
Abstract
In the modern era, the management of fractures is often done by open reduction and internal fixation. The open reduction essentially involves the use of incisions for the exposure of fractured segments followed by reduction and internal fixation. It is not uncommon to find deep lacerations in a trauma setting. These lacerations can be used to one’s advantage (boon) for fracture management and can avoid the need for separate incisions. The purpose of this case report is to present the management of zygomatic complex fracture by utilizing deep lacerations.
Introduction
Soft tissue injuries involving the face are commonly encountered during the management of trauma patients. These injuries may be minimal, leading to the involvement of superficial soft tissue structures, or may be severe enough to involve deeper structures including the facial bones. Various soft tissue wounds can be broadly categorized as abrasions, contusions, lacerations, bite wounds, various degrees of burns, and soft tissue avulsion. 1 The basic rationale behind early soft tissue repair is to close the wound so as to restore tissue integrity and prevent microbial penetration to deeper layers. The purpose of this case report is to present the management of zygomatic complex fracture by utilizing deep lacerations. We did two-staged management of facial lacerations without violating the principles of wound management.
Case Report
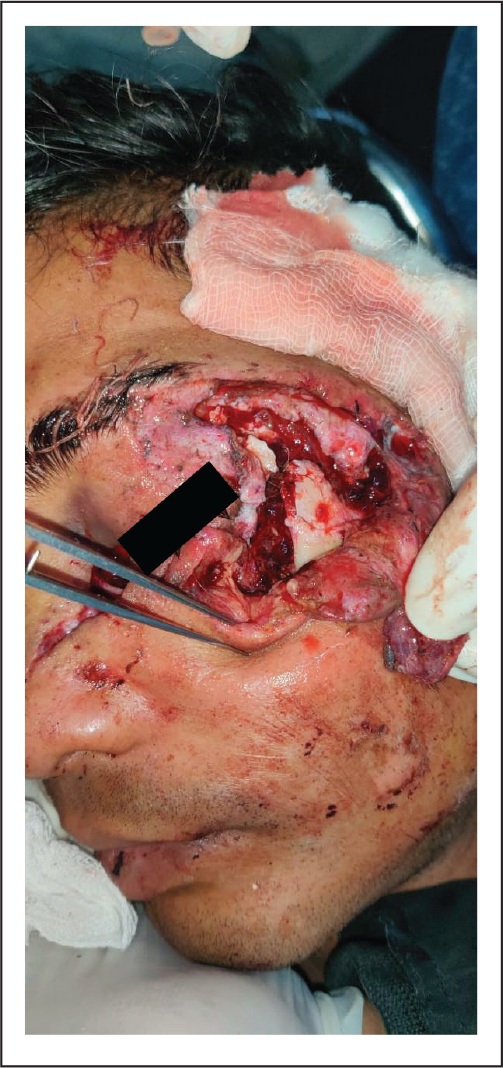
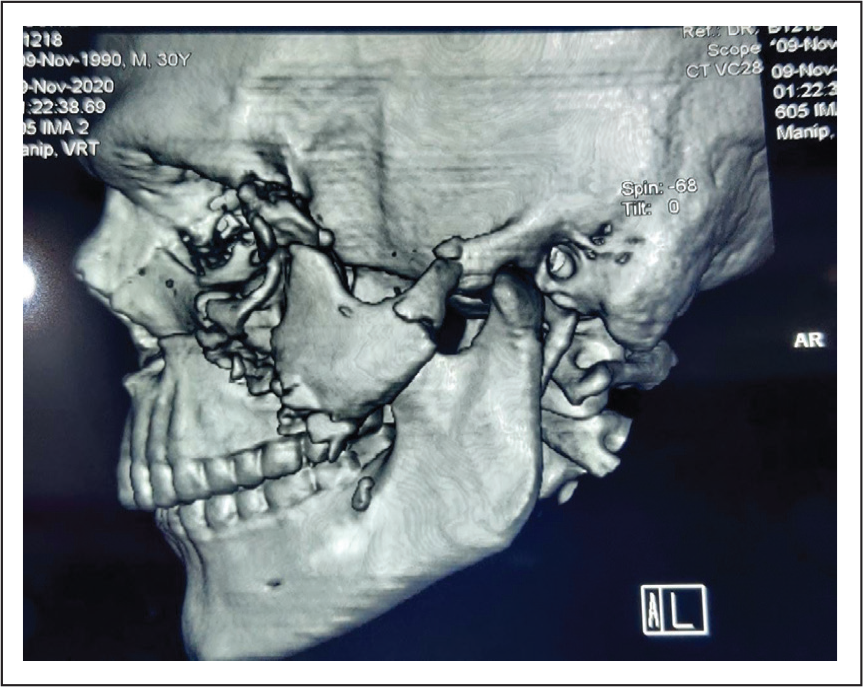
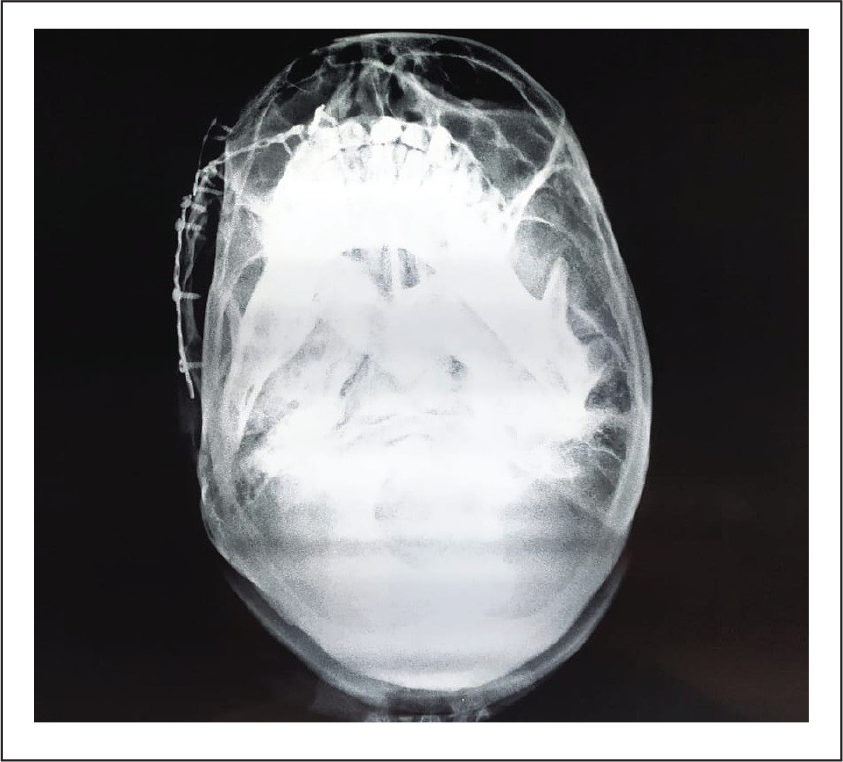
A patient reported to our Department of Oral and Maxillofacial Surgery with facial injuries. There was a history of trauma to the facial area in a road traffic accident that occurred a few hours back. On clinical examination, there were deep lacerations to the face, leading to exposure of the underlying fractured skeleton (Figure 1). A computed tomography scan of the patient revealed the fracture of the left zygomatic complex (Figure 2). It was planned to use these deep lacerations for fracture management. Therefore, after wound debridement and cleaning, temporary sutures were placed to close the wound without much emphasis on layer-wise closure. Antibiotics and anti-inflammatory drugs were started to prevent infection and decrease inflammation. Once the edema subsided, the definitive management of zygomatic complex fracture was done under general anesthesia. The extraoral wound was reopened and the fractured segments were reduced, followed by an internal fixation using miniplates. This is followed by layer-wise closure of the wound using vicryl sutures for deep layers and prolene sutures for skin closure (Figure 3). The postoperative radiographs were taken the next day to check for reduction of fractured segments (Figure 4).
Preoperative Photograph Showing Deep Laceration With Exposure of Underlying Fractured Bones.
Preoperative CT-Scan Showing Comminuted Fracture of Zygomatic Complex.
Postoperative Photograph Showing Closure of Lacerated Wound After Fracture Management.

Postoperative Radiograph Showing Fixation of Fractures by Using Miniplates.
Discussion
Wounds can be divided into 2 basic groups: clean wounds and contaminated wounds. The probability of wound contamination and chances of infection increases considerably with the increase in length of time after the injury. Wound contamination is usually caused by streptococci or staphylococci on the skin of the face and by additional multiple microorganisms in case of intraoral wounds. Wounds involving oral cavity or through-and-through lacerations of the face to involve oral cavity should be regarded as contaminated. 2 Lacerations may be clean or contaminated. They may have well-defined regular margins or contused and ragged margins. The lacerations should be carefully examined, debrided, and thoroughly cleaned followed by a layer-wise closure. 1
The management of soft tissue wounds is usually accompanied by primary closure as early as possible, preferably within the “golden period.” The “golden period” may be regarded as a time ranging from 6 to 24 h after injury. Early wound repair within the “golden period” is recommended for optimal results. 3 However, few clinicians have recommended that the decision to perform primary closure should be based on the mechanism and circumstances of the injury, the time elapsed since the injury, and the degree of contamination. 4
Whenever a trauma victim reports to an emergency setting, the patient is usually in great distress and pain. The definitive management of the patient is usually not possible under local anesthesia. After following the ABCDE parameters of advanced trauma life support protocols (ATLS-Protocols), emergency procedures are performed. Soft tissue injuries are addressed, and fractured skeletons are temporarily stabilized. The definitive treatment is done at a later time in a more controlled environment, usually under general anesthesia. In our case, we had done the temporary primary closure of the wound in an emergency trauma setting within the “golden period” so as to restore tissue integrity and decrease microbial contamination. The basic idea is to explore the same laceration for the management of the fractured skeleton at a later time. The definitive management and layer-wise closure of the wound was done at the time of ORIF of fractures under general anesthesia. We advocate following this two-staged protocol of wound management in case of deep lacerations so as to avoid additional incisions and to do a definitive repair of the wound in a more controlled environment under general anesthesia.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.