
Abstract
Background:
Advance care planning (ACP) is crucial for ensuring quality end-of-life care, yet its implementation remains limited in Thailand.
Objectives:
To understand the attitudes and preferences of older Thai adults towards ACP in primary care settings.
Design:
A cross-sectional study was conducted using structured interviews. Data on demographics, health status, attitudes, and preferences towards ACP were collected. Multivariable analysis was performed to identify factors associated with ACP attitudes and preferences.
Setting/subjects:
Participants aged 60 years or older at the Primary Care Unit of Songklanagarind Hospital, Thailand, between June and December 2022.
Results:
Among 250 participants, 60% had high comorbidity levels (Charlson Comorbidity Index >3). While most participants demonstrated high attitude levels towards ACP, over 40% did not want to make an ACP, and 37.2% wanted to postpone it. Higher educational levels (adjusted OR (aOR) = 2.17, 95% CI: 1.16–4.06) and prior ACP discussions (aOR = 4.08, 95% CI: 1.38–12.08) were significantly associated with high attitude levels. Participants with high attitude levels showed greater odds of desiring to engage in ACP (aOR = 2.81, 95% CI: 1.45–5.42). Those with higher education (aOR = 2.09, 95% CI: 1.1–3.98) and family members who received life-sustaining treatment (aOR = 1.9, 95% CI: 1.02–3.55) were more likely to prefer ACP engagement.
Conclusion:
Tailored education and repeated ACP discussions are needed to bridge the gap between attitudes and engagement among older Thai adults.
Plain language summary
This study looked at how older Thai adults think about advance care planning (ACP), which involves making decisions ahead of time about future medical treatment, especially for serious illness. We interviewed 250 people aged 60 or older at a hospital in Thailand. Most people had a positive view of ACP, but over 40% were hesitant to take part. People with higher education or who had already talked about ACP were more likely to have positive views and want to get involved. Our results showed that having a good attitude about ACP does not always mean people will take action. To help more older adults take part, we recommend creating clear and simple educational programs, considering different learning needs, and giving people more chances to talk about ACP with their healthcare team. These findings can help health providers give better support as older adults plan their future healthcare.
Keywords
Introduction
The global rise in older populations is driving an increase in chronic diseases and geriatric syndromes. 1 In Thailand, nearly 20% of individuals are aged 60 or above, with noncommunicable diseases such as cardiovascular disease, cancer, and stroke as leading causes of death.1,2 Similar patterns are observed in Singapore, where most older patients who died in emergency departments had advanced chronic illnesses, but many still died despite stable or early-stage conditions. 3 Social and psychological risks also contribute to frailty among older adults. 4 As health declines, decision-making often shifts to families when individuals lose capacity.5,6 These challenges highlight the growing need for effective end-of-life care and advance care planning (ACP) to ensure healthcare preferences are respected.
ACP enables older adults to communicate end-of-life care preferences with families and healthcare professionals, helping clarify patient wishes and guide care decisions. 7 Despite widespread policy endorsement and promotion, ACP has not consistently been shown to improve end-of-life care quality or achieve goal-concordant care.8,9 Systematic reviews indicate ACP may modestly benefit patient–physician communication and certain caregiver outcomes, but the impact on broader patient and healthcare system outcomes remains limited and inconclusive.10–12 Implementation of ACP continues to be restricted in many healthcare settings.5,13 For example, only a minority of patients have ACP documentation available during medical emergencies, 14 signalling the need for further research and carefully targeted approaches in primary care and other contexts.
End-of-life care discussions remain complex for older adults, families, and healthcare professionals, especially in Asia, where ACP awareness and participation are low. 15 In countries like Hong Kong and Singapore, less than 40% of older people are aware of ACP, 16 with engagement shaped by demographic factors—such as education, health, and marital status—as well as sociocultural traditions and beliefs.17–19
In Thailand, palliative care and legally binding living wills have been promoted since 2007, but awareness and adoption of ACP remain limited among the public and healthcare professionals. 20 Thai government, in coordination with the Thai Palliative Care Society and other organisations, published ACP standards in 2022 and integrated ACP into national health policies with ongoing provider training and reimbursement. 20 By 2020, ACP became one of three major key performance indicators for health inspection in Thailand, though it remained mostly limited to palliative care patients. 20 ACP discussions are still uncommon in Thai families and are rarely initiated by physicians or relatives,21,22 leaving many older adults without the chance to express their end-of-life care preferences—highlighting a critical gap in expanding ACP beyond palliative contexts.
In Thailand, there is limited public education on ACP, and research on the factors influencing preferences for ACP among older adults is scarce. This study aims to understand the perspectives of older Thai individuals regarding ACP, which can enhance our understanding of ACP from Asian cultural viewpoints, guide effective communication in clinical practice, and inform future interventions for older adults. Specifically, the objectives are to understand older adults’ attitudes and preferences regarding ACP and to identify factors associated with their levels of attitudes and preferences concerning ACP.
Methods
Study design
A cross-sectional study using structured interviews was conducted at the Primary Care Unit (PCU) of Songklanagarind Hospital, Thailand, between 1st June 2022 and 31st December 2022. This study is reported following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement and checklist, 23 with details provided in Supplemental Material 1.
Participants
Patients who visited the PCU and met the specific criteria below were invited to participate in this study.
Inclusion criteria
Aged 60 years or older
Willing to participate in the study
Not in emergency conditions such as acute stroke, hypertensive crisis, hyperglycaemia
Exclusion criteria
Currently undergoing cancer treatment
Have previously completed an ACP
We excluded people who were on cancer treatment, as they might have a higher chance of engaging in ACP as part of their treatment than the general older population,24,25 and this may confound our findings. We also excluded older people who had already completed an ACP. Although their preferences could change over time depending on current health conditions, 10 they might have different views on ACP from other older people at PCU.
Sample size
The infinite population proportion formula below was used to estimate the sample size using the n4studies software.

Due to limited evidence on the attitude levels towards ACP in older adults in Thailand, we used data from our pilot testing (see the section below), which suggested that 18% of older participants had a high attitude level. Hence, we set P = 0.18 and error = 0.05. The sample size was calculated to achieve a power of 0.80, resulting in a requirement of 227 participants; this was increased to 250 to accommodate an anticipated 10% rate of incomplete data.
Data collection
We interviewed participants using a validated structured questionnaire. The questionnaire explored knowledge, attitudes, and willingness to engage in ACP in older adults. Interviews were conducted by a trained family medicine resident under supervision from a geriatric psychiatrist and a family medicine physician. Given the sensitivity of end-of-life topics, interviews took place in a private, quiet room, with participants informed of their right to stop at any time. Basic psychological support and follow-up were available for those experiencing distress; however, most participants reported finding the interviews interesting and felt they increased their awareness of ACP. We also retrieved their medical history regarding comorbidities and treatments through a hospital computerised medical database.
Measurement and tool
In this study, our validated, predetermined questionnaire consisted of three sections as follows (see Supplemental Material 2 for the questionnaire).
(1) Demographic and general data (age, gender, religion, monthly income, education level, occupational status, marital status, cohabiting members, and unfulfilled businesses)
(2) Health-related data (history of using life-sustaining treatments, experience witnessing family members using life-sustaining treatments, experience of caring for family members until death, general health satisfaction, co-morbidities using the Charlson Comorbidity Index (CCI), 26 activity daily living (ADL) using the Barthel Index for basic ADL 27 and the iADL Index for instrumental ADL. 28
(3) Knowledge, attitudes, and preferences regarding ACP
In this study, a questionnaire assessing knowledge, attitudes, and preferences regarding ACP was developed based on a literature review. The content validity was evaluated by three palliative care experts, including one psychiatrist and two family physicians, who rated each item for relevance and suggested revisions. The Item Objective Congruence (IOC) Index was calculated for each item, with revisions made and retested until every item achieved an IOC value >0.5. A pilot test was then conducted with 30 older patients at two PCUs within the hospital’s network, yielding an acceptable Cronbach’s alpha coefficient of 0.82, indicating good internal consistency and reliability of the questionnaire.
The questionnaire on attitudes regarding ACP comprised 3 items on general opinions about ACP and 15 items covering specific statements on positive and negative attitudes, using a 5-point Likert scale (strongly agree to strongly disagree). Responses were transformed into numeric scores of 1–5, with 5 indicating the most positive attitudes. Scores for negative items were reversed, resulting in attitude scores ranging from 15 to 75, with higher scores indicating more positive attitudes towards ACP. To assess participants’ preferences for ACP, they were asked whether they wanted to make an ACP.
Data analysis
The data were entered into Excel and analysed using R software. 29 Categorical data were presented as frequency and percentage, while continuous data were presented as mean (SD) and median (IQR). Associations between categorical variables were tested using Chi-square or Fisher’s exact test, while t test or Rank sum test was used for continuous variables. Attitude scores were classified into Low, Medium, and High levels using the Best criteria. 30 Best 30 suggested assigning scores to Likert-type items and grouping average scores into three categories for interpretation. The interval for each category is found by subtracting the minimum score from the maximum score and dividing by the number of categories.
Factors associated with attitudes and preferences towards ACP were identified from the literature and bivariate analysis (p < 0.20), and then included as covariates in the multivariable logistic regression to adjust for potential confounders. In the regression models, variables were tested using the Variance Inflation Factor with a threshold of less than 10. 31 Statistical significance was considered at p < 0.05.
Results
Participant characteristics
During participant recruitment, 276 eligible individuals were invited to take part in the study. Of these, 26 declined participation, resulting in a final sample of 250 participants included in the study. The most common given reasons were inconvenience regarding timing (18 people) and unwillingness to talk about dying (8 people; data not shown in tables).
From Supplemental Material 3 for characteristics and general information of participants, the study included 250 participants, predominantly female (65.6%), married (77.6%), Buddhist (96%), and currently unemployed (62.0%). The mean age was 70 years (SD = 7.3), with around 80% having completed compulsory education or lower, and most reporting income below Thailand’s average. Over 60% had a CCI of >3, with the most common comorbidities being dyslipidaemia (87.8%), hypertension (62.2%), and diabetes mellitus (28.9%). Most participants (65.6%) expressed satisfaction with their general health status. While only a few (2.8%) had direct experiences of receiving life-sustaining treatments, 38% had witnessed family members undergoing such treatments, and 51.6% had cared for relatives until death (see Supplemental Material 3 for further details).
General attitudes towards advance care plan
In the study, only 18 participants (7.2%) were advised to develop an ACP, while 47 (18.8%) discussed ACP with others, including family and healthcare professionals. Twenty-seven participants (10.8%) knew someone who had an ACP. Regarding general attitudes towards ACP, approximately 60% of participants believed everyone should know (62.8%) and engage (56.4%) in ACP, while only 51.6% wanted to know more about ACP (data not shown in tables).
Specific attitudes towards ACP and associated factors
Table 1 summarises responses to specific attitude items. For analysis, ‘Strongly agree’ and ‘Agree’ were combined, as were the ‘Disagree’ responses. Over half (57.2%) felt that unfinished business left them unprepared for ACP. Nearly one-third reported that ACP caused death anxiety (25.2%) or family discomfort (27.6%). Nonetheless, most participants believed ACP ensures care aligned with their needs (94%), reduces family worries (82.8%), and lessens family conflict (80.8%).
Specific attitudes towards the advance care plan (N = 250).

ACP: advance care planning.
‘Agree’ to these questions indicated negative attitudes towards ACP.
Attitude scores towards ACP were classified as Low (15–35), Medium (35–55), and High (>55) by Best criteria. For analysis, the Low group (n = 3) was merged with Medium (n = 67) due to its small size. Over two-thirds showed high-level attitudes towards ACP. Table 2 shows that higher education (p = 0.002) and prior ACP discussions (p < 0.001) were significantly associated with high attitudes.
Factors associated with positive attitudes towards ACP (n = 250).

ACP: advance care planning; CCI: Charlson Comorbidity Index.
Higher education and previous ACP discussions were significantly linked to higher attitude scores.
Chi-square test.
Rank sum test.
Fisher’s exact test.
Three participants had a low attitude level; 67 had a medium level.
ACP preferences and associated factors
Table 3 shows that over 40% of participants did not want to make an ACP, while 57.6% preferred to develop one, though 64.6% of those wished to delay. The top reasons for declining ACP were death-related concerns (17.9%) and confidence in descendants’ decision-making (16.8%). Those wanting ACP cited reducing descendant burden (29.4%) and feeling prepared (21.6%). Participants preferring to postpone ACP commonly cited waiting until close to the end of life (49.4%) and needing more information (23.6%) (see Supplemental Material 4 for details).
Participant preferences for ACP (n = 250).
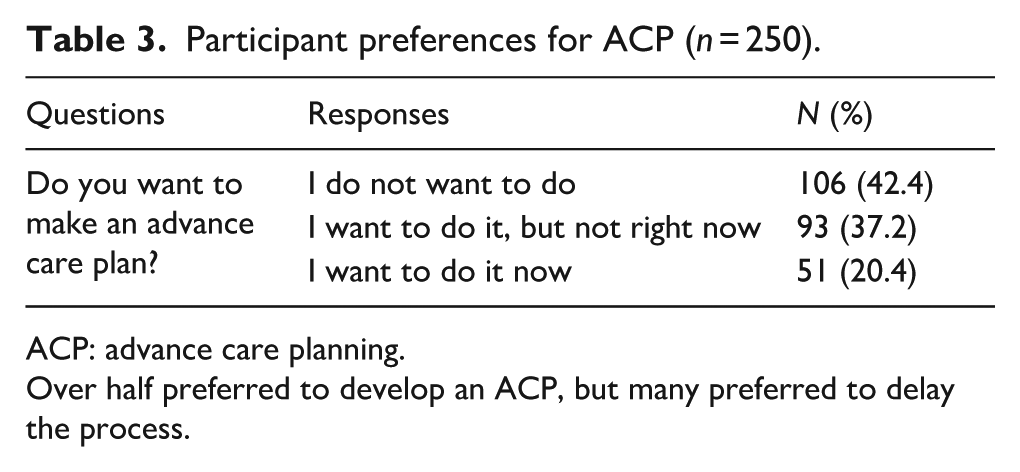
ACP: advance care planning.
Over half preferred to develop an ACP, but many preferred to delay the process.
Table 4 shows that preference for ACP was significantly associated with having a younger age, descendants, higher education, above-average income, and high attitude scores.
Factors associated with ACP preferences (n = 250).

ACP: advance care planning; CCI: Charlson Comorbidity Index.
Having descendants, higher education, above-average income, interest in ACP, and high attitude scores were significantly linked to a preference for ACP.
Chi-square test.
Rank sum test.
Fisher’s exact test.
Three participants had a low attitude level; 67 had a medium level.
Multivariable analysis of factors associated with ACP attitudes and preferences
The multivariable analysis of factors associated with ACP attitudes and preferences is shown in Table 5. People with education above the compulsory level were twice as likely to have higher ACP attitude scores, and those who had already discussed ACP were four times as likely to score higher.
Multivariable logistic regression for factors associated with attitudes and preferences of advanced care plan.
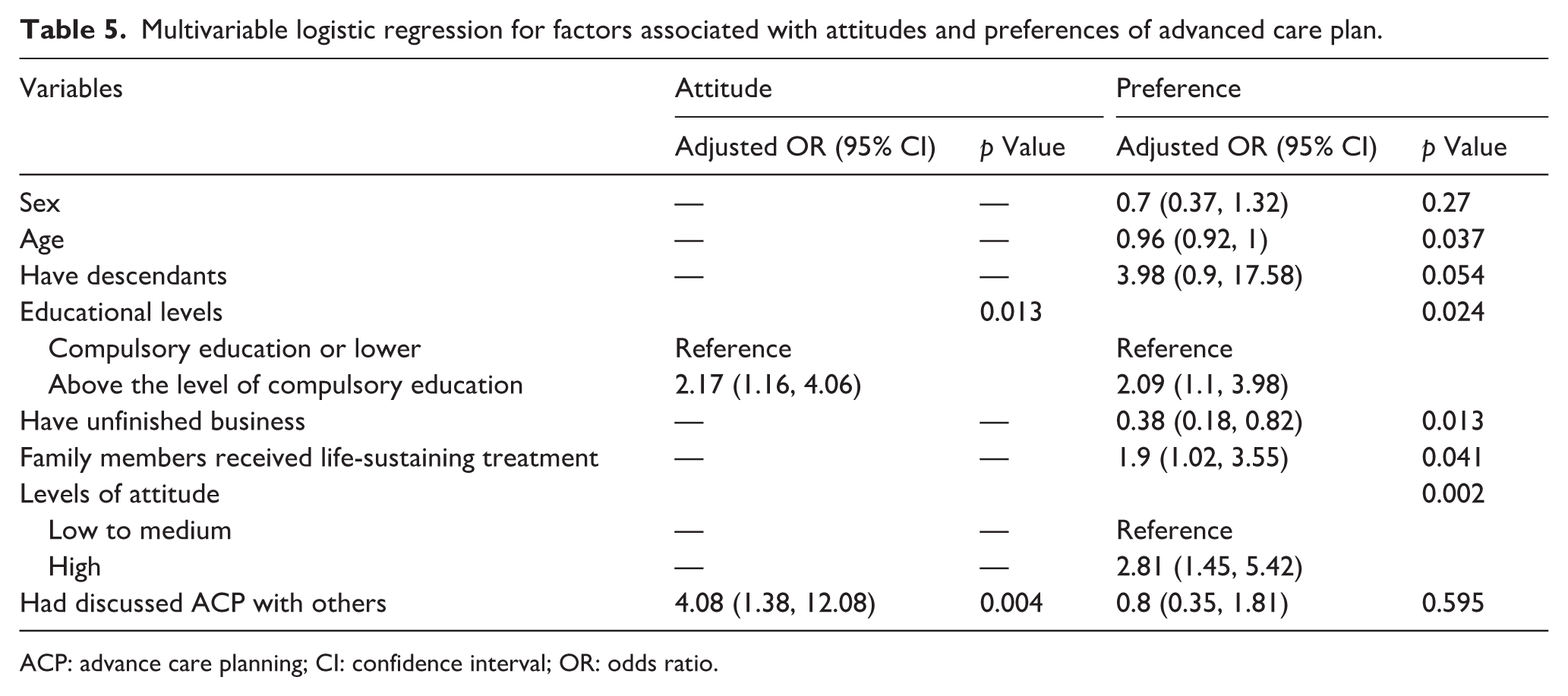
ACP: advance care planning; CI: confidence interval; OR: odds ratio.
From Table 5, participants with higher education and those who had a family member receive life-sustaining treatment were about twice as likely to prefer ACP engagement. Having a higher attitude score towards ACP increased this likelihood by almost three times. In contrast, unfinished business made ACP engagement much less likely.
Discussion
To our knowledge, this is the first study on attitudes and preferences towards ACP among older adults in primary care settings in Thailand. Most participants had chronic physical illnesses (60% had CCI > 3) and generally high levels of attitudes towards ACP. However, current readiness and willingness to engage in ACP appeared low, with over 40% not wanting to make an ACP at all and almost 40% wanting to do so later—findings consistent with prior studies reporting that actual ACP uptake among older adults remains limited despite expressed interest or positive attitudes.32–34 Higher educational levels, prior ACP discussions, and witnessing family members receiving life-sustaining treatments were associated with higher attitude levels and preferences for ACP. Interventions could be tailored to support people with different educational levels, offer recurring ACP discussions, and integrate older adults’ prior caring experiences for family members.
Cultural and religious context influencing ACP in Thailand
Our study revealed a strong association between higher attitudes and preferences towards ACP (adjusted OR = 2.81, 95% CI: 1.45–5.42, p = 0.002). Most older participants recognised ACP’s benefits in facilitating a peaceful death, aligning with predominant Buddhist ideologies in Thailand that view death as a natural and peaceful process.20,35–37 In Thailand, a good death is generally seen as one without suffering or unnecessary life support, occurring naturally after illness, and free from worries due to preparation—such as spiritual readiness and settling family matters.36–38 Dying among loved ones and in a familiar place is also valued.21,38
Due to Thailand’s collectivist, family-oriented culture and traditional paternalism in healthcare, 39 families and physicians often strongly influence medical decisions and may withhold some information from older patients. 40 As seen in our study, older adults also tend to postpone end-of-life choices, preferring to leave decisions to their families and healthcare providers.20,21 This is recognised as a cultural characteristic and common practice in Asia,33,35 but recent studies reported that older adults still wanted to know the complete truths about their illness 36 and be involved in decision-making using ACP, 16 consistent with our findings. In fact, a poor shared decision-making process often leads to suboptimal end-of-life care and psychological and physical burdens on older people and their caregivers.32,41,42 Using ACP, older participants in the current study also perceived it would reduce conflicts and anxiety for family members making end-of-life decisions, protecting the family from emotional, financial, and physical burdens.10,43
Barriers to ACP adoption among older adults
Despite considerable perceived benefits and a desire to have ACP (57.6% of our participants), almost 40% of older participants still wanted to postpone the ACP. We found that those with lower educational levels were significantly less likely to have positive attitudes and preferences regarding ACP, consistent with most literature on ACP engagement. 44 Older adults with lower health literacy—which has been linked to poorer ACP knowledge in existing studies7,45—may also have less favourable attitudes and preferences towards ACP; however, this was not specifically assessed in our study.
Unlike our findings, discussions about ACP were often considered taboo, leading older people, families, and healthcare providers to avoid such discussions.5,10,46 There are prevalent misconceptions that ACP should only be initiated for individuals who are seriously ill and within hospital settings, 35 as well as the belief that signing ACP documents may lead to substandard care. 46 Around one-fifth of older participants in the current study felt hopeless and abandoned by their physicians if offered ACP. An earlier study suggested that most older adults were not willing to abandon their agency but were either unaware of the process of ACP or uncertain of their preferences.11,47,48 However, more than 60% of older participants in our primary settings had CCI > 3, indicating significant health concerns that necessitate end-of-life planning. 49 This older population in primary care settings and their caregivers will inevitably face end-of-life decisions. Tackling misconceptions and uncertainties is paramount to enhancing positive attitudes and engagement in ACP and preventing poor end-of-life care decision-making.7,50
Clinical and research implications
In clinical practice, persistent misconceptions and uncertainties about ACP can be overcome with tailored educational interventions that match patients’ diverse educational backgrounds and by offering repeated opportunities for ACP discussions—approaches shown in our study to foster more positive attitudes and increase uptake. To facilitate busy primary care workflows, clinicians can integrate brief ACP conversations into routine visits (e.g. annual wellness checks or chronic disease management appointments) and use electronic reminders or standardised prompts within patient records to revisit ACP when appropriate.11,51 Designating an ACP coordinator or team member, providing patient information ahead of appointments, and utilising structured tools or checklists can help share the workload and ensure ongoing engagement.11,51
Early integration of palliative care services for older adults diagnosed with life-threatening conditions, including cancers, chronic diseases, dementia, and frailty, is also critical, as palliative care teams can provide relevant information and help develop an ACP for individuals and their families. However, in Thailand, less than 20% of people with palliative care needs receive timely and appropriate consultations, 20 reflecting limited access to palliative care in most low- and middle-income countries. 52 Further research is needed to explore and develop an ACP intervention that is culturally appropriate for the Asian context and healthcare system to promote attitudes and preferences towards ACP.
Strengths and limitations
In this study, we included a considerable number of older participants in primary care settings, enriching our understanding of attitudes and preferences towards ACP among older adults in an Asian context, especially those with multiple comorbidities. However, the study had some limitations that warrant caution when interpreting the data. First, it was a cross-sectional study, so causal relationships could not be inferred. Secondly, we conducted structured interviews rather than using self-administered questionnaires to support older adults with expected cognitive and sensory impairments. However, this may have resulted in social desirability bias, particularly regarding sensitive topics such as ACP and end-of-life care. We also excluded older people who underwent cancer treatment or had an ACP. This might lead to selection bias, so the findings should be interpreted with caution. Future studies may consider including them to further explore the differences. Lastly, attitudes and preferences for ACP among older adults can vary widely, and the quantitative approach in this study might not fully capture these variations. While quantitative research provides an overview and enhances the generalisability of findings, qualitative studies are needed to deepen our understanding and inform future policies and individualised interventions to support and encourage ACP in older adults.
Conclusion
In conclusion, our findings reveal that while most participants had high levels of attitudes towards ACP, there was a significant gap between these attitudes and the willingness to engage in ACP, with many preferring to postpone or avoid it altogether. Factors such as higher education levels, prior ACP discussions, and experiences with family members receiving life-sustaining treatments were associated with more positive attitudes and preferences towards ACP. These findings highlight the need for tailored educational interventions that address common misconceptions, consider varying educational backgrounds, and offer repeated opportunities for ACP discussions. The integration of palliative care services for older adults with life-threatening conditions is crucial but currently limited in Thailand. Future research should focus on developing culturally appropriate ACP interventions that align with Asian healthcare systems and address the unique challenges faced by older adults in this context. Addressing these factors can improve end-of-life care planning and quality of life for older adults in Thailand and similar settings.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251406287 – Supplemental material for Understanding attitudes and preferences towards advance care planning in older adults: Insights from a cross-sectional study in primary care
Supplemental material, sj-docx-1-pcr-10.1177_26323524251406287 for Understanding attitudes and preferences towards advance care planning in older adults: Insights from a cross-sectional study in primary care by Kanthee Anantapong, Pawara Na Rangsee and Thareerat Ananchaisarp in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524251406287 – Supplemental material for Understanding attitudes and preferences towards advance care planning in older adults: Insights from a cross-sectional study in primary care
Supplemental material, sj-docx-2-pcr-10.1177_26323524251406287 for Understanding attitudes and preferences towards advance care planning in older adults: Insights from a cross-sectional study in primary care by Kanthee Anantapong, Pawara Na Rangsee and Thareerat Ananchaisarp in Palliative Care and Social Practice
Supplemental Material
sj-docx-3-pcr-10.1177_26323524251406287 – Supplemental material for Understanding attitudes and preferences towards advance care planning in older adults: Insights from a cross-sectional study in primary care
Supplemental material, sj-docx-3-pcr-10.1177_26323524251406287 for Understanding attitudes and preferences towards advance care planning in older adults: Insights from a cross-sectional study in primary care by Kanthee Anantapong, Pawara Na Rangsee and Thareerat Ananchaisarp in Palliative Care and Social Practice
Supplemental Material
sj-docx-4-pcr-10.1177_26323524251406287 – Supplemental material for Understanding attitudes and preferences towards advance care planning in older adults: Insights from a cross-sectional study in primary care
Supplemental material, sj-docx-4-pcr-10.1177_26323524251406287 for Understanding attitudes and preferences towards advance care planning in older adults: Insights from a cross-sectional study in primary care by Kanthee Anantapong, Pawara Na Rangsee and Thareerat Ananchaisarp in Palliative Care and Social Practice
Footnotes
Acknowledgements
We would like to express our gratitude to all participants for their time and contributions to our study. We also greatly appreciate the assistance of Kittisakdi Choomalee for data analysis.
Correction (March 2026):
This article has been updated to include “Faculty of Medicine” in the authors’ affiliations.
Ethical considerations
This study was approved by the Human Research Ethics Committee (HREC), Faculty of Medicine, Prince of Songkla University (REC 66-094-9-4) on 11 May 2023. Eligible older patients were provided with a participant information sheet in Thai and had the opportunity to discuss any concerns or questions regarding the study.
Consent to participate
Written informed consent was obtained from all participants prior to their inclusion in the study.
Consent for publication
We do not report identifiable information on an individual participant. All participants received information, including the study procedure and publication, and provided written informed consent before they participated in this study.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the Faculty of Medicine, Prince of Songkla University, Thailand. The funder played no role in the study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available at the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.