
Abstract
Oromandibular dystonia (OMD) can be described as a focal dystonia which is characterized by repetitive or sustained contraction of various muscles of mastication, tongue, or face resulting in involuntary jaw opening, closing, deflection, retrusion, or a combination of these. Various abnormal movements like tremor, tics, Parkinsonism, chorea, and dystonia may be seen in patients with traumatic brain injury. Tremor and dystonia are the most common movement disorder seen in such cases. The purpose of this presentation is to report a case of posttraumatic OMD in a head injury patient successfully managed by the use of Botulinum Toxin Type-A.
Introduction
Dystonia is characterized by involuntary muscle contractions, which leads to rhythmic and atypical movement of various parts of the body. Dystonia can be categorized as focal, segmental, multifocal, and generalized depending on the anatomical localization. It can be further classified as primary or secondary dystonia based on the etiological factor. Primary dystonia is idiopathic or inherited or familial. Whereas, secondary dystonia is due to an etiological factor such as trauma, surgery, head injury, and medications. 1
The dystonia that involves the oral cavity is called as oromandibular dystonia (OMD). OMD can be described as a focal dystonia which is characterized by repetitive or sustained contraction of various muscles of mastication, tongue, or face resulting in involuntary jaw opening, closing, deflection, retrusion, or a combination of these. 2 The purpose of this presentation is to report a case of posttraumatic OMD in a head injury patient successfully managed by use of botulinum toxin type-A (BTX-A).
Case Report
A patient reported to our Department of Oral & Maxillofacial Surgery with the chief complaint of repetitive and sustained mouth opening since 15 days. As per the history given by patient’s caretaker, the patient had a traumatic episode (fall from height) leading to head injury 3 months back. The patient was taken to a regional trauma centre where patient was diagnosed to have intracranial hematoma and had undergone temporoparietal craniotomy to evacuate hematoma. The patient remained unconscious for 10 days approximately. After a prolonged hospital stay, patient regained consciousness but did not regain full bodily functions. At the time of reporting to our department, he was bed ridden. Because of diminished respiratory reflexes, respiration was supported by tracheostomy. The nutrition was supported by nasogastric route (Ryle’s Tube). As per the patient’s caretaker, the patient developed repetitive and sustained mouth opening since 15 days. They reported to our department for needful management. The general physical examination revealed poor nutritional status of the patient. The clinical examination revealed repetitive and sustained mouth opening for prolonged period. The sustained open mouth position was present even at the time of patient’s treatment (Figure 1). No other abnormality was detected extraorally as well as intraorally. Based on the case history and clinical examination, a provisional diagnosis of secondary OMD due to head injury was framed. The differential diagnosis includes temporomandibular joint dislocation (TMJ dislocation) and hypocalcemic tetani. The patient was advised to undergo routine blood investigations along with estimation of serum calcium and CT-scan of face (in open mouth position). The laboratory findings were within normal limits. CT-scan revealed translation of bilateral condyles within boundaries of glenoid fossae. Evaluation of electromyographic (EMG) activity of bilateral lateral pterygoid muscle revealed hyperactivity of lateral pterygoid muscles during function. Possibility of hypocalcemic tetani was ruled out as the serum calcium levels were within normal limits. Bilateral TMJ dislocation was ruled out by the computerized tomography findings of normal condylar position at maximum mouth opening. Based on case history, clinical examination, blood investigations, radiological examination, and EMG findings, the final diagnosis of secondary OMD (jaw-opening type) was established. The patient was prescribed antidystonic medications such as carbamazepine (200 mg) orally twice daily and tablet Baclofen (20 mg) orally twice daily for 5 days. There was mild improvement in symptoms on follow-up examination. The further course of treatment was discussed with the caretaker and it was decided to use BTX-A for long-term relief. BTX-A (50 units per muscle) was injected in bilateral lateral pterygoid muscles using intraoral approach. The rationale was to decrease the muscle hyperactivity. The onset of clinical effects of BTX-A in the form of muscle weakness requires approximately 10 to 14 days. So, short-term maxillomandibular fixation (MMF) using Ivy-Eyelet method of wiring was done for 2 weeks. The MMF was done in such a fashion that it will permit 20 to 25 mm of mouth opening corresponding to condylar rotation in glenoid fossae. At the same time, the MMF won’t allow for full translatory movement of condyle as seen at the time of maximum mouth opening (Figure 2). This form of MMF indirectly restricts the full activity of lateral pterygoid muscle. The patient was re-evaluated at 2-week interval and all the dental wirings were removed. The patient remained asymptomatic without recurrence of dystonic movements till the writing of this case report.
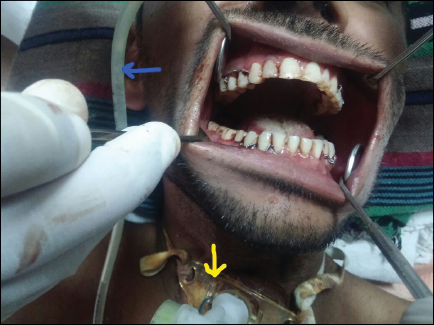
Patient presented with sustained mouth opening (jaw opening dystonia). Additionally, Ryle’s Tube (blue arrow) and Tracheostomy Tube (yellow arrow) are also evident.
Maxillomandibular fixation (MMF) done in such a fashion that it permits 20 to 25 mm of mouth opening.

Discussion
OMD can involve various muscles of mastication, face, or tongue. The clinical presentation can be in the form of repetitive and sustained contraction of involved muscles. With respect to muscles of mastication, the OMD can be classified as mouth-closing dystonia or mouth-opening dystonia. 3 In our case, the clinical features are suggestive of OMD of mouth-opening type.
The exact mechanism behind OMD is not well known. OMD can be related to metabolic disorders, central nervous system trauma, brain hypoxia, and demyelination disorders of brain. 4 Various abnormal movements like tremor, tics, Parkinsonism, chorea, and dystonia may be seen in patients with traumatic brain injury several months following traumatic brain injury. The incidence of such movement disorders ranges between 13% and 66%. Tremor and dystonia are the most common movement disorder seen in such cases. 5 In our case, the OMD was secondary to traumatic brain injury. The onset of OMD was approximately 2.5 years after head injury.
OMD is a relatively rare condition and is often misdiagnosed. As the sign and symptoms are often related to jaw movements, the probability of diagnosing it as TMJ disorders is quite high. The diagnosis of OMD is quite difficult because of its variable clinical presentations. There is no organic test for diagnosis of OMD. The diagnosis is chiefly based on case history, clinical examination, and evidence of muscle hyperactivity based on EMG evaluation. 6 In our case, the patient had a typical history of traumatic head injury. The clinical evaluation revealed repetitive and sustained mouth opening and EMG examination showed hyperactivity of bilateral lateral pterygoid muscles. Based on the case history, clinical presentation, and EMG studies, the diagnosis of secondary OMD was established.
Various treatment modalities for OMD involve physiotherapy, appliance therapy (sensory tricks), antidystonic medications, muscle afferent blocks, BTX-A injections, peripheral surgical procedures, central surgical procedures (deep brain stimulation surgery, pallidotomy, thalamotomy, focused ultrasonic lesioning), and supportive therapy (psychosocial and occupational therapy, support groups participation, cognitive behavioral therapy). 6 We have tried medicinal management for management of OMD. There was only partial relief with medicinal management. Therefore, we opted for BTX-A as its role in the management of OMD is well documented in literature.
The BTX-A is a potent neurotoxin used in the management of OMD. It blocks the release of acetylcholine neurotransmitter at the motor end plate. In the absence of neurotransmitter signal, the muscle gets temporarily denervated due to lack of motor stimulation. 6 The exact dose of BTX-A to be injected is based on the muscle mass. For lateral pterygoid muscle, the dose to be used ranges between 45 and 50 units per muscle.2, 7 We have used 50 units of BTX-A on each side lateral pterygoid muscle.
Role of sensory tricks to relieve dystonia is documented in literature. Alteration in occlusal contacts by use of acrylic appliance is beneficial in mouth-closing dystonia. The mechanism of action is by alteration in sensory/proprioceptive inputs to muscles at the time of occlusal contacts (sensory tricks).1, 3 In our case, the patient was suffering from jaw-opening dystonia. Therefore, alteration in sensory inputs to the involved muscle was desirable during mouth opening. We have done sensory tricks in the form of restricting lateral pterygoid muscle activity by MMF.
Conclusion
Although OMD is not a common clinical entity but its possibility can’t be ruled out entirely. The usual misdiagnosis framed is related to TMJ disorders. Lack of adequate data related to OMD in the literature related to dentistry and oral surgery is the main cause for such misdiagnosis. The oral and maxillofacial surgeons and dentists should consider possibility of OMD unless its possibility is ruled out by various diagnostic tests.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.