patient’s religious or philosophical issues – as can be seen from the large proportion of professionals who considered patient’s beliefs as important in clinical practice and decision-making.31,42 This may be consistent with the duty to evaluate the best clinical decisions for the patient without being influenced by personal values. In general, the tendency to prioritize respect for the dignity and will of the patient seems to emerge from the data of the present research, confirming that the bioethical principle of autonomy plays a major role in clinical practice, in line with what was established by Italian Law 219/2017.6,43,44 However, it is important to remember the still unclear consensus on the concept of ‘dignity’ and the difficulties in adopting a common definition. 45
From our results, the importance given to the patient’s personal beliefs appears to be related to a greater involvement of healthcare professionals in a communication that takes into account the emotional/psychological state of the patient, existential/spiritual matters, and the implications of palliative care, even though, as we have seen before, these areas are still poorly discussed by healthcare professionals in their everyday work. These data could be evidence that encouraging healthcare professionals to place more value on the psychological and existential dimensions can stimulate greater attention to those needs that are not only clinical, in a practice of care that can be truly global. 46
From the patient’s point of view, the importance attributed to the physicians’ beliefs was more heterogeneous: while the majority of relatives considered their own opinion relevant to the patient’s clinical decisions, this was considered important by only half of the patients. However, it is necessary to consider that the situation of vulnerability and weakness in which patients may find themselves can vary, rendering the opinion of healthcare professionals more or less relevant and at the same time perceiving the opinions of relatives as more or less important in decisions concerning EoL.47,48 Indeed, it is interesting to note that a quarter of physicians (26%) said that they did not consider the patient’s beliefs important in their professional decision-making process. It is not easy to understand this result, and a more thorough analysis of the respondents’ perspectives would be useful.
Although professionals are not yet prepared to talk about the existential dimension, spirituality also features in their personal vision of death, where just under half of physicians and nurses, and all psychologists, consider this event to be a spiritual and significant part of life, and the same appears to be true for almost a quarter of patients and relatives.
Our results highlight the importance of reflecting on the emotional and existential dimension of the EoL within the communication and clinical process: indeed, the psychological support and preparation available are judged insufficient to manage the complexity of the communication and decision-making process in EoL.
Better training is also required to enable healthcare professionals to take due account of the existential/spiritual dimension of the patient and even of themselves. The presence of a minority of professionals who still refuse to acknowledge the relevance of these dimensions highlights the need for training that also increases the value placed on these issues within the team, improving the unity and consistency of healthcare professionals, for an integrated and shared approach to the patient’s care.1,49 These data appear in line with the large proportion of healthcare workers who responded to our survey (Table 1) indicating, on the one hand, the lack of previous training in bioethics (29%–60%) and palliative care (14%–57%) and, on the other, a strong desire to receive further training in both bioethics and in palliative care (93%–100%). In this sense, training in bioethics and palliative care can enhance healthcare workers’ ability to discuss EoL topics and also manage the difficult implications of this type of communication.4,14,50–52
To this end, death and illness can no longer be perceived as the ‘limits’ of the medical profession but can begin to take on meaning 53 within a shared and global reflection.
Limitations of the present research include the small number of some professional categories that participated in the study (especially psychologists and healthcare workers) and the possible impact of this on the limited significant results obtained from logistic models. At the same time, as these data were collected for a study conducted in 2018, it would be interesting to replicate the study with a larger sample to explore how the clinical and social situation regarding EoL communication and support has changed in Italy since the implementation of Law 219/2017 and formative trainings developed in last years on it. Furthermore, in future research, we aim to complement the exclusive use of a quantitative methodology with more qualitative techniques, such as focus groups or in-depth interviews, to better understand the psychological and emotional reactions and personal beliefs of both professionals and patients. The findings emerging from this study may also serve as a scientific foundation for future research exploring the direct effects of targeted programmes designed not only to manage communication but also to address the emotional impact experienced by professionals in relation to death and terminal suffering. In particular, such research could investigate how open and shared communication at both interprofessional and intraorganizational levels may mediate these effects and encourage professionals to engage more explicitly with these issues. Finally, the ability to manage communication related also to the patient’s existential issues could itself be considered, through common instruments and recommendations, as a protective factor – one that should not be avoided, but rather integrated into communication programmes aimed at providing a comprehensive EoL care.54,55
Conclusion
This study is among the first to compare perspectives of patients, relatives, and healthcare professionals on communication in an oncological EoL setting, with a focus on their feelings, opinions, and existential/spiritual beliefs.
Our findings underscore the influence of both the psychological and emotional dimensions experienced by all parties involved. Notably, some healthcare professionals feel unprepared to discuss prognosis and EoL issues indicating the need for specific training, while patients ask for more transparent communication but appear uncertain in facing EoL options and choices.
Implementation of educational and organizational interventions and future research on the role of bioethics, palliative care, and communicational and psychological training should be prioritized to integrate a truly global care of the person and an effective patient-centred communication, in order to respond to healthcare professionals’ desire to receive further training, as demonstrated by our study, and to achieve a shared decision-making process, as Italian Law 219 requests.
Footnotes
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Veneto Institute of Oncology Ethics Committee 2018.
Consent to participate
Patients signed a consent form before participating in the study.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received ‘Ricerca Corrente’ funding from the Italian Ministry of Health to cover publication costs.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The questionnaires and data presented in this study are available on request from the corresponding author.