
Abstract
Achieving optimum pain control and anesthesia in maxillofacial fracture trauma individuals will be difficult in some scenarios because of change in position of landmarks due to fracture, trismus, and noncompliant nature of patient due to pain. We did a comparative evaluation of efficiency of inferior alveolar nerve block (IANB) and Vazirani-Akinosi closed mouth nerve block technique to anesthetize the inferior alveolar nerve in trauma patients with trismus and concluded that IANB is superior to Vazirani-Akinosi in terms of onset and efficacy but its application in trauma patients with reduced mouth opening is limited and Vazirani-Akinosi will be the technique of choice in case of such scenarios.
Keywords
Introduction
Maxillofacial fractures can be isolated or associated with complex poly trauma, leading cause of it is road traffic accidents. According to the report published by Road Safety in India, polytrauma comprises of 13.3% of all adult trauma cases. Literature review suggests that isolated maxillofacial fractures account for 37.3% of polytrauma cases.
Current standard approach for managing fractures of maxillofacial area is open reduction and internal fixation with plating and screw fixation.
Achieving optimum pain control and anesthesia in maxillofacial fracture trauma individuals will be difficult in some scenarios because of change in position of landmarks due to fracture, trismus, and noncompliant nature of patient due to pain.
Aim
To evaluate and compare the efficiency of inferior alveolar nerve block (IANB) and Vazirani-Akinosi closed mouth nerve block technique to anesthetize the inferior alveolar nerve in trauma patients with trismus.
Materials and Methods
This study was conducted on maxillofacial trauma patients reported to oral and maxillofacial surgery unit of trauma center of our institution, irrespective of gender, age, and ethnicity, after obtaining proper consent.
This study comprises of 5 patients with maxillofacial trauma who underwent intermaxillary fixation under local anesthesia.
Inclusion Criteria
Patients with isolated maxillofacial injury having trismus because of fracture.
Willing to participate in the study.
Exclusion Criteria
Infection in the site of injection.
Neurologically unstable individual.
Individuals who are medically compromised.
Clinical Picture Depicting Vazirani-Akinosi Nerve Block Technique.

Five patients with B/L mandibular fracture were chosen and each patient was in their own control. Under proper aseptic conditions, IANB using Halsted approach (Figure 2) was given over right side of mandible and Vazirani-Akinosi closed mouth mandibular nerve block technique (Figure 1) was opted for left side.
Time of onset of anesthesia, patients compliance while injecting local anesthesia, and ease of injecting anesthesia by surgeon were assessed for each patient and recorded.
Clinical Picture Depicting Inferior Alveolar Nerve Block Technique.

Results
Results of the Study.
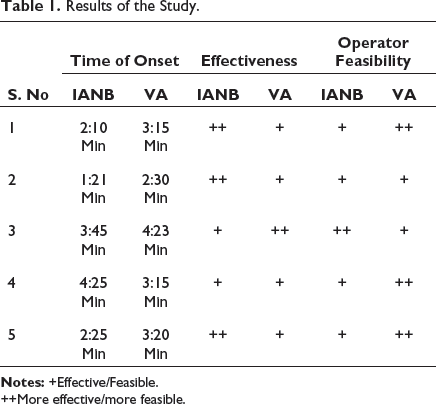
++More effective/more feasible.
Following conclusion can be drawn from Table 1:
IANB is effective compared to Vazirani-Akinosi in anesthetizing inferior alveolar nerve but operator feasibility while administering block is more for Vazirani-Akinosi than IANB due to reduced mouth opening caused by fractured mandible.
Discussion
Trismus in maxillofacial fractures is a common clinical presentation posing difficulty in injecting local anesthesia to block inferior alveolar nerve.
Causes of trismus can be as follows:
Fractured bony segments preventing jaw movements Muscle spasm Posttraumatic swelling and/or hematoma Impingement of zygomatic arch over coronoid process
Some of the accepted techniques to block IANB include intraoral approaches like standard inferior nerve block technique using Halsted approach, Vazirani-Akinosi technique, Gow-Gates technique, Fischer 123 technique; extra oral approach of mandibular nerve block and Kurt Thoma technique. 1
Halsted approach is more acceptable among many contemporaries because of its ease in identification of landmarks, optimum onset time, and clinically acceptable results but its application in trauma patients with trismus will be limited because it requires wide mouth opening.
Vazirani-Akinosi closed mouth mandibular nerve block can be opted in these patients as it can be employed even in case of restricted mouth opening due to trauma.
Both the techniques mainly differ in the area of needle insertion and region anesthetized.
Conventional technique:
Area of insertion: The needle insertion point lies three-fourths of the anteroposterior distance from the coronoid notch back to the deepest part of the pterygomandibular raphe aiming from the contralateral side premolars to a depth of 20 to 25 mm through pterygomandibular space “until needle contacts the bone”, 6 to 10 mm superior to occlusal plane of mandible.
2
Areas anesthetized: Inferior alveolar, a branch of the posterior division of the mandibular division of the trigeminal nerve (V3) Incisive Mental Lingual (commonly)
Vazirani-Akinosi technique:
Area of insertion: Soft tissue overlying the medial (lingual) border of the mandibular ramus directly adjacent to the maxillary tuberosity at the height of the mucogingival junction adjacent to the maxillary third molar to a depth of 25 mm into soft tissue.
3
Areas anesthetized: Inferior alveolar, a branch of the posterior division of the mandibular division of the trigeminal nerve (V3) Incisive Mental Lingual Mylohyoid
Based on the observations from the study, following statements can be derived:
Vazirani-Akinosi outweighs conventional technique in its application in case of individuals having trismus but its failure rate is considerably high due to its arbitrary depth of penetration as it doesn’t involve bony contact of needle. Delayed time of onset and less overall subjective effectiveness of anesthesia following Vazirani-Akinois technique was observed. Conventional technique can be supplemented with a prior Vazirani-Akinosi technique as the closed mouth technique will help in receiving muscle spasm leading to slight increase in mouth opening after which IANB can be given to get optimum results.
Review of literature:
Literature shows contrary views according to the clinical results and aesthetic efficiency of conventional block and Vazirani-Akasoni.
Yücel and Hutchison 4 did a comparative evaluation of conventional block and closed block technique and concluded that direct technique is more effective in blocking IANB than closed mouth technique but stated that closed mouth technique can be a successful alternative in individuals with trismus.
Moreover, literature review on comparative study of Vazirani-Akinosi and IANB and results showed that VaziraniAkinosa is not effective as conventional technique but its advantage in reducing the need of second injection to block buccal nerve has been highlighted.
Mohammad Zahir Kota et al 5 in his study concluded that Vazirani-Akinosi has efficacy same as that of classical IANB and emphasized its strong clinical application in case of limited mouth opening and apprehensive patients.
Literature review shows a gradual change in trend favoring Vazirani-Akinosi in recent years.6 This can be due to adaption of this technique in educational institutions by dental practitioners and increased knowledge about anatomy and landmarks.
Conclusions
Each technique is having its pros and cons but according to the results from this study, conventional IANB is superior to Vazirani-Akinosi in terms of onset and efficacy but its application in trauma patients with reduced mouth opening is difficult. Vazirani-Akinosi will be technique of choice in case of such scenarios where it can be made effective by proper identification of ramal flare in experienced hands or by using it as a supplemental anesthesia.
Footnotes
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.