
Abstract
Objective:
Improve documentation quality of end-of-life family meetings in a tertiary intensive care unit (ICU).
Design:
Before-and-after interventional quality improvement project between October 2018 and February 2020 utilising an electronic pro-forma record.
Setting:
Australian, University affiliated, mixed medical-surgical 22 bed adult ICU.
Participants:
Patients who were admitted to the ICU for active management and subsequently died during that ICU admission. We enrolled 50 patients who died before and 50 patients after the introduction of the electronic family meeting pro-forma record.
Intervention:
Through collaboration with ICU medical and nursing staff, End-of-life Special Interest Group and Clinical Documentation Committee we developed the ICU Family Meeting Discussion Note as an electronic pro-forma record with multiple key fields of entry.
Main outcome measures:
Patient records were examined for the presence of documented details around patient’s admission, family meetings and specific elements surrounding the patient’s death.
Results:
The introduction of a pro-forma record markedly improved the quality of documentation of end-of-life care related family meetings. Documentation increased in recording hospital admission date/time (6% vs 84%), meeting location (14% vs 70%), the reason patients were absent from the meeting (34% vs 72%), the Medical Treatment Decision Maker (MTDM) (10% vs 44%), the patient’s resuscitation status (22% vs 54%), and treatment options discussed (78% vs 94%) (p ⩽ 0.005 for all).
Conclusion:
Introducing an electronic pro-forma record to facilitate family meeting documentation increased the frequency of important recorded information. Further studies are required to assess whether documentation quality improvements are sustainable and whether they affect patient- or relative-centred outcomes.
Introduction
Family meetings are common, occurring regularly during intensive care unit (ICU) admissions. 1 Such meetings are key to improving the understanding, experience and satisfaction of patients and their loved ones and are often used to prepare family for the death of their loved one. 2 Thorough documentation is important for numerous reasons. In addition to being a clinical record with medico-legal implications, it is integral to good clinical management and handover. 3 Well-documented family meetings enable clinicians to carry on the longitudinal conversation with the long stay ICU patient’s family. 4 As critically ill patients are often unconscious, intubated, or possibly delirious, such family meetings are essential to educate loved ones of clinical situations and potential pathways of care moving forward. The meetings may also help bring forth the patient’s health care wishes or advance care plans. 5 In addition, variability in documentation impairs future audits. 6 For all of these reasons, high-quality and consistent documentation is vital.
Anecdotal evidence from our ICU indicated that the rate of documented family meetings was low, and that content was variable and often missing important information. This is not unique to our hospital and has been reported consistently.7,8 Frequency and quality of documentation increases with the introduction of a standardised form.5,9 Any such form that tries to improve documentation would need to be inexpensive as it may be applied to multiple centres, such as using a pro forma record template. In 2010, Nelson et al. 10 reported that the use of a meeting planner and documentation template was associated with improvement in the quality and frequency of family meetings. Furthermore, electronic communication tools have been shown to enhance interdisciplinary collaboration for patients receiving palliative care. 11 Pilot work from the Development of the Serious Illness care programme indicated a dramatic rise in documentation quality before and after the introduction of an electronic medical record (EMR) module. 5
We undertook a quality improvement (QI) project to enhance the quality of documentation of family meetings in our ICU. 12 We hypothesised that an electronic pro forma record coupled with an education programme and periodic reminders would improve the rate of documentation of key information in family meetings of critically ill patients. Our intervention (the pro forma record) was created to capture important details of end-of-life care family meetings in the patient’s EMR. We compared the details of family meeting notes from before and after the introduction of the pro forma record.
Method
Setting
Our hospital is an Australian, University affiliated, mixed medical-surgical 22 bed adult ICU. Specialties include cardiac surgery, neurosurgery, decompensated liver disease, liver transplantation, complex aortic surgery, patients with complex respiratory weaning and patients with acute spinal cord injuries. Documentation at our hospital is a hybrid model with both paper, proprietary intensive care clinical information system and a hospital wide EMR in use. The proprietary intensive care clinical information system is Alarta by Incarta and the EMR software is Millennium PowerChart by Cerner.
Design and phases
The QI project was conducted in our ICU between October 2018 and February 2020. A review of the current literature identified key components of a family meeting. The pro forma record was developed de novo and informed by the literature, senior ICU leadership and hospital committee review to ensure application to our patient population and meeting hospital standards. The first draft, formed from the literature review, was presented to the ICU medical leadership team for feedback and iterative improvement. The draft was then shared at a meeting with the ICU End of Life Care Special Interest group, where suggestions were incorporated. The updated draft was again circulated within the ICU medical leadership team for final approval from clinicians. The pro forma record was then adapted and programmed into the hospital EMR software, Millennium PowerChart, by a Clinical Informatics Analyst (DW). The final form was reviewed by the hospital’s Health Information Services team for medico-legal compliance and approved for use and record by the hospitals Clinical Documentation Committee in May 2019.
The final proforma template (Figure 1) contained fields for details about the patient, the attendees, the meeting location, topics of discussion including resuscitation status before and after the meeting, prognosis, treatment goals and options, questions, conflict, family understanding, and outcomes of the meeting. There were no mandatory fields in the pro forma record. Review of documentation by non-physician practitioners was not included in this QI project.
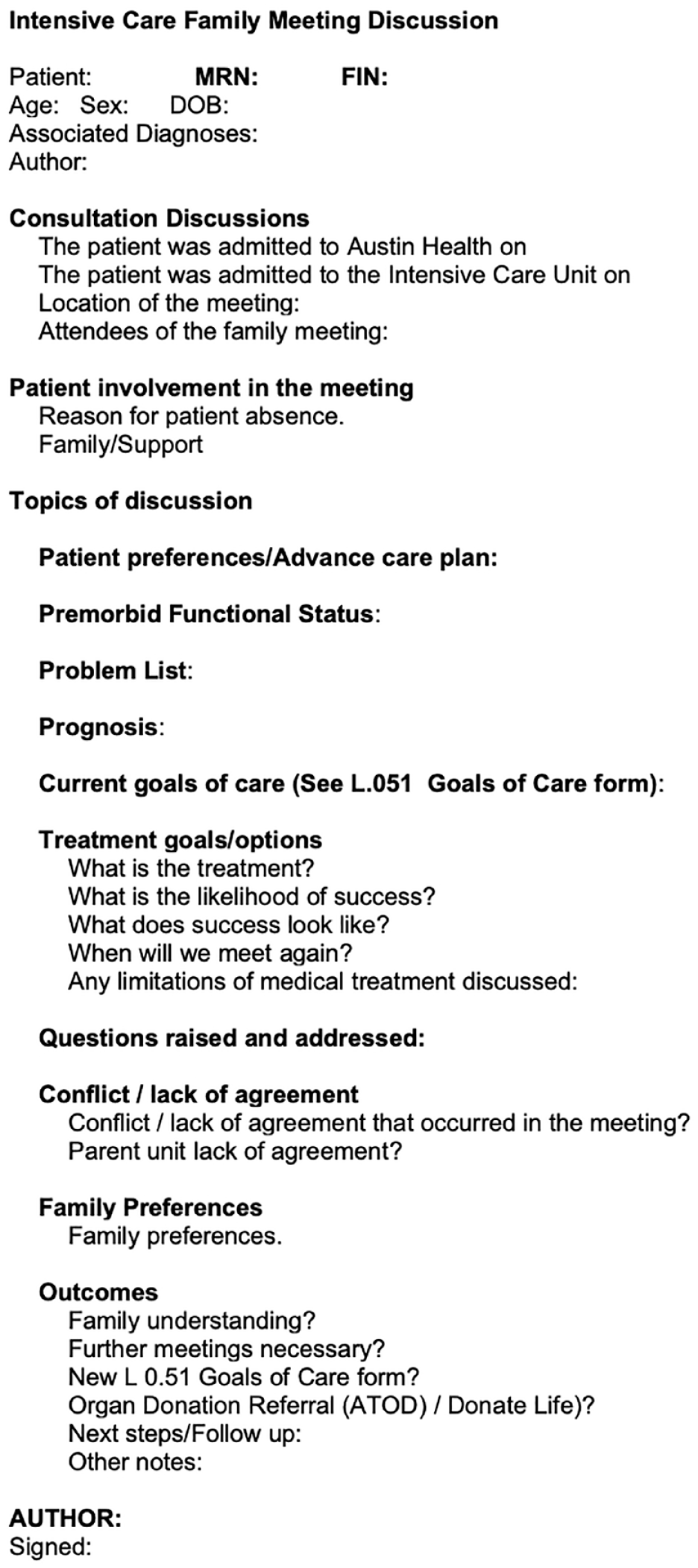
Screen of the electronic standardised pro forma record template, the intervention.
Documentation at baseline
Prior to introduction of the pro forma record, family meetings were documented by the treating intensive care physician. The documentation was non-standardised and freeform, entered in the patients’ medical record wherever the physician deemed appropriate, including hand-written or electronic progress notes. There was no template for this documentation and it occurred after the completion of the family meeting.
Details of intervention
In May 2019, the pro forma record was released to the EMR to help prompt treating clinicians to record salient points from the family meeting with a goal to improve documentation frequency and quality (Figure 1). Education and training on use of the pro forma record was provided to the ICU medical staff. The intensive care physicians were instructed to use the pro forma record in place of their usual documentation method. Documentation was still to be completed after completion of the family meeting. Training was delivered at meetings and medical teaching sessions, and via email to all clinical ICU staff. It was reinforced with periodic reminders, by email and in person. One-page quick reference guides were distributed by email periodically to remind ICU medical staff how to complete the pro forma record. A lead-in time and run-in period of 4 months allowed for training, exposure and new staff to become acquainted with the form. Data collection for patients in the pre-intervention group began in May 2019 and for the post-introduction group in August 2019.
Participants
Eligible patients were any adult patient who was admitted to the ICU for active management and died during that admission. We included a convenience sample of 50 patients in each phase of the QI project. As a pilot, this sample size was chosen based on the anticipated number of eligible patient admissions in a 6-month time period. Patients were excluded if their ICU admission was specifically for end-of-life care.
Eligible patients were audited in a ‘before period’ and ‘after period’. The ‘before period’ was retrospective from May 2019 with sequential identification in reverse chronological order of 50 eligible patients (November 2018 to May 2019). The ‘after period’ included a separate group of 50 eligible patients who were eligible and identified from August 2019 to March 2020 then retrospectively underwent chart review.
Data collection
The data were obtained from first and last meetings recorded in the patient medical record. In instances where there was only one meeting recorded, those details were used. The variables collected are outlined in Figure 1. Data were entered into a data collection form and then collated into a Microsoft Excel (ver. 16.39) spreadsheet by the lead author (AK).
Statistical analysis
Descriptive statistics were performed by an independent investigator (ES) using Stata (MP16.1). Data were analysed as numbers (frequencies), means (standard deviation), and medians (interquartile ranges). Between group comparisons were made by chi squared, unpaired student t or Wilcoxon rank-sum tests, as appropriate. A p value < 0.05 was considered significant.
Results
Baseline Characteristics
Age, primary organ system failure, comorbidities, time to ICU admission and admitting unit are outlined in Table 1. Both groups included patients with a variety of conditions seen in the ICU and a mix of medical and surgical admitting units. The pre- and post-intervention groups were similar aside from an increase in chronic heart failure and median time to ICU admission in the post-intervention group.
Baseline characteristics.
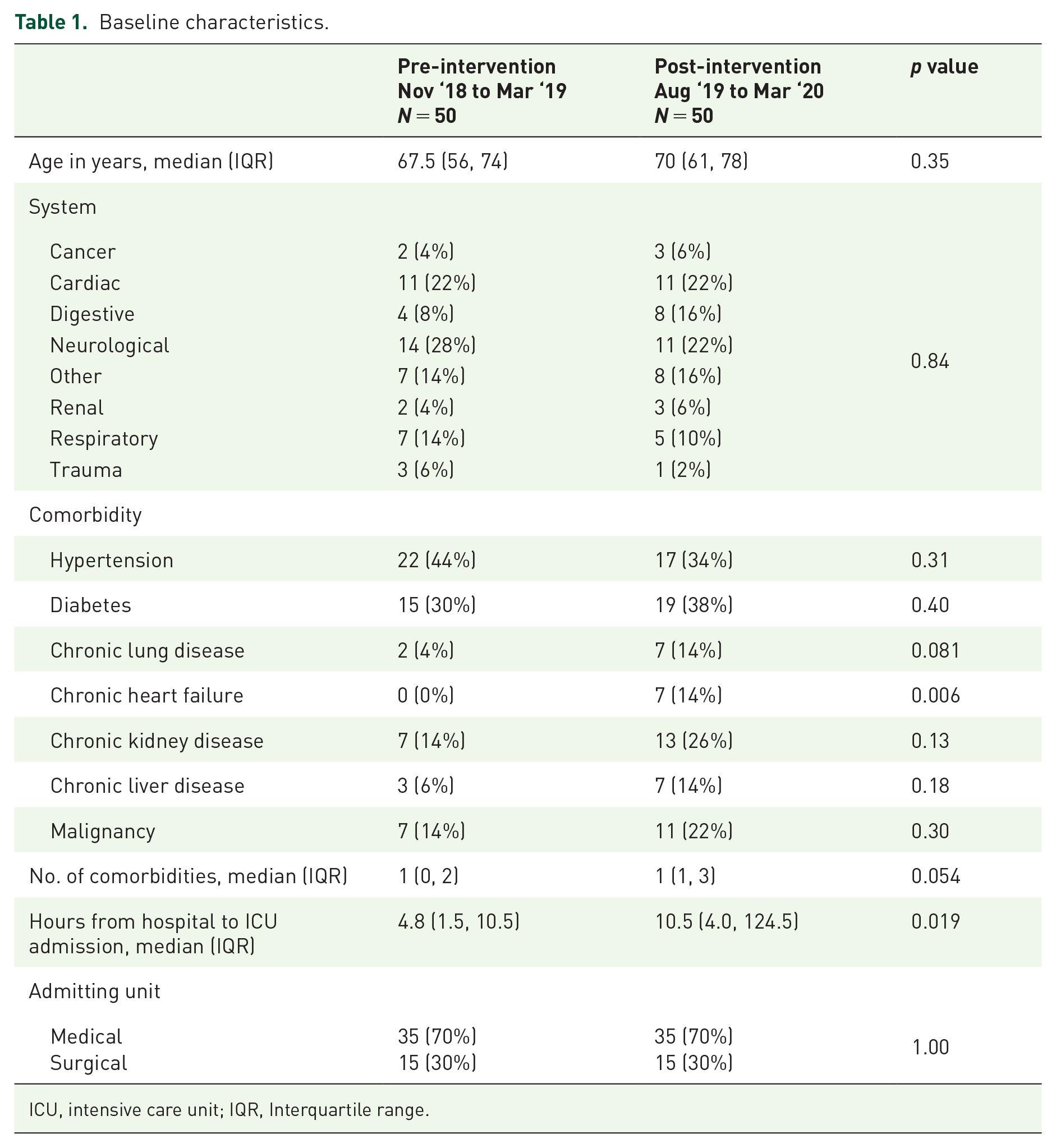
ICU, intensive care unit; IQR, Interquartile range.
Pre-intervention documentation
Key components of documentation were often absent in the pre-intervention period (Table 2). Specifically, hospital admission time and date were recorded 6% of the time, meeting location 14%, reason for the patient’s lack of participation in the meeting was recorded at a rate of 34% and the Medical Treatment Decision Maker was recorded 10% of the time. A patient’s premorbid function was recorded 22% of the time and a patient’s resuscitation status was recorded in 22% of notes examined. Treatment options were recorded 78% of the time and the next steps were recorded 66% of the time. In addition, 68% of notes were recorded in the ICU specific software and 22% were recorded in handwritten notes.
Details of family meeting documentation components.

ICU, intensive care unit; MTDM, Medical Treatment Decision Maker.
Post-intervention documentation
The electronic pro forma record was used 78% of the time compared with 16% recorded elsewhere and 6% with no record (p < 0.001). The intervention was associated with significant improvements (p < 0.001 unless otherwise stated) in where the documentation was recorded, hospital admission date/time, meeting location, the reason that patients were absent from the meeting, the Medical Treatment Decision Maker (MTDM), the patient’s resuscitation status, and treatment options discussed (p = 0.005) (Table 2).
At least one family meeting was documented in both the pre- and post-intervention cohorts in the majority of patients. Among the patients in the pre-intervention group 46 (92%) had a family meeting recorded compared with 47 (94%) in the post-intervention group (p = 0.7).
Documentation of details of deaths that occurred in the ICU
The characteristics surrounding patient deaths was similar in both phases of the QI project (Table 3). No patient in the post-intervention group were classified as ‘for cardiopulmonary resuscitation’ (CPR). Exactly the same proportion were receiving active management and comfort management in both groups. In addition, there was no significant difference in time to instituting comfort care, or to the time from comfort care to death between the two groups.
Resuscitation status and end of life.

CPR, cardiopulmonary resuscitation; ICU, intensive care unit; IQR, Interquartile range.
Documentation in the post-intervention period
Post hoc analysis of the post-intervention group identified a trend towards more thorough documentation with those that used the electronic pro forma record compare with those that did not (Table 4). Significant improvements were observed in the recording of hospital admission date/time (p < 0.001), meeting location (p < 0.001), reason for patient absence (p < 0.001), questions answered (p = 0.04), family preference documentation (p = 0.009) and family understanding documentation (p < 0.001). The patient’s premorbid function was recorded in 69% of notes using the pro forma record compared with 14% using the in-house EMR (p < 0.001). Prognosis was recorded in 97% of pro forma record based notes compared to 86% using the in-house record (p < 0.001). There were trends towards improved documentation in all other categories in the post-intervention group except the ICU admission date/time and the acknowledgement of the presence of a patient’s Advance Care Plan (ACP).
Details of post-intervention group (Aug ‘19 to Mar ‘20) documentation by record location.

ACP, Advance Care Plan; ICU, intensive care unit; MTDM, Medical Treatment Decision Maker.
Discussion
The Australian Commission on Safety and Quality in Health Care has highlighted quality of documentation as a key safety and quality issue. The National Consensus Statement on Essential Elements for Safe High-Quality End of Life Care recommends that ‘Systems should be in place to facilitate appropriate documentation about end of-life care, and to reduce the burden of documentation and data collection when possible’. 3
We conducted a QI project to test the hypothesis that the introduction of a pro forma record increased the capture of key components discussed in family meetings in our ICU. The use of a pro forma record combined with an education and sample training programme was associated with meaningful and statistically significant improvements in the recording of key information discussed in family meetings (Table 2). The use of the electronic pro forma record also trended towards capturing more key components than alternative forms of documentation (Table 4).
Several studies have shown that a template can improve capture of data in documentation which improves qualities of documentation.13,14 This QI project continues the theme that a template improves the quality of key components of documentation in family meetings within a critical care unit. 15 There may be additional education about key elements in a family meeting when physicians use the pro forma record. In this context, repeated use of the pro forma record may act as a prompt to document elements discussed in future meetings or even as a discussion outline.
Of the patients who died during the project period, anticipation of death was documented in 86% and 92% of cases in the pre- and post-period respectively which is consistent with comparable units in Australia (85.7%). 16 In our project, documented family meeting discussions with the family occurred in 92% and 94% of examined records, compared with 90% which Bloomer et al. 16 reported in 2010.
One of the key findings showed a meaningful increase in the recording of the MTDM. This QI project was completed entirely after the commencement of the Medical Treatment Planning and Decisions Act 2016 (Vic) which outlines the legal requirement of searching out MTDMs and ACPs. 17 The family meeting notes using the supplied pro forma record improved documentation of the MTDM and likely enhanced continuity of care for patient care; this potentially ensures better alignment between patient wishes, their documented goals of care and the subsequent clinical course.
Interestingly, although the documentation of resuscitation status was significantly improved with the pro forma record, there was no significant difference between resuscitation status of the patients on arrival to ICU, after the family meeting or at death. It is likely these conversations regarding goals of care were occurring during family meetings throughout the pre and post intervention period, however the documentation of these important measures improved with the pro forma record (Table 2).
Strengths of this QI project include its simplicity and low-cost nature. The generalisability is limited by the use in a single clinical area of a single centre and the short intervention period. Although the documentation is completed by an intensive care physician including a physician in training in our institution, the standardised format of the pro forma record would be amenable to completion by non-physician practitioner. The results only represent a single document with relatively small sample size. We reported minor differences in the baseline characteristics in the two cohorts including a lower average age and frequency of digestive disease in the pre-intervention group. It is unlikely that such differences would have influenced or modified documentation practices or could account for the improved documentation reported.
Further studies need to address whether improved documentation improves patient- or family-centred outcomes, and whether the improved documentation is sustainable. Following this project, further quality improvement cycles will need to be completed with further iteration and refinement of the pro forma record. During the intervention period the pro forma record was solely for use by the ICU department and had not been used by the rest of the hospital. Rollout and education to the rest of the hospital and then other ICUs will need to occur.
In conclusion, we found the implementation of a pro forma record for documenting end-of-life family meetings was associated with improved capture of key components of discussion in the medical record. Post-intervention documentation demonstrated an improvement in certain components of a family meeting note. Further studies are required to assess whether improvements to documentation quality are sustainable and whether there are any impacts to patient- or family-centred outcomes.