
Abstract
Background:
Potentially inappropriate medications (PIMs) pose a significant burden on patients with advanced cancer approaching the end of life. However, trends in the prescription of PIMs and the factors associated with deprescribing PIMs in these patients remain unclear.
Objective:
To describe trends in the prescription of PIMs and explore the factors associated with the deprescribing of PIMs in patients with advanced cancer in Japan.
Design:
Retrospective cohort study using medical claims data.
Methods:
We analyzed patients aged >65 years who were diagnosed with cancer 6 months before death and died between December 2017 and August 2023 in the city of Mito, Ibaraki prefecture, Japan. Sociodemographic, clinical, and prescription data were collected at 6 months (M6), 3 months (M3), and 1 month (M1) before death. PIMs were assessed according to the OncPal Deprescribing Guidelines.
Results:
The mean age of 1269 patients was 80.6 years, and 62.2% were male. PIMs were prescribed to 77.0% at M6, 76.4% at M3, and 70.0% at M1 (p < 0.001, M6 to M1). The factors associated with deprescribing at least one PIM from M6 to M1 included female sex, number of medications at M6, number of comorbidities, admission to a palliative care unit, and admission to a general ward.
Conclusion:
In patients with advanced cancer, PIM use decreased as they approached death. Deprescribing PIMs was more common in females, patients with polypharmacy and comorbidities, and patients admitted to hospitals, especially palliative care units.
Plain language summary
People with advanced cancer often take many medications, and some of these may no longer be helpful or could even be harmful as they near the end of life. These medications are called “potentially inappropriate medications” (PIMs). In this study, we looked at how often PIMs were prescribed to older adults with cancer in the last six months of life, and what factors were linked to stopping them (called “deprescribing”). We used medical records from 1,269 people over age 65 who died from cancer between 2017 and 2023 in Mito City, Japan. We checked their medications at 6 months, 3 months, and 1 month before death. We found that about 77% of patients were prescribed PIMs six months before death, and this number dropped to 70% one month before death. Doctors were more likely to stop at least one PIM in patients who were women, had many health conditions, were taking many medications, or were admitted to a hospital, especially to a palliative care unit. These results suggest that healthcare providers are reviewing and reducing unnecessary medications for people with advanced cancer, especially in hospital and palliative care settings.
Keywords
Background
Polypharmacy—commonly defined as the concurrent use of five or more medications 1 —is prevalent among patients with advanced cancer, a population characterized by limited life expectancy. 2 It could contribute to the use of potentially inappropriate medications (PIMs)—drugs in which the potential harms outweigh the benefits—thereby increasing the risk of adverse drug reactions, drug–drug interactions, and reduced quality of life. 3 Recent studies have reported increasing numbers of medications as death approaches, mainly owing to the addition of symptomatic drugs while preventive drugs are continued.4–6 Given the limited life expectancy, the use of preventive medications may be inappropriate when the time until benefit can be years, and patients are at increased risk of developing an adverse drug event due to their deteriorating pharmacokinetic and pharmacodynamic profiles. 7 Conversely, some medications, including non-steroidal anti-inflammatory drugs (NSAIDs), antidepressants, and benzodiazepines, usually considered to be potentially inappropriate, can be justified for managing symptoms in patients with advanced cancer. 8 In this population, medication optimization includes tailoring medications for preventing and treating existing illnesses and those for controlling symptoms, such as pain, according to individual-specific needs. 6
“Deprescribing” refers to the process of identifying and discontinuing medications that may no longer be beneficial or could potentially be harmful, especially for patients with limited life expectancy or those experiencing adverse effects. 9 This approach is often used to optimize treatment regimens, improve patient quality of life, and reduce the risks associated with polypharmacy and PIMs. According to the literature, it involves careful evaluation by healthcare professionals to manage polypharmacy and improve outcomes. 9 More recently, it emphasized the importance of distinguishing proactive deprescribing—the rational discontinuation of medications aimed at preventing harms—from reactive deprescribing, referring to medication discontinuation in response to adverse clinical triggers. 10 While deprescribing is increasingly recognized as a strategy for medication optimization, it remains underexplored in end-of-life cancer care. To support deprescribing in patients with advanced cancer, various tools and criteria have been proposed to optimize prescribing practices. 11 The OncPal Deprescribing Guideline, developed by Lindsay et al., has been proposed as one criterion for evaluating appropriateness of preventive medications in patients with advanced cancer with a life expectancy of less than 6 months. 12
In the Japanese home healthcare setting, our previous study revealed that two-thirds of Japanese patients with advanced cancer at the end of life were under polypharmacy, and half of them were prescribed at least one PIM, defined by the OncPal Deprescribing Guideline. 13 However, it remains unclear which classes of PIMs are continued, discontinued, or initiated at the end of life. In addition, few studies have investigated factors related to discontinuation of PIMs in the last 6 months for patients with advanced cancer.
Therefore, we aimed to (1) describe the trends in the prescription of PIMs defined by the OncPal Deprescribing Guideline during the latter half of the year before death in elderly patients with advanced-stage cancer and (2) identify factors associated with discontinuation of any PIMs among these patients.
The results of this study will contribute to a better understanding of prescription patterns and trends of preventive medications, and factors associated with discontinuation of such medications among patients with advanced cancer at the end of life. Although this study does not directly assess the clinical burden of preventive medications, the findings provide foundational data that may inform future research on the impact of deprescribing in this population.
Methods
Data source
In the Japanese healthcare system, National Health Insurance is designed for self-employed individuals, retirees, and those not covered by employer-based health insurance. The late-stage elderly medical care system covers individuals aged 75 years and older. 14 Medical insurance claims records included the monthly information of diagnoses, medical procedures, and prescriptions. The recorded diagnoses are based on the original Japanese disease codes linked to the International Classification of Diseases, Tenth Revision (ICD-10).
We used medical and pharmacy claims data from individuals with National Health Insurance for the self-employed and retirees aged under 75 years, and the late-stage medical care system for older adults aged 75 years and older between April 2017 and March 2023, in Mito City. Mito City is the prefectural capital in Ibaraki prefecture, with a population of approximately 266,000 and approximately 73,000 (27.0%) people aged ⩾65 years in 2012. 15
Research design and study population
This retrospective cohort study used the medical claims data. The data of patients who died between April 2019 and June 2022 in the National Health Insurance database and those who died between December 2017 and August 2023 in the late-stage medical care database were extracted. The inclusion criteria were as follows: patients whose primary diagnosis was recorded as cancer in the medical claims data 6 months before death (index time) and patients aged >65 years at the index time. The sample size was not determined by statistical calculation; instead, all eligible cases were analyzed to capture the overall trend.
Measurements
Patient characteristics, such as age, sex, primary site of cancer, and comorbidities, were extracted from medical claims 6 months before death. The recorded diagnoses of cancer and comorbidities were based on the original Japanese disease codes linked to the ICD-10 codes. The cancer types were divided into nine categories based on the classification of the Ministry of Health and Welfare 16 ; that is: (1) oral cavity, pharynx, gastric, and esophageal; (2) colorectal; (3) liver, gallbladder, bile duct, and pancreas; (4) lung; (5) breast; (6) gynecologic; (7) urothelial (bladder, renal, and urothelial) and prostate; (8) hematologic malignancies; and (9) others. Comorbidities were extracted based on previous studies on multimorbidities excluding malignancy 17 ; that is, hypertension, diabetes, hyperlipidemia, cerebrovascular diseases (hemorrhagic stroke, ischemic stroke, and other cerebrovascular diseases), cardiac diseases (ischemic heart disease, heart failure, atrial fibrillation, and poor circulation in the lower limbs), chronic respiratory diseases (asthma, chronic obstructive pulmonary disease, and chronic bronchitis), digestive diseases (stomach problems, colon problems, and chronic hepatitis), kidney diseases or failure, urologic diseases (neurogenic bladder, overactive bladder, and prostatic hypertrophy), arthritis or rheumatoid arthritis, chronic musculoskeletal conditions causing pain or limitation, fractures (femur fractures and other fractures), osteoporosis, dementia, neurological diseases (Parkinson disease and epilepsy), mental disorders (depression and anxiety), and thyroid disorders. ICD-10 codes are listed in Supplemental File 1.
The use of home medical care (HMC) and admissions to hospital general wards or palliative care units (PCU) were also extracted from medical claims during the period from 164 to 31 days before death. In Japan, HMC includes regular doctor visits, typically once or more per month, to provide medical management, including regular medication prescriptions covered by health insurance. HMC can offer primary, post-acute, and long-term care as well as palliative care for patients with advanced cancer in their homes, enabling home death. 18
Dependent variable
The dependent variable was the prevalence of PIMs specified in the OncPal Deprescribing Guidelines, and discontinuation of PIMs was defined as a reduction of more than one regular preventive drug listed in the Guidelines. To evaluate medications, we extracted orally administered prescriptions issued during the periods of 0–30 days (1 month: M1), 75–105 days (3 months: M3), and 165–195 days (6 months: M6) before death. Injections and topical drugs, which are commonly used to alleviate symptoms in patients with advanced cancer, were not assessed because we focused on the orally administered preventive drugs listed on the OncPal Deprescribing Guidelines. In addition, we accounted for the duration of medication prescription by adding the number of days to the prescription date and included medications whose final date of use fell within the same specified periods. Within each period, we counted the number of medications and determined the presence or absence of each PIM listed in the OncPal Deprescribing Guidelines. The claims data included prescribed medications based on the Ministry of Health, Labour and Welfare (MHLW) drug codes (YJ codes). The codes are managed by the MHLW for drug price standards and feature 12-digit alphanumeric drug codes. A list of YJ codes for drugs that correspond to PIMs was created (Supplemental File 2), and patients taking PIMs were identified in the database. When applying the OncPal Deprescribing Guidelines, blood pressure and sugar were not evaluated because of the nature of the medical claims. In addition, the use of complementary and alternative medicines was not available in the database, although it was listed in the guidelines. We defined polypharmacy as the presence of five or more prescriptions. 19
Statistical analysis
First, the basic characteristics of the patients were described, and the number of medications and PIMs of the patients at M6, M3, and M1 were described. Second, we assessed the change in the number of medications using the Wilcoxon signed-rank test and the frequency of PIMs using the McNemar test. In addition, the percent change in the prevalence of each PIM and its drug class from M6 to M1 was calculated, and the change was analyzed using the McNemar test. Third, factors associated with stopping any PIMs between M6 and M1 were investigated in patients who were prescribed at least one PIM at M6, using a logistic regression model. In the multivariate analysis, age, sex, number of medications at M6, number of comorbidities, use of HMC, admission to the PCU between M6 and M1, and admission to the general ward between M6 and M1 were included as independent variables.
The results of the logistic regression analysis were presented as odds ratios (ORs) and 95% confidence intervals (CI). All analyses were performed using SPSS version 27 (IBM, Armonk, NY, USA), and statistical significance was set at p < 0.05 (two-sided). As this study used health insurance claims data, there were no missing values. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental File 3). 20
Ethical considerations
This study was approved by the Ethics Committee of the Institute of Medicine, University of Tsukuba (Approval Number: 1870–2). The requirement for consent from the individual participants was waived owing to the anonymity of the data. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Results
Characteristics of participants
In total, 1269 adult patients with advanced cancer who had already been diagnosed with cancer as the main disease 6 months before death were analyzed in this study. The basic patient characteristics are shown in Table 1. The mean age was 80.6 years, and 62.2% of patients were male. The cancer types are shown in Table 1, with colorectal, respiratory, and esophagus/stomach cancers being the most common, in descending order. The most common comorbidities, in order of frequency, were digestive diseases, hypertension, chronic musculoskeletal conditions, and cardiac disease. The median number of comorbidities, excluding cancer, was five per patient.
Basic characteristics of the study population (n = 1269).

SD: standard deviation; IQR: interquartile range; HMC: home medical care; PCU: palliative care unit.
Trends in PIMs during the last 6 months of life in patients with advanced cancer
The average number of medications administered at M6, M3, and M1 was 7.0 (4.3), 7.3 (4.5), and 7.3 (5.2), respectively (Table 2). The prevalence of any PIMs listed in OncPal Deprescribing Guidelines was 77.0% at M6, 76.4% at M3, and 70.0% at M1, with a significant difference between M6 and M1 (p < 0.001).
Trends in prescribed medications during the last 6 months of life in elderly patients with advanced cancer (n = 1269).

M6: 6 months before death; M3: 3 months before death; M1: 1 month before death; IQR: interquartile range; PIM: potentially inappropriate medication; DPP-4: Dipeptidyl Peptidase-4; SGLT-2: Sodium-Glucose Co-Transporter-2; GLP-1: Glucagon-Like Peptide-1; CAM: complementary and alternative medicine.
McNemar test between M6 and M1.
Wilcoxon test between M6 and M1.
p < 0.05.
Discontinuation and change in prescriptions of PIMs at the end of life in patients with advanced cancer
Frequent PIMs discontinued between M6 and M1 included antiplatelets (−19.8%, p < 0.001), antihypertensive (−20.9%, p < 0.001), dyslipidemia (−49.5%, p < 0.001), oral hypoglycemics (−31.9%, p < 0.001), osteoporosis medications (−25.9%, p = 0.018), and vitamins and minerals (−15.0%, p = 0.016). Conversely, the prevalence of peptic ulcer prophylaxis did not differ significantly between M6 and M1 (+2.0%, p = 0.534).
Logistic regression model revealed that females compared with males (adjusted odds ratio (aOR) 1.35, 95% CI: 1.02–1.79), the number of medications at M6 (aOR 1.08, 95% CI: 1.04–1.13), the number of comorbidities (aOR 1.08, 95% CI: 1.01–1.16), admission to PCU between M6 and M1 (aOR 11.63, 95% CI: 6.60–20.48), and admission to general wards between M6 and M1 (aOR 1.54, 95% CI: 1.14–2.06) were associated with discontinuation of any PIMs between M6 and M1 (Table 3).
Factors associated with deprescribing of any PIMs from M6 to M1 using logistic regression analysis (n = 977).
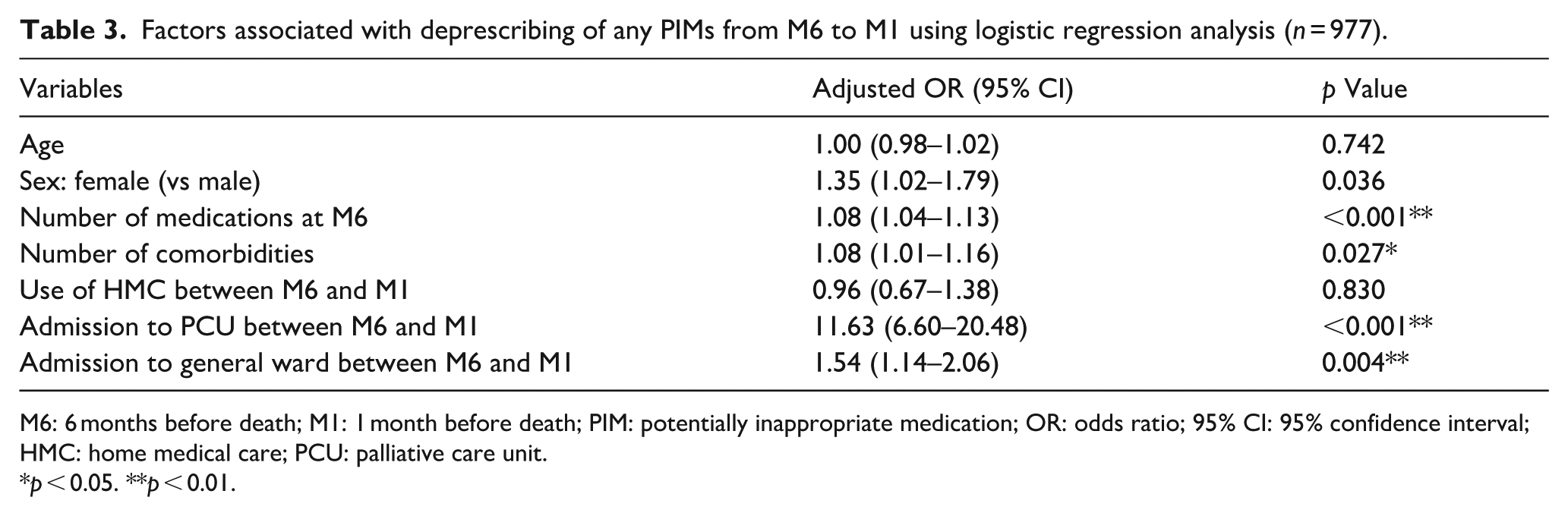
M6: 6 months before death; M1: 1 month before death; PIM: potentially inappropriate medication; OR: odds ratio; 95% CI: 95% confidence interval; HMC: home medical care; PCU: palliative care unit.
p < 0.05. **p < 0.01.
Discussion
Our results showed that patients with advanced cancer tended to have a decrease in the prescription of PIMs as they approached the end of life, although there was a slight overall change. We also identified factors associated with their discontinuation. To the best of our knowledge, this is the first study in Asian countries to use claims data to describe trends in PIMs during the last 6 months of life in patients with advanced cancer. We also explored the factors associated with the discontinuation of these medications.
We showed that approximately three-quarters of patients with advanced cancer at the end of life were prescribed at least one preventive drug for chronic diseases listed in the OncPal Deprescribing Guideline. This could be potentially inappropriate, considering that the study population died within 6 months. The prevalence of PIMs among patients with advanced cancer receiving palliative care ranged from 22% to 95%, depending on the study population and criteria used. 21 The most frequent PIMs at M6 in our study were: (1) peptic ulcer prophylaxis, (2) antihypertensives, (3) vitamins and minerals, (4) dyslipidemia medications, and (5) oral hypoglycemics, which are similar to those of a previous report. 22 These drugs can be targeted for dose reduction or discontinuation when indications or symptoms are lacking. 12
In our study, preventive drugs for chronic diseases such as antihypertensives, statins, or anti-diabetics were discontinued as death approached. In contrast, the use of peptic ulcer prophylaxis did not change significantly. A similar trend was observed in a previous study conducted in Sweden, though the change in antihypertensives, vitamins and minerals, and bisphosphonates was not significant. 5 These differences may reflect variations in clinical practice patterns in cultures and regions. These results suggest that physicians discontinue preventive drugs, considering the limited life expectancy of patients with advanced cancer. However, we operationalized deprescribing as observed discontinuation of PIMs, recognizing that this may not always reflect a proactive, clinician-initiated deprescribing process. In addition, we acknowledge that clinical and patient outcomes were not assessed in this study. Therefore, caution is needed when interpreting the appropriateness of these prescriptions solely based on medication class or guideline criteria.
In particular, the prevalence of peptic ulcer prophylaxis remained relatively unchanged throughout the final months of life, which is similar to a previous study. 23 However, other studies showed a decrease in the trend.22,24 One possible explanation is that patients with advanced cancer often receive medications such as corticosteroids or NSAIDs for symptom management, which are known to increase gastrointestinal risk. Thus, clinicians may be reluctant to discontinue gastroprotective agents, even in the context of deprescribing other preventive medications. In addition, routine continuation of such medications may occur due to prescribing inertia or perceived low harm.
In the present study, among patients with advanced cancer approaching the end of life, female patients compared to male patients, those taking more medications, those with more comorbidities, and those admitted to the hospital (including the PCU and other wards) were more likely to be associated with deprescribing of PIMs. A study conducted in Japan reported that factors associated with the reduction of cardiovascular preventive medications in patients receiving home healthcare included advanced age, duration of home visits, cancer, dementia, and Parkinson’s disease. 25
In our study, female patients were more likely to have PIMs discontinued. According to a previous systematic review, sex was not associated with patients’ attitudes toward deprescribing among older adults. 26 However, one study found that female sex was a significant predictor of willingness to have medications deprescribed, with the odds increasing threefold in female patients. 27 The authors suggested that this association might be partly explained by differences in medication adherence. Moreover, sex differences in involvement in the deprescribing process may also contribute. This may be explained by the fact that female patients were more aware of harmful medications and were more likely than men to initiate a deprescribing conversation and to seek out medication-induced harm. 28 Further studies are needed to understand the relationship between sex and deprescribing in this population.
The finding that deprescribing is implemented more frequently in patients with polypharmacy and multiple comorbidities is also reasonable because patients with multimorbidity and polypharmacy are willing to be deprescribed. 29 Deprescribing occurs more frequently in patients admitted to general wards or PCUs. This may reflect reactive deprescribing based on a decline in the general condition of the patients at the time of hospitalization. In addition, multidisciplinary medication reconciliation after hospitalization may have contributed to deprescribing. Deprescribing in our findings is more likely to occur in PCU admissions than in general ward admissions. A previous study has indicated that palliative care consultation was associated with improved medicines optimization. 30 The findings suggest that palliative care physicians may be more proactive in deprescribing as part of a comprehensive approach focused on quality of life and reduction of treatment burden at the end of life. The factors identified in this study are not modifiable, making direct intervention difficult. However, recognizing these characteristics may be valuable for healthcare professionals when considering deprescribing during medication review. Conversely, interventions for patients in whom deprescribing is less likely remain a challenge for future research.
This study had several limitations. First, recording bias or missing data may have occurred because this study was conducted using claims data. This could lead to the overestimation or underestimation of the prevalence of comorbid diseases. However, regarding prescriptions, this study included various physician prescriptions, making the results more robust. Second, we focused on patients who were diagnosed with cancer at least 6 months before death; therefore, patients with shorter intervals between diagnosis and death were not evaluated. Third, as blood pressure data were not obtained from the claims data, antihypertensive drugs were overestimated as PIMs. Fourth, we did not assess drugs other than those listed in the OncPal Deprescribing Guidelines. It was unclear what kind of symptomatic drugs, such as opioids and laxatives, were additionally prescribed in the last 6 months for patients with advanced cancer. Fifth, because this study was based on data from a single municipality, its generalizability to other countries may be limited. Japan’s healthcare and cultural context—characterized by universal health coverage, high trust in physicians, and a strong societal emphasis on medication adherence—differs from other healthcare systems. 31 These findings should be interpreted with caution when applied to different cultural or healthcare settings. Sixth, we could not understand the process of deprescribing, that is, how physicians explained deprescribing to patients and their caregivers, and their responses about deprescribing. Future research should explore how physicians, patients, and caregivers feel about deprescribing in this population, and the physical and psychological impact of deprescribing on patients. Seventh, our findings should be interpreted with caution, as this is a retrospective observational study in which causal relationships cannot be established. In addition, the absence of clinical indicators such as performance status or symptom burden raises the possibility of confounding. Eighth, due to the nature of claim-based data, it was difficult to know the clinical intent behind medication changes and distinguish between proactive and reactive deprescribing. The observed associations partly reflect patients’ underlying clinical deterioration or transitions in care settings, rather than proactive or structured deprescribing practices.
Conclusion
It was found that elderly patients with advanced cancer tend to have a decrease in the prescription of PIMs as they approach the end of life, still with room for deprescribing, considering their limited life expectancy. Female sex, more medications and comorbidities, and hospital admission, including PCUs, were associated with deprescribing of PIMs among patients with advanced cancer approaching the end of life. Recognizing these characteristics may be valuable for healthcare professionals when considering deprescribing during medication review and proactive deprescribing efforts, rather than reactive deprescribing needs to be enhanced as part of a comprehensive strategy for medication optimization. The impact of deprescribing among patients with advanced cancer and interventions for patients in whom deprescribing is less likely remain a challenge for future research.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251403020 – Supplemental material for Trends in prescriptions and factors associated with discontinuation of potentially inappropriate medications in elderly patients with advanced cancer at the end of life: A retrospective cohort study
Supplemental material, sj-docx-1-pcr-10.1177_26323524251403020 for Trends in prescriptions and factors associated with discontinuation of potentially inappropriate medications in elderly patients with advanced cancer at the end of life: A retrospective cohort study by Shoichi Masumoto, Yu Sun, Mikiya Sato, Kenji Momo, Jun Hamano, Chihiro Nishiura, Kenji Fujimoto and Tetsuhiro Maeno in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524251403020 – Supplemental material for Trends in prescriptions and factors associated with discontinuation of potentially inappropriate medications in elderly patients with advanced cancer at the end of life: A retrospective cohort study
Supplemental material, sj-docx-2-pcr-10.1177_26323524251403020 for Trends in prescriptions and factors associated with discontinuation of potentially inappropriate medications in elderly patients with advanced cancer at the end of life: A retrospective cohort study by Shoichi Masumoto, Yu Sun, Mikiya Sato, Kenji Momo, Jun Hamano, Chihiro Nishiura, Kenji Fujimoto and Tetsuhiro Maeno in Palliative Care and Social Practice
Supplemental Material
sj-docx-3-pcr-10.1177_26323524251403020 – Supplemental material for Trends in prescriptions and factors associated with discontinuation of potentially inappropriate medications in elderly patients with advanced cancer at the end of life: A retrospective cohort study
Supplemental material, sj-docx-3-pcr-10.1177_26323524251403020 for Trends in prescriptions and factors associated with discontinuation of potentially inappropriate medications in elderly patients with advanced cancer at the end of life: A retrospective cohort study by Shoichi Masumoto, Yu Sun, Mikiya Sato, Kenji Momo, Jun Hamano, Chihiro Nishiura, Kenji Fujimoto and Tetsuhiro Maeno in Palliative Care and Social Practice
Footnotes
Acknowledgements
ORCID iDs
Ethical considerations
This study was approved by the Ethics Committee of the University of Tsukuba (Approval No. 1870–2).
Consent to participate
The requirement for consent from the individual participants was waived owing to the anonymity of the data.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are available from Mito City, Ibaraki, Japan, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. However, data are available from Mito City upon reasonable request and with permission.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.