
Abstract
The zygomatic bone’s lateral prominence and convexity make it the most important bone to provide aesthetic facial appearance and set the face width, but at the same time, this prominence and convexity make this bone more susceptible to injury. Among facial injuries, zygomatic-complex fractures or tripod fractures are the second most common fractures after nasal fractures. This study has performed a comparative assessment of fixation of zygomatic buttress by L and Z shaped plate. Fourteen zygomatic-complex fracture patients were selected and split into two groups, further divided into two subgroups (A, B). Group A patients were treated with a titanium Z shaped plate and Group B with L shape plate. One point fixation was performed and was observed in terms of stability, aesthetics and prevention of vertical or horizontal axis of rotation of the fracture segment. Z-shaped plates showed some advantage over L-shaped plates so there use can be preferred in complex fractures where comminuted bone pieces are scattered.
Introduction
The face is more prone to injury as it is the most noticeable part of body. Most of the impact of injuries on the face is borne by the malar region because of its prominence. The second most common mid-facial bone to fracture is ZMC, after the nasal bones and overall represents 45% of all midface fractures. 1 However, the incidence and aetiology of this fracture differ. According to some books, the main cause of zygomatic bone fracture is road accidents. These fractures are initially treated for function and aesthetics based on their site and severity along with considering other injuries and condition of patient. Zygomatico-maxillary complex bone can withstand greater force without being fractured and on experiencing heavy force gets separated away from the nearest bone or nearby suture line. Buttresses after being disrupted by the force of the external injury and the pull of the muscle, get rotated around horizontal and vertical axis. Many implant systems are present for treating mid-facial fractures like 1.0, 1.3, 1.5, and 2.0 mm mini plates. 2 Miniplates are found to be more efficient in stabilising the bone of the midface with nominal complication. 3 However, two to three screws per fragment cannot be placed in the zygomatic buttress as the amount of bone is not adequate. More surgical exposure is required for two plating systems and more tissue retraction which can cause infra-orbital nerve injury. To overcome this problem, various plate designs have been put forward. 4 A single L, Y, Z plate has been used in the treatment of zygomatic-complex fractures, which confirms the tensile stress pattern at the buttress region. L and Z shaped plate design address a large fracture zone and are adjustable to fit with the anatomy of zygomatic-complex.
Methodology
A randomised clinical study was done in the oral and maxillofacial surgery department after getting ethical approval from ethical committee with SVIEC/ON/DENT/BNPG18/D19028.
A study was done to evaluate stability, surgeons opinions on Z plate and L plate in midface fracture. Preoperative photos and 3DCT with face reconstruction were taken and assessed for treatment planning for Group A (Figures 1 and 2) and Group B (Figures 3 and 4). Pre-operative occlusion was also assessed in Group A (Figure 5) and Group B (Figure 6). Patients were operated under general anaesthesia/local anaesthesia, following standard aseptic protocols. Traditional maxillary vestibular incision was used to approach the midface. After gaining the proper access to the fracture site, reducing the fracture fragments in proper position and obtaining the occlusion state which was present before trauma, fixation was performed. Internal fixation was performed at ZMB, using L plate for Group A (Figure 7) and Z plate for Group B (Figure 8). Intra-oral closure was done with resorbable sutures. All patients were given intravenous antibiotics and analgesics. A post-operative PNS was taken to confirm reduction of fracture segment in Group A (Figure 9) and Group B (Figure 10). Post-operative occlusion was assessed on day 1 in Group A (Figure 11) and Group B (Figure 12). Post-operative pain, paraesthesia, mouth opening, plate fracture, and salivary fistula were checked on 1st, 3rd, 7th, 15th day and 1 month.
Group A-L Plate; Preoperative Profile Photo.

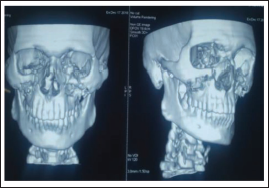
Group A-L Plate; Pre-operative Ct-scan.
Group B-Z Plate. Preoperative Profile Photo.

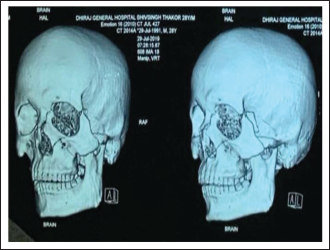
Group B-Z Plate. Pre-operative CT-scan.
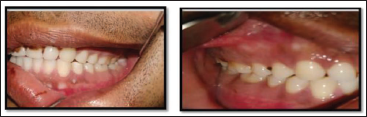
Group A-L Plate; Pre-operative Occlusion.

Group B-Z Plate. Pre-operative Occlusion.
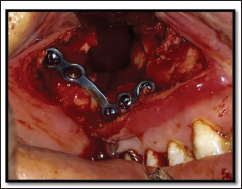
Group A-L Plate; Intra-operative Photo.
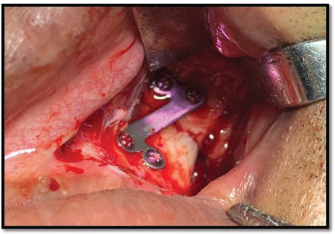
Group B-Z Plate. Intra-operative Photograph–Z Shape Plate.
Group A-L Plate; Post-operative Radiograph.

Group B-Z Plate. Post OP Radiograph.

Group A-L Plate; Post-operative Occlusion.

Group B-Z Plate. Post-operative Occlusion.

Results
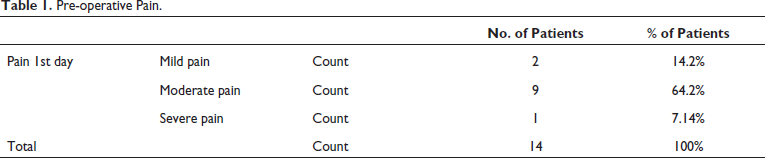
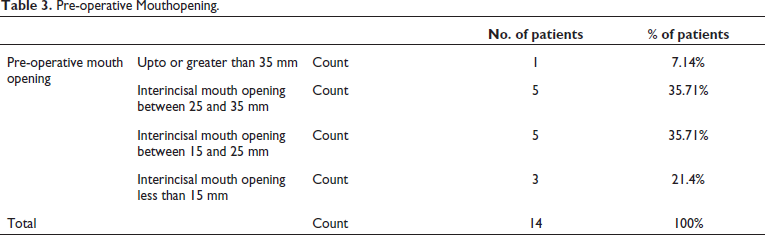
Preoperative pain (Table 1) and occlusion (Table 2) was checked. Preoperative mouth opening was recorded as more than 35 mm in 7.14%, 25-35 mm in 35.71% of cases followed by 15-25 mm in 35.71% and less than 15 mm in 21% (Table 3).
Pre-operative Pain.
Pre-operative Occlusion.

Pre-operative Mouthopening.
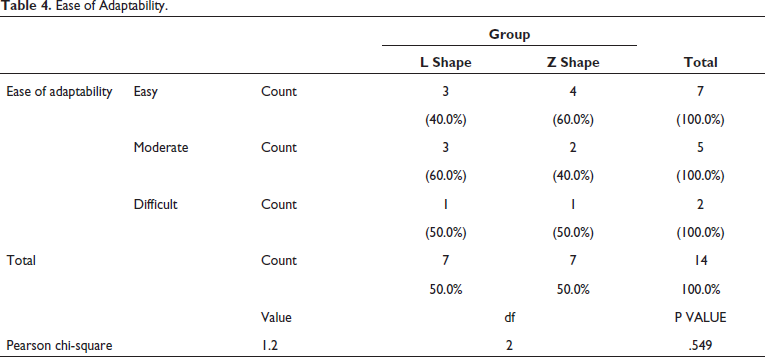
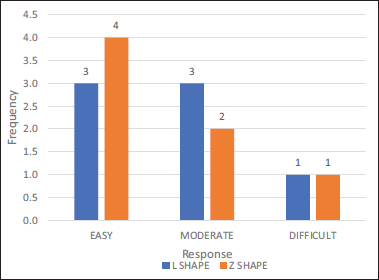
The adaptability of a plate of Group A was difficult in one patient and was moderately easy in three patients and easy to adapt in three patients out of seven. Whereas, it was difficult in one patient moderately easy in two patients and easy in four of the patients out of seven of Group B (Table 4, Figure 13).
Ease of Adaptability.
Ease of Adaptability.
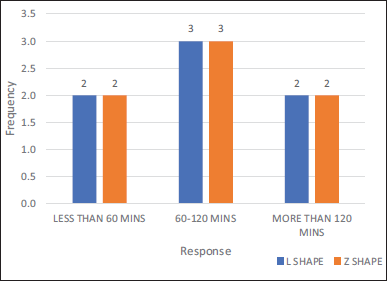
Total time taken was counted from the time of incision till the closure of fracture site. Which was less than 60 min in two patients, of about 60-120 min in three patient and more than 120 min in two patients of Group A. Whereas the total time taken in surgery was less than 60 min in two patients, about 60-120 mins in three patients and more than 120 min in two patients of Group B. Thus, no significant change in ease of adaptability was seen (Table 5, Figure 14).
Time Taken for Surgery.
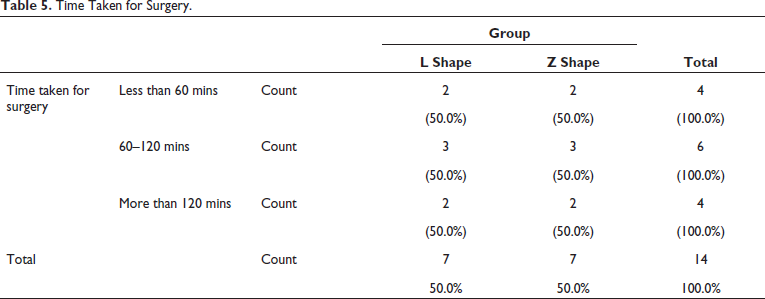
Time Taken for Surgery.
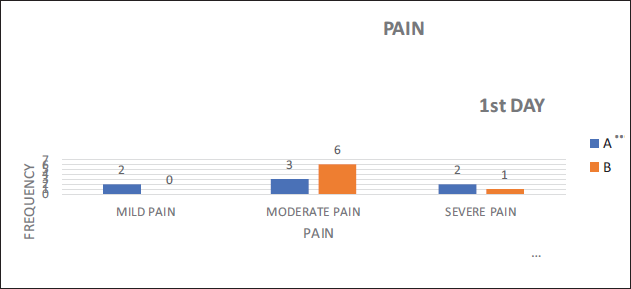
Post-operative pain on 1st day of Group A, two patients had mild pain, three patients had moderate pain, two patients had severe pain. Whereas on POD 1 of Group B, six patients had moderate pain and one had severe pain (Table 6, Figure 15). Pain on POD 30 of Group A was four patients had no pain, three patients had mild pain. For Group B six patients had no pain and one patient had mild pain (Table 7, Figure 16).
Post-operative Analysis. Pain on POD 1.
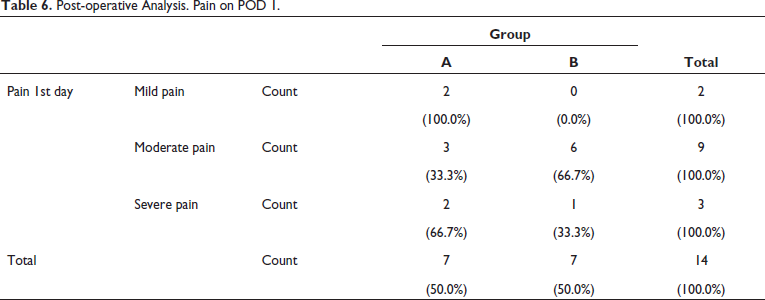
Pain on POD 1.
Pain POD 30.
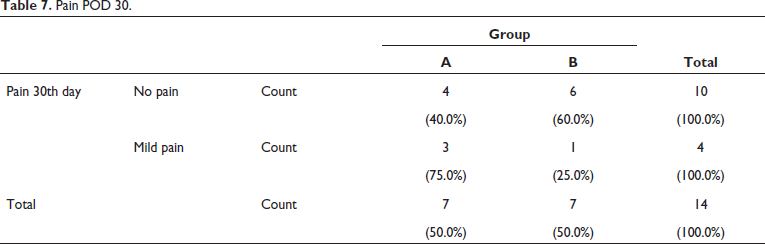
Pain on POD 30.
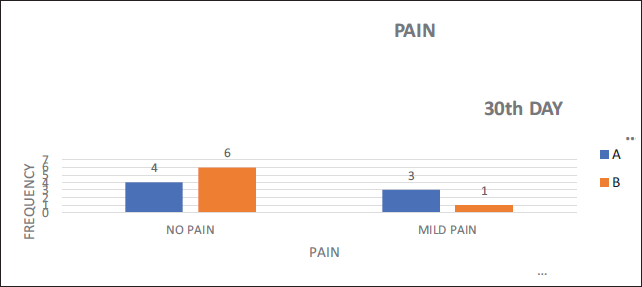
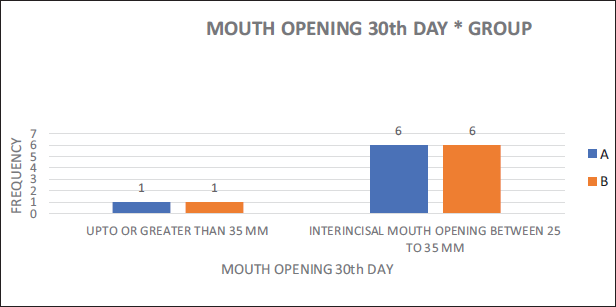
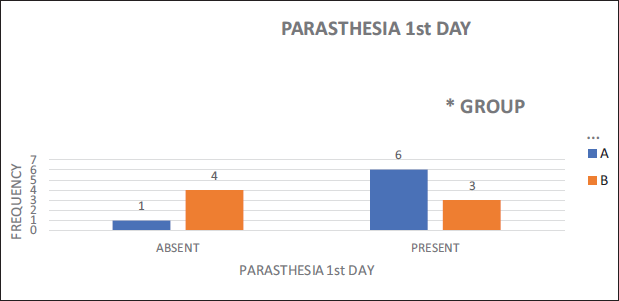
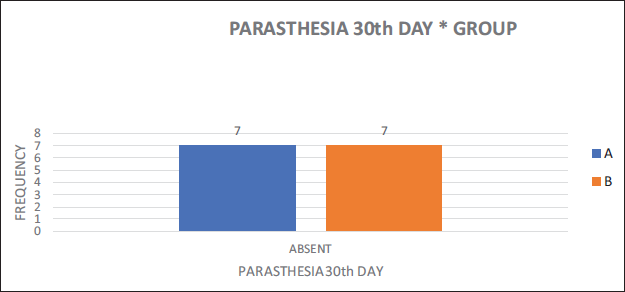
Mouth opening on POD 1 in 3 patients had a mouth opening of 25-35 mm and four patients had 15-25 mm of Group A. whereas 5 patients had 25-35 mm mouth opening and two patients had 15-25 mm mouth opening in Group B (Figure 17). Mouth opening on POD 30 1 patient had mouth opening more than 35 mm and six patients had 25-35 mm mouth opening of the Group A. In Group B one patient had mouth opening up to 35 mm and six patients had 25-35 mm mouth opening of Group B (Figure 18). Paraesthesia on POD 1 (Figure 19) and POD 30 (Figure 20) was also assessed.
Mouth Opening on 1st Day Postoperatively.
Mouth Opening on 30th Day Postoperatively.
Paraesthesia on Post-operative Day 1.
Paraesthesia on Post-operative Day 30.
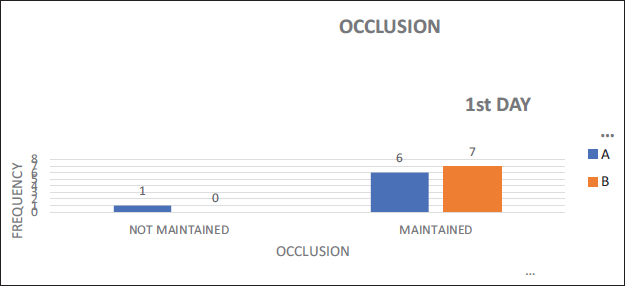
Post-operative occlusion was maintained in 46.2% of Group A and 53.85% of Group B out of total on day 1 (Table 8, Figure 21) and 100% of patient’s occlusion was maintained on 30th day in both groups (Table 9, Figure 22).
Occlusion on POD 1.
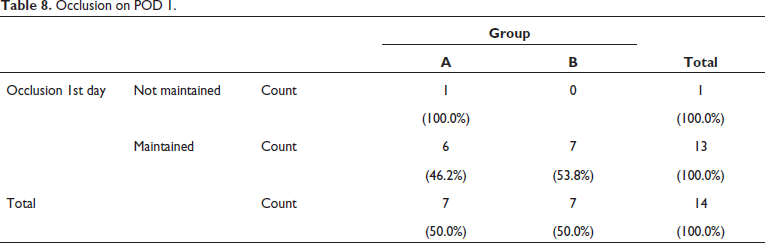
Occlusion on POD 1.
Occlusion POD 30.
Occlusion on POD 30.
Discussion
The union of the zygoma, affects a great deal of the face’s functional and cosmetic features. Due to its prominence, it cannot withstand the force of facial traumas. Fixation on the zygomatic fracture requires taking into account buttresses of face, because rebuilding these structures is one of its main objectives. The naso-maxillary buttress (medial buttress), the pterygo-maxillary (posterior buttress), which connect the maxilla posteriorly to the sphenoid bone and the lateral or zygomatico-maxillary (ZM) buttress come into play in ZMC fractures. The ZM buttress is important as it connects the zygomatic process of the temporal bone by the lateral maxillary alveolus.
These buttresses provide structural stability so that they can tolerate forces. 5 According to Jain et al., incidence of ZMC fractures differs depending on socioeconomic trends, geographical location, incidence of road traffic accidents (RTAs), abuse of alcohol and drugs. According to various literature, the 2nd most common fractures of the face are ZMC fractures. 6 Wu CM et al. said that due to the significant influence of malar prominence on facial aesthetics, management of zygoma fractures is essential clinically. Conventionally most maxillofacial surgeons have used plates and screws of titanium for osteosynthesis to get a rigid fixation, although there are not many drawbacks to this technique, some of the disadvantages are implant exposure, loosening of the screws, pain, irritation, sensitisation of temperature. 7 Surgical therapy is not needed if fractures are un-displaced and without functional disturbances. Damage or impingement of infra-orbital nerve in complex fractures, results in either temporary or permanent neurological impairment. This dislocated bony fragment requires surgical correction. An impaired coronoid function may be result of fractured zygomatic arch that moves medially, further reducing mouth’s opening. Thus, such cases require open or closed reduction of the fracture fragments. 8 Surgical treatment is not advised if the fracture fragments are minimally displaced or if no displacement is seen. Also, in patients with or without health issues, conservative management is preferred over surgical procedures. Some patients may adhere to conservative management and prefer to have some minor facial deformity which may be permanent. 9 If there is bone fragment movement, instability or comminution, surgical intervention is necessary. The main goals of treatment are precise anatomic reduction of the fracture segments with proper fixation. According to Marinho R et al. FZS and ZMB are important areas for fixation of complex fractures because they are needed for rebuilding the midface’s vertical and horizontal buttresses. Further, if fracture still remains unstable and additional fixation is needed infra-orbital rim and/or the zygomatic arch are used as fixation points. 9 Kim et al. show that one-point fixation has the advantage of taking less time to complete the surgery than multiple-plate fixation and does not involve extra skin incisions that may leave scars. Here, we report the outcomes of our surgery by one-point fixation at the ZM buttress in patients who had ZMC fractures but no comminuted lateral orbital rim fracture. 10 Bradley D et al. in their study suggests that the ZM buttress has been a preferred choice for one-point fixation, while others suggest FZ suture as their primary choice. According to some studies, in any displaced ZMC fracture the fixation of both the IOR and FZ is recommended. If the displacement is more than 5 mm fixation by three points is advised. 6 Ellis et al. show that when there is zygomatic-complex fracture, fixation at zygomatic buttress gives a significant mechanical advantage for stabilising the fracture fragment by avoiding medial rotation of complex into the maxillary sinus. 11 Fujioka et al. showed that fixation by one point gives three-point alignment and stable fixation in non-comminuted fractures. 8 In Tripathi N et al. study he suggests following only one point fixation either at zygomatic buttress or at fronto-zygomatic suture. He observed that the zygomatic buttress directly opposes the pull of the masseter muscle, hence it is regarded as one of the ideal sites for fixation. In ZMC fracture, the fronto-zygomatic suture has thick bone and thus becomes a good site for fixation. 12
Out of 14 cases that underwent ORIF one point fixation was performed in most patients (n = 8) 57.1%. Two-point fixation was performed in (n = 5) 35.71% of the patients and three-point fixation was done in 7.14% (n = 1). Among all the cases performed in our institute one point fixation, was done at ZM buttress region. According to literature, the Z-M buttress is the primary choice for one-point fixation which provides sufficient stability without the need for fixation at F-Z and a similar result was seen in our study.
Demographic data in our study showed that 30 years is the mean age for ZMC fractures and all 14 patients were male. Hence the incidence is higher in men with respect to women. According to Bradley et al. men are more likely than women to have ZMC fractures, which often occur in the 3rd decade of life. 6 According to Punjabi et al. the most frequent cause of zygomatic bone fractures was RTAs, which accounted for 50%. Other prevalent causes were assault (23.17%), fall (20.73%), sports injuries (3.65%), and others (2.43%). A little more on the right side (55%) than the left (45%) was implicated. 13 Every patient in our study had a history of traffic accidents as their aetiology. Before surgery, we assessed all of the patients for mouth opening, occlusion, discomfort, and paraesthesia. The pain was analysed using the VAS score given by Sirintawat N et al. 14 which shows 21.47% patients had mild pain, 64.2% had moderate pain and 14.2% patients had severe pain preoperatively. The pre-operative occlusion was not maintained in 50% patients and 50% patients came with occlusion maintained were included in our study. 15 Borba et al. suggested that fracture itself and surgery for its correction have a negative effect on mouth opening range; however, the capacity of mouth opening presents signs of recovery since the first post-operative week, with notable progression until one month after surgery. So, in our study also mouth opening of the patients of both groups has been increased over follow-up days.
Noor M et al. aid that nerve injury following fracture may present with various pathophysiology involving traction, pressure, ischaemia, inflammation and physical damage of the infra-orbital nerve resulting in sensory neuropathy as a post-operative complication. 16 There was no case of plate fracture and infection in either of the two groups of our study. The patients of both groups did not complain of mobility of plate or segmental mobility of the fracture.
Conclusion
Internal fixation is always preferred treatment for displaced ZMC fractures. We conclude from this study that there were no significant issues with Z and L plate groups experiencing almost similar results. The outcomes of both plates are trustworthy for isolated, non-comminuted zygomatic fractures, and they might be utilized as an additional optional fixation method for zygomatic fractures. In certain situations Z-shaped plates showed some advantage over L-shaped plates, due to there Z structure and anatomic adaptability, and so were used in complex fractures where bone pieces are scattered or comminuted. However, to identify and fully comment on advantages, challenges and disadvantages of Z plate, a larger sample size and longer follow-up is necessary.
Footnotes
Acknowledgement
The authors would like to thank Dr. Gulam Naviwala for his comments, insightful suggestions and careful reading of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.